")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Validity of Virtual Courage for Trainees in High-Risk Occupations
Authors Wang J, Wang H, Jiang J, Cheng X, Xu K, Xia F, Chang L, Ji Y, Feng Z
Received 1 May 2022
Accepted for publication 30 June 2022
Published 14 July 2022 Volume 2022:15 Pages 1783—1796
DOI https://doi.org/10.2147/PRBM.S371653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jia Wang,1 Huizhong Wang,2 Juan Jiang,2 Xiaotong Cheng,3 Ke Xu,4 Fan Xia,2 Le Chang,2 Yede Ji,5 Zhengzhi Feng1
1Department of Developmental Psychology of Armyman, School of Psychology, Army Medical University, Chongqing, People’s Republic of China; 2School of Psychology, Army Medical University, Chongqing, People’s Republic of China; 3Unit 32298 of the Chinese People’s Liberation Army, Weifang, People’s Republic of China; 4Shigatse Branch, Xinqiao Hospital, Army 953 Hospital, Army Medical University, Shigatse, People’s Republic of China; 5Army Engineering University, Xuzhou, People’s Republic of China
Correspondence: Zhengzhi Feng, Developmental Psychology for Armyman, Department of Medical Psychology, Army Medical University, No. 30, Gaotanyan Street, Shapingba District, Chongqing, 400038, People’s Republic of China, Email [email protected]
Background: Employees in high-risk occupations are exposed to tremendous work stress that hinders organizational effectiveness and personal mental health. Based on positive psychology, courage can be considered a protective factor that buffers the adverse effect of high-risk surroundings on employees. However, little is known about the way courage is simulated or evaluated in response to safety concerns. Virtual reality (VR) is an accessible tool for courage simulation due to its immersive qualities, presence and interactive features and may provide a promising pathway to achieve a scientific, accurate and ecologically valid evaluation of high-risk employees.
Methods: The sample consisted of 51 high-risk employees who were recruited voluntarily. Before and after experiencing the VR courage scenarios, the participants completed the VR features questionnaire, the Physical Courage at Work Scale (PCWS), the Courage Measure (CM), and the Positive and Negative Affect Scale (PANAS). During the process of watching the VR courage scenarios, the participants’ heart rate and skin conductance at resting-state baseline and during virtual courage scenarios were recorded through HTC VIVE Pro Eye and BioGraph Infiniti 8.
Results: The results support the hypothesis and reveal that the interaction, immersion and presence scores of the scenarios were all significantly higher than the median 4 points. The score for the CM in the posttest was significantly higher than that in the pretest. The scared and afraid scores for the posttest were significantly higher than those for the pretest. The heart rate and skin conductance of each scenario showed an increase compared with the baseline. The Pearson’s correlation between physiological indicators and the score of the PCWS was 0.28∼ 0.54.
Conclusion: This study developed virtual courage for high-risk occupations based on well-established theory and VR technology. Experimental data revealed that the paradigm conformed to the requirements of VR features and was able to activate fear and evoke the quality of courage. Thus, the virtual courage paradigms have good validity in simulating scenarios for high-risk employees, which might accelerate organizational effectiveness while buffering working stress.
Keywords: high-risk occupations, employees, courage, virtual reality
Introduction
High-risk occupations (eg, firefighters, soldiers, policemen, paramedics, blue-collar workers, miners) have rates of nonfatal injuries and illness that are more than double the rate per 10,000 national full-time workers in addition to the risk of trauma or physical threat because employees are often exposed to injury or death during their daily work.1–5 For instance, soldiers face as many as 15 combat threats, such as “attacked or ambushed” and “received incoming fire”.6 For firefighters and paramedics, researchers have used principal component analysis methods from 33 incident stressors and identified 5 components: catastrophic injury to oneself or a coworker, gruesome victim incidents, rendering aid to seriously injured/vulnerable victims, minor injury to the self, and exposure to death and dying.7 From the perspective of cognitive neuroscience, when human beings encounter threats, they engage in defensive behaviors. These freeze, flight and avoidance behaviors can enhance people’s chances of survival in life-endangering situations.8 That is, defensive behaviors, as evolutionarily adaptive responses, can help people avoid potential danger.9 However, in dangerous occupations, employees must endure risks to accomplish their duties or mission. These risks may undermine employees’ subsequent health by producing physical, psychological and behavioral dysfunction and may hinder organizational efficiency and productivity. Andersen (2019) investigated 2678 employees who were exposed to work-related violence and threats and found that 13.9% of employees reported short-term PTSD and 17.9% reported long-term PTSD.10 The COVID-19 pandemic, which has been perceived as a traumatic stressor for physical, emotional and cognitive threats, has had detrimental mental health impacts on frontline paramedics.11,12 A systematic review reported that in a sample of 22,380 frontline healthcare workers, the prevalence rates of depression, anxiety and stress were 24.3%, 25.8%, and 45%, respectively.13 Additionally, people in risky workplaces experience an increased risk of mental health sequelae, which in turn predict subsequent deterioration in job satisfaction, involvement and organizational commitment and may lead to a decline in work-related and organizational effectiveness.14 Consequently, the paradox between performing obligatory hazardous duties and instinctively defensive behaviors remains. A predisposition to courage might provide enough inner strength to perform the appropriate behaviors in high-risk circumstances.3
Courage is an ancient virtue, and recent investigations into implicit theories as well as related experimental studies of courage have introduced an empirical approach to studying the topic.15 From the perspective of positive psychology, courage is considered a character strength.16 Rate et al systematically reviewed the 29 definitions in existing studies of courage and identified four necessary components of implicit theories of courage: risk, perceived fear, intentionality/deliberation and noble/good act.15 Additionally, Norton noted that courage should be defined as a behavioral approach despite the experience of fear, which can be considered a state of courage when facing a risk that can evoke fear.17 Howard expanded courage into a specific realm, physical courage, and suggested that under the threat of physical health, individuals take actions to complete their duties, responsibilities, and organizational goals to save others from casualty despite the risk of harm to the individual’s physical health.3 Based on various theoretical hypotheses, a number of studies have proven that courage can promote individuals’ well-being and organizational efficiency in certain dangerous occupations. For example, Howard et al’s study enrolled 368 United States Air Force Academy cadets and showed that when accounting for irrelevant variables, physical courage was significantly related to military performance. In addition, Rachman’s research clearly showed that among bomb-disposal operators, parachutists and veterans, a higher level of courage led to a better level of mental and physical well-being and operational performance.18 In addition, positive psychologists have linked courage to well-being and life satisfaction and the alleviation of depression and distress.19 Therefore, it is essential to enhance the predisposition to courage, which can promote and accelerate organizational effectiveness and individual well-being for employees in high-risk workplaces. Nonetheless, traditional studies have mainly focused on psychological intervention and emphasized the pathological angle.2 These studies lack ecological validity to potentially simulate high-risk operating environments.20 The main components of courage are risk, perceived fear, intentionality/deliberation, and noble/good act; thus, the core elevating strategy was to establish a risky workplace in which subjective fear was activated and then provide a choice of whether to fulfil a noble/good duty or give up. However, for high-risk surroundings, a trade off exists between the perfect training effect and safety concerns. With the development of new virtual reality (VR) technology, this puzzle awaits a promising solution.
VR is an accessible approach for courage simulation due to its immersive presence and interaction features. It is a computer simulation technology that can interact with users in the “real” environment (vision, hearing, smell, etc.) through computer-generated 3-dimensional stimulation.21 Immersion is the degree of physical stimulation to the sensory systems and the sensitivity of the system to motor inputs, which involves the objective input of a physical stimulus. Its level mainly represents the physical attributes of the input stimulus.21 The psychological product of technological immersion is presence, namely, the psychological sensation of being in the virtual environment instead of the physical environment. Presence allows users to react to stimuli even if they consciously know they are in a nonreal-world environment, and the brain response is similar to that in the real environment.22 A previous study showed that there were no significant differences in pride, joy, awe, disgust, fear, or sadness between virtual situations and real situations, since different emotion-induced patterns are highly correlated with presence in virtual environments.23 Finally, interaction reflects the process by which users interact with the virtual environment through external devices by using highly sensitive headsets and spatial positioning and tracking systems. The user is set as the reference frame from the first-person perspective. By tracking the user’s head and body movement, the sensor sends the monitored user position parameters to the computer to realize the interaction between the user subject and the virtual environment. Furthermore, users can interact with specific tasks in the virtual environment through external handles, rifles and other controllers to realize the specific operation steps of psychological training.24 Virtual environments provide an interface that allows employees to be immersed within controlled stimuli (visual, auditory, motor and haptic conditions) in which the contexts are relevant to the real world; they affect individuals’ nervous systems and facilitate new possibilities for behavioral and emotional modification with the same effectiveness as real stimuli.22,24 Furthermore, a systematic review indicated that stress management training can significantly inhibit the sympathetic nerve activity of soldiers under virtual battlefield conditions and activate parasympathetic nerve activity through training of relaxation techniques and reappraisal strategies.25 There is increasing evidence that VR technology is effective in psychological training for management, such as emotion regulation,26 resilience27 and stress.25 Regarding courage, related research has noted that psychological and physiological indicators can be evaluated on the bravery spectrum. Norton and Howard suggested that reliable and valid psychological questionnaires, the Courage Measure questionnaire17 and Physical Courage at Work Scale3 can assess individuals’ levels of courage based on their theoretical hypothesis. In addition, fear and intentionality/deliberation are prominent subordinate components of courage. Therefore, subjective fear ratings and the decision to continue or retreat are behavioral indicators of courage that emphasize fear ratings18,28 and choices29–31 when people encounter risk situations that might be detrimental to their physical fitness. On the one hand, fear is an adaptive emotion that allows human beings to remain alert to danger; nevertheless, overwhelming terror is thought to have maladaptive functions in terms of both cognitive and behavioral responses.28 According to studies of soldiers, the more valorous military personnel are, the greater they endure adverse fear32 and know how to control or recover from this fear.18 On the other hand, courageous people experience less behavioral avoidance; for example, individuals with greater courage move closer to spiders.17 Similarly, physiological indicators mainly focus on variations in specific brain regions, skin conductance, and heart rate. Nili et al noted that the mechanisms of courage in daily life are associated with activity in the subgenual anterior cingulate cortex (sgACC) and inhibit the amygdala,33 which is implicated in processing fear and retreat and plays a role through the generation of autonomic responses to attenuate skin conductance and heart rate.28,33 That is, simulating high-risk workplaces using VR technology may adequately represent a risky workplace by activating employees’ fears and strengthening their courage, leading them to overcome or endure fear to achieve a duty or noble goal unless they give up when accompanied by the monitoring of psychological, behavioral and physical indicators of the training effect.
Taken together, employees in high-risk occupations can be exposed to overwhelming stress level, which deteriorates mental health and hinders simultaneous organizational effectiveness. Those in high level of courage would be more likely to cope the detrimental effect by the intention of effective acting under conditions of fear towards the noble goals in high-risk surroundings. Therefore, it is essential to improve and implement courage. However, since safety concerns limit the authenticity and intensity of training effect, VR technology could simulate the high-risk environment by playing an illuminating tool.
Thus, to prevent psychosocial dysfunction and organizational ineffectiveness among employees who have been exposed to traumatic events in high-risk settings, a possible protective approach related to courage simulation needs to be identified. Although many studies have focused on psychological skill maintenance,2,34 few have directly focused on courage paradigms. Considering the above, VR courage paradigms are needed so that people in high-risk occupations can avoid injuries from the real world while strengthening their inner courage despite overwhelming traumatic stress and organizational ineffectiveness. Accordingly, the VR courage scenario will induce a sense of fear in high-risk employees’ in an attempt to evoke their physiological responses and subjective feedback. Our hypothesis is that virtual courage paradigms using VR are statistically reliable and valid for high-risk employees.
Methods
Participants
The participants included 51 high-risk employees who were recruited voluntarily and anonymously (gender: 10 female, 41 male; age±SD:18.43±1.93, range 18–29). We chose our participants from among firefighters due to their high-risk professional properties,35,36 such as rescuing individuals during disaster37 and providing emergency medical service.38 The inclusion criteria were as follows: 18 years old or older, right-handed, no history of mental or psychiatric illness, visual acuity or corrected visual acuity of 1.0 or above, normal hearing, willingness to participate in the study, and signing the informed consent form. The exclusion criteria were participating in another experimental study within the past 3 months and 3D motion sickness that made the individual unable to cooperate with the experiment. The study was approved by the ethics committee of Army Medical University and complies with the Declaration of Helsinki (No. 2020-024-03). The participants provided written informed consent before completing the questionnaires and experiments.
Dependent Variables
VR Measurement
To measure immersion, we used a Game Engagement Questionnaire39 by McMahan. Similarly, to measure perceptions of presence, we administered the Slater-Usoh-Steed Presence Questionnaire.40 Interaction was assessed with the Perceived Behavioral Control and Perceived Ease-Of-Use subscale from Chang’s study.41,42 Twenty-five items were used with a 7-point Likert scale. In the current sample, the Cronbach’s α coefficients of the subscales were above 0.80, 0.83, and 0.81, indicating good reliability.
Courage Measurement
Courage was assessed with two questionnaires: the Physical Courage at Work Scale (PCWS)3 and the Courage Measure (CM).17 The PCWS focuses on physical courage, emphasizing a courageous predisposition in which the risks involved might affect employees’ physical well-being.43,44 The PCWS consists of 30 items rated from 1 (minor agreement) to 7 (severe agreement) and five factors including immediate danger, providing for family, others’ aggression, reporting violations and helping society (Appendices). The model fit indices were above the acceptable thresholds. In the fit indices, minimum fit function chi-square/degrees of freedom (CMIN/DF) was 2.54<5, the comparative fit index (CFI) was 0.95>0.90, the Tucker-Lewis index (TLI) was 0.93>0.90, the standardized root mean square residual (SRMR) was 0.07<0.08, and the root mean square error of approximation (RMSEA) was 0.07<0.08. In the Chinese version of the PCWS,45 confirmatory factor analysis indicated that there were five factors involved, similar to the original version, and the model fit indices were above the acceptable thresholds (CMIN/DF=4.60, CFI=0.95, TLI=0.94, SRMR=0.05, RMSEA=0.07). In the present study, Cronbach’s α coefficient was 0.92 overall, and for each factor, it was 0.90, 0.78, 0.85, 0.74, and 0.77 respectively, indicating that reliability and validity were good.
The CM was developed by Norton et al and provides an operational definition of courage as persistence or perseverance despite experiencing fear in high-risk situations. The scale consists of 12 items, rated from 1 (never) to 7 (always) (Appendices). The Cronbach’s α coefficient was 0.92, and the test-retest correlation at three weeks was 0.66 (p<0.001). The majority of researchers agree with this measurement of the CM.46–49 In the present study, Cronbach’s α coefficient was 0.72, and the model fit indices were above the acceptable thresholds (CMIN/DF=1.15, CFI=0.98, TLI=0.97, SRMR=0.07, RMSEA=0.05), indicating that reliability and validity were good.
Emotional and Behavioral Indicators
Fear was assessed with the Positive and Negative Affect Scale (PANAS). The ratings ranged from 1 (no fear) to 5 (severe fear) in the virtual courage scenario. The PANAS consists of 20 items rated from 1 (very slightly) to 5 (very much); half measure positive emotion and the other half gauge negative emotion50 (Appendices). In this study, two items, scared and afraid, were used to evaluate fear pre- and postexperiment. In the present study, Cronbach’s α coefficients were 0.76 and 0.78, indicating good reliability.
The choice of courageous action was assessed with questions within the virtual courage scenarios, such as “You may be physically threatened or even hurt; do you continue or give up?” The participants chose yes or no on a virtual gamepad to interact with the virtual courage scenarios. The frequency of courageous action was automatically recorded by the virtual courage software.
Physiological Indicators
Skin conductance and heart rate were recorded by BioGraph Infiniti.51 The laboratory temperature was controlled at 25~28 °C, and the participants’ fingers were wiped with alcohol swabs to ensure the stability of skin conductance. In the experiment, two Ag/AgCl electrodes were wrapped around the middle finger and ring finger of the left hand with a 120 Hz sampling rate. The heart rate collection point was the first finger.
The data was inspected for movement artifacts by removing the data with extreme values greater than two standard deviations. We did not transformed the data before analysis since we use non-parametric test to assess and analyze the physiological data.
Virtual Courage Scenarios
From our previous investigations, the top five risk scenarios were earthquake rescue (completing the parachute jump mission), anti-terrorist operation rescue, earthquake rescue (completing a transfer mission), medical rescue, and traffic accident rescue (Table 1). Based on the main components of courage, that is, risk, fear, intentionality/deliberation, and noble/good act,15 each scenario was developed with varying levels of four dimensions (Table 2). Risk occurs in events that may threaten individuals’ lives or cause physical damage. Earthquakes, terrorist attacks, viral infections, and car accidents were extracted.53 Additionally, fear factors were drawn from fear survey schedule III, which includes frequently encountered fear stimuli (the scale includes 76 items and 6 categories). In the virtual courage scenario, fear of heights, explosions, corpses, viruses and blood were extracted.54,55 Intentionality/deliberation is generally linked with the decision-making process to determine whether courageous behavior occurs.55,56 In each scenario, the subjects made decisions and were asked, “You may be physically threatened or even hurt; do you continue or give up?” Finally, selfless sacrifices for external noble motivation and prosocial or social-oriented acts were involved in the component of noble/good acts.15,57–59
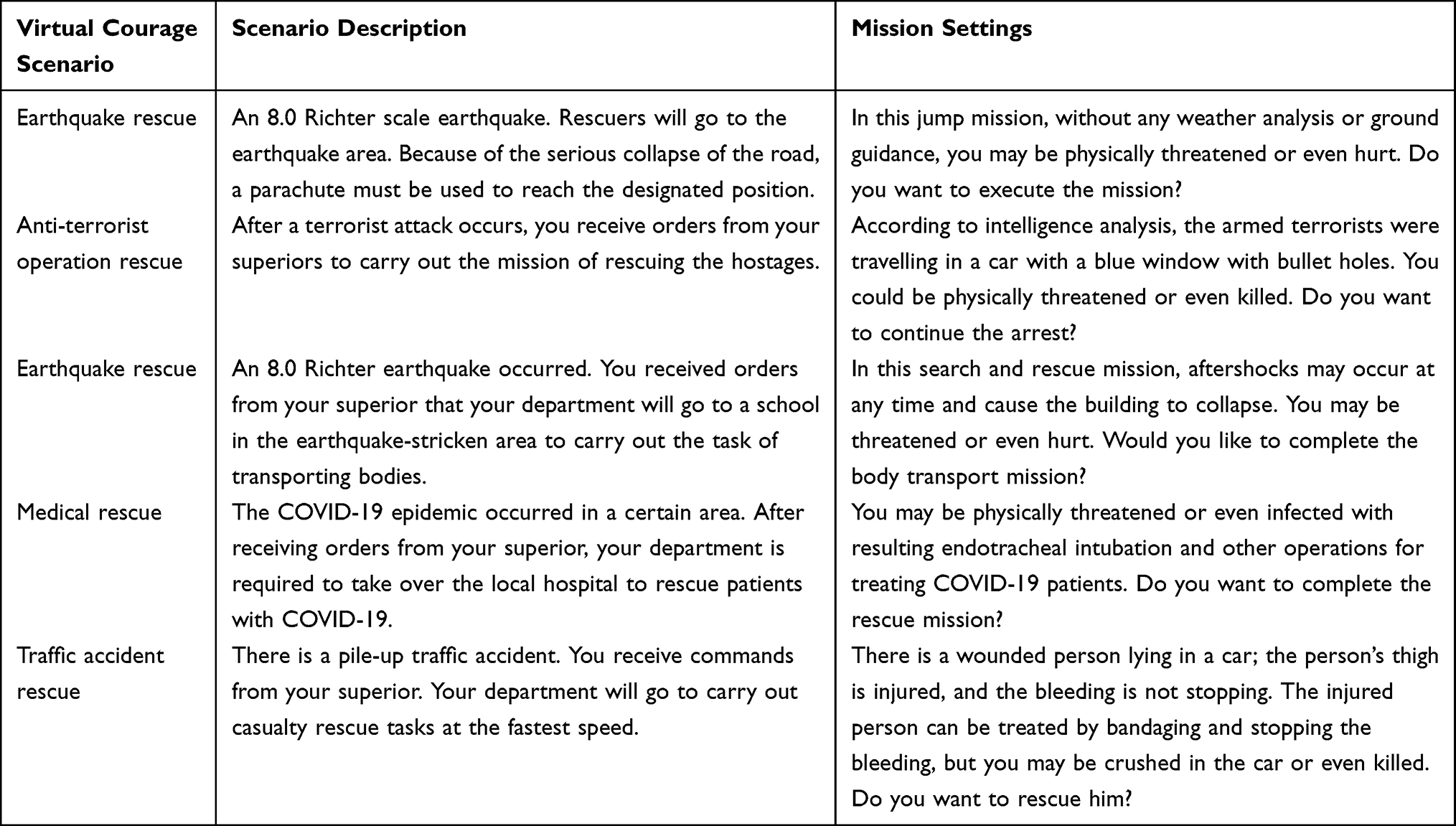 |
Table 1 Description of the Virtual Courage Scenario |
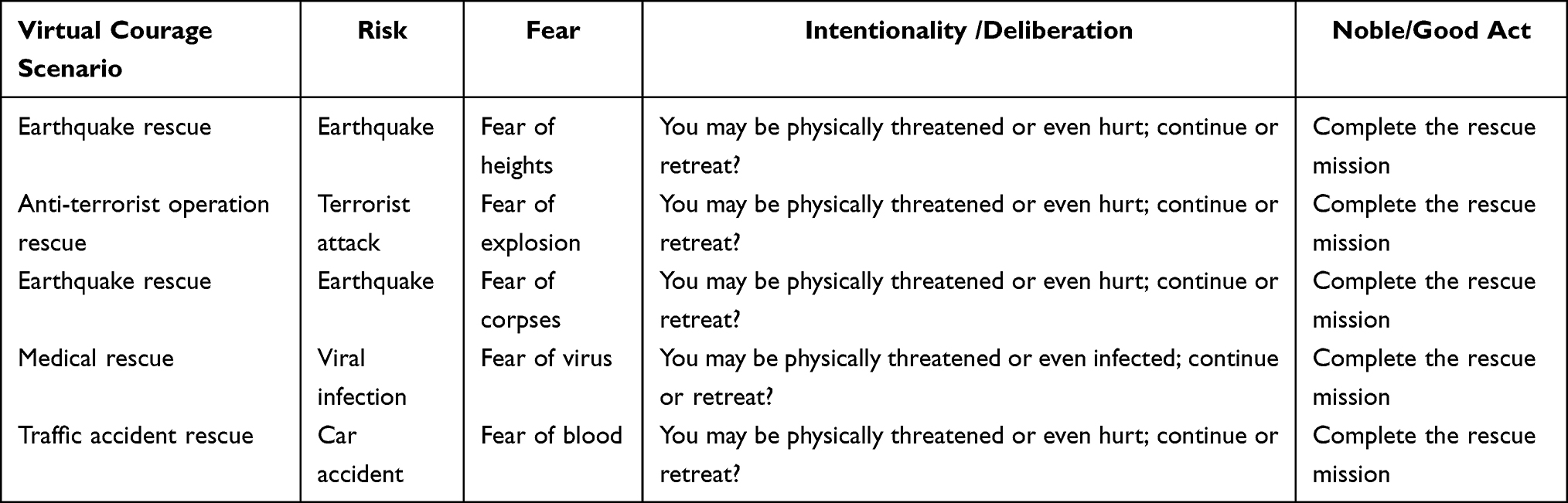 |
Table 2 The Dimensions of the Virtual Courage Scenario |
The Unity 3D platform was used to develop virtual courage scenarios through real-time 3D graphics generation technology, wide-angle (wide-field) stereoscopic display technology, tracking technology and dynamic environment modelling technology. Examples of earthquake rescue (fear of corpses) scenarios are shown in Figure 1. Tracking and interactive devices are shown in Figure 2.
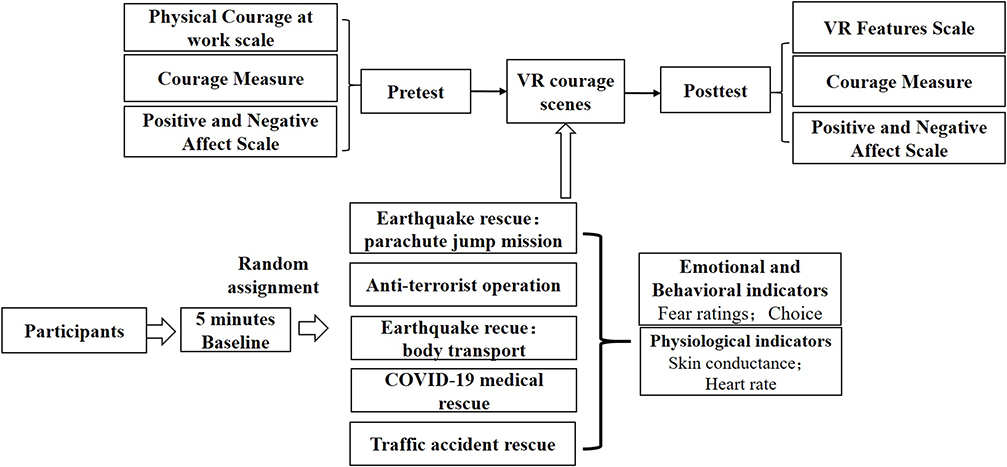 |
Figure 1 Examples of earthquake rescue scenarios. |
 |
Figure 2 Examples of tracking and interactive devices. |
Procedure
The survey was guided by a psychological researcher in the VR laboratory. The participants were administered a battery of questionnaires, and missing or irregular answers were excluded. The questionnaires were administered before and after the participants watched the VR courage scenarios. Before the experiment, 5 minutes of resting-state baseline was recorded (physiological indicators). Then, the participants were randomly assigned to 1 of 5 virtual courage scenarios, and each scenario’s physiological indicators were recorded (Figure 3).
 |
Figure 3 Flow Diagram of Experiment. |
Apparatus
The VR task was implemented on HTC VIVE Pro Eye (professional edition), including a headset (width: 255 mm, height: 128 mm, weight: 790 g, resolution ratio: 2880×1600, 45° field-of-view), positioner (Steam VR 2.0) and joy pad. The software was run on a Windows 10 system, i9-9900K CUP, RTX2080Ti VGA Card, 32 GB RAM.
The physiological feedback instrument was a BioGraph Infiniti 8 channel produced by Canada Thought Technology.51,52
Statistical Analysis
The five scenarios of courage were evaluated as a whole since the scores of the VR features were representative of the all situation. The evaluation of VR features with respect to courage scores was first tested with descriptive statistics analysis and a one-way Wilcoxon test.
Then, we explored the validity of virtual courage paradigms. The scores of PCWS were assessed before the experiments. The scores of CM and afraid, scared were assessed before and after the experiments since the aims of study was to evaluated the courage scenarios as a whole. The CM scores before and after the VR scenarios were compared with a paired Wilcoxon test.
Additionally, for behavioral indicators, all participants chose to complete the mission during the each scenario. The behavioral indices before and after the VR scenarios were compared with a paired Wilcoxon test. The physiological indices were compared between the baseline and virtual scenarios with a paired Wilcoxon test.
Finally, Pearson’s correlation analysis between the scores of the PCWS and physiological indexes was performed.
Among them, 2 participants of CM data missed, 1 participants of skin conductance and heart rate in earthquake rescue (completing the parachute jump mission) and traffic accident rescue data missed, 3 participants of skin conductance and heart rate in earthquake rescue (completing a transfer mission) data missed. All analyses were conducted using SPSS 21.0. And the calculation of effect size (Cohen’s d) was using the Software JASP (https://jasp-stats.org/).
Results
Evaluation of VR Features
The scores of interaction, immersion and presence were higher than the median 4 points for all scenarios. The result of the one-way Wilcoxon test showed that the score of each indicator was significantly higher than the theoretical median value, which indicated that the subjects’ evaluation of interaction, immersion and presence was significantly higher than the theoretical median value (Table 3).
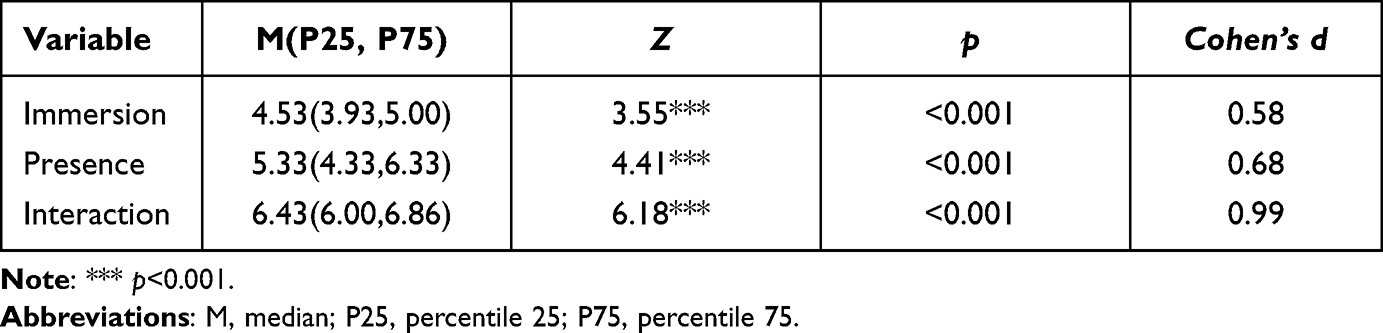 |
Table 3 Test of the Differences Between the Variables and the Median Value (n=51) |
Evaluation of Courage
The scores on the PCWS ranged from 74 to 179 [M (137, 158)]. The descriptive statistics of the CM scores are shown in Table 4. The score for courage in the pretest was significantly lower than that in the posttest (Z =3.06, p =0.002, Cohen’s d =0.52).
 |
Table 4 Test of the CM Score Difference Between the Pretest and Posttest (n=49) |
Evaluation of Emotional and Behavioral Indicators
In the pretest, the scores of the items scared (p<0.001, Cohen’s d =0.81) and afraid (p<0.001, Cohen’s d =0.82) were significantly lower than the theoretical median (3 points). The paired Wilcoxon test showed that in the posttest, the scared (p<0.001, Cohen’s d =0.95) and afraid (p<0.001, Cohen’s d =0.95) scores were significantly higher than the theoretical median (3 points). In further exploration of the fear ratings between the pre- and posttest, the results indicated that the posttest scores of both scared (p<0.001, Cohen’s d =0.95) and afraid (p<0.001, Cohen’s d =0.99) were significantly higher than the pretest scores (Table 5).
 |
Table 5 Test of the Differences in Fear Variables Between the Pretest and Posttest (n=51) |
All participants chose to complete the mission.
Evaluation of Physiological Indicators
The descriptive statistics of heart rate are shown in Table 6. The heart rate values of each scenario showed an increase compared with the baseline.
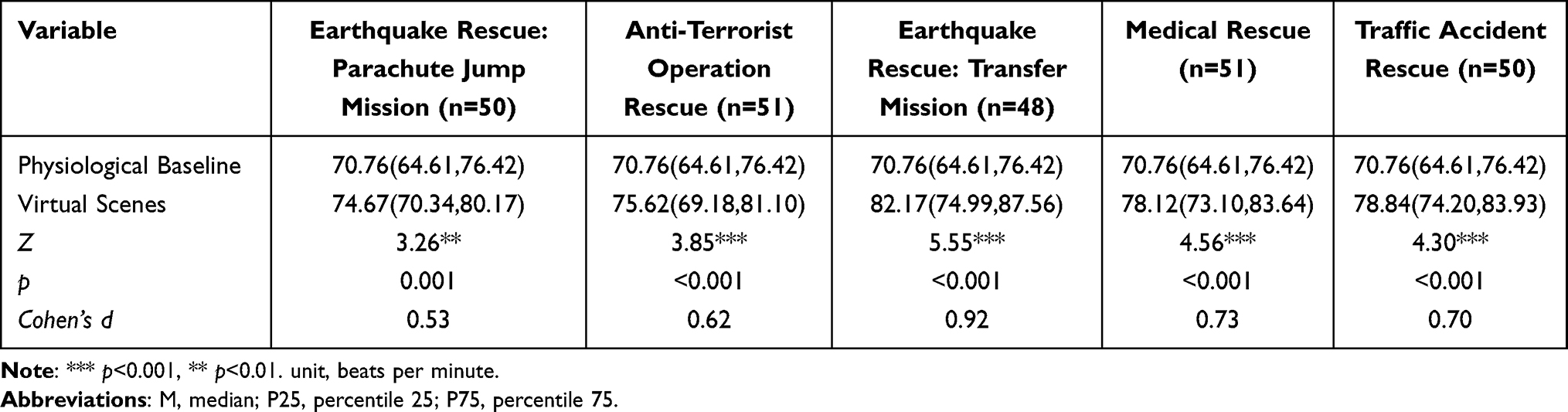 |
Table 6 Test of the Heart Rate Differences Between Pretest and the Baseline [M(P25, P75)] |
The descriptive statistics of skin conductance are shown in Table 7. The skin conductance values of each scenario showed an increase compared with the baseline.
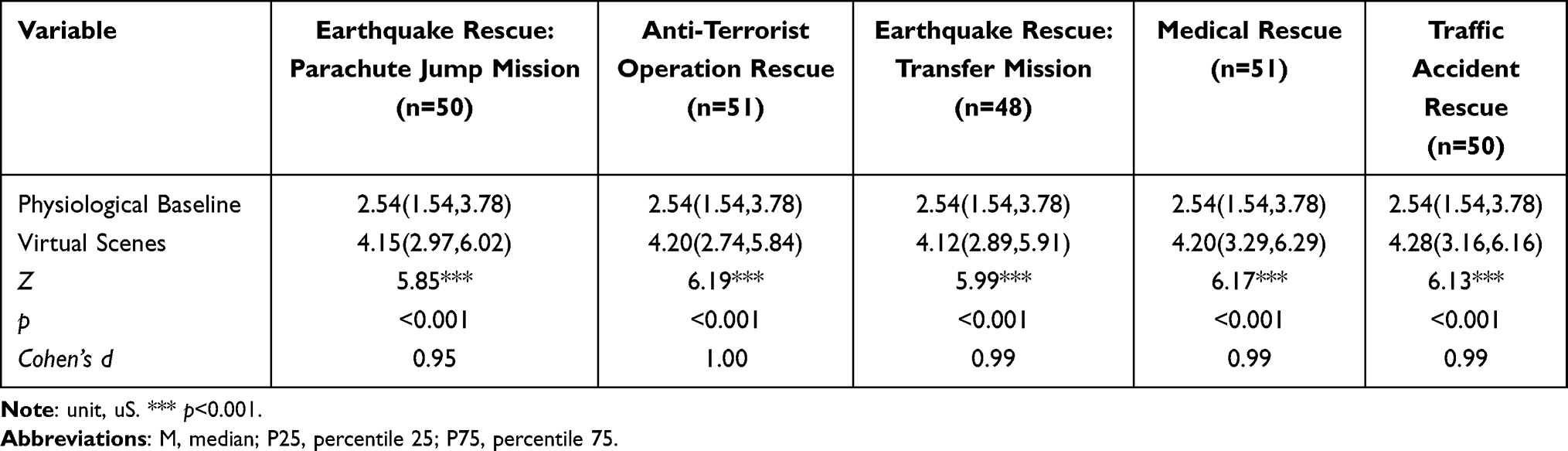 |
Table 7 Test of the Skin Conductance Differences Between Pretest and the Baseline [M(P25, P75)] |
Pearson’s correlation analysis revealed that in addition to the heart rate in the traffic accident scenario and earthquake rescue/parachute scenario, all other physiological indicators were negatively associated with the PCWS score (Table 8).
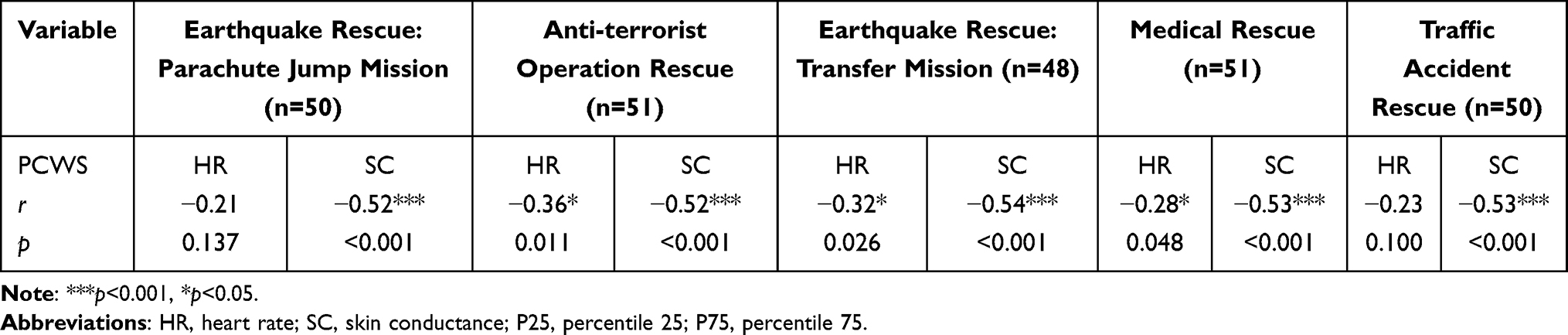 |
Table 8 Correlation Analysis Between Physiological Indicators and the PCWS Score |
Discussion
Trainees in high-risk occupations lack professional skills and experiences to deal with perilous circumstances. However, their career requirements push them to handle hazardous situations. Developing a virtual high-risk environment might provide new opportunities to elevate predispositions (such as courage) to manage hazardous situations.60 Each of the remaining virtual scenarios was typical for firefighters and other high-risk employees who participate in imminently life-threatening rescues. Meanwhile, virtual courage paradigms can represent elements of courage, such as risk, perceived fear, intentionality/deliberation, and noble/good act, which align with the subjective experience of courage theory.61 Each virtual courage scenario reflected the essential prerequisite of brave behavior in a high-risk workplace and corresponded to various elements of the courage components. For example, in the virtual medical rescue scenario, especially the COVID-19 pandemic scenario, the event design of risk and fear components required medical practitioners or paramedics to embody fearlessness or to experience fear but still deal with the events.47,62 The determination of courage requires high-risk employees to decide whether to proceed with a rescue mission while risking infection, injury or death, which means that the quality of decisiveness must be applied to respond to events in the scenario.56 For example, in virtual earthquake rescue, a decision is made by the participant through a joy pad by interacting with scenario questions such as “You may be physically threatened or even hurt; continue or retreat”. In the process of achieving the noble/good goal, rescuers encounter multiple challenges, such as fear and difficulties. Therefore, the design of the event requires rescuers to develop tenacity and toughness to deal with the scenario events.32,63 This development of virtual courage paradigms is consistent with the conceptions of courage in process theory,55 subjective experience theory61 and cognitive theory,64 which highlight risk, fear and decision-making processes from the perspectives of their particular theoretical foundation.
Immersion, presence and interaction are features of VR that are prioritized. Immersion emphasizes the vividness of simulation,21 presence underlines the psychological feeling of the virtual environment, and interaction focuses on the users’ interactivity. The evaluation scores in these courage scenarios were above 4 points (p<0.01), in agreement with previous studies and indicating that the VR features were above the median.65,66 These results indicated that the virtual scenarios we established possessed good physical properties and enabled subjective experiences similar to the real-world experiences; that is, they allowed the subjects to be immersed in the scenario even though they consciously knew that the immersive scenario did not happen in the real world.24,67 In addition, interactivity is reflected in the scenarios in which the subjects complete the corresponding task. The score of interactivity in the VR system was above 6 points (p<0.01), which means that the scenario interaction property in this study was at a high level.41,68 Consequently, given the requirements for VR, the utility of virtual systems for courage meets or exceeds the specified standard requirements, which establishes a foundation for their application in simulating high-risk operations and improving courage paradigms.30
The PCWS represented trait-oriented stability.3 Correlation analysis confirmed that people with high-level predispositions to physical courage have inverse activations of heart rate and skin conductance.18 The reason is that the physiological responses indicate a stress response (heart rate and skin conductance evoked), which possibly mediates this relationship between physiological arousal and courage.18,32,33 This result is consistent with previous studies showing that brave bomb-disposal operators and soldiers showed lower physiological reactivity (cardiac reactivity) and less fear due to a substantial increase in courage, skill and confidence after completing a specialized course.18 In the virtual courage scenarios, the behavioral indicators and physiological indicators revealed that the individuals’ fear was evoked, which provided a stimulation to train or boost courage in specific conditions. For emotional indicators in virtual courage paradigms, the subjective posttest scores of being scared and afraid were both higher than the pretest and the median scores. This result revealed that the subjects’ fear emotions were effectively awakened, which provided the basis for stimulating scenarios for high-risk employees.15 As for behavioral indicators, all participants chose to complete the mission for the possible reasons were that firefighters were trained by tolerance of risk so that participants could complete the mission without retreating2 and that the phenomenon of social desirability, in which a tendency of respondents to give answers to make them better to meet the social norms.69 In terms of physiological indicators, the participants’ heart rate and skin conductance in the virtual courage scenarios were both higher than those at baseline, indicating that physiological fear reactions were significantly activated by the simulation.30,70 The simulating effect of the virtual courage scenarios may occur through three possible psychological paths. First, individuals learned how to endure and confront fear. From an evolutionary perspective, an optimal level of fear can increase one’s awareness and have adaptive significance under jeopardy. However, if fear is overwhelming, it will cause the individual to freeze or flight, which leads to a state of incapability.28 VR courage scenarios can provide training in situations that help employees regulate fear and conquer intense fear. Additionally, they allow coping skills to be mastered. By immersion within the VR courage scenarios, individuals are confronted with risk or threat, and they have to manage their skills to complete the rescue mission. During the course, inner strength or personal growth might occur.32 Last, the direction of the motivational system was altered. Fear activates the brain’s aversion/avoidance motivation system to keep away from danger.8 However, achieving duty requires high-risk employees to conquer fear towards the noble goal, which might mean activating an appetitive or approach motivational system.71 Hence, the pre- and posttest scores on CM proved the effectiveness of the evaluation. The CM was used to evaluate courageous acts in high-risk operational sites, which can be considered state-oriented bravery that might align with inordinate risk.17 The pre- and posttest scores showed that after the participants were immersed in the virtual courage scenarios, there was an increased effect on state courage. This phenomenon might be associated with exposure to a moderate fear level with which the participant can cope well, which increases the individual’s confidence to conquer fear and achieve the goal.32,47
Conclusion
This study developed virtual courage paradigms for high-risk occupations based on well-established theory and VR technology. The experimental data revealed that the paradigms conformed to the requirements of VR features and were able to activate fear and elevate the quality of courage. Thus, virtual courage paradigms have good validity and can be applied to simulate scenarios for high-risk employees, which might accelerate organizational effectiveness while buffering work stress.
The current study has several limitations. First, the participants were high-risk trainees who lack rich experience, and further study should explore the courage paradigm effect in expert high-risk employees. Additionally, female firefighters were recruited in the experiment because the number of women is increasing worldwide, reaching 6.3% of firefighters.72 However, the 10 female participants are not representative from the perspective of statistics, and more women firefighters should be investigated so that gender differences in courage can be uncovered. Second, in the behavioral indicator, no participants chose to abandon the rescue mission, and the decision time from was not recorded, leading to each component of courage not matching the precise reaction time so that the results did not allow analysis of the effect of each component. Then, the stimulus was generated only through visual, auditory and motor sensation since subjective fear was at a moderate level. Further research should diversify the types of stimulation, such as pain perception and tactile and olfactory stimulation, to form a physiology-driven adaptive virtual stimulation with big data. Physiological state feedback can be implemented based on specific subjects and can include a stimulated production module, a synchronous physiological reaction module, a module for participants’ emotional evaluation and an adaptively generated new stimulus module.73 Hence, the system could be controlled precisely according to the specific situations with a variety of stimuli similar to real-world situations, ensuring ecological validity. In addition, only heart rate and skin conductance were used as physiological indicators in this study to determine the possible association between the predisposition for courage and the autonomic nervous system. Further studies should enrich stimulation monitoring, such as by utilizing functional magnetic resonance imaging technology and transcranial magnetic stimulation technology to explore neural circuitry in the brain or taking samples of blood to test cortisol and inflammatory cytokines to examine the neuroendocrine system. Thus, the system could establish behavioral, psychological, and physiological multidimensional indicators to achieve an accurate evaluation that supports a qualitative standard for assessments. Crucially, further research should add training modules into virtual courage scenarios, for instance, virtual extinction74 or virtual-reality exposure therapy75 for fear reduction, decision-making training to cultivate the effectiveness of risk decision-making76 and battlemind training32 to foster toughness and perseverance towards noble goals.
Informed Consent Statement
Informed consent was obtained from all of the subjects involved in the study.
Funding
This study was financially supported by Natural Science Foundation of Chongqing (No.cstc2018jcyjAX0276).
Disclosure
The authors declare no conflict of interest.
References
1. Roberts SE, Jaremin B, Lloyd K. High risk occupations for suicide. Psychol Med. 2013;43(6):1231–1240. doi:10.1017/S0033291712002024
2. Jonker BE, Graupner LI, Rossouw L. An intervention framework to facilitate psychological trauma management in high-risk occupations. Front Psychol. 2020;11:530. doi:10.3389/fpsyg.2020.00530
3. Howard MC, Reiley PJ. Physical courage predicts relevant outcomes in associated contexts: the creation of a measure and empirical analysis into the construct. J Bus Res. 2020;110:80–94. doi:10.1016/j.jbusres.2019.12.015
4. Smith J, Purewal BP, Macpherson A, Pike I. Metrics to assess injury prevention programs for young workers in high-risk occupations: a scoping review of the literature. Health Promot Chronic Dis Prev Can. 2018;38(5):191–199. doi:10.24095/hpcdp.38.5.01
5. Siordia C, Galley F. Participation of workers of Asian ancestry in high-risk occupations in the United States: 2009 to 2017. J Immigr Minor Health. 2020;22(5):1010–1016. doi:10.1007/s10903-020-01006-5
6. Mitcheli MM, Gallaway MS, Millikan AM, Bell MR. Combat exposure, unit cohesion, and demographic characteristics of soldiers reporting posttraumatic growth. J Loss Trauma. 2013;18(5):383–395. doi:10.1080/15325024.2013.768847
7. Beaton R, Murphy S, Johnson C, Pike K, Corneil W. Exposure to duty-related incident stressors in urban firefighters and paramedics. J Trauma Stress. 1998;11(4):821–828. doi:10.1023/A:10244
8. Rösler L, Gamer M. Freezing of gaze during action preparation under threat imminence. Sci Rep-UK. 2019;9(1):17215. doi:10.1038/s41598-019-53683-4
9. Blanchard DC. Translating dynamic defense patterns from rodents to people. Neurosci Biobehav Rev. 2017;76:22–28. doi:10.1016/j.neubiorev.2016.11.001
10. Andersen LP, Hogh A, Elklit A, Andersen JH, Biering K. Work-related threats and violence and post-traumatic symptoms in four high-risk occupations: short- and long-term symptoms. Int Arch Occup Environ Health. 2019;92(2):195–208. doi:10.1007/s00420-018-1369-5
11. Sommer JL, Mota N, Reynolds K, El-Gabalawy RE. COVID-19 as a traumatic stressor is an indicator of mental health symptomatology. Psychiatry Res. 2021;300:113936. doi:10.1016/j.psychres.2021.113936
12. Shahzad F, Du J, Khan I, et al. Perceived Threat of COVID-19 contagion and frontline paramedics’ agonistic behaviour: employing a stressor-strain-outcome perspective. Int J Env Res Pub Health. 2020;17(14):5102. doi:10.3390/ijerph17145102
13. Salari N, Khazaie H, Hosseinian-Far A, et al. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: a systematic review and meta-regression. Hum Resour Health. 2020;18(1). doi:10.1186/s12960-020-00544-1
14. Vinokur AD, Pierce PF, Lewandowski-Romps L, Hobfoll SE, Galea S. Effects of war exposure on air force personnel’s mental health, job burnout and other organizational related outcomes. J Occup Health Psych. 2011;16(1):3–17. doi:10.1037/a0021617
15. Rate CR, Clarke JA, Lindsay DR, Sternberg RJ. Implicit theories of courage. J Posit Psychol. 2007;2(2):80–98. doi:10.1080/17439760701228755
16. Peterson C, Seligman M. Character Strengths and Virtues: A Handbook and Classification. Vol. 7. New York: Oxford University Press; 2004.
17. Norton PJ, Weiss BJ. The role of courage on behavioral approach in a fear-eliciting situation: a proof-of-concept pilot study. J Anxiety Disord. 2009;23(2):212–217. doi:10.1016/j.janxdis
18. Rachman SJ. Fear and courage: a psychological perspective. Soc Res. 2004;71(1):149–176. doi:10.1353/sor.2004.0060
19. Gayton SD, Kehoe EJ. Character strengths of junior Australian army officers. Mil Med. 2019;184(5–6):147–153. doi:10.1093/milmed/usy251
20. Lan F, Yiannakou I, Scheibler C, et al. The effects of fire academy training and probationary firefighter status on select basic health and fitness measurements. Med Sci Sport Exer. 2021;53(4):740–748. doi:10.1249/MSS.0000000000002533
21. Bohil CJ, Alicea B, Biocca FA. Virtual reality in neuroscience research and therapy. Nat Rev Neurosci. 2011;12(12):752–762. doi:10.1038/nrn3122
22. Tarr MJ, Warren WH. Virtual reality in behavioral neuroscience and beyond. Nat Neurosci. 2002;5(5):1089–1092. doi:10.1038/nn948
23. Chirico A, Gaggioli A. When virtual feels real: comparing emotional responses and presence in virtual and natural environments. Cyberpsychol Behav Soc Netw. 2019;22(3):220–226. doi:10.1089/cyber.2018.0393
24. Sanchezvives MV, Slater M. From presence to consciousness through virtual reality. Nat Neurosci. 2005;6(4):332–339. doi:10.1038/nrn1651
25. Pallavicini F, Argenton L, Toniazzi N. Virtual reality applications for stress management training in the military. Aerosp Med Hum Perform. 2016;87(12):1–10. doi:10.3367/AMHP.4596.2016
26. Colombo D, Díaz García A, Fernandez Álvarez J, Botella C. Virtual reality for the enhancement of emotion regulation. Clin Psychol Psychother. 2021;28(3):519–537. doi:10.1002/cpp.2618
27. Rizzo A, John B, Newman B, et al. Virtual reality as a tool for delivering PTSD exposure therapy and stress resilience training. Mil Behav Health. 2013;1(1):52–58. doi:10.1080/21635781.2012.721064
28. Ralphs A. The biology of fear. Curr Biol. 2013;23(2):79–93. doi:10.1016/j.cub.2012.11.055
29. Yancey JR, Bowyer CB, Foell J, Boot WR, Patrick CJ. Boldness moderates the effects of external threat on performance within a task-switching paradigm. J Exp Psychol Hum Percept Perform. 2019;45(6):758–770. doi:10.1037/xhp0000631
30. Lin JT. Fear in virtual reality (VR): fear elements, coping reactions, immediate and next-day fright responses toward a survival horror zombie virtual reality game. Comput Hum Behav. 2017;72:350–361. doi:10.1016/j.chb.2017.02.057
31. Cougle JR, Hawkins KA. Priming of courageous behavior: contrast effects in spider fearful women. J Clin Psychol. 2013;69(9):896–902. doi:10.1002/jclp.21961
32. McGurk D, Castro CA. Courage in combat. In: The Psychology of Courage Modern Research on an Ancient Virtue. Washington: American Psychological Association; 2009.
33. Nili U, Goldber H, Weizman A, Dudai Y. Fear thou not: activity of frontal and temporal circuits in moments of real-life courage. Neuron. 2010;66(6):949–962. doi:10.1016/j.neuron.2010.06.009
34. De Terte I, Stephens C. Psychological resilience of workers in high-risk occupations. Stress Health. 2014;30(5):353–355. doi:10.1002/smi.2627
35. Lim G, Jang T, Sim C, Ahn YS, Jeong KS. Comparison of cortisol level by shift cycle in Korean firefighters. Int J Env Res Pub Health. 2020;17(13):4760. doi:10.3390/ijerph17134760
36. Geuzinge R, Visse M, Duyndam J, Vermetten E. Social embeddedness of firefighters, paramedics, specialized nurses, police officers, and military personnel: systematic review in relation to the risk of traumatization. Front Psychiatry. 2020;11. doi:10.3389/fpsyt.2020.496663.
37. Kaya E, Altintas H. Willingness of firefighting program students to work in disasters—Turkey. Prehosp Disaster Med. 2018;33(1):13–22. doi:10.1017/S1049023X17007087
38. Tamminen JI, Hoppu SE, Kämäräinen AJJ. Professional firefighter and trained volunteer first-responding units in emergency medical service. Acta Anaesth Scand. 2019;63(1):111–116. doi:10.1111/aas.13224
39. Fox CM, Brockmyer JH. The development of the game engagement questionnaire: a measure of engagement in video game playing: response to reviews. Interact Comput. 2013;25(4):290–293. doi:10.1093/iwc/iwt003
40. Slater V, Usoh M, Steed A. Depth of presence in virtual environments. Presence. 1994;3(2):130–144. doi:10.1162/pres.1994.3.2.130
41. Chang CW, Heo J, Yeh SC. The effects of immersion and interactivity on college students’ acceptance of a novel VR- supported educational technology for mental rotation. Ieee Access. 2018;6:66590–66599. doi:10.1109/ACCESS.2018.2878270
42. Venkatesh V. Determinants of perceived ease of use: integrating control, intrinsic motivation, and emotion into the technology acceptance model. Inform Syst Res. 2000;11(4):342–365. doi:10.1287/isre.11.4.342.11872
43. Kugel U, Hausman C, Black L, Bongar B. Psychology of Physical Bravery. Oxford Handbooks Online: Oxford University Press; 2017.
44. Olsthoorn P. Courage in the military: physical and moral. J Mil Ethics. 2007;6(4):270–279. doi:10.1080/15027570701755471
45. Jia W, Zhong WH, Juan J, Wei L, Ping TH, Zhi FZ. Revision of the physical courage at work scale. J Environ Occup Med. 2022;39(1):36–40.
46. Ginevra MC, Magnano P, Ernesto L, et al. The role of career adaptability and courage on life satisfaction in adolescence. J Adolesc. 2018;62(1):1–8. doi:10.1016/j.adolescence.2017.11.002
47. Magnano P, Paolillo A, Platania S, Santisi G. Courage as a potential mediator between personality and coping. Pers Indiv Differ. 2017;111:13–18. doi:10.1016/j.paid.2017.01.047
48. Magnano P, Santisi G, Zammitti A, Zarbo R, Nuovo SD. Self-perceived employability and meaningful work: the mediating role of courage on quality of life. Sustainability-Basel. 2019;11(3):764. doi:10.3390/su11030764
49. Detert JR, Bruno EA. Workplace courage: review, synthesis, and future agenda for a complex construct. Acad Manag Ann. 2017;11(2):593–639. doi:10.5465/annals.2015.0155
50. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037/0022-3514.54.6.1063
51. Hanzelka M, Dan J, Szabó Z, Roubal Z, Dohnal P, Kadlec R. Methods and experiments for sensing variations in solar activity and defining their impact on heart variability. Sensors-Basel. 2021;21(14):4817. doi:10.3390/s21144817
52. Thomas BL, Viljoen M. EEG brain wave activity at rest and during evoked attention in children with attention-deficit/hyperactivity disorder and effects of methylphenidate. Neuropsychobiology. 2016;73(1):16–22. doi:10.1159/000441523
53. Franco ZF, Blau K, Zimbardo PG. Heroism: a conceptual analysis and differentiation between heroic action and altruism. Rev Gen Psychol. 2011;15(2):99–113. doi:10.1037/a0022672
54. Landy FJ, Gaupp LA. A factor analysis of the fear survey schedule-III. Behav Res Ther. 1971;9(2):89–93. doi:10.1016/0005-7967(71)90065-9
55. Petersen SE. A Repertory Grid Evaluation of a Multidimensional Theory of Courage. Kansas: The University of Kansas; 2004.
56. Kugel U. Physical Courage Among Military Personnel and Veterans. California: Doctor of Philosophy, Palo Alto University; 2014.
57. Rate CR. What is Courage? A Search for Meaning. New Haven: Yale University; 2007.
58. Goethals GR, Allison ST. Making heroes: the construction of courage, competence and virtue. Adv Exp Soc Psychol. 2012;46:184–231. doi:10.1016/B978-0-12-394281-4.00004-0
59. Howard MC, Farr JL, Grandey AA, Gutworth MB. The Creation of the Workplace Social Courage Scale (WSCS): an investigation of internal consistency, psychometric properties, validity, and utility. J Bus Psychol. 2017;32(6):673–690. doi:10.1007/s10869-016-9463-8
60. Engelbrecht H, Lindeman RW, Hoermann S. A SWOT analysis of the field of virtual reality for firefighter training. Front Robot AI. 2019;6. doi:10.3389/frobt.2019.00101.
61. Hannah ST, Sweeney PJ, Lester PB. Toward a courageous mindset: the subjective act and experience of courage. J Posit Psychol. 2007;2(2):129–135. doi:10.1080/17439760701228854
62. McCabe S, Carpenter RW, Arndt J. The role of mortality awareness in heroic enactment. J Exp Soc Psychol. 2015;61:104–109. doi:10.1016/j.jesp.2015.08.001
63. Maddi SR. The courage and strategies of hardiness as helpful in growing despite major, disruptive stresses. Am Psychol. 2008;63(6):563–564. doi:10.1037/0003-066X.63.6.563
64. Woodard CR. Hardiness and the Concept of Courage. California: Doctor of philosophy in psychology, Fielding Graduate University; 2001.
65. Chang C, Yeh S-C, Li M, et al. The introduction of a novel virtual reality training system for gynecology learning and its user experience research. IEEE Access. 2019;7:43637–43653. doi:10.1109/ACCESS.2019.2905143
66. Yua X, Cui X, Cao Z, et al. Attentional bias towards threatening visual stimuli in a virtual reality-based visual search task. Acta Psychol Sin. 2018;50:22–636. doi:10.3724/SP.J.1041.2018.00622
67. Yeh S, Hou C, Peng W, et al. A multiplayer online car racing virtual-reality game based on internet of brains. J Syst Archit. 2018;89:30–40. doi:10.1016/j.sysarc.2018.06.004
68. Tsai C, Yeh S, Huang Y, Wu Z, Cui J, Zheng L. The effect of augmented reality and virtual reality on inducing anxiety for exposure therapy: a comparison using heart rate variability. J Healthc Eng. 2018;2018:1–8. doi:10.1155/2018/6357351
69. Perinelli E, Gremigni P. Use of social desirability scales in clinical psychology: a systematic review. J Clin Psychol. 2016;72(6):534–551. doi:10.1002/jclp.22284
70. Diemer J, Lohkamp N, Mühlberger A, Zwanzger P. Fear and physiological arousal during a virtual height challenge—effects in patients with acrophobia and healthy controls. J Anxiety Disord. 2016;37:30–39. doi:10.1016/j.janxdis.2015.10.007
71. Bradley M, Lang PJ. Measuring emotion: behavior, feeling, and physiology. In: Lane RD, Nadel N, editors. Cognitive Neuroscience of Emotion. New York: Oxford University Press; 2000.
72. Watkins ER, Walker A, Mol E, Jahnke S, Richardson AJ. Women firefighters’ health and well-being: an international survey. Women Health Issues. 2019;29(5):424–431. doi:10.1016/j.whi.2019.02.003
73. Popovic S, Horvat M, Kukolja D, Dropuljic B, Cosic K. Stress inoculation training supported by physiology-driven adaptive virtual reality stimulation. Stud Health Technol Inform. 2009;144:50–54. doi:10.1109/CAMSAP.2009.5413285
74. Maples-Keller JL, Yasinski C, Manjin N, Rothbaum BO. Virtual reality-enhanced extinction of phobias and post-traumatic stress. Neurotherapeutics. 2017;14(3):554–563. doi:10.1007/s13311-017-0534-y
75. Beidel DC, Frueh BC, Neer SM, et al. Trauma management therapy with virtual-reality augmented exposure therapy for combat-related PTSD: a randomized controlled trial. J Anxiety Disord. 2019;61:64–74. doi:10.1016/j.janxdis.2017
76. Yang Q, Zhao D, Wu Y, Tang P, Gu R, Luo Y. Differentiating the influence of incidental anger and fear on risk decision-making. Physiol Behav. 2018;184:179–188. doi:10.1016/j.physbeh
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.