")
Back to Journals » Clinical Ophthalmology » Volume 16
The Value of Preoperative Laboratory Investigations in Healthy Individuals Undergoing Elective Cataract Surgeries
Authors Prapakornkovit V , Rattanasombat K, Ratanasukon M
Received 8 March 2022
Accepted for publication 12 May 2022
Published 25 May 2022 Volume 2022:16 Pages 1605—1612
DOI https://doi.org/10.2147/OPTH.S364532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Virintorn Prapakornkovit, Kanjutha Rattanasombat, Mansing Ratanasukon
Department of Ophthalmology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Correspondence: Mansing Ratanasukon, Department of Ophthalmology, Faculty of Medicine, Prince of Songkla University, 15 Karnjanavanich Road, Hat Yai, Songkhla, 90110, Thailand, Tel +6674451380, Fax +6674451381, Email [email protected]
Purpose: To evaluate the number of patients with abnormal preoperative laboratory test results and determine the benefits of these tests in healthy individuals scheduled for elective cataract surgeries.
Patients and Methods: This study was conducted at Songklanagarind Hospital, Thailand. The data were collected from January 1, 2020, to August 31, 2021. The results of laboratory investigations, consisting of a complete blood count (CBC), including hemoglobin (Hb), hematocrit (Hct), and platelet count; chest X-ray (CXR); electrocardiography (EKG); and anti-human immunodeficiency virus (anti-HIV), were evaluated and analyzed. Additional management actions and rates of postponement or cancellation of surgeries were also evaluated.
Results: In total, 401 participants were enrolled in this study. The rates of abnormal investigation results were 40.2% for EKG, 15.5% for CXR, 12.7% for Hb, 11.7% for Hct, 2.0% for platelet count, and 0.2% for anti-HIV. The preoperative tests that required additional management and postponement/cancellation of surgeries were CXR (5.5% and 1.7%, respectively), EKG (2.5% and 0.5%, respectively), and anti-HIV (0.2% and 0%, respectively). Moreover, age ≥ 60 years was associated with a significantly higher rate of positive preoperative EKG findings (relative risk, 4.64; p = 0.017).
Conclusion: The CBC test was not beneficial as a preoperative laboratory investigation for healthy individuals in any age group who were scheduled for elective cataract surgery. However, EKG, CXR, and anti-HIV test results were valuable. Patients aged ≥ 60 years were at risk of having positive EKG results that could result in cancellation or postponement of surgery.
Keywords: elective cataract surgery, phacoemulsification, pre-operative investigations, electrocardiography
Plain Language Summary
The value of preoperative laboratory investigations in healthy individuals undergoing elective cataract surgeries.
Introduction
Cataract surgery is an ophthalmic surgical procedure practiced worldwide.1 The operation has a low risk of systemic and local complications even though it is usually performed in older adults.2,3 However, most ophthalmologists usually request laboratory investigations prior to surgery, even in healthy patients who have no known systemic conditions.1,3 The purpose of routine investigations is to detect abnormal medical conditions;2,3 however, it is questionable whether these conditions change perioperative management or preclude patients from surgery.
According to a 2019 Cochrane systematic review of preoperative tests for cataract surgeries, these routine tests did not show beneficial surgical outcomes.1,3–6 The investigations also did not reduce the risk of intraoperative and postoperative adverse ocular events.1,3–6 Furthermore, one study revealed that the cost of surgeries was 2.55 times higher when preoperative tests were required.7 These results raised concerns among many ophthalmologists regarding the value or benefit of such preoperative investigations in healthy patients with cataracts.
Currently, routine preoperative investigations of elective cataract surgeries at Songklanagarind Hospital in southern Thailand show very few positive results and have a low impact on whether the surgeries will be conducted or canceled. Our study investigations consisted of a complete blood count (CBC), chest X-ray (CXR), anti-human immunodeficiency virus (anti-HIV), and electrocardiography (EKG). The total cost of these investigations per patient was reported to be approximately US$ 23,8 which adds up to approximately US$ 46,000 for 2000 elective cataract surgeries annually. Therefore, this study was conducted to investigate the incidence and severity of abnormal preoperative laboratory investigation results and the value or benefit of the tests in healthy individuals scheduled for elective cataract surgeries.
Materials and Methods
Study Design
This study was a prospective review of the medical records of patients in Songklanagarind Hospital in southern Thailand from January 1, 2020, to August 19, 2021. Information for this study was obtained by accessing medical records, and no changes were imposed on the routine procedure. Inform consent was waived due to minimal risk, and the study was approved by the Human Research Ethics Committee of Prince of Songkla University. The study protocol followed the tenets of the Declaration of Helsinki. The study has been registered with the Thai Clinical Trials Registry (registration number TCTR20200512004). Patients aged ≥18 years without documented underlying diseases who were scheduled for elective cataract surgeries, including phacoemulsification, extracapsular or intracapsular cataract extraction with or without intraocular lens implantation, or scleral fixation under local or topical anesthesia, were recruited. Patients who were scheduled for emergency cataract removal, namely patients with phacomorphic or phacolytic glaucoma and those who underwent cataract surgery combined with other surgeries, such as trabeculectomy or pars plana vitrectomy, were excluded.
Data Collection
The data collected consisted of demographic data (age, sex, diagnosis, and procedures) and the results and severity of preoperative investigations (CBC, CXR, anti-HIV, and EKG). The results of CBC, anti-HIV, and EKG tests were reviewed and evaluated by ophthalmology residents who were responsible for preoperative laboratory evaluation. The results and further management suggestions for preoperative CXR were taken from the official report and interpreted by radiologists.
The preoperative CBC data included patients’ hemoglobin (Hb), hematocrit (Hct), and platelet count. On this basis, patients were divided into three groups: normal, nonspecific abnormal, and specific abnormal. The results of the normal group were within the standard hospital reference range. The results of the nonspecific abnormal group were between those of the normal group and those of the specific abnormal group; however, the patients in the nonspecific abnormal group did not require additional management. The results of the specific abnormal group met the threshold for blood transfusion guidelines according to the National Institute for Health and Care Excellence (NICE) guidelines;9 therefore, the patients in the specific abnormal group required additional management.
Patients were also divided into the following three groups based on their CXR and EKG results: normal, nonspecific abnormal, and specific abnormal. The normal group had results that were reported as normal or unremarkable. The nonspecific abnormal group had mildly abnormal CXR or EKG reports that did not require any consultation. The specific abnormal group had markedly abnormal CXR or EKG reports that required additional consultation and possible management. The specific abnormal CXR results included reports of tuberculosis (TB) infection, lung mass, lung atelectasis, thyroid mass, aortic aneurysm, and hiatal hernia. The specific EKG results considered abnormal were myocardial infarction, cardiac arrhythmia, bradycardia, prolonged QT, left ventricular hypertrophy, and second-degree atrioventricular block.
The specific abnormal groups of CBC, CXR, and EKG were referred to the internal medicine department for preoperative co-evaluation consultation. The decision to repeat or further investigate the abnormal results was deferred to the consulting internists. The rates and reasons for additional management, surgical postponement, or cancellation were evaluated.
Statistical Analysis
The data were analyzed using the R program version 4.1.0 (The R Group, Vienna, Austria) with EpiCalc software. Continuous demographic data are shown as mean and standard deviation or median and interquartile range. Discrete data, including the number of abnormal tests, number of postponements or cancellations, and number of additional management cases, are shown as frequency and percentage.
Fisher’s exact or Pearson’s chi-squared test was used to analyze the predictive factors associated with abnormal test results, additional management, and cancellation/postponement of the operation. Statistical significance was set at p<0.05.
Results
Demographic Data
In total, 401 patients were included. Table 1 provides an overview of the patient demographics. The mean age was 64.9±12.6 years (range, 19–95), and 51.1% of the participants were male. Phacoemulsification was the most frequently performed procedure (92.8%), whereas only 4.7% of the procedures involved extracapsular cataract extraction.
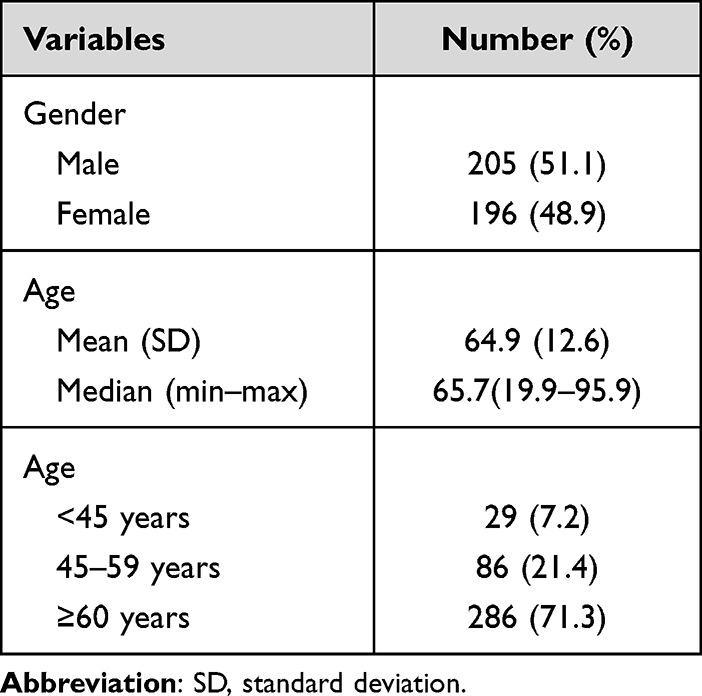 |
Table 1 Patient Demographic Data |
Preoperative Laboratory Results
The CBC test results, including those for Hb, Hct, and platelet count, are shown in Table 2. The mean Hb level in this study was 13.5 g/dL, Hct was 41.0%, and platelet count was 252,000/µL. The overall rates of nonspecific abnormal Hb, Hct, and platelet count were 12.7%, 11.7%, and 2.0%, respectively. None of the patients showed any specific abnormal results.
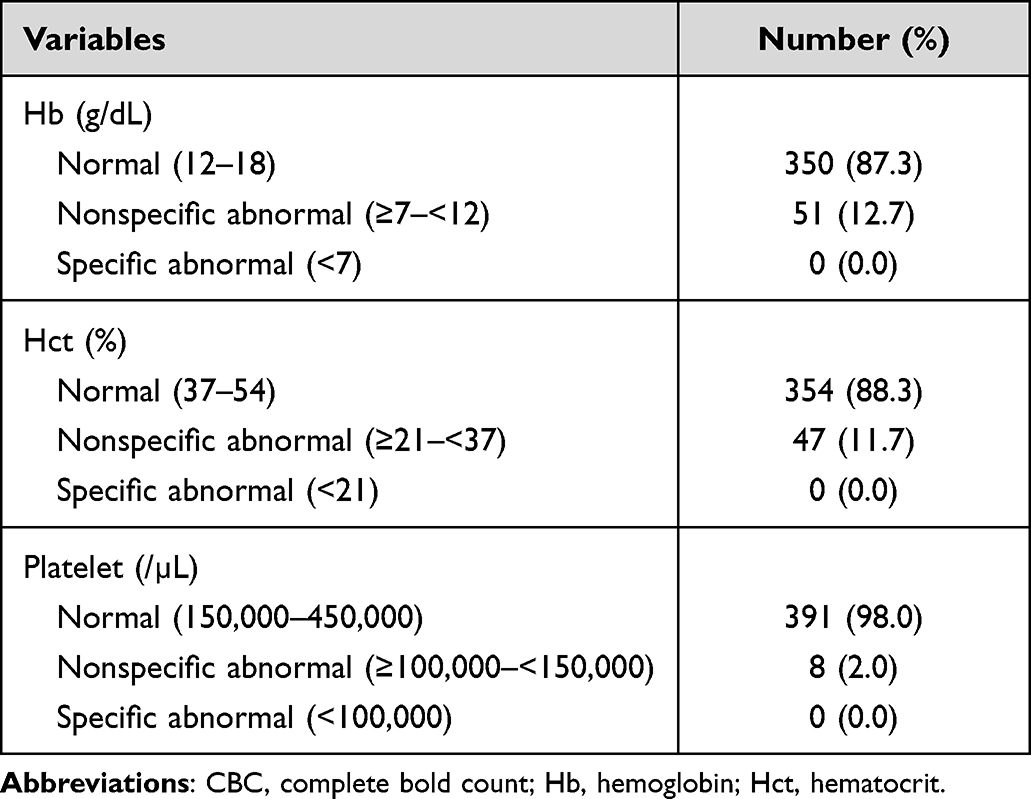 |
Table 2 Results of the CBC Investigations |
The results of anti-HIV, CXR, and EKG tests are shown in Table 3. Abnormal EKG results were the most commonly noted findings. The overall abnormal EKG rate was 40.2%, which included a specific abnormal rate of 7.2%. Abnormal CXR results were the second most common finding, with a rate of 15.5%. The specific abnormal CXR group had a rate of 7.5%, and the results were divided into suspected TB infection (2.5%) and non-TB (5.0%). The lowest abnormal result was that of anti-HIV test for a single patient who had an inconclusive result.
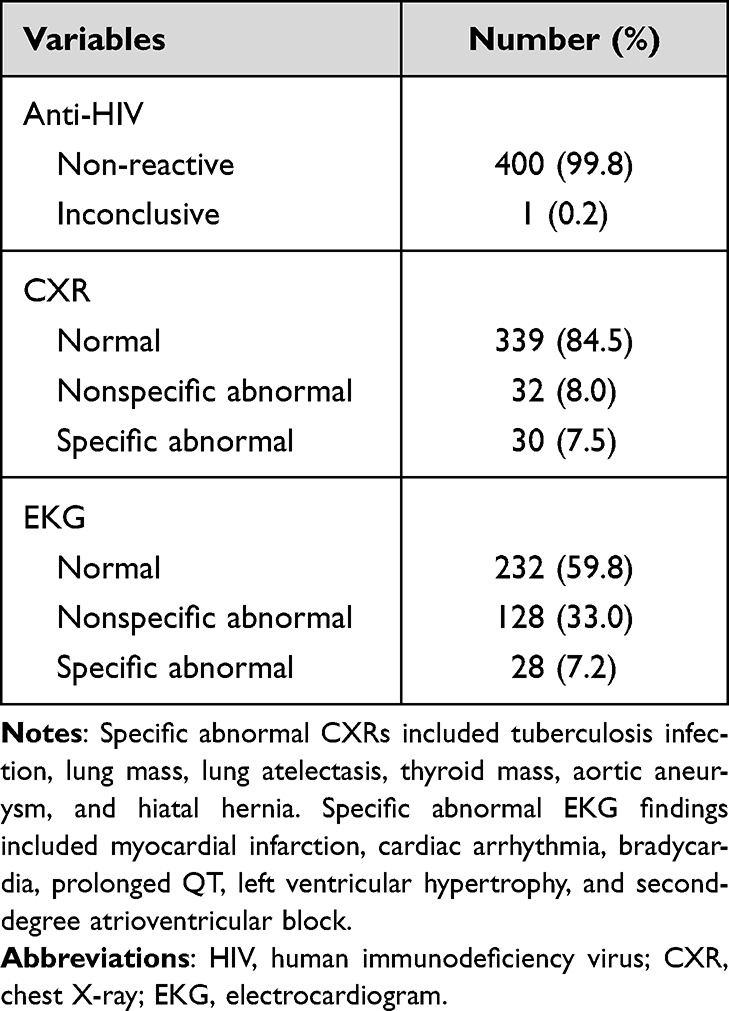 |
Table 3 Results of the Anti-HIV, CXR, and EKG Investigations |
Effects of Preoperative Investigations on the Management of Patients
Our study results indicated that only 33 of 401 (8.2%) patients required additional management. For example, chest computed tomography is required in patients with suspected lung cancer or TB infection based on CXR results. Exercise stress tests were required in patients with suspected myocardial infarction based on the EKG results. The most common preoperative investigation that required additional management was CXR (22 patients, 5.5%), followed by EKG (10 patients, 2.5%) (Figure 1). Only 1 patient required additional management according to the anti-HIV results, leading to the anti-HIV test being repeated. No additional management was required for any patient based on the CBC results.
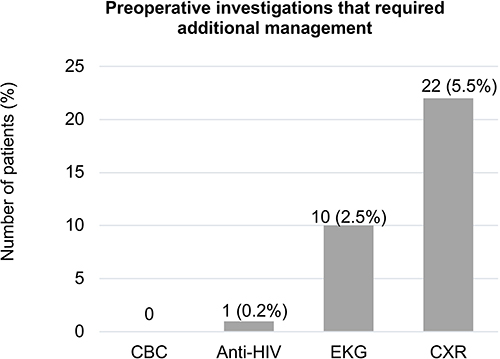 |
Figure 1 Bar graph shows the number of patients who had abnormal preoperative laboratory results that required additional management. |
We followed up on 33 cases (8.2%) that required additional management. Only 9 of 401 patients (2.2%) had surgery that was canceled or postponed because of their abnormal preoperative investigation results (Table 4 and Figure 2). We found that 1.7% of cataract surgeries were rescheduled or canceled due to abnormal CXR results, followed by 0.5% of the cases due to abnormal EKG results. No surgeries were postponed or canceled owing to CBC or anti-HIV results. Moreover, there were other miscellaneous reasons for cancellation or postponement that did not correlate with abnormal preoperative test results, such as the Coronavirus Disease 2019 pandemic and acute illness.
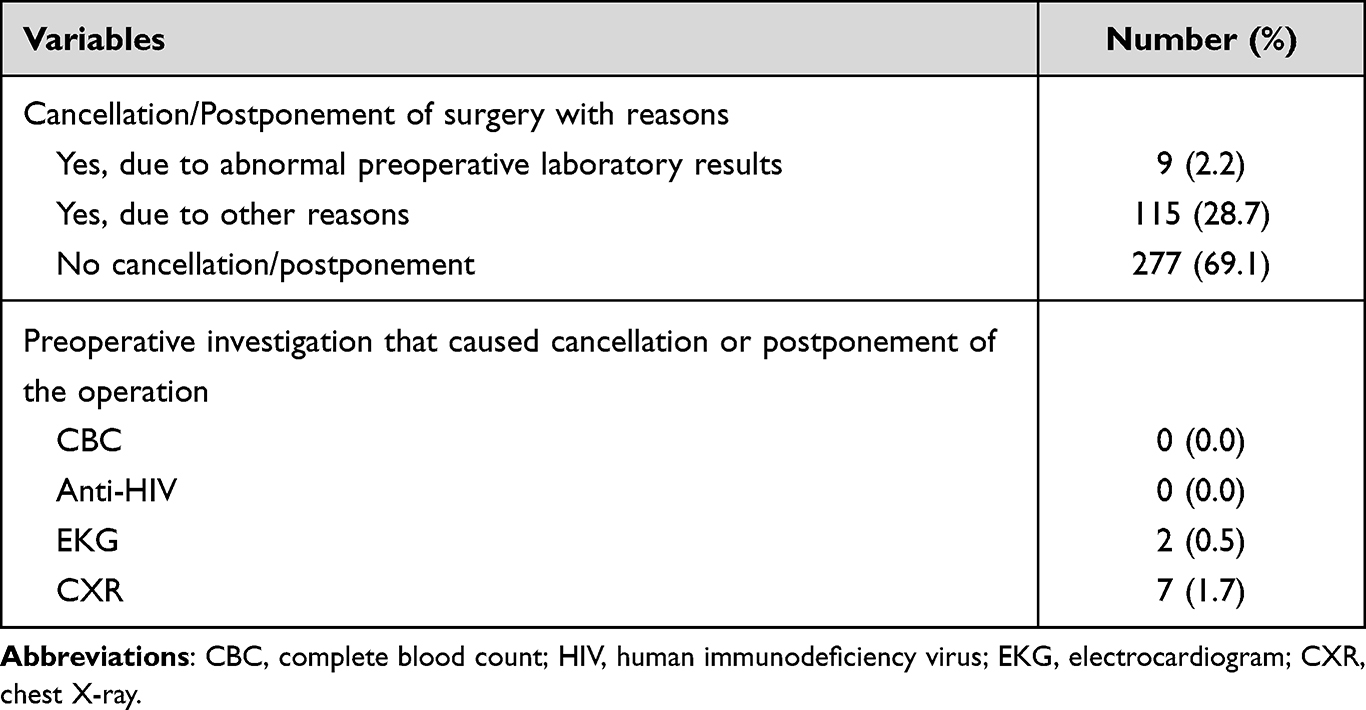 |
Table 4 Cancellation or Postponement of Surgery |
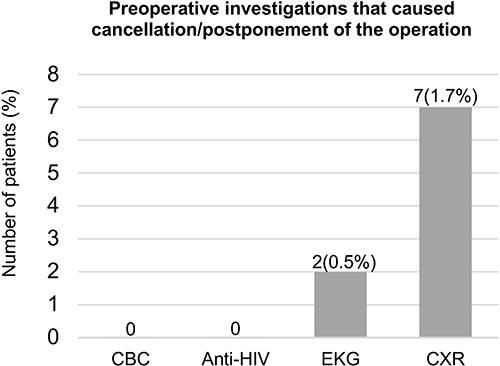 |
Figure 2 Bar graph showing numbers of patients who cancelled/postponed surgery due to the results of the preoperative investigations. |
Risk Factors Associated with Specific Abnormal Preoperative Investigations and Cancellation or Postponement of the Operation
Tables 5 and 6 show the univariate analysis of risk factors associated with specific abnormal preoperative investigations and cancellation or postponement of the operation. The specific abnormal preoperative EKG results were statistically associated with age group; there was a higher prevalence in patients aged ≥60 years (p=0.014) (Table 5), and the relative risk was 4.64 (95% confidence interval, 1.12–19.19; p=0.017). The specific abnormal preoperative CXRs showed no association with sex or age (Table 6).
 |
Table 5 Results of the Univariate Analysis of Risk Factors Associated with Abnormal Preoperative EKG and Cancellation or Postponement of the Operation |
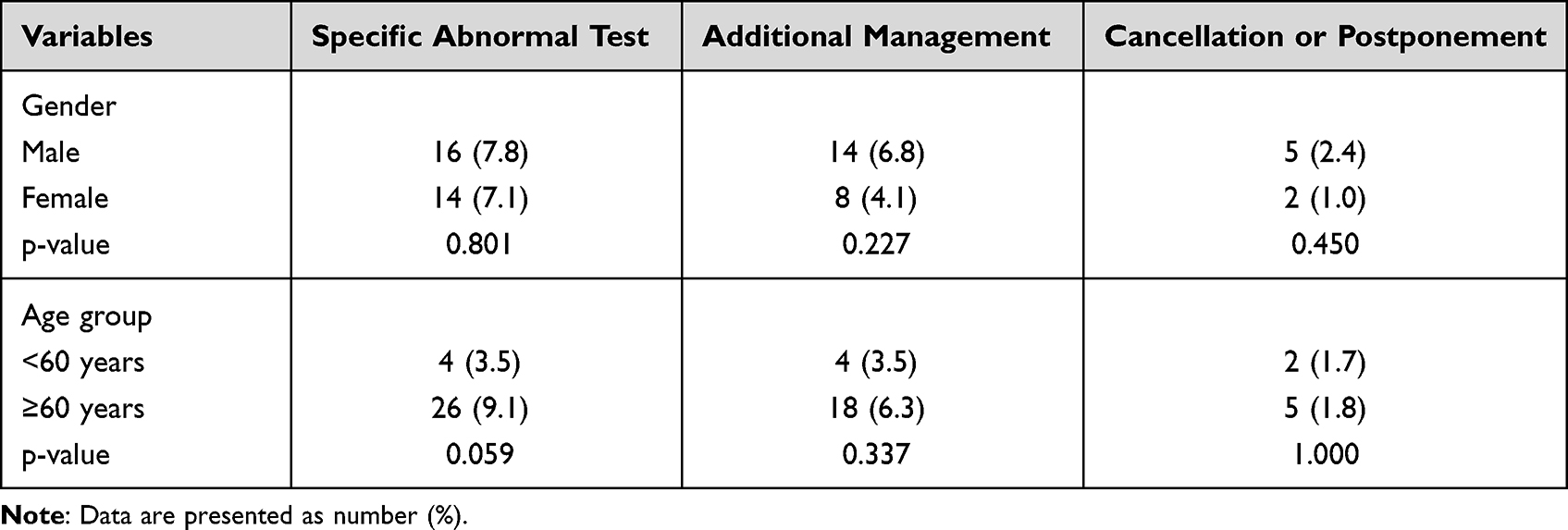 |
Table 6 Results of the Univariate Analysis of Risk Factors Associated with Specific Abnormal Preoperative CXR and Cancellation or Postponement of the Operation |
Discussion
Preoperative medical testing for all types of surgery accounts for approximately US$ 30 billion in health care costs annually.4 Since cataract surgery is commonly performed worldwide, the total cost of routine medical testing before cataract surgery exceeds US$ 150 million annually.4 Copious research has raised questions concerning the value of routine medical testing before elective surgery.4
In 2000, Schein et al4 published a large randomized controlled trial in which 19,557 patients who were scheduled for cataract surgeries did not undergo preoperative testing or usual care. The results revealed no difference in outcomes between the two groups, and abnormal preoperative test results did not predict outcomes. Their conclusion was reinforced by the 2019 Cochrane review.1
In 2007, Shah et al10 evaluated the significance and cost-effectiveness of routine preoperative laboratory investigations in healthy patients who underwent elective ear, nose, and throat surgeries. They found abnormal test results in only 3 of 600 laboratory investigations from a total of 150 patients. Chinachot et al11 also studied the incidence, severity, and factors that led to abnormal preoperative test results among 6280 patients who underwent general anesthesia in Thailand. The study showed that only older adult patients or those with an American Society of Anesthesia score >1 had higher rates of abnormal preoperative investigation results. These two studies seem to demonstrate that laboratory investigations might have no benefit in preoperative evaluations or management of healthy individuals. In 2018, Harder et al12 published a study on the frequency of abnormal findings on routine CXRs before cardiac surgery in 1136 patients. The reported results showed that 50% of the patients had one or more abnormalities on the CXR, 1.3% needed further analysis, and only 0.2% of the CXR led to postponement of surgery, whereas the surgery was not canceled in any of the patients.
To our knowledge, our study is the first in Thailand to evaluate the benefits of preoperative investigations in healthy patients scheduled to undergo cataract surgery under routine local or topical anesthesia. The CBC results from our study showed that the overall rates of abnormal Hb, Hct, and platelet count were 12.7%, 11.7%, and 2.0%, respectively. However, interestingly, none of the patients met the criteria for blood transfusion according to the NICE guidelines;9 therefore, none of the patients required additional management owing to the results of the CBC. This study had a much lower rate of abnormal CBC compared to that in a study by Chinachot et al,11 which reported rates of 38.5% and 45% for abnormal Hb and Hct levels, respectively. The most likely reason is that our study only included healthy individuals who had no underlying systemic disease, which led to a lower rate of abnormal CBC. The overall abnormality rate of EKG was 40.2%, which was much higher than that reported in the previous study.11 The rate of specific abnormalities in the EKG group was 7.2%. That result was associated with the group of patients aged ≥60 years, which was comparable with the results of a previous study.11 Two patients had surgical postponement or had the surgery canceled due to the preoperative EKG results. The overall abnormal CXR rate was 15.5%. This was in accordance with the 15.7% reported by Chinachot et al11 but was much lower than the 50% reported by Harder et al.12 The rate of specific abnormalities in the CXR group was 7.5%, with 5.5% requiring further analysis, and 7 patients (1.7%) either postponed or canceled the surgery. Ten patients (2.5%) were suspected of having TB infection on CXRs. Therefore, a preoperative CXR investigation is justified, especially since TB is endemic in Thailand and easily spreads to other patients and medical personnel. The lowest abnormal result was that of anti-HIV in 1 patient who had an inconclusive result that led to further analysis, but there was no postponement or cancellation of surgery due to the positive result of the anti-HIV investigation.
The results of the study support the hypothesis that some preoperative tests, such as CBC, are not very informative for clinical preoperative evaluations. However, some investigations have benefited from other factors. An anti-HIV test is still necessary in terms of hospital policy. The test is intended as a universal precaution for all medical staff and operating theaters. Moreover, because of the high incidence of TB infections in the country, CXR is essential for evaluating and controlling its spread. The EKG test also has the benefit of detecting heart disease before anesthesia in older adult patients. For these reasons, although our report shows a low incidence of abnormal specific preoperative tests, these three preoperative investigations (CXR, EKG, and anti-HIV) need to be performed.
Some major limitations of this study include (1) the relatively small number of patients, (2) the COVID-19 pandemic that caused a substantial reduction in the study population, and (3) operations under general anesthesia were not included. However, to the best of our knowledge, this is the first study in Thailand to investigate the rates and severity of abnormal preoperative laboratory investigation results in healthy patients scheduled for elective cataract surgeries. This study used routine clinical care at a tertiary care hospital; therefore, the results may be generalized to other types of ophthalmic surgical procedures such as pterygium excision, benign mass excision, and strabismus surgery. In the future, if CBC is no longer included in routine preoperative investigations for healthy patients undergoing cataract surgery, the cost of preoperative investigations in the hospital can be lower by US$ 1700 each year.
Conclusion
Our study found that the CBC test was not beneficial in preoperative laboratory investigations in any age group of healthy patients who underwent elective cataract surgery. However, EKG, CXR, and anti-HIV tests are valuable. Patients aged ≥ 60 years had a small risk of having positive EKG results that could result in cancellation or postponement of surgery.
Data Sharing Statement
The data that support the findings of this study are available on request from the author, KR ([email protected]). The data are not publicly available due to the privacy of research participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Keay L, Lindsley K, Tielsch J, Katz J, Schein O. Routine preoperative medical testing for cataract surgery. Cochrane Database Syst Rev. 2019;1:CD007293. doi:10.1002/14651858.CD007293.pub4
2. Fleisher LA, Fleischmann KE, Auerbach AD, et al. ACC/AHA. Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Developed in Collaboration with the American College of Surgeons; 2014, American Society of Anesthesiologists, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Anesthesiologists, and Society of Vascular Medicine Endorsed by the Society of Hospital Medicine. J Nucl Cardiol. 2015;22(1):162–215. doi:10.1007/s12350-014-0025-z
3. Routine preoperative laboratory testing for patients scheduled for cataract surgery. American Academy of Ophthalmology; 2014. Available from: https://www.aao.org/clinical-statement/routine-preoperative-laboratory-testing-patients-s.
4. Schein OD, Katz J, Bass EB, et al. The value of routine preoperative medical testing before cataract surgery. Study of medical Testing for cataract Surgery. N Engl J Med. 2000;342(3):168–175. doi:10.1056/NEJM200001203420304
5. Lira RP, Nascimento MA, Moreira-Filho DC, Kara-José N, Arieta CE. Are routine preoperative medical tests needed with cataract surgery? Rev Panam Salud Publica. 2001;10(1):13–17. doi:10.1590/s1020-49892001000700003
6. Cavallini GM, Saccarola P, D’Amico R, Gasparin A, Campi L. Impact of preoperative testing on ophthalmologic and systemic outcomes in cataract surgery. Eur J Ophthalmol. 2004;14(5):369–374. doi:10.1177/112067210401400502
7. Arieta CEL, Nascimento MA, Lira RPC, Kara-José N. [Waste of medical tests in preoperative evaluation for cataract surgery]. Cad Saude Publica. 2004;20(1):303–310. Danish. doi:10.1590/s0102-311x2004000100048
8. Songklanagarind hospital. Health check-up package [Internet]; 2019. Available from: https://hospital.psu.ac.th/2ServiceCure_Check.php.
9. National Institute for Health, Excellent C. Blood transfusion guideline [NICE guideline:24]; 2015.
10. Shah SA, Sajid T, Asif M, Khan F, Ghani R. Significance and cost effectiveness of pre-operative routine laboratory investigations in young healthy patients undergoing elective ear, nose and throat surgery. J Ayub Med Coll Abbottabad. 2007;19(2):3–6.
11. Chinachot T, Turasakul P, Wachjanawach C, Sooksri N. Incidence, severity and factors lead to abnormal pre-operative blood chemistry, CBC, chest X-ray and EKG in routine preoperative investigation. Thai J Anaesthesiol. 2016;42:69–87.
12. den Harder AM, de Heer LM, de Jong PA, Suyker WJ, Leiner T, Budde RPJ. Frequency of abnormal findings on routine chest radiography before cardiac surgery. J Thorac Cardiovasc Surg. 2018;155(5):2035–2040. doi:10.1016/j.jtcvs.2017.12.124
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.