")
Back to Journals » OncoTargets and Therapy » Volume 8
The utility of bexarotene in mycosis fungoides and Sézary syndrome
Authors Panchal MR, Scarisbrick J
Received 12 September 2014
Accepted for publication 18 November 2014
Published 3 February 2015 Volume 2015:8 Pages 367—373
DOI https://doi.org/10.2147/OTT.S61308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Faris Farassati
Manisha R Panchal, Julia J Scarisbrick
Department Dermatology, University Hospital Birmingham, Birmingham, UK
Abstract: Cutaneous T-cell lymphoma (CTCL) is an umbrella term that encompasses a group of neoplasms that have atypical T-lymphocytes in the skin. Mycosis fungoides (MF) is the most common type of CTCL and Sézary syndrome (SS) is the leukemic form. Treatment for CTCL is dependent on the stage of disease and response to previous therapy. Therapy is divided into skin-directed treatment, which tends to be first line for early-stage disease, and systemic therapy, which is reserved for refractory CTCL. Bexarotene is a rexinoid and was licensed in Europe in 2002 for use in patients with advanced disease that have been refractory to a previous systemic treatment. We review the use of bexarotene as monotherapy and in combination with other treatments.
Keywords: retinoid, CTCL, cutaneous T-cell lymphoma
Introduction
Primary cutaneous T-cell lymphoma (CTCL) is a group of extranodal non-Hodgkin lymphoma and represents around 70% of primary cutaneous lymphomas. Primary cutaneous lymphomas are classified according to the World Health Organization (WHO) – European Organization for Research and Treatment of Cancer (EORTC) and subdivided into lymphomas that are indolent and those with aggressive subtypes. Mycosis fungoides (MF) is typically an indolent disease and the most common subtype of CTCL.1 MF usually presents with patches and plaques confined to the skin (early-stage disease IA–IIA) and may progress to develop skin tumors, erythroderma, or nodal or visceral involvement (advanced stage disease IIB–IVB). However, 25% will present with advanced stage disease. Survival in the early stages may be long (10–25 years), whilst those with advanced disease have a poor prognosis and a median survival of 1–4 years. Sézary syndrome (SS) is the leukemic form of CTCL and presents in advanced disease with erythroderma, lymphadenopathy, and circulating Sézary cells.
Diagnosis of MF may be a challenge, especially in the early stages and may require multiple biopsies for histology, immunophenotype, and molecular studies. Other investigations include peripheral blood samples for full blood count, renal function, liver function, lactate dehydrogenase, Sézary cell count, lymphocyte subsets, CD4/CD8 ratio, human T-cell lymphotropic virus (HTLV)-1 serology, and T-cell receptor gene analysis of peripheral blood mononuclear cells. Imaging in the form of computed tomography (CT) of the neck, chest, abdomen, and pelvis should be performed in patients with stage IIA–IV CTCL (Bunn and Lambert system). All patients should be fully staged according to the tumor, node, metastases, and blood (TNMB) classification and assigned a stage IA–IVB at diagnosis.2 Similarly, at stage progression, TNMB should be recorded.
There is no algorithm for treatment of MF/SS but published guidelines are available and offer treatment options.3–7 Treatment is dependent on the stage of disease and responsiveness to previous therapy. Treatment is divided into skin-directed therapy and systemic treatments. Early-stage disease should be treated with skin-directed therapy, which includes topical steroids, psoralens and ultraviolet A (PUVA), narrowband ultraviolet B (UVB), superficial radiotherapy, topical retinoids, and topical cytostatic agents such as mechlorethamine or carmustine (BCNU). Skin-directed therapy may be used in combination with systemic agents for progressive disease. Systemic therapy includes interferon alpha, retinoids, methotrexate, histone deacetylase inhibitors, extracorporeal photopheresis (ECP), monoclonal antibody therapy (alemtuzumab, brentuximab), single-agent chemotherapy (doxorubicin, gemcitabine), and multi-agent chemotherapy, which is typically a last resort. Systemic therapies may be combined, but evidence is lacking that combinations are more effective.8 For patients with advanced disease who achieve a remission, allogeneic stem cell transplantation may offer prolonged survival.9–13
Retinoids are immunomodulating agents that are structurally similar to vitamin A and have been used in CTCL for over 2 decades. The first retinoids used in clinical practice in CTCL bind to retinoic acid receptors and include isotretinoin, etretinate, and acitretin. Bexarotene is a synthetic retinoid and member of a subclass of retinoids called rexinoids that selectively activate retinoid X receptors (RXRs) and have distinct biological activity from retinoic acid receptor agonists. Bexarotene binds to and activates RXR-α, -β, and -γ, which act as transcription factors to regulate a range of cellular processes, including cellular differentiation and proliferation, apoptosis, and insulin sensitization.14 Bexarotene is the first selective retinoid binding to the RXR, to be studied in humans.15 It was approved by the US Food and Drug Administration in 1999 and licensed in Europe in 2002 for the treatment of patients with advanced CTCL refractory to at least one systemic treatment. Bexarotene has also been shown to be an effective and safe treatment for refractory early-stage CTCL.16 Bexarotene produced dose-dependent apoptosis of CTCL cell lines and of peripheral blood T-cells from patients with SS in two-thirds of patients (n=9) studied.17,18 Bexarotene has effects on cell differentiation and apoptosis and also downregulates chemokine receptor type 4 (CCR4) and E-selectin expression, affecting malignant T-cell trafficking to the skin.19 It has been used both as monotherapy and combination therapy for CTCL.
Bexarotene gel is also available and used for early-stage CTCL in patients with refractory disease but is not European Medical Agency (EMA)-approved in the UK and will not be discussed further in this paper. Here, we review the use of oral bexarotene in the treatment of MF/SS.
Methods
Literature on the use of bexarotene for MF/SS as classified by the WHO-EORTC were reviewed. AMED, EMBASE, HMIC, MEDLINE, PsycINFO, BNI, CINAHL, and HEALTH BUSINESS ELITE databases were searched. Clinical trials and review articles in all languages were considered.
Bexarotene
Bexarotene capsules are available (Targretin® capsules, 75 mg) and are EMA-approved for treatment of the skin manifestations of advanced stage (IIB–IVB) CTCL in adult patients refractory to at least one systemic treatment and were launched in the UK in 2002. In the US, bexarotene is FDA-approved as a second-line treatment for early- and late-stage refractory disease (IB–IVB). Targretin® is produced as soft capsules containing a liquid suspension of 75 mg of bexarotene per capsule. The dose is dependent on the body surface area. The recommended initial dose is 300 mg/m2/day and this is taken as a single oral daily dose with a meal. Two hours after ingestion, it reaches peak plasma levels and has a half-life of 7 hours. To minimize side effects, an initial dose of 150 mg/m2/day may be appropriate. The dose is then adjusted up or down according to clinical response and toxicity to a maximum of 650 mg/m2/day.
In responders, treatment should be continued. Bexarotene may also be safely combined with other anti-CTCL therapies including PUVA, ECP, methotrexate, and alpha interferon to augment responses.
It is 99% protein-bound and metabolized by cytochrome P450 3A4 (CYP3A4) to hydroxybexarotene and oxybexarotene and excreted in the bile. It is therefore recommended that bexarotene should be avoided in patients with hepatic impairment. Other contraindications include a history of pancreatitis, hypervitaminosis A and pregnancy. The following advice is issued to patients taking bexarotene: “You must use effective contraception (birth control) continuously starting 1 month before beginning treatment with TARGRETIN® capsules until 1 month after you stop taking TARGRETIN® capsules. It is strongly recommended that two reliable forms of contraception be used together. At least one of these two forms of contraception should include condoms, diaphragms, cervical caps, IUDs, or spermicides. If you are male and your partner is pregnant or capable of becoming pregnant, you should discuss with your doctor the precautions you should take”.14
Bexarotene side effects
Side effects from bexarotene are frequent but predictable. Lipid abnormalities and most commonly hypertriglyceridemia is universal. Patients must be counseled on a low-fat diet. Pre-treatment with fenofibrate starting 1 week before bexarotene is recommended.20–22 Patients on a statin may be switched to rosuvastatin instead of fenofibrate, which may be added if triglycerides remain high.20
Thyroid stimulating hormone (TSH) suppression happens in all patients. Thyroxine replacement is recommended from day 1 at a dose of 25–50 μg once daily orally and titrated to keep the free thyroxine level in the upper third of normal, which allows improved lipid control.20
Leukopenia may occur and was reported in 18% of patients in early studies. It may occur as a late side effect and may be managed with granulocyte colony-stimulating factor.23
Other side effects include anemia and peeling of skin on the hands in the first 2 weeks.
A UK Consensus Statement on safe prescribing of bexarotene for patients with CTCL was published in 2012, which provides a protocol for safe utility of bexarotene. The management of side effects is essential to safe prescribing (Table 1).
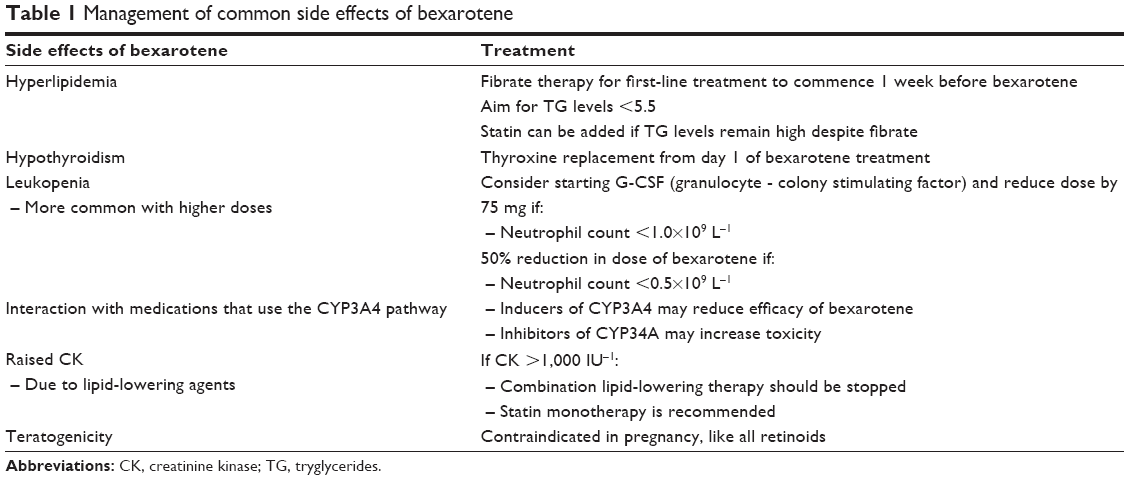 | Table 1 Management of common side effects of bexarotene |
Bexarotene monotherapy
The efficacy of retinoids in the treatment of CTCL was first observed in the 1980s in patients that received isotretinoin and acitretin. Bexarotene use is supported by two Phase II/III trials conducted in both early-stage16 (58 patients) and late-stage disease (94 patients).24 In the treatment of advanced stage CTCL, 45% of patients achieved an overall response rate (ORR) on a dose of 300 mg/m2/day, and 55% achieved ORR on 650 mg/m2/day. Side effects were noted to be dose-dependent. Decreased skin erythema, scaling, and pruritus were reported with blood improvement in those patients with erythrodermic disease. The median duration of response was 7–9 months. In early-stage disease, 15 (54%) of 28 patients at 300 mg/m2/day (95% confidence interval [CI]: 35%–72%), and 10 (67%) of 15 patients at above 300 mg/m2 had a partial response (PR).
Several large single and multicenter studies of bexarotene therapy in MF/SS have been published showing similar efficacy (Table 2).
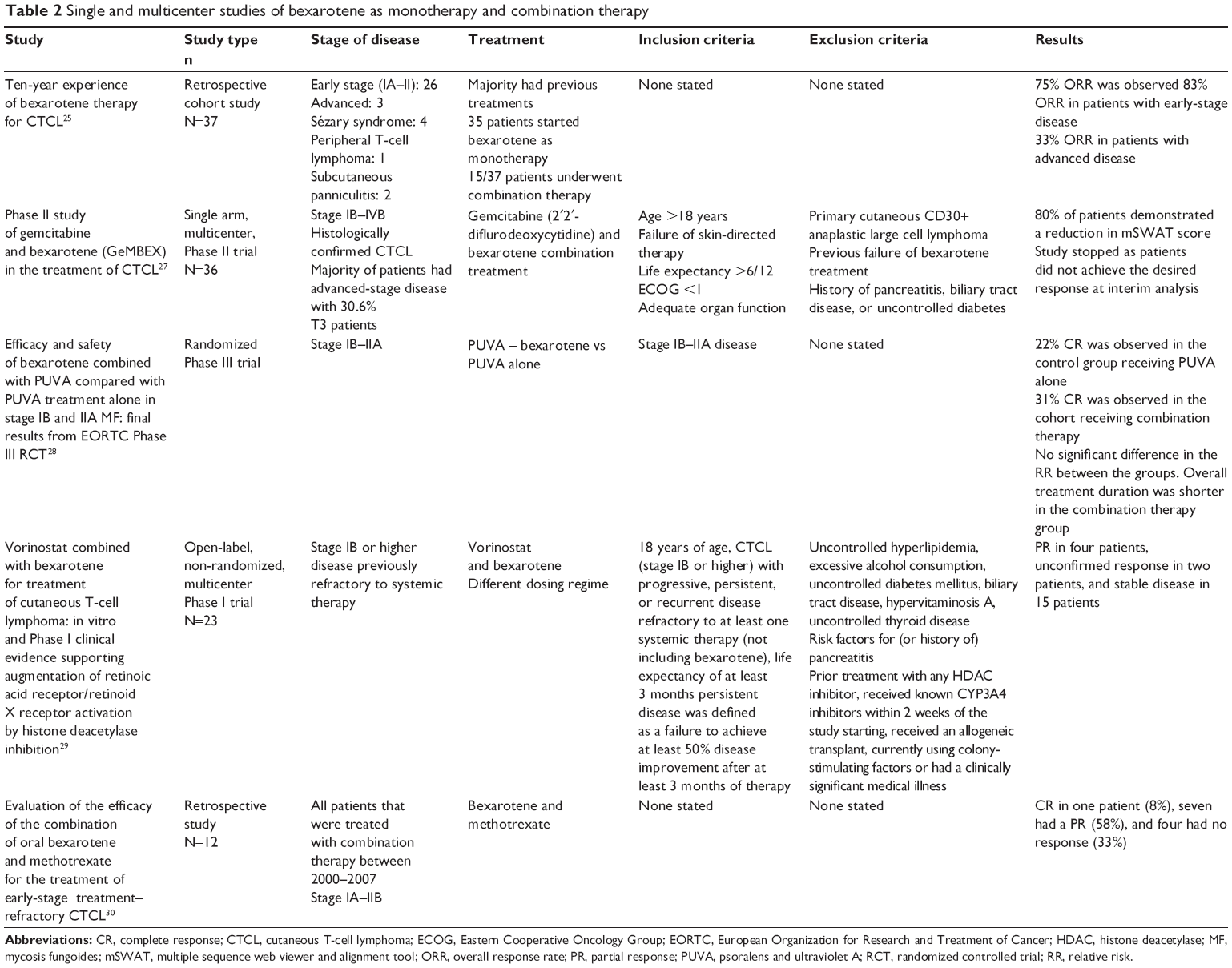 | Table 2 Single and multicenter studies of bexarotene as monotherapy and combination therapy |
Talpur et al evaluated 70 patients treated with oral bexarotene. The overall response rate (RR) was 48% and was higher in early-stage disease (RR: 53%) compared to advanced stages (RR: 46%). Four patients receiving monotherapy had a complete response (CR) of greater than 3 years’ duration and received maintenance dosing. When bexarotene was combined with other active CTCL therapies, higher RRs were achieved in patients with advanced disease, without unacceptable side effects.22
Abbott et al performed a retrospective study on 66 patients treated with bexarotene therapy for early (IB–IIA) and advanced (IIB–IVB) CTCL. Fifty-two out of 66 (79%) patients completed over 1 month of therapy with an intention-to-treat response rate of 44% (29/66). Nine percent had CR and 35% had PR. Median time to maximal response was 3 months (1–9 months) and median response duration was 8 months (1 to >48 months). Responses were seen in all stages and were higher in advanced stages. Responses were seen in skin, blood, and lymph nodes.23
Väkevä et al reported their 10-year experience of using bexarotene therapy for CTCL in 37 Finnish patients. Dose ranged between 75–675 mg/day. Seventy-five percent of the patients achieved an ORR that was higher in early-stage disease; 83% of patients with early-stage disease were responders compared to 33% with advanced disease.25
Quéreux et al reported on 32 patients with CTCL treated with bexarotene. A clinical response was reported in 60%, with a median response duration of 16 months. Responses were similar in early- and late-stage disease. Treatment for over 5 years was safely administered.26
Bexarotene combination therapy
Bexarotene has been used with various combinations of anti-CTCL therapies. Typically, this has been PUVA, interferon alpha, and ECP.22,25,27–30 Triple therapy with interferon and ECP is in widespread use for erythrodermic disease. Other combinations include vorinostat, methotrexate, denileukin diftitox, and gemcitabine. Many of these studies were retrospective and involved small patient numbers from single institutions. Furthermore, these studies lack a validated scoring system to assess tumor burden and data regarding the duration of response and disease-free survival (DFS)/overall survival (OS). However, more recently, prospective studies have been undertaken, which are discussed below.27–29 Such combinations appear safe but have not shown a credible increase in response rates.
Whittaker et al assessed the use of bexarotene in combination with PUVA compared to PUVA alone in early-stage disease (IA–IIA). This randomized Phase III study included 87 treated patients. Forty-one of 87 received PUVA and 46/47 received PUVA and bexarotene. The ORR was high at 71% for PUVA alone and 77% in the combination arm. Median duration of response was 9.7 months and 5.8 months, respectively. No significant difference in response rate was observed in both groups (P=0.57); however, fewer sessions of PUVA were required in the combination arm of the study.28
In a prospective Phase I/II trial of bexarotene and vorinostat in 23 patients with advanced refractory CTCL, the ORR was only 26%, which was not superior to results from trials that tested the individual substances; also, a high rate of adverse events and severe adverse events were observed.25,29
Illidge et al conducted a Phase II combination study of gemcitabine (pyrimidine antimetabolite) and bexarotene in the treatment of CTCL. Both of these medications are used in combination in a clinical setting. The study hypotheses were that gemcitabine would reduce the burden of disease and bexarotene would improve the quality and durability of clinical response. Patients that had failed skin-directed therapy and one systemic agent with stage IB–IVB biopsy–proven CTCL were included in the study. Modified skin severity assessment tool (mSWAT) and imaging studies were used to accurately calculate response rate. An ORR of 31% was observed at 12 weeks and 14% at 24 weeks. The trial did not proceed to the second stage as at interim analysis the response rates failed to reach the criteria for trial continuation.27 Complete remissions were not observed in this trial. The authors report that the management of bexarotene-induced hyperlipidemia necessitated dose reductions or the cessation of bexarotene treatment.27
A Phase I/II study of relapsed or refractory MF in 14 patients treated with pralatrexate at 15 mg/m2/week for three of 4 weeks combined with 150–300 mg/m2 of daily oral bexarotene found response rates of 50%. Pralatrexate in combination with low-dose oral bexarotene was well-tolerated and capable of providing long-term responses in patients of advanced-stage MF.31
A Phase I trial of bexarotene and denileukin diftitox in 14 patients with relapsed or refractory CTCL treated with escalating doses of bexarotene (75–300 mg/day) and denileukin diftitox (18 μg/kg per day ×3 days every 21 days) found an ORR of 67% (four CR, four PR). This combination was well-tolerated, with leukopenia being the predominant side effect.32
Discussion
Bexarotene is a safe and effective treatment for advanced refractory MF/SS. Side effects are predictable, dose-related, and may be managed safely by following published algorithms for safe prescribing.20 Patients should be counseled on following a low-fat diet and contraception advice (1 month before to 1 month after therapy). They must be aware that regular blood monitoring and additional therapy with thyroxine and lipid-lowering therapy are mandatory.
After historical use of combinations of retinoids with phototherapy and interferon alpha in MF/SS, bexarotene was used in combination with these therapies, but many studies are retrospective and lack well-defined endpoints. It is most likely that those patients with refractory disease received combinations to try and improve efficacy, which makes it difficult to compare response rates to monotherapy. More recently, a number of well-controlled prospective studies involving combination with PUVA, gemcitabine, vorinostat, denileukin diftitox, and pralatrexate have been published. Although these bexarotene combinations are generally well-tolerated, no synergistic activity has been shown to significantly increase response rates, and optimal combinations have not yet been identified.
Conclusion
Bexarotene remains a valued therapy for advanced MF/SS, with activity in early refractory disease as well as advanced disease.
Disclosure
JS has received honoraria and meeting sponsorship from Teva. The other authors report no conflicts of interest in this work.
References
Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphoma. Blood. 2005;105(10):3768–3785. | ||
Olsen E, Vonderheid E, Pimpinelli N, et al; ISCL/EORTC. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713–1722. | ||
Whittaker SJ, Marsden JR, Spittle M, Russell Jones R; British Association of Dermatologists; U.K. Cutaneous Lymphoma Group. Joint British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous T-cell lymphomas. Br J Dermatol. 2003;149(6):1095–1107. | ||
Trautinger F, Knobler R, Willemze R, et al. EORTC consensus recommendations for the treatment of mycosis fungoides/Sézary syndrome. Eur J Cancer. 2006;42(8):1014–1030. | ||
Willemze R, Hodak E, Zinzani PL, Specht L, Ladetto M; ESMO Guidelines Working Group. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6:vi149–vi154. | ||
National Comprehensive Cancer Network [webpage on the Internet]. NCCN Clinical Practice Guidelines in Oncology (NCCN guidelines): Non Hodgkin’s Lymphomas. Version 4. 2014. Available from: http://www.nccn.org/professionals/physician_gls/pdf/nhl.pdf. Accessed September 6, 2014. | ||
Sugaya M, Hamada T, Kawai K. Guidelines for the management of cutaneous lymphomas (2011): a consensus statement by the Japanese Skin Cancer Society – Lymphoma Study Group. J Dermatol. 2013;40(1):2–14. | ||
Humme D, Nast A, Erdmann R, Vandersee S, Beyer M. Systematic review of combination therapies for mycosis fungoides. Cancer Treat Rev. 2014;40(8):927–993. | ||
Lechowicz MJ, Lazarus HM, Carreras J, et al. Allogeneic hematopoietic cell transplantation for mycosis fungoides and Sezary syndrome. Bone Marrow Transplant. 2014;49(11):1360–1365. | ||
Duarte RF, Boumendil A, Onida F, et al. Long-term outcome of allogeneic hematopoietic cell transplantation for patients with mycosis fungoides and Sézary syndrome: a European society for blood and marrow transplantation lymphoma working party extended analysis. J Clin Oncol. 2014;32(29):3347–3348. | ||
Jacobsen ED, Kim HT, Ho VT, et al. A large single-center experience with allogeneic stem-cell transplantation for peripheral T-cell non-Hodgkin lymphoma and advanced mycosis fungoides/Sezary syndrome. Ann Oncol. 2011;22(7):1608–1613. | ||
Molina A, Zain J, Arber DA, et al. Durable clinical, cytogenetic, and molecular remissions after allogeneic hematopoietic cell transplantation for refractory Sezary syndrome and mycosis fungoides. J Clin Oncol. 2005;23(25):6163–6171. | ||
Duarte RF, Canals C, Onida F, et al. Allogeneic hematopoietic cell transplantation for patients with mycosis fungoides and Sézary syndrome: a retrospective analysis of the Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. J Clin Oncol. 2010;28(29):4492–4499. | ||
Electronic Medicines Compendium [webpage on the Internet]. Targetin Capsules [updated April 4, 2013]. Available from: https://www.medicines.org.uk/emc/medicine/26618. Accessed September 6, 2014. | ||
Boehm MF, Zhang L, Badea BA, et al. Synthesis and structure-activity relationships of novel retinoid X receptor-selective retinoids. J Med Chem. 1994;37(18):2930–2941. | ||
Duvic M, Martin AG, Kim Y, et al; Worldwide Bexarotene Study Group. Phase 2 and 3 clinical trial of oral bexarotene (Targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma. Arch Dermatol. 2001;137(5):581–593. | ||
Zhang C, Hazarika P, Ni X, Weidner DA, Duvic M. Induction of apoptosis by bexarotene in cutaneous T-cell lymphoma cells: relevance to mechanism of therapeutic action. Clin Cancer Res. 2002;8(5):1234–1240. | ||
Budgin JB, Richardson SK, Newton SB, et al. Biological effects of bexarotene in cutaneous T-cell lymphoma. Arch Dermatol. 2005;141(3):315–321. | ||
Richardson SK, Newton SB, Bach TL, et al. Bexarotene blunts malignant T-cell chemotaxis in Sezary syndrome: reduction of chemokine receptor 4-positive lymphocytes and decreased chemotaxis to thymus and activation-regulated chemokine. Am J Hematol. 2007;82(9):792–797. | ||
Scarisbrick JJ, Morris S, Azurdia R, et al. U.K. consensus statement on safe clinical prescribing of bexarotene for patients with cutaneous T-cell lymphoma. Br J Dermatol. 2013;168(1):192–200. | ||
Assaf C, Bagot M, Dummer R, et al. Minimizing adverse side-effects of oral bexarotene in cutaneous T-cell lymphoma: an expert opinion. Br J Dermatol. 2006;155(2):261–266. | ||
Talpur R, Ward S, Apisarnthanarax N, Breuer-Mcham J, Duvic M. Optimizing bexarotene therapy for cutaneous T-cell lymphoma. J Am Acad Dermatol. 2002;47(5):672–684. | ||
Abbott RA, Whittaker SJ, Morris SL, et al. Bexarotene therapy for mycosis fungoides and Sézary syndrome. Br J Dermatol. 2009;160(6):1299–1307. | ||
Duvic M, Hymes K, Heald P, et al; Bexarotene Worldwide Study Group. Bexarotene is effective and safe for treatment of refractory advanced-stage cutaneous T-cell lymphoma: multinational phase II-III trial results. J Clin Oncol. 2001;19:2456–2471. | ||
Väkevä L, Ranki A, Hahtola S. Ten-year experience of bexarotene therapy for cutaneous T-cell lymphoma in Finland. Acta Derm Venereol. 2012;92(3):258–263. | ||
Quéreux G, Saint-Jean M, Peuvrel L, Brocard A, Knol AC, Dréno B. Bexarotene in cutaneous T-cell lymphoma: third retrospective study of long-term cohort and review of the literature. Expert Opin Pharmacother. 2013;14(13):1711–1721. | ||
Illidge T, Chan C, Counsell N, et al. Phase II study of gemcitabine and bexarotene (GEMBEX) in the treatment of cutaneous T-cell lymphoma. Br J Cancer. 2013;109(10):2566–2573. | ||
Whittaker S, Ortiz P, Dummer R, et al. Efficacy and safety of bexarotene combined with psoralen-ultraviolet A (PUVA) compared with PUVA treatment alone in stage IB-IIA mycosis fungoides: final results from the EORTC Cutaneous Lymphoma Task Force phase III randomized clinical trial (NCT00056056). Br J Dermatol. 2012;167(3):678–687. | ||
Dummer R, Beyer M, Hymes K, et al. Vorinostat combined with bexarotene for treatment of cutaneous T-cell lymphoma: in vitro and phase I clinical evidence supporting augmentation of retinoic acid receptor/retinoid X receptor activation by histone deacetylase inhibition. Leuk Lymphoma. 2012;53(8):1501–1508. | ||
Kannangara AP, Levitan D, Fleischer AB Jr. Evaluation of the efficacy of the combination of oral bexarotene and methotrexate for the treatment of early stage treatment-refractory cutaneous T-cell lymphoma. J Dermatol Treat. 2009;20(3):169–176. | ||
Talpur R, Thompson A, Gangar P, Duvic M. Pralatrexate alone or in combination with bexarotene: long-term tolerability in relapsed/refractory mycosis fungoides. Clin Lymphoma Myeloma Leuk. 2014;14(4):297–304. | ||
Foss F, Demierre MF, DiVenuti G. A phase-1 trial of bexarotene and denileukin diftitox in patients with relapsed or refractory cutaneous T-cell lymphoma. Blood. 2005;106(2):454–457. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.