")
Back to Journals » Clinical Ophthalmology » Volume 11
The use of Wavelight® Contoura to create a uniform cornea: the LYRA Protocol. Part 1: the effect of higher-order corneal aberrations on refractive astigmatism
Authors Motwani M
Received 3 February 2017
Accepted for publication 18 April 2017
Published 16 May 2017 Volume 2017:11 Pages 897—905
DOI https://doi.org/10.2147/OPTH.S133839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Manoj Motwani
Motwani LASIK Institute, San Diego, CA, USA
Purpose: To demonstrate how higher-order corneal aberrations can cancel out, modify, or induce lower-order corneal astigmatism.
Patients and methods: Six representative eyes are presented that show different scenarios in which higher-order aberrations interacting with corneal astigmatism can affect the manifest refraction. WaveLight® Contoura ablation maps showing the higher-order aberrations are shown, as are results of correction with full measured correction using the LYRA (Layer Yolked Reduction of Astigmatism) Protocol.
Results: Higher-order corneal aberrations such as trefoil, quadrafoil, and coma can create ovalization of the central cornea, which can interact with the ovalization caused by lower-order astigmatism to either induce, cancel out, or modify the manifest refraction. Contoura processing successfully determines the linkage of these interactions resulting in full astigmatism removal. Purely lenticular astigmatism appears to be rare, but a case is also demonstrated. The author theorizes that all aberrations require cerebral compensatory processing and can be removed, supported by the facts that full removal of aberrations and its linkage with lower-order astigmatism with the LYRA Protocol has not resulted in worse or unacceptable vision for any patients.
Conclusion: Higher-order aberrations interacting with lower-order astigmatism is the main reason for the differences between manifest refraction and Contoura measured astigmatism, and the linkage between these interactions can be successfully treated using Contoura and the LYRA Protocol. Lenticular astigmatism is relatively rare.
Keywords: topographic guided ablation, LASIK, PRK, WaveLight Contoura, uniform cornea, higher order aberrations
Introduction
The nature of the effects of higher-order corneal aberrations on lower-order corneal astigmatism has until now been poorly understood. If the corneal astigmatism differed from the manifest astigmatism, it was usually diagnosed as lenticular astigmatism through a process of exclusion. Some authors have also performed studies to show that the posterior surface of the cornea can also cause astigmatism, but the amount of induction of astigmatism has been relatively small (on the order of a fraction of a diopter).1–3
Topography-guided ablation, market name Contoura on the WaveLight® excimer lasers (WaveLight, Erlangen, Germany), has added yet another element of uncertainty. Often the manifest refraction (cyclopleged or not) and the autorefraction do not correspond with the astigmatism that Contoura processing results in. In parts 2 and 3 of this series, the author has shown that correcting with Contoura processing through the LYRA (Layer Yolked Reduction of Astigmatism) Protocol results in correction of astigmatism in virtually all cases, and has also demonstrated that treatment on the wrong manifest astigmatism axis can result in loss of effectiveness of astigmatism correction and also induction of a whole new astigmatism on an oblique axis.4,5
We examined patients who had a significant difference between manifest refraction and Contoura measured astigmatism in an effort to delineate the reasons for induction, modification, and reduction of astigmatism by the corneal aberrations. Our hypothesis was that the higher-order aberrations (HOAs) were directly modifying the lower-order astigmatism in such a way as the combination of the distortion of the two necessitated the cortical processing to pick a point of “least confusion,” resulting in a manifest refraction that was often significantly different from the Contoura measured astigmatism/axis.
Figure 1 shows how with-the-rule and against-the-rule create an oval-shaped central cornea. The arrows show the direction of the “bowtie.” This demonstrates the ovalization caused by these two types of lower-order astigmatism.
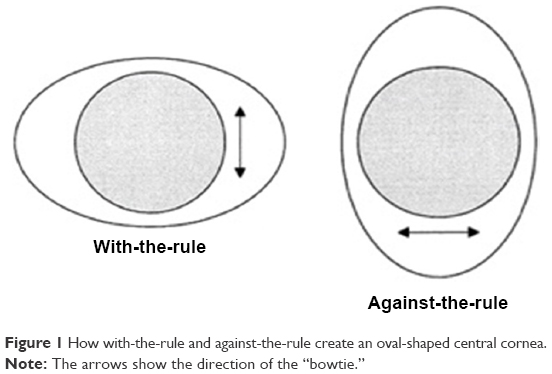 | Figure 1 How with-the-rule and against-the-rule create an oval-shaped central cornea. |
Patients and methods
An analysis was performed by the author in patients who had full Contoura measured correction performed as per the LYRA Protocol, which allows for Contoura processing to determine the linkage in between the aberration correction layer and the refraction correction layer. The LYRA Protocol is as follows:
- Enter the manifest/cycloplegic refraction into Contoura during presurgical planning.
- Zero out the astigmatism and sphere to see ablation pattern for the aberration correction layer.
- Enter Contoura measured astigmatism and axis for the final correction. The ablation map at this point should be similar to the Pentacam anterior elevation map. This will assist understanding the ablation when there is a significant discrepancy between manifest versus measured astigmatic power and axis.
- The sphere is now entered after adjustment for the spherical equivalent of the change in astigmatism.
Aberration correction was visualized on the treatment planning page of Contoura by zeroing out the refraction, and displaying Contoura correction of the aberration. This can only be done in the Contoura surgical planning software. The change of shape to the central cornea was determined using this method, and comparison against the manifest refraction astigmatism and axis was performed. The examination of a large number of eyes resulted in six categories where manifest astigmatism was different from corneal astigmatism. Those categories are listed below.
All patients were analyzed using the Topolyzer Vario, and all patients had correction by one surgeon (MM) at one center using the WaveLight® EX500 system with Contoura and the WaveNet server.
As part of this analysis, patients had cyclopleged manifest refractions performed to rule out the existence of lenticular accommodation of astigmatism. For purposes of this paper, a “manifest refraction” will be a cyclopleged one, essentially the refraction that we obtain using the phoropter with patient subjective input.
All cases below each have a preoperative topography, postoperative topography, and aberration ablation pattern to determine the type of aberration. The aberration ablation pattern was obtained by the method described above.
All patients provided written consent to have their data published in this paper.
Results
Case 1: corneal aberration induction of manifest astigmatism (Figure 2)
- Preoperative manifest refraction: −1.00, −2.75×8 with best-corrected visual acuity (BCVA) of 20/20
- Preoperative autorefraction: −0.50, −2.50×171
- Measured Contoura correction: −1.40, −2.00×1
- Postoperative refraction and vision at 3 months: plano; 20/15.
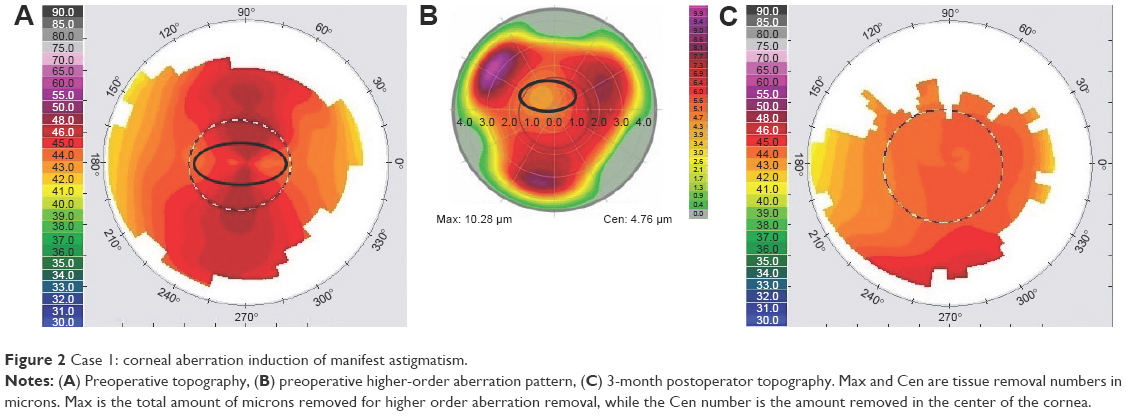 | Figure 2 Case 1: corneal aberration induction of manifest astigmatism. |
In this case, the HOA creates an oval that adds to the lower-order astigmatism oval, increasing the manifest astigmatism. When the HOA is treated, the amount of astigmatism correct is decreased as demonstrated by the Contoura measured correction and postoperative result.
Case 2: corneal aberration cancellation of manifest astigmatism (Figure 3)
- Preoperative manifest refraction: −1.50 with BCVA of 20/20
- Preoperative autorefraction: −2.00
- Measured Contoura correction: −1.12, −0.77×121
- Postoperative refraction and vision at 1 week: plano; 20/15.
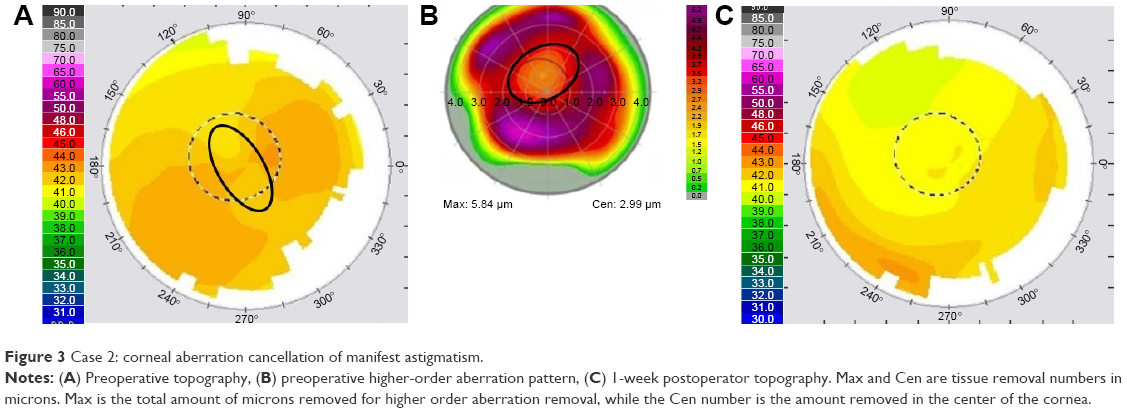 | Figure 3 Case 2: corneal aberration cancellation of manifest astigmatism. |
This particular patient had his entire lower-order astigmatism completely cancelled out by the HOA, resulting in a manifest refraction with no astigmatism (no astigmatism on the autorefraction also). The oval caused by the lower-order astigmatism is oblique (oblique astigmatism has only been seen rarely by us), as is the ovalization created by the HOAs, and the two ovals completely cancel each other out during manifest refraction. Removing the HOA reveals the lower-order astigmatism underneath, which can be recognized as “bowtie” astigmatism on the cornea.
Case 3: corneal aberration cancellation via oblique aberration and cerebral processing (Figure 4)
- Preoperative manifest refraction: −2.75 with BCVA of 20/20
- Preoperative autorefraction: −3.75, −0.25×150
- Measured Contoura correction: −2.40, −0.77×1
- Postoperative refraction and vision at 1 month: −0.25; 20/15.
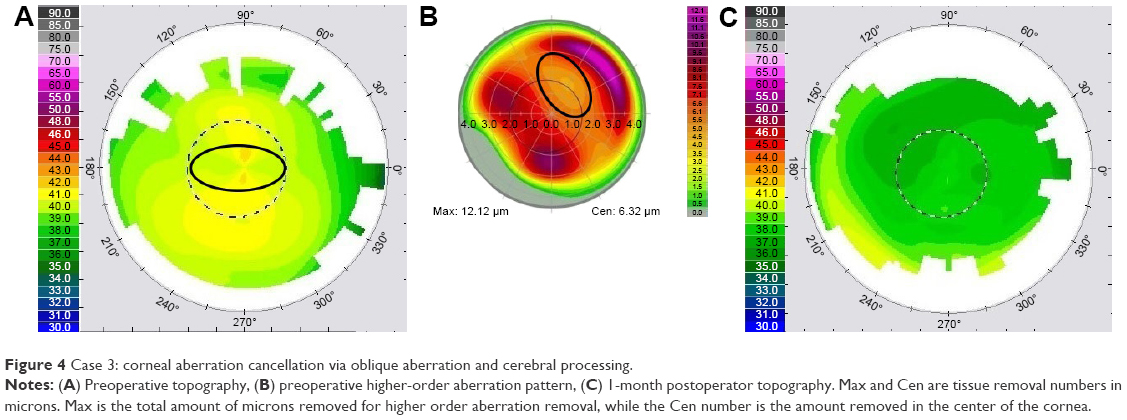 | Figure 4 Case 3: corneal aberration cancellation via oblique aberration and cerebral processing. |
This patient shows with-the-rule astigmatism on topography, but has a manifest refraction and autorefraction that essentially shows no astigmatism. The ablation pattern shows correction of trefoil, but the oval created is not along the axis expected to cancel out the corneal lower-order astigmatism. It is at an oblique angle. The other eye of this patient had a similar with-the-rule astigmatism on topography, similar lack of astigmatism of manifest and autorefraction, but the aberration oval was perpendicular to the lower-order astigmatism and clearly cancelled it out. This one is at an oblique angle, so it appears that somehow the patient’s cerebral processing is working similar to the other eye, but somehow still cancelling out the astigmatism with an oblique aberration. It is difficult to see how even examining this aberration in three dimensions would somehow create an ovalization that was directly perpendicular to the oval created by the lower-order “bowtie” astigmatism.
The result of Contoura measured correction resulted in 20/15 vision with all astigmatism removed in both eyes.
Case 4: aberration induction of astigmatism with dilation of the pupil (Figure 5)
- Preoperative manifest refraction: −7.75, −1.00×75 with BCVA of 20/20
- Preoperative autorefraction: −8.00, −0.75×75
- Measured Contoura correction: −8.00, −0.07×121
- Postoperative refraction and vision at 1 month: plano; 20/15.
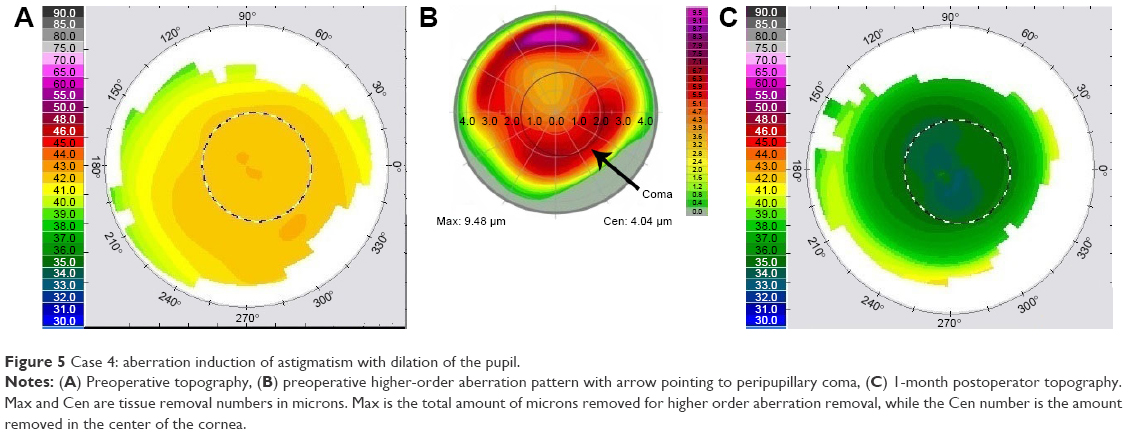 | Figure 5 Case 4: aberration induction of astigmatism with dilation of the pupil. |
This patient has coma directly adjacent to the pupil, causing manifest refraction and autorefraction of astigmatism. The presence of this “high spot” peripupillary coma creates a localized distortion and astigmatism on manifest refraction. Removal of that coma completely eliminates the astigmatism and essentially leaves sphere. The sphere was corrected resulting in a uniform-looking cornea and 20/15 vision.
Case 5: oblique manifest astigmatism induced by corneal aberration (Figure 6)
- Preoperative manifest refraction: −2.50, −0.50×155 with BCVA of 20/20
- Preoperative autorefraction: −2.75, −0.50×142
- Measured Contoura correction: −2.00, −1.50×1
- Postoperative refraction and vision at 1 month: plano; 20/15.
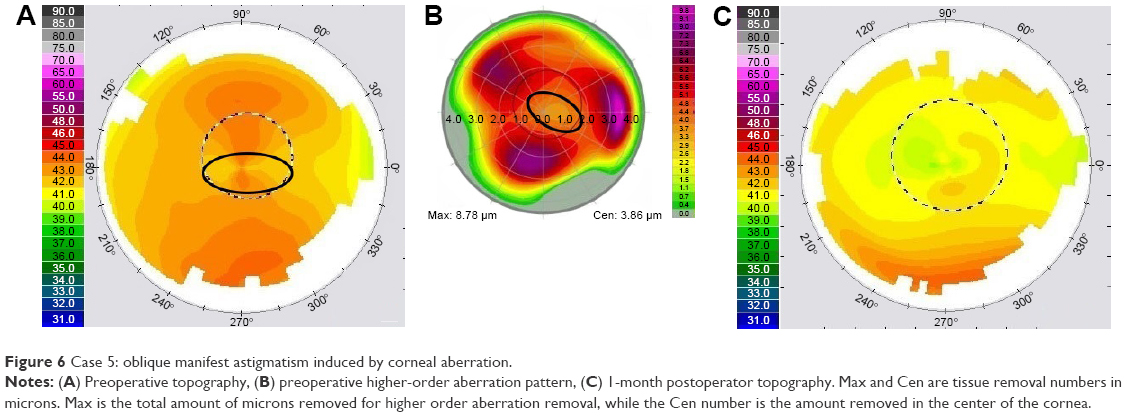 | Figure 6 Case 5: oblique manifest astigmatism induced by corneal aberration. |
This patient has an obvious with-the-rule “bowtie” astigmatism, yet both manifest and autorefraction show an oblique astigmatism of a much smaller magnitude. In this particular case the trefoil is creating an oval that is at an oblique angle cancelling out the with-the-rule astigmatism and also creating an oblique astigmatism. Removing the aberration results in 1.50 D of with-the-rule astigmatism. The topography shows signs of the epithelium still becoming uniform from epithelial molding to the aberration. This will likely smooth out 3–6 months postprocedure.
Case 6: pure lenticular astigmatism (Figure 7A–C)
 | Figure 7 (A) Case 6: topolyzer topography of patient. (B) Case 6: Contoura surgical planning page showing higher-order aberration pattern and measured astigmatism. (C) Case 6: wavefront scan showing higher amount of astigmatism. |
This case has a wavefront measured astigmatism of −3.5 D at 84 degrees, a manifest astigmatism of −1.75 D at 90 degrees, and a Contoura measured astigmatism of −1.49 D at 81 degrees. The Contoura measured astigmatism is very close to the manifest astigmatism, while the wavefront shows a much higher amount of measured astigmatism. In this case, the corneal aberration is cancelling out astigmatism that can only be coming from the lens, and treating the Contoura measured will reveal astigmatism from the lens. The diagnosis of such a case is best done with wavefront measurement, and treatment of residual astigmatism can either be done with wavefront-guided or likely even wavefront-optimized correction. If the surgeon elects to treat, they must inform the patient of the need for re-treatment if cataract surgery is ever necessary.
Discussion
This understanding of how HOAs affect lower-order astigmatism came about as an attempt to understand why the LYRA Protocol using the measured Contoura astigmatism is effective. Different theories were examined, but the underlying fact was that using the LYRA Protocol eliminated astigmatism, and resulted in good vision even when the manifest astigmatism/axis differed markedly from the Contoura measured astigmatism/axis. Over time, examining the HOA pattern of patients in relation to their lower-order astigmatism, and the changes from manifest refraction to Contoura measured led to an understanding of how the HOAs were interacting with the lower-order astigmatism. Essentially, this understanding was “reverse-engineered” from the realization that the LYRA Protocol works and creates more uniform corneas.
The author initially considered the theory that lenticular accommodation of the cornea may exist to explain some of the differences between manifest and measured refraction. This would be where the lens is capable of accommodating in such a way as to correct or even cause astigmatism. This has never been proven to exist, but was a theory that was considered. Cycloplegia would actually provide a different astigmatism refraction that would be closer to or equivalent to the Contoura measured astigmatism if lenticular accommodation of astigmatism was present. Unfortunately, in no cases that the author examined was this demonstrated, and all patients considered for this analysis had cyclopleged refractions to rule out any accommodative aspect. What we have theorized is that peripheral or central HOAs create an ovalization in the central cornea (within the mesopic pupil), resulting in a deformed central ray of light forming a lower-order astigmatism. Therefore, the manifest refraction is a result of the oval shapes created by lower-order and higher-order astigmatism and its resulting central ray of light interaction. Corneal lower-order astigmatism essentially creates an oval shape in the center of the cornea, as shown in the figures. Corneal aberrations such as trefoil and quadrafoil can also create an oval shape to the central cornea, and depending on how the two ovals of higher-order and lower-order aberration line up, it will either increase or decrease the manifest measurement of astigmatism.
The author further theorizes that the central ray of light forms the main part of vision, and the refraction requested by the patient achieves the best possible correction that minimizes cerebral confusion via the addition of spherical or astigmatism glass correction. This visual impression of the patient is widely determined by the shape formed by low- and high-order aberrations that pass the central portion of the cornea and form the related focusing at the retinal level. Aberrations located at the periphery will influence the overall quality of vision. Spherical aberration, for example, is understood to affect night vision. It adds or reduces the amount of refraction (depending on the orientation of the spherical aberration) when the pupil widens. The dilated pupil allows the pre-existent HOA to become dominant and change the focus quality at the retinal level. This paper in contrast seeks to demonstrate that HOAs can also affect the visual impression of the patient. Furthermore, the autorefractometer might not be able to detect the difference between HOA and lower-order aberration, because it measures only the central 2 mm of the cornea and, therefore, the ray of light deformed by the lower-order aberrations and HOAs.
What we have observed across the examination of many patients is that the majority of HOAs are trefoil, with a lesser amount of quadrafoil, and coma. When the aberration is examined using the treatment planning page, it was possible in some cases to see the oval created by the aberration and how it impacted the actual corneal astigmatism. Unfortunately, aberrations are not two dimensional, they are three dimensional and the ovals simply do not line up in all two-dimensional ablation maps.
Contoura with LYRA Protocol results in many cases with a completely different measured astigmatism and axis versus the manifest. In the author’s experience, performing this procedure has not worsened patients’ vision, which would occur if the hypotheses presented here were incorrect. The author surmises that it is cerebral processing that compensates for the distortion caused by HOAs. The cerebral cortex must interpolate information where it becomes distorted by an HOA, and removal of that HOA would remove the need for that interpolation. Although there has been some conjecture in the past that some aberrations may be good, that is, as in fighter pilots that have 20/10 vision and HOAs, the author believes that the high resolution for the 20/10 vision comes from a high density of photoreceptors in the retina in these individuals, and a fighter pilot’s or baseball player’s high capabilities in dynamic vision testing are due to rapid cerebral interpolation to compensate for distortion created by HOAs. If this is the case, then removal of the HOAs on a person who is already 20/10 would result not in better Snellen visual acuity (which would be limited by retinal photoreceptor density in the macula), but in faster response times as cerebral processing/interpolation would no longer be necessary. Furthermore, the ability to clearly see the edges of objects would allow for faster “locking in” by the brain for dynamic motion, likely resulting in better response time to a 95 mile per hour fastball or a fast flying opposing fighter that require responses in the milliseconds. The author now postulates that there is no such thing as a “good” aberration, but essentially all aberrations are bad and require cerebral processing to compensate for them. Treating these HOAs to make a more uniform cornea will simply allow a clear path of light that will not need to be compensated for.
At this point, it should be mentioned that too much emphasis can be placed on the Snellen visual acuity. We have all seen 20/15 patients who are not happy, and we have treated patients for halos who are clearly 20/15 but have 0.5 D of astigmatism and complain about their night vision. Treating that residual astigmatism significantly improves the night time vision and decreases halos. In our experience, a patient who is 20/20 without halos is happier than a 20/15 with halos. An eye with 20/15 or 20/10 vision after laser correction means that the treatment allowed the retina to more fully achieve its resolution, but it does not guarantee that aberrations or incomplete treatment of the cornea will not result in a patient who is not completely happy.
For purposes of visualization, with-the-rule astigmatism essentially results in a horizontally oval cornea. If the aberration also creates an oval that is horizontal, the manifest astigmatism will be greater than the corneal astigmatism. If the aberration creates a vertical oval on the same type of cornea, the manifest astigmatism will be cancelled out or less than the corneal astigmatism. Depending on the axes of the two “ovals” the manifest and measured axis may be significantly different also. With further refinement of the Contoura software, we would be able to specifically quantify the axis of the oval created by the aberration, as we can quantify the axis created by lower-order corneal astigmatism, and with that create a vector diagram that can accurately predict the axis. This would be interesting for demonstrative purposes, but in essence Contoura does it for us by giving us the final result of astigmatism and axis by calculating this interaction.
The author understands that separating these interactions as has been done in this paper is artificially attempting to break down complex three-dimensional interactions between the HOA and the lower-order astigmatism into a two-dimensional image for illustration purposes. We do not expect to find these interactions in every single case, but in many cases this interaction can be visualized. The main takeaway from these cases is that the interactions are mainly corneal in nature, and rarely involve the lens as has been postulated for many years via data from wavefront maps.
Cases 1 and 2 essentially demonstrate either cancellation or induction of astigmatism with ovalization created by the HOAs that is either on the same axis or perpendicular to the oval created by the lower-order astigmatism.
Case number 3 demonstrated a different sort of issue, where the oval shape created by the aberration was oblique to the axis of the corneal astigmatism, yet seemed to fully cancel it out. This is a case we cannot fully explain via corneal factors. This patient also did not display any astigmatism on cyclopleged refraction, or autorefraction. Although it is possible that the oval created centrally is not as oblique as the overall shape of the trefoil aberration in his cornea, we think just as likely it may be that cerebral processing is involved. This patient’s other eye had a textbook cancellation of with-the-rule astigmatism by corneal aberration. It may very well be that there was partial compensation of the astigmatism in case 3 by the aberration, and partial compensation of the corneal astigmatism via cerebral processing. We know that manifest refraction is based simply on the point of least confusion of vision, and we know that what we “see” is actually subject to cerebral processing.
This particular case was an anomaly, and the only one that the author has seen like this, where it seems cerebral processing somehow allowed an oblique aberration to cancel out a regular with-the-rule astigmatism. In this case, it is difficult to see even how examining this aberration in three dimensions would somehow create an ovalization that was directly perpendicular to the oval created by the lower-order “bowtie” astigmatism. In case 5, we also demonstrate a case where an oblique aberration appears to cancel out a with-the-rule lower-order astigmatism. In that case, an oblique astigmatism is created on manifest refraction. In this case, there is no oblique astigmatism on manifest refraction, just a complete cancellation of with-the-rule astigmatism. Cerebral processing is responsible for Figure 5, where the lines do not look parallel but actually are. This type of simple drawing is an example of how cerebral processing can be used to alter how we “see” things.
Case 4 demonstrates how coma peripheral to the pupil can result in incorrect measurement of astigmatism in a dark room with a mydriatic pupil, or during cyclopleged refraction. Correction of this astigmatism results would lead to an incorrect result, as there is no actual astigmatism, but a localized distortion created by the “high spot” of the peripupillary coma. Such a patient may have decreased or no manifest astigmatism with a meiotic pupil, as the pupil may close enough to decrease or eliminate the distortion created by the coma. Removal of the coma results in a cornea that has no astigmatism on either manifest or cyclopleged refraction. Not only can the coma cause a manifest astigmatism, but it can also change the axis of astigmatism of an actual lower-order corneal astigmatism, resulting in an incorrect treatment. This particular patient had astigmatism at an oblique axis on manifest, cyclopleged manifest, and also autorefraction. Contoura measured showed no astigmatism at all, supported by the fact that no lower-order astigmatism is noted on the preoperative topography. Similar examples can be demonstrated with corneal keratoconus patients where the predominating aberration is coma (except in the case of central keratoconus).
Case 5 demonstrates how an oblique aberration oval changes the with-the-rule astigmatism noted on topography to an oblique manifest astigmatism. This case shows how the interaction between lower- and higher-order astigmatism can also end up with an oblique axis of astigmatism being created. In this particular case not only does the oblique oval created by the trefoil cancel out the with-the-rule astigmatism, but it also creates a tangential astigmatism at an oblique axis.
After observing the interactions between higher- and lower-order astigmatism over many Contoura with LYRA Protocol corrections, some observations have been made. The vast majority of lower-order astigmatism is actually either with- or against-the-rule, with an axis of astigmatism usually within ±15 degrees of the 90 degree and 180 degree axes. It appears that oblique manifest astigmatism seems to be mainly caused by either an oblique oval created by an aberration, or by peripupillary coma that affects the mydriatic and cyclopleged manifest measurements.
Case 6 demonstrates pure lenticular astigmatism. This patient has minimal lower- or higher-order corneal astigmatism, but has a manifest refraction showing astigmatism. This patient has not had laser vision correction performed.
Pure lenticular astigmatism appears to be more uncommon than originally thought. In the analysis of author MM’s patients, since performing Contoura with LYRA Protocol corrections, no patients had demonstrated lenticular astigmatism. Contributor SL has seen 4–5 eyes with lenticular astigmatism several years and thousands, of eyes examined. In all cases of lenticular astigmatism there was little to no corneal aberration or corneal astigmatism present, with significant astigmatism on manifest refraction. Such a case is presented here as case 6, and the author believes that such a case should be carefully approached as the center of lenticular astigmatism may be different than the center for wavefront-optimized or wavefront-guided treatment. Although theoretically a patient may exist with corneal aberration, corneal astigmatism, and lenticular astigmatism, neither the author nor the contributors have seen such a patient to this point. Such a patient would have residual astigmatism after all corneal aberrations and astigmatism were eliminated. Enhancement of such a patient could likely be done through wavefront-guided ablation, or even perhaps by wavefront-optimized ablation to eliminate residual astigmatism. The takeaway message, though, is that lenticular astigmatism is much less common than has been estimated. This has been a diagnosis of exclusion, as there was incomplete understanding of the nature of how HOAs interact with lower-order astigmatism.
While conducting literature searches for this paper, the author could not find a single study or paper proving lenticular astigmatism’s existence except for the report of an unusual patient. Literature searches concerning lenticular accommodation of astigmatism also found no evidence of such. Finally, studies that analyzed posterior corneal astigmatism demonstrated only very small amounts of astigmatism, on the order of small fractions of a diopter.1–3
Conclusion
Finally, it is important to note that Contoura is able to calculate the linkage between the HOAs and lower-order astigmatism. We do not regularly spend time finding the ovalization interactions between the HOAs and lower-order astigmatism. Contoura calculates this for us as we will demonstrate in Part 3 of this series.5
Acknowledgments
The author thanks Sissimos Lemonis (SL) for inspiration and collaboration and to Ron Pei, OD, for editing.
Author contribution
Dr MM was involved in the conception, design, data collection, analysis, and interpretation, as well as writing and critical revision of the paper.
Disclosure
Dr Motwani has received a grant from Alcon for a previous unrelated study. The Contoura system using the LYRA Protocol was developed by Dr Motwani in conjunction with Sissimos Lemonis of WaveLight® Lasers. The author reports no other conflicts of interest in this work.
References
Yamaguchi T, Ohnuma K, Tomida D, et al. The contribution of the posterior surface to the corneal aberrations in eyes after keratoplasty. Invest Ophthalmol Vis Sci. 2011;52(9):6222–6229. | ||
Oshika T, Tomidokoro A, Tsuji H. Regular and irregular refractive powers of the front and back surfaces of the cornea. Exp Eye Res. 1998;67(4):443–447. | ||
Nakagawa T, Maeda N, Kosaki R, et al. Higher-order aberrations due to the posterior corneal surface in patients with keratoconus. Invest Ophthalmol Vis Sci. 2009;50(6):2660–2665. | ||
Motwani M. The use of WaveLight® Contoura-measured astigmatism to create a uniform cornea: the LYRA Protocol part 2: the consequences of treating astigmatism on an incorrect axis via excimer laser. Clin Ophthalmol. In press 2017. | ||
Motwani M. The use of WaveLight® Contoura-measured astigmatism to create a uniform cornea: the LYRA Protocol part 3: results from 50 eyes. Clin Ophthalmol. In press 2017. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.