")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 16
Therapeutic Strategies for Mitigating Driving Risk in Patients with Narcolepsy
Received 24 July 2020
Accepted for publication 25 September 2020
Published 12 November 2020 Volume 2020:16 Pages 1099—1108
DOI https://doi.org/10.2147/TCRM.S244714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Catherine A McCall,1,2 Nathaniel F Watson3
1Department of Pulmonary, Critical Care, and Sleep Medicine, VA Puget Sound Health Care System, Seattle, WA, USA; 2Department of Psychiatry and Behavioral Sciences, University of Washington Sleep Medicine Center, Seattle, WA, USA; 3Department of Neurology, University of Washington Sleep Medicine Center, Seattle, WA, USA
Correspondence: Catherine A McCall
VA Puget Sound Health Care System, 1660 S. Columbian Way, Seattle, WA 98108, USA
Email [email protected]
Abstract: Narcolepsy is a central nervous system hypersomnia disorder characterized by uncontrollable episodes of daytime sleep, sleep state instability, and cataplexy (sudden loss of muscle tone precipitated by emotion). Individuals with narcolepsy report more frequent sleep-related crashes, near crashes, and drowsy driving than drivers with other sleep disorders. As such, evaluating risk of sleep-related crashes is of great importance for this patient population. There are no established guidelines for ensuring driving safety in patients with narcolepsy; however, many providers currently use a combination of subjective report, report of prior crashes or near-misses, report of previously falling asleep while driving, sleepiness screening tools, and maintenance of wakefulness testing (MWT) to determine risk. Driving simulator tests, though often unavailable to the clinician, provide data to support the use of MWT for evaluation of alertness in drivers with narcolepsy. Treatments such as modafinil may improve driving performance; however, the impact of other treatments such as stimulants and sodium oxybate on driving has not been extensively studied. Behavioral and lifestyle modifications may also reduce risk, including scheduled naps, driving only short distances, and avoiding driving after meals, sedating medications, and alcohol intake. Even with effective treatment, alertness in patients with narcolepsy may never reach that of normal drivers; however, studies have suggested that narcolepsy patients may be able to drive safely with appropriate limitations.
Keywords: narcolepsy, cataplexy, driving, safety
Introduction
Narcolepsy is a lifelong disorder of hypersomnolence characterized by daily periods of irrepressible need to sleep, or frequent daytime lapses into sleep. The diagnosis typically requires a formal series of laboratory studies to demonstrate objective daytime sleepiness with the presence of two or more sleep-onset rapid eye movement (REM) periods during multiple sleep latency testing (MSLT).1 Narcolepsy can only be diagnosed in the absence of other causes of hypersomnia, such as untreated obstructive sleep apnea, chronic insufficient sleep, and sedating medications or drugs. Some patients with narcolepsy also experience cataplexy, a phenomenon in which strong emotions precipitate bilateral loss of muscle tone with retained consciousness, and/or sleep paralysis, the complete inability to move after a partial awakening from REM sleep. Treatment of narcolepsy is generally symptomatic, and may include wakefulness-promoting medications such as stimulants, REM-suppressing medications for the treatment of cataplexy, and/or sodium oxybate (Xyrem®), a sodium salt of gamma-hydroxybutyric acid (GHB) that enhances sleep consolidation and reduces cataplexy.2,3
Drowsy driving risk is a high concern for individuals with narcolepsy. Episodes of excessive sleepiness may occur at any point of the day and are difficult to resist regardless of the situation. Additionally, narcolepsy is a disorder not only of hypersomnolence but of REM sleep dissociation. Those with narcolepsy are more likely to enter a state of REM sleep during brief episodes of sleep, during which a state of paralysis occurs, leading to higher risk of a crash when driving. Cataplexy occurring as a sequalae to a strong emotion can cause loss of muscle tone to the arms, legs, and/or posture and may also increase risk of a crash.4 Mitigating strategies to reduce risk of drowsy driving crashes should optimally account for all of these risks.
Epidemiological and crash report data indicate a large proportion of narcolepsy patients experience sleepiness that interferes with driving (Table 1). It should be noted that few of these studies analyze accident risk separately for treated versus untreated patients with narcolepsy. One study of adults with narcolepsy found 66% reported falling asleep at the wheel, 29% experience cataplexy while driving, and 12% experience sleep paralysis while driving.4 Individuals with narcolepsy have a three- to four-fold increased risk of crashing compared to those without narcolepsy, with over a third reporting an accident due to sleepiness.5–7 Narcolepsy has also been found to confer greater risk for sleep-related accidents than other sleep disorders.8,9 In one study of patients with sleep apnea, narcolepsy, and other hypersomnia disorders, the proportion of patients with narcolepsy reporting sleep-related accidents was more than four times that of controls. Narcolepsy patients who reported having accidents were not more objectively sleepy on MSLT than those who did not have accidents, suggesting factors other than sleepiness contribute to accident risk.9 In January 2010, the Federal Motor Carrier Safety Administration’s Medical Review Board concluded that even those narcolepsy patients who are treated still show abnormal levels of daytime sleepiness, and recommended all individuals with narcolepsy be ineligible for a commercial driver’s license, even with treatment.10
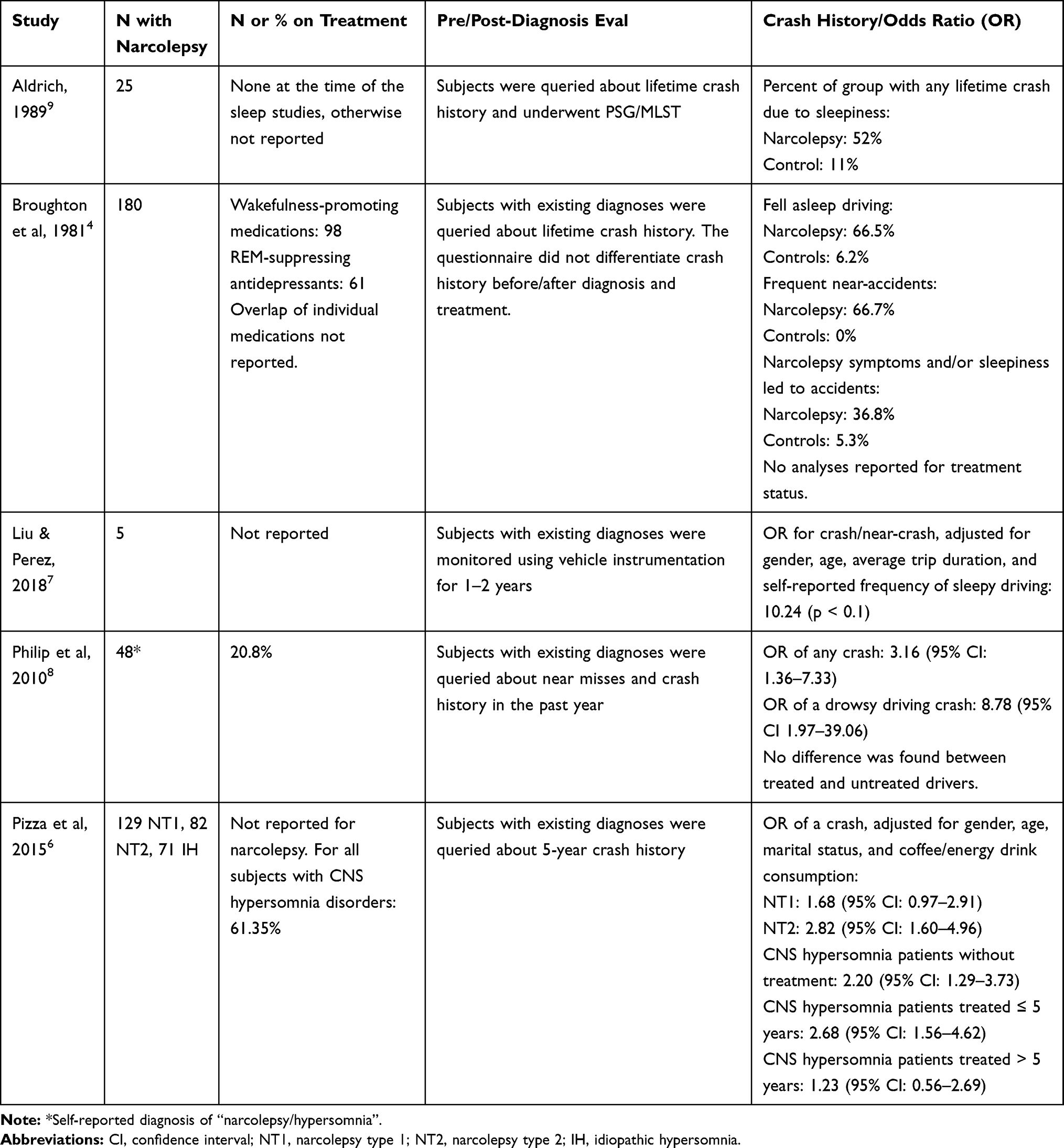 |
Table 1 Studies Assessing Crash Risk in Patients with Narcolepsy |
Despite the evidence supporting the need for therapeutic risk reduction, monitoring, and mitigation of drowsy driving in those with narcolepsy, there is a relative paucity of studies investigating these strategies. This may be due to the fact that narcolepsy is a relatively rare disorder, occurring in only about 0.05% of the general population.11,12 In this paper, we review the evidence for evaluating and mitigating risk for sleep-related crashes in individuals with narcolepsy.
Evaluation of Crash Risk
There are currently no universally accepted guidelines for assessing risk of drowsy driving in narcolepsy patients. Research studies on crash risk in sleepy patients typically employ tests of real or simulated driving; however, these measures are not typically available to the clinician. In practice, evaluation of driving risk typically relies on self-reported sleepiness, in conjunction with objective measures of daytime sleepiness and sleep propensity. Of note, many studies examining measurements of sleepiness and driving risk include both patients with narcolepsy and those with other central nervous system (CNS) hypersomnia disorders, such as idiopathic hypersomnia (IH). Although IH is also defined as a disorder with pathologic sleepiness, it lacks features of narcolepsy, such as cataplexy, sleep paralysis, and sleep stage instability, that may increase risk of drowsy driving accidents.1
Subjective measures of sleepiness include the Epworth Sleepiness Scale (ESS), a series of questions assessing how likely the respondent is to doze off in a variety of situations.13 The ESS is the most widely used tool for assessing sleep propensity in both research and clinical practice. Some studies have found that high scores at this scale seem to be clearly linked with accident risk;8,14–16 however, others have not found a clear correlation with real or simulated driving performance.17,18 Measures of self-reported sleepiness often do not reflect performance on cognitive or vigilance testing.19–21 Additionally, one’s ability to rate their own sleepiness and impairment is negatively impacted by sleepiness, similar to those driving while intoxicated.22,23 Objective measures are therefore favored to accurately rate the risk of a drowsy driving accident.
The most frequently used objective measure of sleepiness for assessing safety to drive is the maintenance of wakefulness test (MWT).24,25 The MWT requires the patient to sit quietly in a dimly lit room without falling asleep, with a maximum duration of 40 minutes for each of 4 sessions. Mean sleep onset latencies (SOL) under 8 minutes are considered abnormal, but SOL between 8 and 40 minutes are of uncertain significance. The current American Academy of Sleep Medicine guideline discusses indications for the use of the MWT in assessing ability to stay awake, but cautions that its predictive value for assessing actual accident risk has not been established.25 One study found MWT mean sleep latency correlated with the mean number of inappropriate lane changes for both untreated and treated (e.g., with modafinil) CNS hypersomnia disorder patients. However, the MWT did not correlate with deviation from the center of the lane in untreated or treated patients.26 A study of MWT scores and driving simulator performance in CNS hypersomnia disorder patients found worse performance in the pathologically sleepy group (defined as mean SOL of 19 minutes or less). Although those participants with intermediate sleepiness (mean SOL 20–33 minutes) had more inappropriate lane crossings, the difference between this group and the alert (mean SOL 34–40 minutes) and control (mean SOL >34 minutes) groups was statistically nonsignificant15 (Figure 1). Another study comparing the MWT to both simulated and real driving in CNS hypersomnia disorders found untreated patients had both shorter SOL on the MWT (median 20.8 minutes) and worse simulated driving performance compared to treated patients. Treated patients had shorter SOL (median 34.9 minutes) than controls (median 40 minutes), but driving performance was identical.18 This suggests hypersomnia patients with MWT scores between 30 and 40 minutes may have appropriate driving performance. Indeed, based on current research, Ingram et al recommended to use a minimally acceptable MWT result of 30 minutes for narcolepsy patients, with the understanding that almost all patients with narcolepsy continue to have some degree of sleepiness even with effective pharmacologic therapy.27
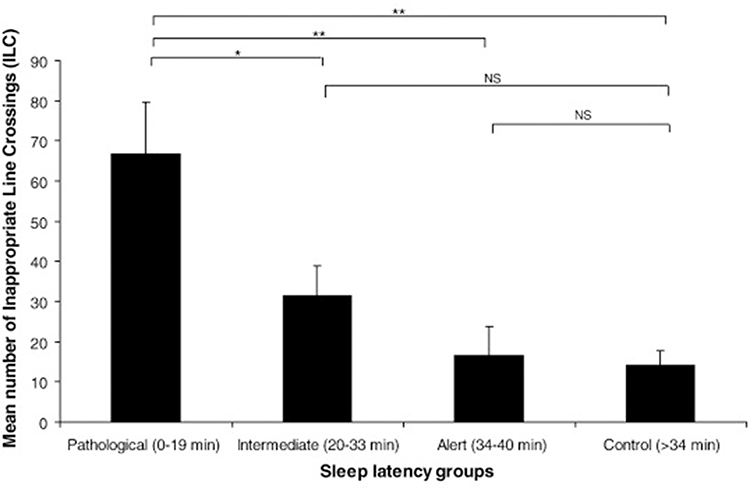 |
Figure 1 Mean number of inappropriate lane crossings for individuals in different categories of Maintenance of Wakefulness score. Reprinted from Internat J Psychophys, 89, Philip P, Chaufton C, Taillard J, et al. Maintenance of Wakefulness Test scores and driving performance in sleep disorder patients and controls. 195–202, copyright (2013), with permission from Elsevier.15 *and **= statistically significant difference; NS = non-statistically significant difference. |
The multiple sleep latency test (MSLT), in contrast, has been found to have a relatively lower correlation with driving performance in patients with narcolepsy, or no correlation at all.6,18 The MSLT is a daytime test, typically performed the day after an overnight laboratory polysomnogram, that entails a series of 4–5 nap opportunities spread throughout the day. A patient is considered to have objective sleepiness if their mean sleep latency is ≤8 minutes. A diagnosis of narcolepsy also requires the occurrence of at least two REM periods within 15 minutes of sleep onset. The MSLT measures objective sleepiness for untreated patients in order to diagnose a hypersomnia disorder, and does not ask the patient to try to stay awake or alert. Accordingly, the MWT is considered more sensitive to changes to the ability to stay awake as a result of treatment.28 The MWT and MSLT essentially measure different aspects of sleepiness, with the MWT evaluating sleep tendency plus the ability to maintain arousal, whereas the MSLT is a measure of sleep propensity alone. The MWT is therefore a closer approximation of driving alertness.18
As noted in previous sections, sleepiness may be only one facet of risk for drowsy driving accidents in patients with narcolepsy. Driving involves the ability to divide attention between stimuli, remain vigilant through monotonous driving scenarios, and react appropriately to sudden changes. One study tested whether neuropsychological testing of alertness, vigilance, and divided and continuous attention could be used to predict simulated driving performance, but found no correlation between these measures with high inter-participant differences.17 For patients with narcolepsy, sudden stress or emotional triggers may also present risk of accidents independently of sleepiness due to cataplexy. There is no test available to predict this risk. Some authors have also suggested individuals with narcolepsy have a perceptual-encoding deficit (dysfunctional processing of relevant stimulus properties leading to slower response time) that may affect performance, though without reported impairment in motor speed, vigilance, information processing speed or decision-making accuracy.29
The most accurate objective test of driving ability available is a real driving test. Most studies on driving performance hold this as the gold standard when comparing other measures. Driving tests of patients with narcolepsy are typically performed in research settings and are not practically feasible from a clinical standpoint. As an alternative testing measure, simulated driving tests have been developed to test highway driving scenarios, measuring such events as inappropriate line crossings (ILC) and the standard deviation of lateral position (SDLP), which is a measure of the deviation of the vehicle from the center of the lane. In simulator studies, patients with narcolepsy demonstrated more SDLP, hit obstacles more frequently, and had a higher crash rate than controls.17,18,30 At least one study found similar results in simulated and real SDLP performance in CNS hypersomnia patients.18 The authors suggest using both simulated driving and the MWT may provide complementary measures for evaluating sleep-related driving impairment.
One survey of 52 pediatric sleep providers on assessing readiness to drive for adolescents with narcolepsy found that the most important clinical factors included history of previous fall-asleep crashes or near-miss crashes, followed by subjective sleepiness as reported by the patient or caregiver, and then cataplexy as reported by the patient or caregiver.27 Measures such as the MWT and MSLT were given somewhat lower weight (Figure 2). Fifty-four percent of respondents were unsure whether their US state allows physicians to report a patient to the department of motor vehicles who has a condition that makes driving unsafe, and 46% of respondents practicing in a mandatory reporting state reported they were uncertain whether their state mandated reporting. In the US, six states require mandatory reporting of medical conditions that could impair driving (California, Delaware, Nevada, New Jersey, Oregon, and Pennsylvania) to licensing or public health authorities.27 Each of these states has different procedures for communicating concerns for driving risk. Providers may be liable for negligence if they fail to report a patient with narcolepsy who is later involved in a motor vehicle accident. Other states allow reporting, or may request completion of a medical form after the driver’s license applicant self-reports a condition that impairs driving. Driver’s license applicants in the European Union and United Kingdom also require assessment of fitness to drive.31 These issues highlight the differences between measures in academic and research settings and the “real world” evaluation of sleep-related accident risk for patients with narcolepsy.
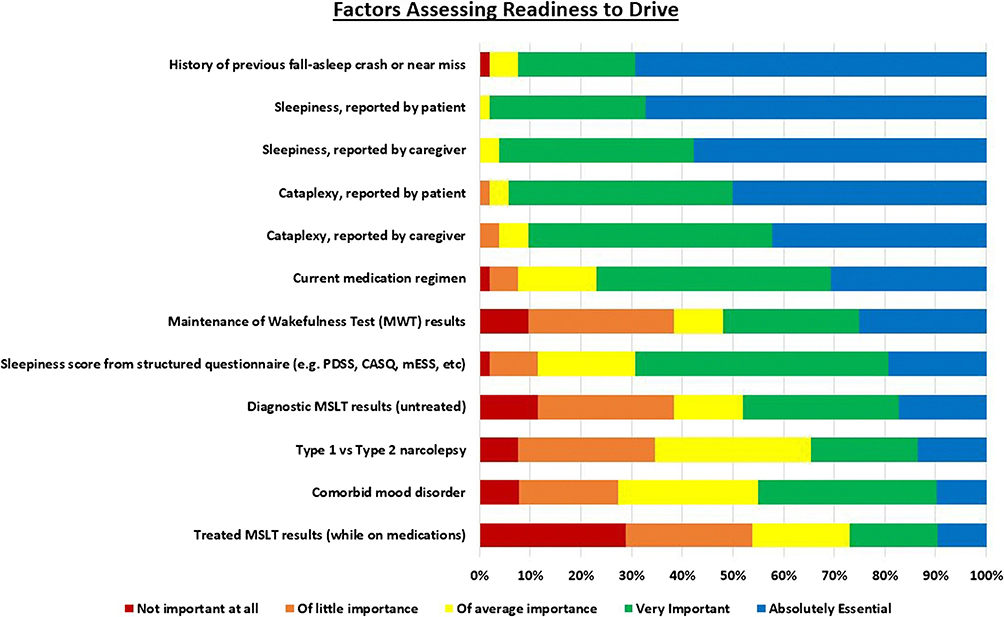 |
Figure 2 Factors considered important by pediatric sleep providers when assessing the readiness to drive safely in patients with narcolepsy. Reprinted by permission from Springer Nature, Springer, Sleep Breath, Assessing readiness to drive in adolescents with narcolepsy: what are providers doing? Ingram DG, Marciarille AM, Ehsan Z, Perry GV, Schneider T, Al-Shawwa B. Copyright (2019), 23(2):611‐617.27 |
Pharmacologic Treatments as Risk Mitigation
Wakefulness-Promoting Medications
The mainstay of treatment for CNS hypersomnia disorders such as narcolepsy are wakefulness-promoting medications and stimulants.32 These medications reduce excessive sleepiness in patients with narcolepsy; however, the ability of a patient with narcolepsy to stay awake is rarely comparable to normal controls even with treatment.32,33 The most commonly used medications are wakefulness-promoting agents (modafinil and armodafinil), but stimulants such as methylphenidate and amphetamine salts are also frequently used.34 Two additional medications, solriamfetol and pitolisant, have also been recently approved for treating excessive daytime sleepiness in narcolepsy. Few studies have assessed how effective wakefulness-promoting medications and stimulants are for improving driving performance in narcolepsy patients. Two studies in narcolepsy patients found modafinil improved real driving performance relative to placebo, although it did not improve lane-keeping to the level of control drivers.18,26 In reports of real accident history, the use of modafinil or methylphenidate has been associated with lower risk of motor vehicle accident injury in drivers with narcolepsy.35 Likewise, a study of self-reported crashes found that while untreated CNS hypersomnia patients reported more crashes over the past five years than controls, there was no difference in reported crashes between hypersomnolence patients treated with a psychostimulant medication for the past five years and controls.6
Although stimulants may improve clinical symptoms and reduce drowsy driving risk, they also have potential adverse effects. Non-stimulant wake-promoting medications such as modafinil and armodafinil generally have mild side effects including headache, nausea, dry mouth, and loss of appetite.36 Stimulant drugs such as methylphenidate and amphetamine salts typically have more pronounced side effects including anxiety, arrhythmias, loss of appetite, nausea, insomnia, and psychosis.37 Although abuse potential can be problematic in patients receiving stimulants, this issue is rare among individuals with a definitive narcolepsy diagnosis.34
Sodium Oxybate
Sodium oxybate (Xyrem®) also improves sleepiness in narcolepsy. This medication is a GABAB receptor agonist and central nervous system depressant that is approved for the treatment of narcolepsy. The medication is taken in two doses overnight, one at bedtime and the second 2.5 to 4 hours later. Sodium oxybate can treat cataplexy, improves subjective daytime sleepiness, increases ability to remain awake in maintenance of wakefulness test (MWT) performance, and reduces sleep attacks in those with narcolepsy.3,34 The mechanism by which excessive sleepiness is improved is likely related to decreased arousals, increased sleep efficiency, and increased slow wave sleep.38 However, it may take as long as two months for patients to experience treatment response, with one study showing maximum effect after 106 days for excessive sleepiness and 213 days for cataplexy.39 As a sodium salt of GHB, sodium oxybate can impair driving after being ingested due to profound sleepiness and reduced consciousness, and there have been reports of “sleep driving” in patients while taking it.40–45 However, sodium oxybate has a half-life of only 30–40 minutes, with rapid clearance, reducing the incidence of these medication-related parasomnias.46 One study assessed driver simulator performance on sodium oxybate and found severe driving impairment one hour after dosing that was similar to drivers with breath alcohol concentrations of 0.08% to 0.1%, which is considered legally impaired for drivers in the US. However, driving performance returned to baseline after three and six hours, and no GHB was detected in the serum of participants after 6 hours.40 Patients should be counseled regarding their dose times to ensure at least 6 hours have passed since their last dose before driving. (Xyrem product information, www.xyrem.com)
Other treatments for cataplexy include antidepressants such as serotonin-norepinephrine reuptake inhibitors (SNRIs) like venlafaxine, selective serotonin reuptake inhibitors (SSRIs) like fluoxetine, and tricyclic antidepressants (TCAs) such as clomipramine.47,48 The mechanism of action for these agents is to suppress REM sleep by increasing brainstem monoamine levels. Another medication shown to have positive effect on both daytime sleepiness and cataplexy is pitolisant, a histamine H3 receptor inverse agonist.49 Effects of these medications specifically on driving performance in narcolepsy patients have not been evaluated.
Behavioral Measures as Risk Mitigation
Regardless of the risk mitigation measures employed, all patients with narcolepsy should be counseled about the risk of crashes occurring as a result of sleepiness, cataplexy, and sleep paralysis. Symptoms of drowsy driving may include disconnected thoughts, difficulty focusing, daydreaming, heavy eyelids, frequent blinking, head nodding, difficulty remembering the last few miles drive, and lane drifting.50,51 Studies have consistently shown that the drowsy driver’s ability to self-rate driving impairment is unreliable, thus drivers should plan ahead if sleepiness is anticipated.23 Individuals with narcolepsy should also reduce risk of cataplexy by avoiding emotional triggers known to precipitate its occurrence, if possible.
Successful behavioral mitigation measures for reducing drowsy driving risk in narcolepsy patients also include scheduling naps before driving, keeping trips short, taking nap breaks during longer drives, and taking turns driving with another person.52,53 Avoiding nighttime shift work or driving at times when the individual might be especially sleepy (for example, late night or early morning) may also reduce the risk of a drowsy driving crash. Additional recommendations for timing of driving and lifestyle include avoiding driving after meals, consumption of simple sugars, alcohol (which may cause rebound cataplexy after metabolism), and medications that increase daytime sleepiness, such as anxiolytics, antihistamines, and long-acting hypnotics.54
Adequate sleep is the only proven preventative measure against fall asleep crashes in the general population. In patients with narcolepsy, planned naps can be an effective therapeutic strategy and can mitigate the risk of drowsy driving.54,55 Studies on the effectiveness of naps in normal participants have shown a short 15–20 minute nap improves driving performance, with longer naps causing grogginess due to sleep inertia upon awakening.56,57 Drinking 1–2 cups of coffee and pulling over for a 20-minute nap has also been shown to temporarily increase alertness in drowsy drivers, although again this was a study of normal adults.58 One study of a repeated nap paradigm in narcolepsy with cataplexy patients found a single long nap, one-third the duration of nocturnal sleep (~2–3 hours) and occurring 12 hours after the nocturnal midsleep time, improved reaction time performance.55 Naps may also improve performance on the MWT as a proxy measure of driving alertness.59,60
Caffeine use has been well studied in non-narcoleptic subjects as a wakefulness-promoting substance that is widely used and easily obtained. A recent systematic review and meta-analysis of 45 studies found caffeine improved performance on tests of attention, executive function, response time, as well as measures of driving performance.61 In patients with narcolepsy, caffeine has been found in limited research to improve sleepiness, but studies are lacking on its effectiveness to mitigate driving risk.62 Strategic dosing with caffeine or a prescribed stimulant medication prior to driving may be considered as an augmenting agent to further reduce risk of drowsy driving.
Other behavioral measures such as exercise, chewing gum, listening to music, opening car windows, talking to passengers, or talking on a cell phone are not beneficial for normal drivers, let alone those with narcolepsy, and may even increase risk of crashes due to distraction.63,64
With appropriate driving precautions and effective treatment, patients with narcolepsy may be able to drive safely. Indeed, a case–control study focused on driving behavior and crash history found narcolepsy patients over 40 years old who adopted effective behavioral strategies such as napping, taking medications before driving, and pulling over for a nap when sleepy had even fewer crashes than controls.65 There is little evidence that narcolepsy is continuously progressive. In fact, older patients with narcolepsy may be generally less sleepy than younger patients, and less likely to demonstrate REM sleep desynchrony, despite experiencing age-related decrements in sleep quality.66 Worsening sleepiness in older patients with narcolepsy should prompt evaluation for comorbid sleep disorders such as obstructive sleep apnea. However, to our knowledge, studies on driving performance in patients with narcolepsy have not compared simulated or actual driving performance by age group.
Conclusion
Narcolepsy is a chronic CNS hypersomnia causing significant impairment in multiple aspects of life including driving performance. The disorder often arises in the adolescent and young adult years, when most people are beginning to drive. Patients with narcolepsy are at higher risk of sleep-related accidents than the normal population due to the propensity for sleep attacks, sleep paralysis, and cataplexy. Given the morbidity and mortality associated with drowsy driving, which kills over 6000 people per year in the United States, and the high risk of narcolepsy patients for sleep-related accidents, strategies to evaluate and modify driving risk are of high importance.67 There are no established guidelines for determining appropriateness for driving in treated narcolepsy patients; additionally, many providers may not be aware of mandated reporting requirements in their region. When evaluating driving risk, the use of the MWT may be the most commonly used objective measure of alertness. Although caution should be used in applying MWT as a predictive measure for driving performance or risk, it can help establish the ability of the narcolepsy patient to resist sleep propensity. Use of the MWT should especially be considered for new or young drivers, patients with residual sleepiness, and those with prior history of fall-asleep crashes.
Narcolepsy treatments have demonstrated some efficacy in improving wakefulness and reducing cataplexy in patients with narcolepsy; however, few studies have evaluated whether these treatments improve driving safety. Modafinil may improve both MWT scores and driving performance in narcolepsy patients, though not to the level of normal drivers. Sodium oxybate (Xyrem) impairs driving after ingestion, but has a short half-life and improves next-day alertness. Other behavioral measures that may reduce driving risk include scheduled naps, driving only short distances at one time, and avoiding factors that may increase sleepiness, such as driving after heavy meals, simple carbohydrates, sedating medications, and alcohol intake.
Narcolepsy is a rare sleep disorder, but the impacts of unsafe driving in this population due to excessive sleepiness, cataplexy, and sleep paralysis are potentially far-reaching. Additional research on the impacts of narcolepsy treatment on driving safety are warranted, especially for newer medications, caffeine, and behavioral strategies that are the cornerstones of current recommendations for safe driving in all sleepy patients. Clinical providers should also be educated on the risks of drowsy driving, how to screen for potentially unsafe driving, when to consider MWT, and whether reporting a diagnosis of narcolepsy to departments of public health or motor vehicles is required in their state or country. Providers should understand how to effectively counsel patients on safe driving practices, particularly for new drivers. With the appropriate treatment, counseling, precautions and limits, many narcolepsy patients may be able to drive safely during everyday life.
Disclosure
The authors report no conflicts of interest for this work.
References
1. American Academy of Sleep Medicine. The International Classification of Sleep Disorders - Third Edition (ICSD-3). Darien, IL: American Academy of Sleep Medicine; 2014.
2. Fuller DE, Hornfeldt CS. From club drug to orphan drug: sodium oxybate (Xyrem) for the treatment of cataplexy. Pharmacotherapy. 2003;23(9I):1205–1209. doi:10.1592/phco.23.10.1205.32756
3. Alshaikh MK, Tricco AC, Tashkandi M, Mamdani M, Straus SE, BaHammam AS. Sodium oxybate for narcolepsy with cataplexy: systematic review and meta-analysis. J Clin Sleep Med. 2012;8(4):451–458. doi:10.5664/jcsm.2048
4. Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, Nevsimalova S, Roth B. Life effects of narcolepsy in 180 patients from North America, Asia and Europe compared to matched controls. Can J Neurol Sci. 1981;8(4):299–304. doi:10.1017/S0317167100043419
5. Valley V, Broughton R. Daytime performance deficits and physiological vigilance in untreated patients with narcolepsy-cataplexy compared to controls. Rev Electroencephalogr Neurophysiol Clin. 1981;11(1):133–139. doi:10.1016/S0370-4475(81)80044-5
6. Pizza F, Jaussent I, Lopez R, et al. Car crashes and central disorders of hypersomnolence: a french study. PLoS One. 2015;10(6):e0129386. doi:10.1371/journal.pone.0129386
7. Liu S-Y, Perez MA, Lau N. The impact of sleep disorders on driving safety—findings from the Second Strategic Highway Research Program naturalistic driving study. Sleep. 2018;41(4). doi:10.1093/sleep/zsy023
8. Philip P, Sagaspe P, Lagarde E, et al. Sleep disorders and accidental risk in a large group of regular registered highway drivers. Sleep Med. 2010;11(10):973–979. doi:10.1016/j.sleep.2010.07.010
9. Aldrich MS. Automobile accidents in patients with sleep disorders. Sleep. 1989;12(6):487–494. doi:10.1093/sleep/12.6.487
10. Medical Review Board, U.S. Department of transportation federal motor carrier safety administration meeting summary, January 6, 2010. Available from: https://www.fmcsa.dot.gov/sites/fmcsa.dot.gov/files/docs/Final_Jan_6_2010_MRB_Meeting_Summary.pdf.
11. Ohayon MM, Priest RG, Zulley J, Smirne S, Paiva T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology. 2002;58(12):1826–1833. doi:10.1212/WNL.58.12.1826
12. Longstreth WJ, Koepsell T, Ton T, Hendrickson A, van Belle G. The epidemiology of narcolepsy. Sleep. 2007;30(1):13–26. doi:10.1093/sleep/30.1.13
13. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
14. Howard ME, Desai AV, Grunstein RR, et al. Sleepiness, sleep-disordered breathing, and accident risk factors in commercial vehicle drivers. Am J Respir Crit Care Med. 2004;170(9):1014–1021. doi:10.1164/rccm.200312-1782OC
15. Philip P, Chaufton C, Taillard J, et al. Maintenance of Wakefulness Test scores and driving performance in sleep disorder patients and controls. Int J Psychophysiol. 2013;89(2):195–202. doi:10.1016/j.ijpsycho.2013.05.013
16. Powell N, Shechtman K, Riley R, Guilleminault C, Chiang R, Weaver E. Sleepy driver near-misses may predict accident risks. Sleep. 2007;30:331–342. doi:10.1093/sleep/30.3.331
17. Kotterba S, Mueller N, Leidag M, et al. Comparison of driving simulator performance and neuropsychological testing in Narcolepsy. Clin Neurol Neurosurg. 2004;106(4):275–279. doi:10.1016/j.clineuro.2003.12.003
18. Sagaspe P, Micoulaud-Franchi JA, Coste O, et al. Maintenance of wakefulness test, real and simulated driving in patients with narcolepsy/hypersomnia. Sleep Med. 2019;55:1–5. doi:10.1016/j.sleep.2018.02.009
19. Findley L, Suratt P, Dinges D. Time-on-task decrements in “Steer Clear” performance of patients with sleep apnea and narcolepsy | sleep | oxford academic. Sleep. 1999;22(6):804–809. doi:10.1093/sleep/22.6.804
20. Kotterba S, Rasche K, Widdig W, Blombach S, Duchna K, Duchna H-W. Vigilance and neuropsychological capacity in obstructive sleep apnea syndrome and chronic obstructive pulmonary disease. Somnologie. 1998;2:117–122. doi:10.1007/s11818-998-0016-x
21. Kotterba S, Rasche K, Widdig W, et al. Neuropsychological investigations and event-related potentials in obstructive sleep apnea syndrome before and during CPAP-therapy. J Neurol Sci. 1998;159(1):45–50. doi:10.1016/S0022-510X(98)00131-2
22. Van Dongen HPA, Maislin G, Mullington JM, Dinges DF. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003;26(2):117–126.
23. Reyner LA, Horne JA. Falling asleep whilst driving: are drivers aware of prior sleepiness? Int J Legal Med. 1998;111(3):120–123. doi:10.1007/s004140050131
24. Bhat A, Marciarille AM, Stevens D, Ingram DG. Drowsy driving considerations in non-commercial drivers for the sleep physician. J Clin Sleep Med. 2019;15(7):1069–1071. doi:10.5664/jcsm.7898
25. Littner M, Kushida C, Wise M, et al. Practice parameters for clinical use of the multiple sleep latency test and the maintenance of wakefulness test. Sleep. 2005;28(1):113–121. doi:10.1093/sleep/28.1.113
26. Philip P, Chaufton C, Taillard J, et al. Modafinil improves real driving performance in patients with hypersomnia: a randomized double-blind placebo-controlled crossover clinical trial. Sleep. 2014;37(3):483–487. doi:10.5665/sleep.3480
27. Ingram DG, Marciarille AM, Ehsan Z, Perry GV, Schneider T, Al-Shawwa B. Assessing readiness to drive in adolescents with narcolepsy: what are providers doing? Sleep Breath. 2019;23(2):611–617. doi:10.1007/s11325-019-01799-2
28. Sangal RB, Thomas L, Mitler MM. Maintenance of wakefulness test and multiple sleep latency test; measurement of different abilities in patients with sleep disorders. Chest. 1992;101(4):898–902. doi:10.1378/chest.101.4.898
29. Henry G, Satz P, Heilbronner R. Evidence of a perceptual-encoding deficit in narcolepsy?. Sleep. 1993;16(2):123–127. doi:10.1093/sleep/16.2.123
30. Findley L, Unverzagt M, Guchu R, Fabrizio M, Buckner J, Suratt P. Vigilance and automobile accidents in patients with sleep apnea or narcolepsy. Chest. 1995;108(3):619–624. doi:10.1378/chest.108.3.619
31. Driver and Vehicle Licensing Agency. Neurological disorders: assessing fitness to drive. Available from: https://www.gov.uk/guidance/neurological-disorders-assessing-fitness-to-drive#primarycentral-hypersomnias–including-narcolepsy-type-1-and-type-2-narcolepsy-with-cataplexy.
32. Mitler MM, Aldrich MS, Koob GF, Zarcone VP. Narcolepsy and its treatment with stimulants. ASDA standards of practice. Sleep. 1994;17(suppl_8):352–371. doi:10.1093/sleep/17.suppl_8.S103
33. Boivin DB, Montplaisir J, Petit D, Lambert C, Lubin S. Effects of modafinil on symptomatology of human narcolepsy. Clin Neuropharmacol. 1993;16(1):46–53. doi:10.1097/00002826-199302000-00005
34. Takenoshita S, Nishino S. Pharmacologic management of excessive daytime sleepiness. Sleep Med Clin. 2017;12(3):461–478. doi:10.1016/j.jsmc.2017.03.019
35. Tzeng NS, Hsing SC, Chung CH, et al. The risk of hospitalization for motor vehicle accident injury in narcolepsy and the benefits of stimulant use: a nationwide cohort study in Taiwan. J Clin Sleep Med. 2019;15(6):881–889. doi:10.5664/jcsm.7842
36. Roth T, Schwartz JRL, Hirshkowitz M, Erman MK, Dayno JM, Arora S. Evaluation of the safety of modafinil for treatment of excessive sleepiness. J Clin Sleep Med. 2007;3(6):595–602. doi:10.5664/jcsm.26970
37. Leonard BE, McCartan D, White J, King DJ. Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects. Hum Psychopharmacol. 2004;19(3):151–180. doi:10.1002/hup.579
38. Plazzi G, Pizza F, Vandi S, et al. Impact of acute administration of sodium oxybate on nocturnal sleep polysomnography and on multiple sleep latency test in narcolepsy with cataplexy. Sleep Med. 2014;15(9):1046–1054. doi:10.1016/j.sleep.2014.04.020
39. Bogan RK, Roth T, Schwartz J, Miloslavsky M. Time to response with sodium oxybate for the treatment of excessive daytime sleepiness and cataplexy in patients with narcolepsy. J Clin Sleep Med. 2015;11(4):427–432. doi:10.5664/jcsm.4598
40. Liakoni E, Dempsey DA, Meyers M, et al. Effect of γ-hydroxybutyrate (GHB) on driving as measured by a driving simulator. Psychopharmacology (Berl). 2018;235(11):3223–3232. doi:10.1007/s00213-018-5025-2
41. Centola C, Giorgetti A, Zaami S, Giorgetti R. Effects of GHB on psychomotor and driving performance. Curr Drug Metab. 2018;19(13):1065–1072. doi:10.2174/1389200219666180124113802
42. Wallace DM, Maze T, Shafazand S. Sodium oxybate-induced sleep driving and sleep-related eating disorder. J Clin Sleep Med. 2011;7(3):310–311. doi:10.5664/JCSM.1082
43. Bosman IJ, Lusthof KJ. Forensic cases involving the use of GHB in The Netherlands. Forensic Sci Int. 2003;133(1–2):17–21. doi:10.1016/S0379-0738(03)00044-6
44. Al-Samarraie MS, Karinen R, Mørland J, Stokke Opdal M. Blood GHB concentrations and results of medical examinations in 25 car drivers in Norway. Eur J Clin Pharmacol. 2010;66(10):987–998. doi:10.1007/s00228-010-0870-x
45. Couper FJ, Logan BK. GHB and driving impairment. J Forensic Sci. 2001;46(4):15070J. doi:10.1520/jfs15070j
46. Liechti ME, Quednow BB, Liakoni E, et al. Pharmacokinetics and pharmacodynamics of γ-hydroxybutyrate in healthy subjects. Br J Clin Pharmacol. 2016;81(5):980–988. doi:10.1111/bcp.12863
47. Reading P. Cataplexy. Pract Neurol. 2019;19(1):21–27. doi:10.1136/practneurol-2018-002001
48. Houghton WC, Scammell TE, Thorpy M. Pharmacotherapy for cataplexy. Sleep Med Rev. 2004;8(5):355–366. doi:10.1016/j.smrv.2004.01.004
49. Szakacs Z, Dauvilliers Y, Mikhaylov V, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2017;16(3):200–207. doi:10.1016/S1474-4422(16)30333-7
50. Lyznicki JM, Doege TC, Davis RM, Williams MA. Sleepiness, driving, and motor vehicle crashes. Council on Scientific Affairs, American Medical Association. JAMA. 1998;279(23):1908–1913. doi:10.1001/jama.279.23.1908
51. Mathis J, Hess CW. Sleepiness and vigilance tests. Swiss Med Wkly. 2009;139(15–16):214–219.
52. Scammel T Treatment of narcolepsy in adults - UpToDate. https://www.uptodate.com/contents/treatment-of-narcolepsy-in-adults.
53. Safety | narcolepsy. Available from: http://healthysleep.med.harvard.edu/narcolepsy/living-with-narcolepsy/safety.
54. Garma L, Marchand F. Non-pharmacological approaches to the treatment of narcolepsy. Sleep. 1994;17(suppl_8):97–102. doi:10.1093/sleep/17.suppl_8.S97
55. Mullington J, Broughton R. Scheduled naps in the management of daytime sleepiness in narcolepsy-cataplexy. Sleep. 1993;16(5):444–456. doi:10.1093/sleep/16.5.444
56. Dinges DF, Orne MT, Whitehouse WG, Orne EC. Temporal placement of a nap for alertness: contributions of circadian phase and prior wakefulness. Sleep. 1987;10(4):313–329.
57. Wertz AT, Ronda JM, Czeisler CA, Wright KP. Effects of sleep inertia on cognition. JAMA. 2006;295(2):163–164. doi:10.1001/jama.295.2.163
58. Reyner LA, Horne JA. Suppression of sleepiness in drivers: combination of caffeine with a short nap. Psychophysiology. 1997;34(6):721–725.
59. Guilleminault C, Stoohs R, Clerk A. Daytime somnolence: therapeutic approaches. Neurophysiol Clin. 1993;23(1):23–33. doi:10.1016/S0987-7053(05)80280-1
60. Rogers A, Aldrich M. The effect of regularly scheduled naps on sleep attacks and excessive daytime sleepiness associated with narcolepsy. Nurs Res. 1993;42:111–117. doi:10.1097/00006199-199303000-00009
61. Irwin C, Khalesi S, Desbrow B, McCartney D. Effects of acute caffeine consumption following sleep loss on cognitive, physical, occupational and driving performance: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2020;108:877–888. doi:10.1016/j.neubiorev.2019.12.008
62. Aldosari MS, Olaish AH, Nashwan SZ, Abulmeaty MMA, BaHammam AS. The effects of caffeine on drowsiness in patients with narcolepsy: a double-blind randomized controlled pilot study. Sleep Breath. 2020. doi:10.1007/s11325-020-02065-6
63. Horne R, Reyner LA. Driver sleepiness. J Sleep Res. 1995;4(S2):23–29. doi:10.1111/j.1365-2869.1995.tb00222.x
64. Redelmeier DA, Tibshirani RJ. Association between cellular-telephone calls and motor vehicle collisions. N Engl J Med. 1997;336(7):453–458. doi:10.1056/NEJM199702133360701
65. Kotterba S, Muller N, Stener G, Mayer G. Driving in narcolepsy: analysis by questionnaire among patients. Somnologie. 2002;6:39–50. doi:10.1046/j.1439-054x.2002.02003.x
66. Chakravorty SS, Rye DB. Narcolepsy in the older adult: epidemiology, diagnosis and management. Drugs Aging. 2003;20(5):361–376. doi:10.2165/00002512-200320050-00005
67. Tefft B. Prevalence of Motor Vehicle Crashes Involving Drowsy Drivers, United States, 2009–2013. Washington, DC: AAA Foundation for Traffic Safety; 2015.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.