")
Back to Journals » International Journal of General Medicine » Volume 15
The Weighted Combination of the Epworth Sleepiness Scale and the STOP-Bang Questionnaire Improved the Predictive Value of for OSAHS in Hypertensive Patients
Authors Sun DS, Xu SK, Wang L , Zhang L, Yu HY, Shen JQ
Received 30 January 2022
Accepted for publication 5 August 2022
Published 29 August 2022 Volume 2022:15 Pages 6909—6915
DOI https://doi.org/10.2147/IJGM.S360544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dong-Sheng Sun,1 Shao-kun Xu,1 Lin Wang,1 Li Zhang,1 Hai-Yan Yu,2 Juan-Qin Shen3
1Geriatric Medicine Center, Department of Geriatric Medicine, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China; 2Department of Internal Medicine, Beiyuan District, Yiwu Hospital of Traditional Chinese Medicine, Yiwu, 322000, People’s Republic of China; 3Heart Center, Department of Cardiovascular Medicine, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China
Correspondence: Juan-Qin Shen, Department of Cardiovascular Medicine, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital of Hangzhou Medical College, Hangzhou, 310014, People’s Republic of China, Tel +86 571 87312433, Fax +86 571 87091089, Email [email protected]
Purpose: Hypertension interrelated with obstructive sleep apnea hypopnea syndrome (OSAHS), worsening morbidity and mortality. It is urgent to screening OSAHS from hypertensive patients. An ideal effective questionnaire screening approach for OSAHS is lacking. In this study, we aimed to explore a new OSAHS screening method via weighted combining the current used Epworth sleepiness scale (ESS) and STOP-Bang questionnaire (SBQ) upon calculation.
Patients and Methods: Three hundred and sixteen hypertensive patients with suspicion of the OSAHS were enrolled and randomized in the study into ESS, SBQ and portable respiratory polysomnography (RP) tests. The predictive value of ESS, SBQ and weighted combination were evaluated by calculating the area under curve (AUC), sensitivity and specificity, positive and negative likelihood ratio.
Results: Both the two scales alone and weighted combination were closely related with apnea hypopnea index (AHI), minimum oxygen saturation and average oxygen saturation at night (P < 0.05). The AUC, sensitivity and specificity, positive predictive value (PPV) and negative predictive value (NPV) of ESS in predicting OSAHS were 79.0%, 74.8%, 75.6%, 80.1% and 57.5%, respectively. For SBQ, they were 73.6%, 67.0%, 68.6%, 65.1% and 75.2%, respectively. In contrast, the AUC, sensitivity, and specificity of the combined approach were 82.5%, 73.9% and 82.6%.
Conclusion: The weighted combination of ESS and SBQ could improve the diagnostic ability of OSAHS in patients with hypertension, not only in the accuracy and sensitivity, but also for its easy procedure and accessibility and in hospital. Therefore, the weighted combination approach of ESS and SBQ is promising for OSAHS screening.
Keywords: weighted combination, Epworth sleepiness scale, STOP-bang questionnaire, obstructive sleep apnea hypopnea syndrome
Introduction
Obstructive sleep apnea hypopnea syndrome (OSAHS) caused intermittent hypoxemia and hypercapnia due to the repeated partial or complete upper airway obstruction during sleep and resulted in hypoventilation or apnea,1,2 and OSAHS is closely related with refractory hypertension and high morbidity and mortality.3,4 It is reported that the prevalence in OSAHSA is increasing, affecting at least 25% adults, and it is as high as 49% of the elderly population.5 Furthermore, the number of patients with moderate and/or severe OSAHS has reached 425 million worldwide aged from 30 to 69 years.6 It should be noted that hypertension is closely related with OSAHS.3 30–50% of hypertensive patients have OSAHS and 50–92% of patients with OSAHS are accompanied by hypertension.4 OSAHS and hypertension are risky, let alone they simultaneously occurred. Therefore, it is clinically important to diagnose OSAHS symptom in hypertensive patients.
The gold standard for the diagnosis of OSAHS is Polysomnography (PSG). However, it required specific environment, complicated procedure, time-consuming and long-time appointment in advance in addition to the expensive cost and inconvenient use.7 Increasing researchers are recommending the use of portable respiratory polysomnography (RP) for sleep monitoring. However, it is limited by the 7-h wearing of specific monitor and half an hour to analyze the data. To address this dilemma, questionnaire approaches have been developed for clinical screening of OSAHS, such as the Epworth Sleepiness Scale (ESS), the STOP-Bang Questionnaire (SBQ) and Berlin questionnaire.8,9 They are convenient, easy for data analysis, have acceptable sensitivity, and specificity. Comparison has been performed between these questionnaires, and each of these methods has advantages and deficiencies indeed. Relative satisfied but far from ideal screening abilities were achieved in predicting OSAHS using ESS and SBQ alone.10,11 Gong et al found that although the ESS alone has acceptable clinical predictive value for OSAHS patients with hypertension, but the severity of OSAHS could not be precisely predicted from ESS score.12 Therefore, it is rationale to take the advantages of two or more approaches via combination, and evaluation of the screening ability upon combining these questionnaires is lacking. Considering that the ESS score is mainly based on subjective cognition and the SBQ scores are mainly based on objective index, we develop a screening approach by weighted combining the ESS and SBQ based on calculation and evaluate its predicting values for OSAHS in Chinese hypertensive patients.
Materials and Methods
Subjects
A total of 316 hypertensive patients with suspicion of OSAHS in the hypertension outpatient department of Zhejiang Provincial People’s Hospital and the hypertension prevention and treatment center of Yiwu City were enrolled from October 2018 to September 2020. This study complies with the Declaration of Helsinki and was approved by the ethics committee of Zhejiang Provincial People’s Hospital (2019KY335), and all enrolled participants signed the informed consent form.
The inclusion criteria: (1) met the diagnostic criteria of Chinese guidelines for the management of hypertension, 2018. Patients were taking antihypertensive medicine or those without antihypertensive drugs, but had a systolic blood pressure (SBP) ≥140 mmHg and/or diastolic blood pressure (DBP) ≥90 mmHg (1 mm = 0.133 kpa);6 (2) have autonomous behavioral and cognitive abilities to fill out the questionnaire accurately; (3) meet at least one of the following conditions: a, loud snoring at night, b. nocturnal apnea and choking during sleep, c. daytime lethargy, d. refractory or intractable hypertension, e. obesity.
Exclusion criteria: (1) patients with incomplete questionnaire; (2) patients who refused to portable RP examination, (3) patients with OSAHS who were already treated with ventilator, (4) mainly central or mixed OSAHS, (5) patients with severe organ failure.
Data Collection of Participants
Trained staff collected data including anthropological characteristics (gender, age, etc), anthropometric indexes (height, weight, and blood pressure), other symptoms (sleep quality, snoring during sleep, apnea, suffocating awakening and their severity and duration), conditions of long-term use of sedative-hypnotic (dose and duration if any), and other comorbidities (diabetes, psychiatric disease, and pharyngeal diseases, such as antiadoncus).
Evaluation of the ESS and SBQ
All patients were evaluated with the ESS and SBQ by professionally trained investigators before RP monitoring. Patients rated the degree of drowsiness in 8 states by themselves: sitting reading, watching TV, sitting still in public places (such as in the theatre or during a meeting), not taking a rest in the middle of a long ride (more than 1 hour), sitting talking with people, taking a rest after meals (without drinking), driving and other traffic lights, and resting in the afternoon. The corresponding scores were 0, 1, 2, and 3, respectively, for never, rarely, sometimes, and often. 1–8 points are normal, 9–15 points are narcolepsy, and 16–24 points are excessive narcolepsy. The higher the score of the patient, the higher degree of daytime narcolepsy is.
The SBQ is a two-level yes or no scoring method for 8 questions. The specific questions are as follows: 1. Snoring, whether you snore loudly, louder than your voice, or can be heard outside a closed door? 2. Fatigue, do you often feel tired, tired or sleepy during the day? 3. Observation, has anyone observed that you stop breathing when you sleep? 4. Blood pressure, have you ever been or are you currently suffering from hypertension? 5. BMI, is BMI greater than 30? BMI calculation formula: BMI = weight (kg)/height (m)2 (example: 70 kg/(1.75 m × 1.75 m) = 22.86 kg/m2). 6. Are you older than 50? 7. Neck circumference, is the neck circumference greater than 40 cm? 8. Gender: male? If the answer is “yes”, 1 point will be obtained; otherwise, 0 point will be obtained.
To assure the accuracy of questionnaires, investigators could offer appropriate explanations to patients, but no guidance, and some of the questions could be answered by patients’ family member or cohabitant.
Portable Respiratory Polysomnography (RP) Monitoring
RP monitoring was performed using a portable sleep apnea monitor for at least 7-h consecutive sleep at night (Alice Nightone, Philips, USA). Drugs or food that affect sleep (such as coffee, alcohol, hypnotic, or sedative drugs) were not allowed on the day of test. RP monitoring index included oronasal airflow, ribcage and abdominal movements, electrocardiogram, pulse, blood oxygen saturation, body position, snoring. A thermistor was used for oronasal airflow monitoring, while ribcage and abdominal respiratory movement were recorded with thoracoabdominal belt sensors.
Diagnostic Criteria of OSAHS
Diagnosis of OSAHS was based on medical history, physical sign, and RP monitoring results. OSAHS can also be diagnosed if clinical symptoms occurred, such as nocturnal sleep snoring with apnea, daytime somnolence (ESS score ≥9), narrowed or clogged upper airway, and those who had an apnea-hypopnea index (AHI) ≥5 times/h. For Patients without severe daytime somnolence (ESS score <9, AHI ≥ 10 times/h or AHI ≥5 times/h), but companied with cognitive dysfunction, hypertension, coronary heart disease, cerebrovascular disorder, diabetes mellitus, insomnia as well as one or more of OSAHS comorbidities can also be diagnosed.8
The severity of OSAHS was classified based on the number of AHIs according to the “Guidelines for the diagnosis and treatment of obstructive sleep PSG apnea hypoventilation syndrome”, where 5–15 AHIs/h was regarded mild, 15–30 AHIs/h was considered moderate, and >30 AHIs/h was severe.9
Statistical Analysis
All categorical variables were summarized as frequency (n) and proportions (%), and continuous variables were presented as means ± standard deviations (Mean ± SD). The correlation of ESS score, SBQ and CDF score with AHI, mean oxygen saturation, and minimum oxygen saturation were analysed. Normality tests were performed for continuous variables before analysis. Normal distributed variables were analysed using Pearson correlation, and Spearman correlation analysis for data disobey normal distribution. Logistic regression was used to combine ESS and SBQ for a new co-diagnostic factor (ESS+1.83 stop-bang). The receiver operating characteristics (ROC) curve was plotted and calculated to test the sensitivity, specificity, and area under curve (AUC) of ESS, SBQ and combined approach, and calculate the difference of AUC by Delong test. The optimal cut-off point was selected by calculating the Yordon index, and the positive predictive value (PPV) and negative predictive value (NPV). P < 0.05 was considered statistically significant. SPSS 22.0 for Windows (SPSS Inc., Chicago, IL) was used for statistical analysis.
Results
Clinical Characteristics of Patients
A total of 316 patients were enrolled in this study, with 252 (79.7%) male and 64 (20.3%) female. The average age was 47.1 ± 12.6 years and mean body mass index (BMI) was 27.2 ± 3.4 kg/m2. The mean score of ESS was 6.9 ± 3.7, and 4.7 ± 1.7 for the mean score of SBQ, while the mean score of co-diagnostic factor was 15.4 ± 4.9. Of these, 100 patients (31.6%) had an ESS ≥ 9. In RP, frequencies of mild, moderate, and severe OSAHS were 21.2% (67), 17.1% (54), and 25.3% (80), respectively. The mean and minimum oxygen saturation were 93.4 ± 2.5% and 78.3 ± 9.9%, shown in Table 1.
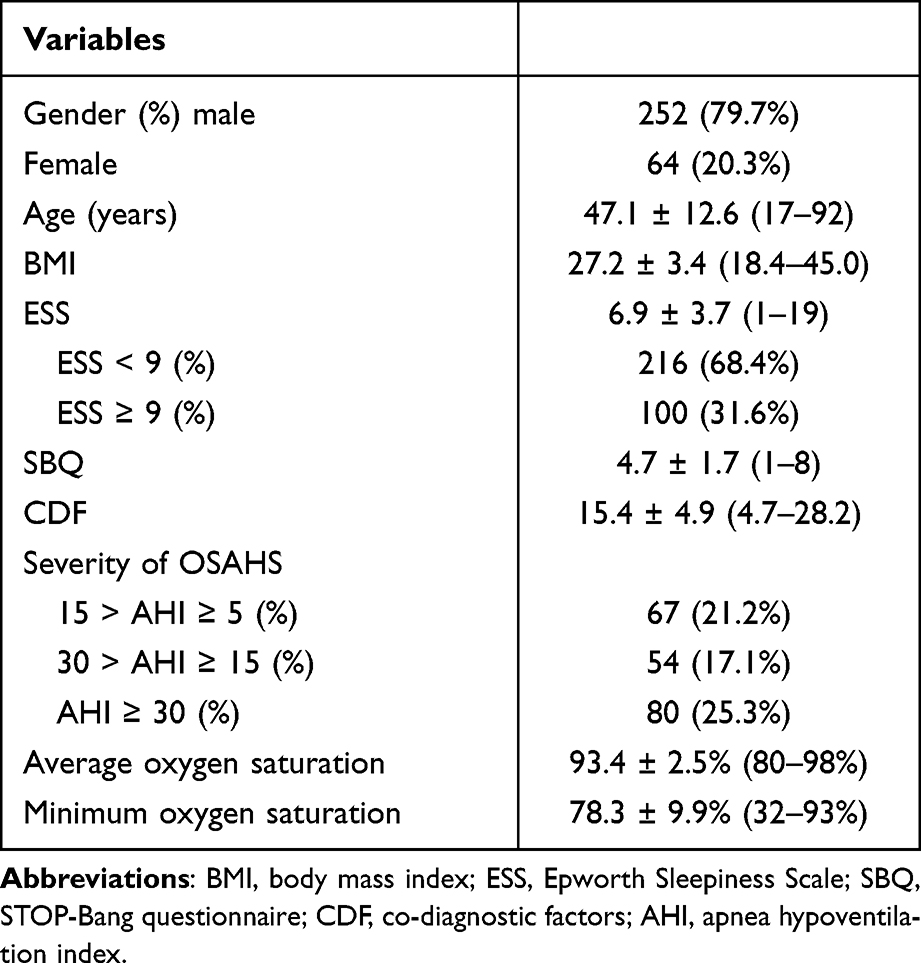 |
Table 1 General Clinical Data Characteristics (n=316) |
Correlation Analysis
After further adjusting for sex, age and body weight, ESS, SBQ and co-diagnostic factor were positively correlated with AHI (B = 0.375, 0.365, 0.440, respectively, all P < 0.0001), and negatively correlated with mean oxygen saturation (B = −0.143, −0.225, −0.202, respectively, all P < 0.05) and minimum oxygen saturation (B = −0.153, −0.256, −0.222, respectively, P < 0.05) (Table 2).
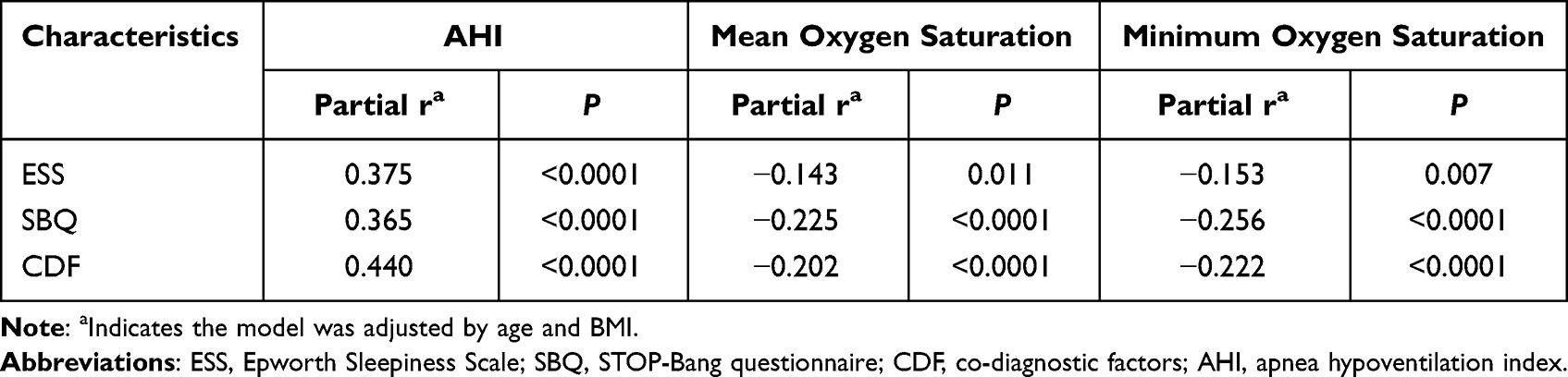 |
Table 2 Correlation of ESS, SBQ and CDF with AHI, Mean Oxygen Saturation, and Minimum Oxygen Saturation (n = 316) |
Evaluation of the Diagnostic Value of ESS, SBQ and Co-Diagnostic Factors for OSAHS
In ESS, the cut-off value, sensitivity, specificity, AUC, PPV, NPV and Youden index for diagnosing OSAHS were 5.5, 74.8%, 75.6%, 79%, 80.1%, 57.5% and 0.5, respectively. In SBQ, those were 4.5, 67.0%, 68.6%, 73.6%, 65.1%, 75.2% and 0.321. The cut-off value, sensitivity, specificity, AUC, and Youden index of the co-diagnostic factor was 14.2, 73.9%, 82.6%, and 82.5% and 0.527, respectively. Notably, the AUC of combined diagnostic factor (CDF, Figure 1) was significantly higher than either ESS (standard error = 0.0135, P < 0.01) or SBQ (standard error = 0.0265, P < 0.01) alone (Table 3). Comparing AUC, SBQ and CDF calculated by Delong test, p = 0.0007; Es compared with CDF, p = 0.009; while p = 0.15 when comparing SBQ and ESS.
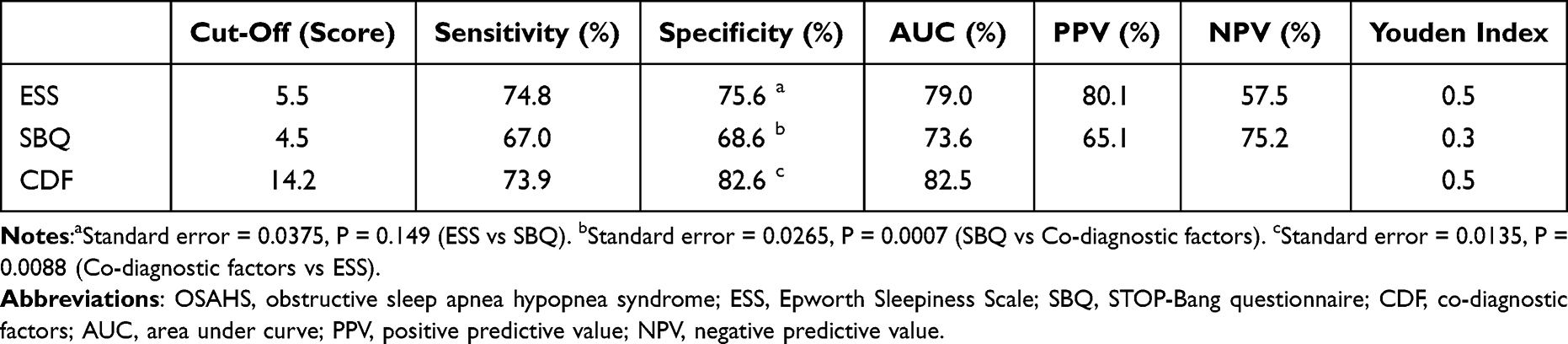 |
Table 3 Predictive Parameters for OSAHS from ESS, SBQ and CDF |
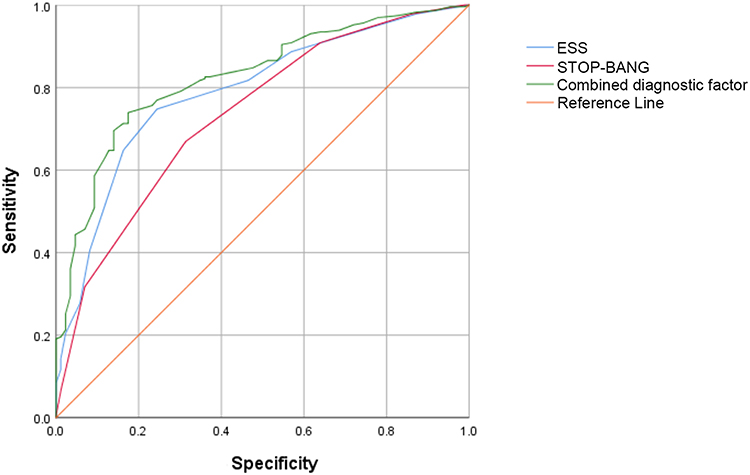 |
Figure 1 Predictive parameters for OSAHS from co-diagnostic factors (ROC curve). |
Discussion
OSAHS has been reported to cause multi-organ, multi-system damage, and induce hypertension, coronary atherosclerotic heart disease, arrhythmia, cerebrovascular disease, cognitive dysfunction, and type 2 diabetes since 1970s.13 It interrelated with hypertension, making the diagnosis and treatment of hypertensive patients worse. Therefore, early diagnosis and treatment of OSAHS among hypertensive patients is urgent. The current used OSAHS screening questionnaires, such as ESS and SBQ, both have merits and drawbacks. We investigated the potential of combining ESS and SBQ for OSAHS screening among hypertensive patients so as to taking the merit of ESS in subjective cognition and the advantage of SBQ in objective index together.
The ESS developed by Johns MW was to evaluate patients with inexplicable daytime lethargy or fatigue, and it is widely used in clinical OSAHS screening.11 Other data from patients, such as BMI, age, neck circumference, and gender should be taken into consideration to improve the accuracy of ESS when screening OSAHS from hypertensive patients. It should be noted that other factors, such as diseases (episodic sleeping sickness and restless legs, the hangover effect of long-term oral sedative-hypnotic drugs), occupational related factors (jobs like health-care workers and drivers in three-shifts style) could induce daytime lethargy or fatigue. All these factors would affect the accuracy of OSAHS screening. In the present study, we obtained a significant higher specificity (75.6%) and lower sensitivity (74.8%) than Wang’s results (sensitivity of 86% and specificity of 48%) in ESS for OSAHS screening, indicating notable variations using ESS alone. However, the sensitivity and specificity could achieve as high as 93% and 86%, respectively, when ESS was combined with oxygen desaturation index,14 suggesting the results of ESS for OSAHS screening could be improved via combining with other factors. In addition, ESS score is a subjective assessment method without clear and uniform scoring criteria, thus significant variations existed and conclusion from certain study could not fit all population.15
STOP-Bang score is based on the STOP questionnaire (SBQ, snoring, fatigue, sleep apnea, hypertension) and supplemented with factors like BMI, age, neck circumference and gender. SBQ had good reliability and validity in screening for OSAHS.15 But, other factors, such as race, may potentially affect the SBQ screening ability for OSAHS. Yu’s screening result from 148 patients with suspected OSAHS using SBQ demonstrated a significantly higher sensitivity (85.6%) than our result in this study (67.0%),16 the variation is probably caused by the larger BMI of patients in the Yu’s study (29.6 ± 3.3) than that of the patients in this study (27.2 ± 3.4). The sensitivity, specificity, and AUC of the SBQ alone in this study was 67.0%, 68.6% and 73.6%, respectively, indicating an unmet need in screening ability when using SBQ alone.
In this study, we found that the specificity and AUC (82.6% and 82.5%) were significantly higher than those from ESS (75.6% and 79.0%) and SBQ alone (68.6% and 73.6%, respectively) after weighted combination of ESS and SBQ. The possible reason is that we emphasize the sensitivity and specificity while taking both subjective and objective factors into consideration in the weighted combination. It is superior to ESS in terms of dependence on patients’ cognition. On the other hand, it makes up for the disadvantage of SBQ’s depending on objective factors. The weighted SBQ can emphasize the importance of objective factors without neglecting subjective factors, which could comprehensively reflect the basic situation of patients.
Limitations
Firstly, this study combined the ESS and SBQ as a new tool for predicting OSAHS, and we found that the sensitivity and AUC were less than ideal. It may be necessary to re-select other indicators from the hypertensive patients to further improve OSAHS screening ability. Secondly, only 2 study centers were included in this study, and the clinical significance of this approach needs to be verified in more centers in the future. Lastly, this study uses RP as a diagnostic tool for OSAHS rather than polysomnography, which may affect our results. Further studies using polysomnography are needed to confirm our findings.
Conclusion
The weighted combination of ESS and SBQ significantly improved the diagnostic ability of OSAHS in patients with hypertension, not only in the accuracy and sensitivity, but also for its easy procedure and accessibility and in hospital. The higher prediction value making the weighted combination approach an easy and promising screening tool in clinical screening OSAHS from hypertensive patients.
Acknowledgments
This work was supported by Zhejiang Province Basic Public Welfare Research Program Project (Grant No. LGF20H020009) and Taizhou Science and Technology Plan Project (No: 22ywb105).
Disclosure
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
1. Qaseem A, Holty JE, Owens DK, et al. Management of obstructive sleep apnea in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2013;159(11):471–483. doi:10.7326/0003-4819-159-11-201312030-00009
2. Worsnop CJ, Naughton MT, Barter CE, et al. The prevalence of obstructive sleep apnea in hypertensives. Am J Respir Crit Care Med. 1998;157(1):111–115. doi:10.1164/ajrccm.157.1.9609063
3. Kario K, Hettrick DA, Prejbisz A, et al. Obstructive sleep apnea-induced neurogenic nocturnal hypertension: a potential role of renal denervation. Hypertension. 2021;77(4):1047–1060. doi:10.1161/HYPERTENSIONAHA.120.16378
4. Li A, Roveda JM, Powers LS, et al. Obstructive sleep apnea predicts 10-year cardiovascular disease related mortality in the Sleep Heart Health Study: a machine learning approach. J Clin Sleep Med. 2022. doi:10.5664/jcsm.9630
5. Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389–1400. doi:10.1001/jama.2020.3514
6. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
7. Gottlieb E, Khlif MS, Bird L, et al. Sleep architectural dysfunction and undiagnosed obstructive sleep apnea after chronic ischemic stroke. Sleep Med. 2021;83:45–53. doi:10.1016/j.sleep.2021.04.011
8. Gong Y, Zhang J. Study on pre-judgment value of Epworth sleepiness scale in hypertension complicating obstructive sleep apnea hypopnea syndrome. J Mod Med Health. 2020;36:
9. Xiong M, Hu W, Dong M, et al. The screening value of ESS, SACS, BQ, and SBQ on obstructive sleep apnea in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:2497–2505. doi:10.2147/COPD.S223354
10. Seguro F, Bard V, Sedkaoui K, et al. Screening obstructive sleep apnea-hypopnea syndrome in hypertensive patients: a comparative study of the efficiency of the Epworth sleepiness scale. BMC Pulm Med. 2018;18(1):173. doi:10.1186/s12890-018-0737-y
11. Pivetta B, Chen L, Nagappa M, et al. Use and performance of the STOP-bang questionnaire for obstructive sleep apnea screening across geographic regions: a systematic review and meta-analysis. JAMA Netw Open. 2021;4(3):e211009. doi:10.1001/jamanetworkopen.2021.1009
12. Wang W, Yuan S, Grange JML, et al. Evaluating the performance of five scoring systems for prescreening obstructive sleep apnea-hypopnea syndrome. Sleep Breath. 2021;25:1685–1692. doi:10.1007/s11325-020-02227-6
13. Zhang X. Guidelines for the diagnosis and treatment of obstructive sleep apnea hypopnea syndrome (2011 revision). Chin J Tuberc Respir Dis. 2012;01:9–12.
14. Wang B, Bai Y, Zhang S, et al. Clinical value of oxygen reduction index combined with ESS score in the diagnosis of obstructive sleep apnea hypopnea syndrome. Guangdong Med J. 2019;40:
15. Wu W, Huang C, Li D, et al. Application of the STOP-bang questionnaire in screening obstructive sleep apnea-hypopnea syndrome. J Wenzhou Medl Univ. 2018;48:257–261.
16. Yu Y, Mei W, Chol RJ. Comparison of Epworth sleepiness scale vs. STOP-bang questionnaire as screening tools for obstructive sleep apnea-hypopnea syndrome. Acta Med Univ Sci Technol Huazhong. 2012;41:465–469.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.