")
Back to Journals » Patient Preference and Adherence » Volume 17
The Treatment Satisfaction in Patients and Their Partners Treated with Low-Intensity Extracorporeal Shock Wave Therapy and Sildenafil: A Prospective Non-Randomized Controlled Study
Authors Wang D, Wang SJ, Li YJ, Liu CH, Li YQ, Zhang YS, Yan S
Received 30 November 2022
Accepted for publication 10 February 2023
Published 8 March 2023 Volume 2023:17 Pages 583—589
DOI https://doi.org/10.2147/PPA.S399776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Dong Wang,* Shi-Jun Wang,* Ying-Jie Li, Chun-Hui Liu, Yong-Qiang Li, Yin-Sheng Zhang, Su Yan
Department of Urology, Peking Union Medical College Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su Yan, Department of Urology, Peking Union Medical College Hospital, No. 1 of Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86 13801326306, Fax +86 10 69152520, Email [email protected]
Background: Phosphodiesterase 5 inhibitors (PDE5Is) and other more invasive options merely provide symptomatic relief rather than a permanent improvement in erectile dysfunction (ED), whereas the long-term improvement in ED via low-intensity extracorporeal shockwave therapy (Li-ESWT) has been confirmed. So far, no comparative study of sildenafil versus Li-ESWT has been conducted with respect to treatment satisfaction.
Objective: In this study, we aim to compare erectile function status and satisfaction rates in patients who received sildenafil or Li-ESWT for ED.
Methods: Patients complaining of ED were considered candidates. Participants chose to enter one of two active treatment groups according to their treatment intention—either a 9-week Li-ESWT regimen or 100 mg on-demand sildenafil. The erectile function was evaluated using the erectile function domain of the International Index of Erectile Function questionnaires (IIEF-EF), while the treatment satisfaction was evaluated using the Erectile Dysfunction Inventory of Treatment Satisfaction questionnaires (EDITS).
Results: We enrolled 72 participants in the study (42 in the Li-ESWT group and 30 in the sildenafil group). Patients in both groups were young men. Four weeks after the last session, the IIEF-EF score for Li-ESWT and sildenafil was 16.3± 5.5 and 18.3± 6.5 (P > 0.05), respectively. The total EDITS index of the patient version and the partner version were similar in the two groups. Among EDITS questions measuring overall satisfaction and efficacy duration, the score was higher in the Li-ESWT group.
Conclusion: We found that Li-ESWT may have better satisfaction than on-demand sildenafil for young ED patients. However, further studies are needed to determine the factors influencing satisfaction.
Keywords: erectile dysfunction, Erectile Dysfunction Inventory of Treatment Satisfaction, low-intensity extracorporeal shock wave therapy, sildenafil
Introduction
Erectile dysfunction (ED) is a condition that affects more than 50% of males aged 40–70 years.1 However, recent reports indicate that ED is widespread among young males.2 Moreover, ED is a shared sexual problem that has a significant impact on the sexual satisfaction of both, patients and their partners.3
Although phosphodiesterase 5 inhibitors (PDE5Is) are a huge step forward in the management of ED, they are far from flawless. Prominent shortcomings of PDE5Is are their non-universal success rate, absence of spontaneity, and life-long drug commitment.4 PDE5Is and other more invasive options merely provide symptomatic relief rather than a permanent improvement of the condition.5,6 The discontinuation rate with PDE5is remains very high, in addition to efficacy, partner satisfaction represented the most important reasons for PDE5i discontinuation.7
The major potential advantage of low-intensity extracorporeal shockwave therapy (Li-ESWT) is the promising restoration of the ability to have spontaneous erections.8,9 Improvement in erectile function using Li-ESWT to the corporal bodies has been validated in human clinical trials.10–12 However, no comparative study of sildenafil versus Li-ESWT has been conducted concerning the satisfaction aspect. Herein, we performed a comparative analysis of the two treatments using validated instruments to assess ED treatment satisfaction of both, patients and their partners.
Materials and Methods
Screening, Inclusion and Exclusion Criteria
This study is a prospective, non-randomized, controlled clinical trial. From April 2019 to April 2020, patients complaining of ED during a consultation at our andrology outpatient clinic were considered candidates. Inclusion criteria were men who had a complaint of ED for at least 6 months, were at least 18 years old, and were in stable relationships. During the first visit, subjects were screened according to the eligibility criteria and filled out the International Index of Erectile Function (IIEF) questionnaire.
Patients were excluded on the grounds of IIEF-EF score ≥ 26, anatomic penile deformation or penile prosthesis, unstable medical (including clinically significant hepatobiliary or renal disease, and unstable cardiovascular disease) or psychiatric condition, treatment with anticoagulants, a previous history of a neurological pathology, radical pelvic surgery, irradiations, as well as hypogonadism.
Patients with diverse pathogenesis, including psychogenic, organic, and mixed ED, were enrolled. The organic pathogenesis was characterized by symptoms such as diabetes, cardiovascular comorbidities, and negative nocturnal and morning erections. Participants with substantial psychological problems and nocturnal or morning erections were diagnosed as psychogenic. Rigiscan was used to record nocturnal penile tumescence and rigidity (NPTR) parameters. Men with both psychogenic and organic manifestations were diagnosed with mixed ED.
Study Protocol
After a 4-week washout period of past treatment, participants entered one of two active treatment groups—either 9-week Li-ESWT (treatment group) or 100 mg on-demand sildenafil therapy (control group) according to their intention of treatment. Erectile function was assessed by the erectile function domain of IIEF (IIEF-EF), which is sensitive to ED treatment. IIEF-EF score of ≤ 25 was defined as ED.13
For the Li-ESWT protocol, the treatment scheme entailed 2 sessions per week for 3 weeks and was repeated after a 3-week interval. Omnispec ED1000 (Medispec Ltd., Yehud, Israel) was used to produce low-intensity shock waves.10 Li-ESWT was applied in each treatment session for 3 min at 5 different penile anatomical sites (3 locations on the penile shaft and 2 on the penile crura). Each Li-ESWT session comprised of 300 shocks per treatment point at an energy density of 0.09 mJ/mm2 and a frequency of 120/min. For the sildenafil protocol, the participants self-administered sildenafil at a dose of 100 mg 1 hour before each event of intercourse.
The follow-up visit was scheduled 4 weeks after the final session, when participants completed the IIEF-EF and Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS) questionnaires. The study and treatment flow chart is presented in Figure 1. Erectile function improvement was evaluated using IIEF-EF. A 4-point improvement in IIEF-EF defined a positive result of minimal clinically important difference (MCID).14 The primary outcome was the satisfaction of the patients and their partners, as measured by EDITS.15
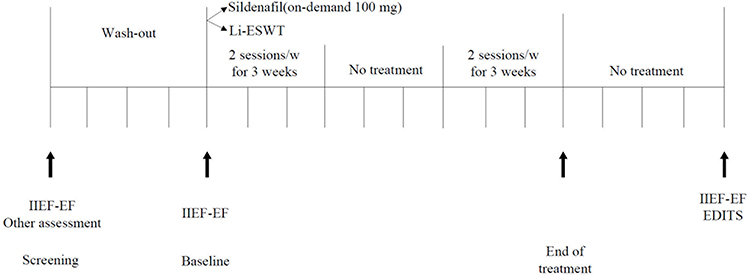 |
Figure 1 Patients flow chart. Abbreviations: Li-ESWT, low-intensity extracorporeal shock wave therapy; IIEF-EF, erectile function domain of International Index of Erectile Function questionnaire. |
Statistical Analysis
The baseline characteristics were compared using the Student’s t-test or Mann–Whitney U-test for quantitative variables, and the chi-square test for categorical variables. Descriptive statistics for the duration of disease in both groups were shown as median along with the 25th (P25) and 75th percentile (P75) due to skewed distribution, and the Mann–Whitney U-test was used to compare the differences in median levels for the duration of disease between both groups. The means of the overall IIEF-EF and the overall EDITS scores between the two treatment groups were compared using the Student’s t-test and further using the analysis of covariance for adjustment for appropriate potential confounding variables. Statistical significance was defined as P < 0.05. All data were analyzed using SPSS for Windows software (ver. 20.0; SPSS Inc., Chicago, IL, USA).
Results
Initially, a total of 126 patients were screened and met the inclusion criteria. Based on the exclusion criteria, 31 patients were then excluded, and 95 participants were recruited for the study. Follow-up was carried out from September 2019 to August 2020. Nine participants dropped out in the Li-ESWT group, and 14 participants dropped out in the sildenafil group. Overall, 72 patients and their partners were analyzed. The patient flow chart is presented in Figure 2. The patients in the two groups have similar demographic profiles except for age (31.2±5.2 in the sildenafil group vs 33.9±6.2 in the Li-ESWT group, P < 0.05) (Table 1).
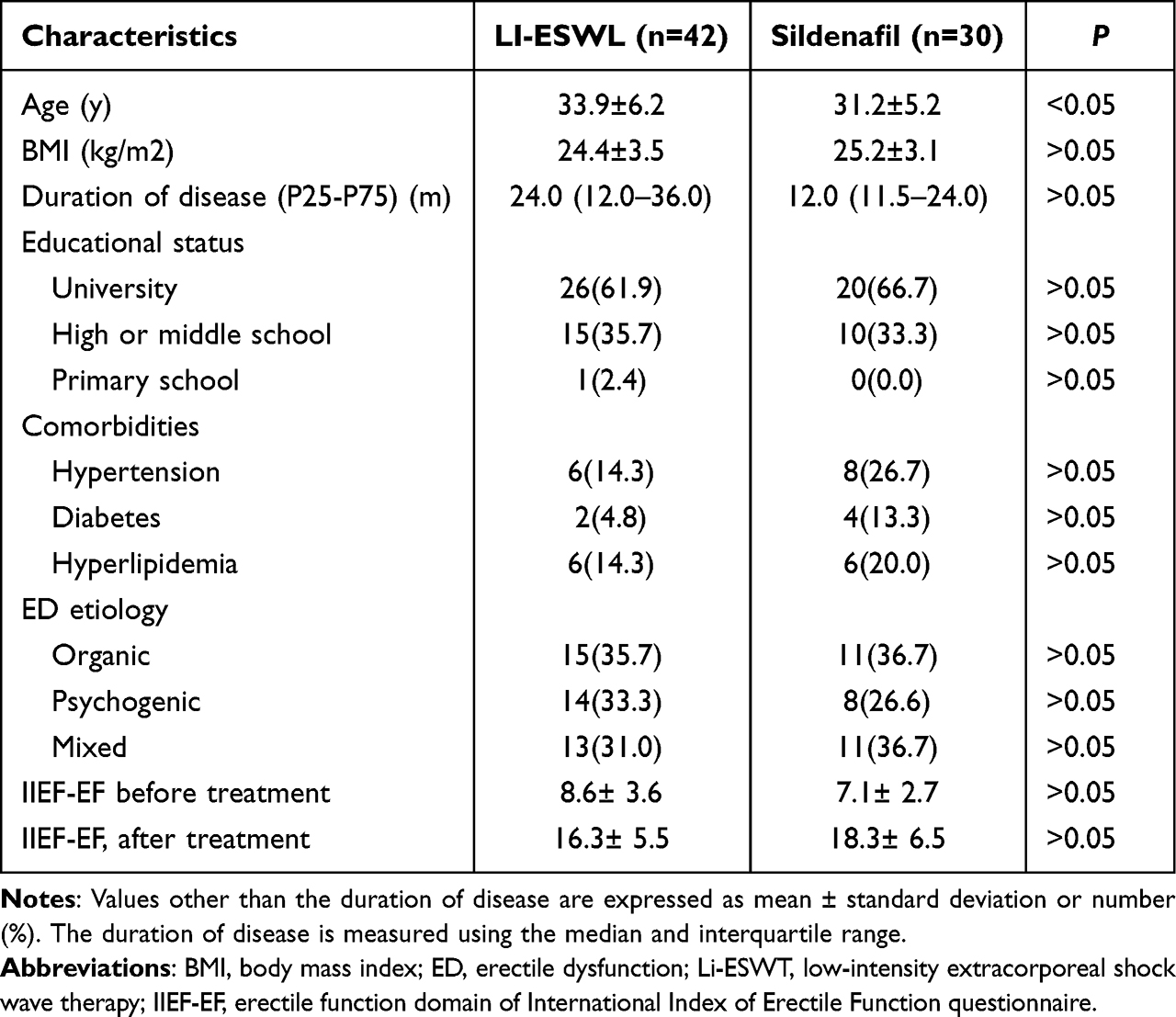 |
Table 1 Baseline Characteristics of Participants in Two Treatment Groups |
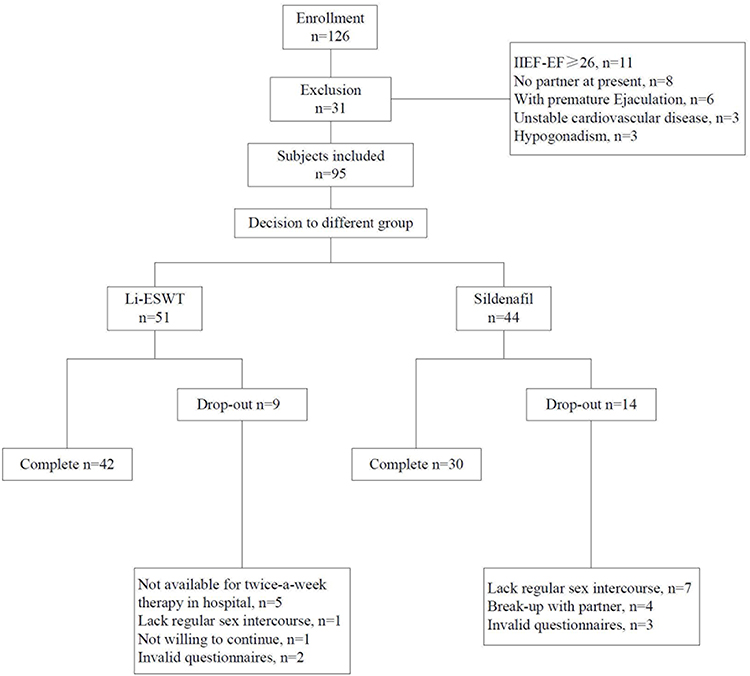 |
Figure 2 Study and treatment flow chart. Abbreviations: IIEF-EF, erectile function domain of International Index of Erectile Function questionnaire; Li-ESWT, low-intensity extracorporeal shock wave therapy; EDITS, Erectile Dysfunction Inventory of Treatment Satisfaction questionnaire. |
Four weeks after the final session, the mean (SD) score in IIEF-EF for Li-ESWT and sildenafil was 16.3± 5.5 and 18.3± 6.5 (P > 0.05), respectively. According to MCID criteria, the ratio of patients who reported positive results was 80.0% in the sildenafil group and 59.5% in the Li-ESWT group, respectively (κ2 = 0.09, P > 0.05).
The total EDITS score and index score of both, the patient version and partner version, were similar in the two groups (Table 2). More detailed analysis of each question in EDITS indicated that a significantly higher number of patients and partners in the Li-ESWT group responded 3 or 4 (very satisfied or somewhat satisfied) to question 1 in the patient and partner version assessing overall satisfaction with treatment than those in the sildenafil group. Furthermore, patients and partners gave the same response to question 6 in the EDITS patient version and question 4 in the partner version, respectively, which address the satisfaction with the duration of intercourse (Table 3).
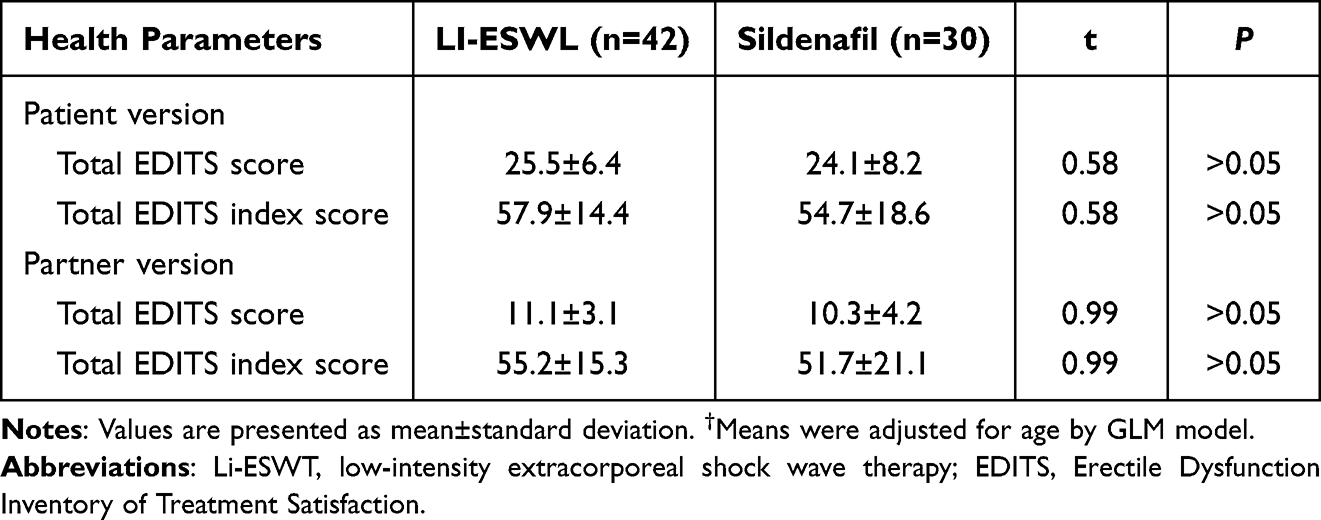 |
Table 2 The Total EDITS Scores and Total EDITS Index Scores at the First-Month Follow-Up After Treatment by Adjustment† |
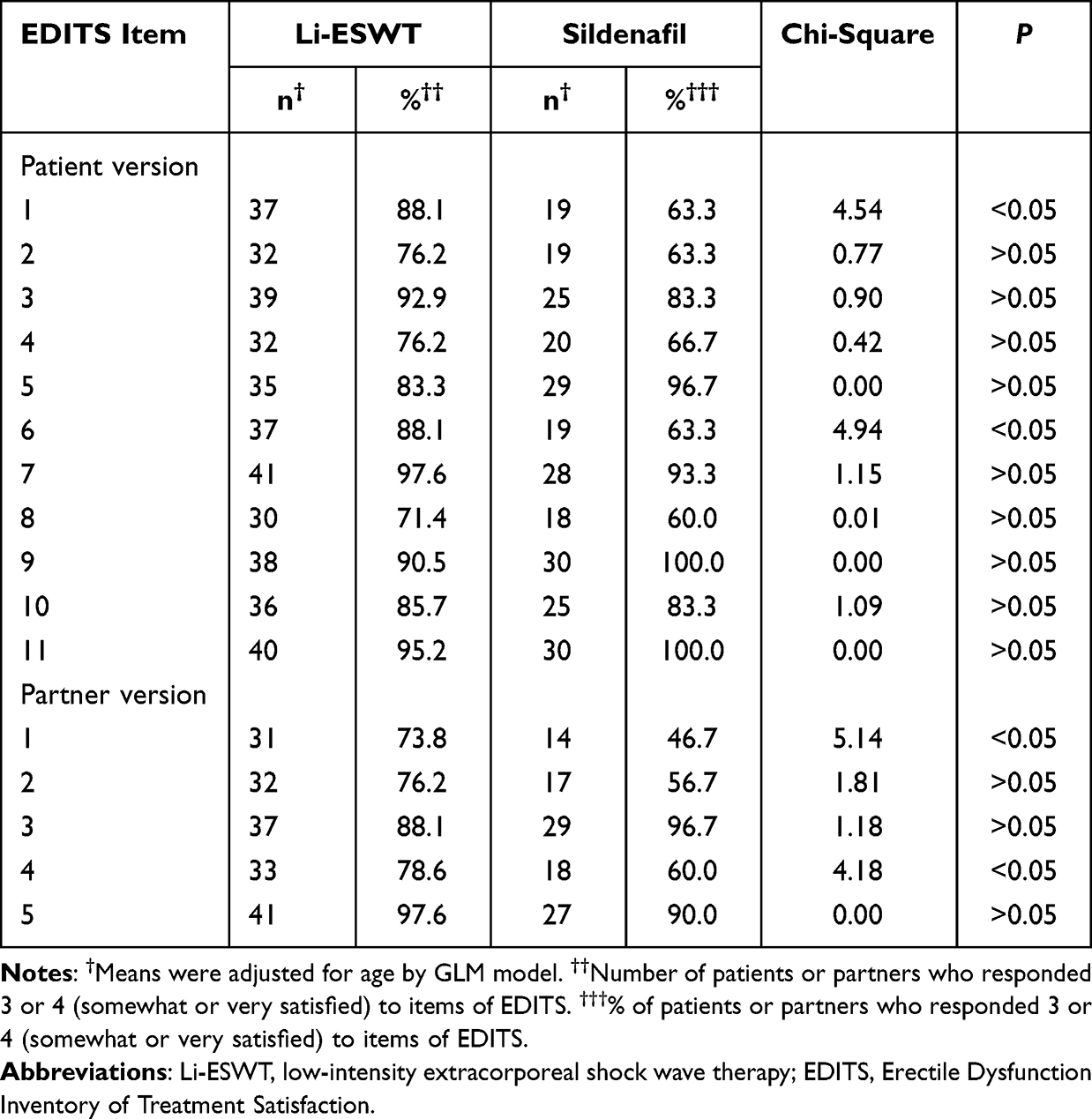 |
Table 3 Comparison of Patients and Female Partners’ Degree of Treatment Satisfaction Assessed by EDITS by Adjustment† |
No participant discontinuation due to adverse events was observed. The only treatment-emergent adverse events in the sildenafil group were flushing and headache (1/30, 3.3%). Other than local penile pain (1/42, 2.4%), no adverse effects were encountered in the Li-ESWT group.
Discussion
The international consensus panel defined ED treatment effectiveness as “a combination of two factors, treatment responsiveness and treatment satisfaction.” In addition, treatment satisfaction was based on a combined assessment of patient and partner satisfaction.16 We applied standardized subjective outcome measurements—IIEF-EF to evaluate erectile function and EDITS to evaluate treatment satisfaction. Furthermore, the treatment satisfaction of partners was also evaluated. To our knowledge, this is the first study to compare treatment effectiveness in patients with ED treated with sildenafil and Li-ESWT from three dimensions: erectile function, and treatment satisfaction of both, patients and partners.
In this trial, Li-ESWT showed a similar treatment outcome to sildenafil for general ED patients. A high response to treatment (5-point increase) was observed in more than 50% of patients in both groups. The improvements in the IIEF-EF score indicated that both therapies were effective in improving erectile function, which is consistent with our earlier result.12 However, in comparison with the previous results, the improvement in erectile function in the Li-ESWT group for ED in this study is relatively low. For example, significant increases in IIEF-EF scores were recorded in all men in a precursor study by application of Li-ESWT for ED in 20 middle-aged men.10 Another study revealed that 72.4% of participants reached an Erection Hardness Score of ≥ 3 after Li-ESWT treatment.11 The reason for the less obvious improvement in the trial may be related to the large proportion of psychogenic ED in our patients.
Satisfaction is one of the most important factors for determining treatment compliance by patients,6 which is particularly evident in young ED patients.7 Moreover, partners of ED patients with more satisfied sexual intercourse may play a positive role in sustaining patient compliance.3,17 In this study, the results showed that patients and their partners in the Li-ESWT group had similar total EDITS and EDITS Index scores as those in the sildenafil group. However, more patients and their partners in the Li-ESWT group were very satisfied and somewhat satisfied with the duration of intercourse compared with those in the sildenafil group. The improvement effect sustained 1 month after Li-ESWT treatment without any additional active intervention, implying that LI-ESWT exerted a genuine physiologic effect on cavernosal tissue. The result is in accordance with other clinical trials.18,19 The underlying basis of the lasting effect of Li-ESWT treatment may be attributable to its neovascularization mechanisms.9,20 Another unexpected finding was the higher rate of overall satisfaction of patients and partners in the Li-ESWT group, indicating the potential advantage of Li-ESWT.
This study has several limitations. First, a small cohort was included in this study, which is a universal drawback among LI-ESWT clinical trials.18,21,22 Second, penile hemodynamics were not measured to confirm the improvement of cavernous blood inflow or penile rigidity. NPTR recording in our study, was only applied to measure the baseline of male erectile capacity and diagnose vasculogenic ED, which should have offered an objective assessment of erection potency change after treatment. In addition, penile Doppler ultrasound could be considered to measure arterial inflow and venous outflow.23 Third, the follow-up duration of 1 month may be short, considering that angiogenesis induced by Li-ESWT requires a longer time.23 Fourth, subgroup comparison was not applied to identify different etiologic groups. Considering the underlying neovascularization mechanisms of Li-ESWT, vasculogenic ED is anticipated to be the ideal candidate for this treatment. However, in terms of mechanisms such as nerve regeneration, other patients such as psychogenic ED patients may also be the marvelous option to be studied.24,25 Lastly, the study was non-randomized and single-centered; these results require multicentered and randomized trials for confirmation.
Conclusions
Our results suggest that Li-ESWT had better satisfaction than on-demand sildenafil in young ED patients and their partners, while the efficacy of the two treatment methods was similar. Considering that our study was non-randomized, in order to confirm the conclusions of our study and clarify the influencing factors of LI-ESWT treatment satisfaction, we need to further expand the sample size and conduct a multi-center RCT study.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This is a non-randomized clinical trial, registered at Chinese Clinical Trial Registry (ChiCTR, http://www.chictr.org.cn/edit.aspx?pid=36572&htm=4), number ChiCTR1900021685. This study was conducted in accordance with the declaration of Helsinki. The present study protocol was reviewed and approved by the Ethics Committee of the Peking Union Medical College Hospital (Reg. No. S-K696). Informed consent was submitted by all subjects when they were enrolled.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts male aging study. J Urol. 1994;151(1):54–61. doi:10.1016/S0022-5347(17)34871-1
2. Capogrosso P, Colicchia M, Ventimiglia E, et al. One patient out of four with newly diagnosed erectile dysfunction is a young man--worrisome picture from the everyday clinical practice. J Sex Med. 2013;10:1833–1841.
3. Dean J, Rubio-Aurioles E, McCabe M, et al. Integrating partners into erectile dysfunction treatment: improving the sexual experience for the couple. Int J Clin Pract. 2008;62:127–133.
4. Shamloul R, Ghanem H. Erectile dysfunction. Lancet. 2013;381:153–165.
5. Hatzimouratidis K, Amar E, Eardley I, et al. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010;57:804–814.
6. Hanson-Divers C, Jackson SE, Lue TF, Crawford SY, Rosen RC. Health outcomes variables important to patients in the treatment of erectile dysfunction. J Urol. 1998;159:1541–1547.
7. Corona G, Rastrelli G, Burri A, et al. First-generation phosphodiesterase type 5 inhibitors dropout: a comprehensive review and meta-analysis. Andrology. 2016;4::1002–1009.
8. Schoofs E, Fode M, Capogrosso P, Albersen M. Current guideline recommendations and analysis of evidence quality on low-intensity shockwave therapy for erectile dysfunction. Int J Impot Res. 2019;31:209–217.
9. Sokolakis I, Dimitriadis F, Teo P, Hatzichristodoulou G, Hatzichristou D, Giuliano F. The basic science behind low-intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic scoping review of pre-clinical studies. J Sex Med. 2019;16:168–194.
10. Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol. 2010;58:243–248.
11. Gruenwald I, Appel B, Vardi Y. Low-intensity extracorporeal shock wave therapy--a novel effective treatment for erectile dysfunction in severe ED patients who respond poorly to PDE5 inhibitor therapy. J Sex Med. 2012;9:259–264.
12. Lei Q, Wang D, Liu C, Ji Z, Yan S. Comparison of the efficacy and safety of low-intensity extracorporeal shock wave therapy versus on-demand sildenafil for erectile dysfunction. Transl Androl Urol. 2021;10:860–868.
13. Rosen RC, Cappelleri JC, Gendrano N
14. Rosen RC, Althof SE, Giuliano F. Research instruments for the diagnosis and treatment of patients with erectile dysfunction. Urology. 2006;68:6–16.
15. Althof SE, Corty EW, Levine SB, et al. EDITS: development of questionnaires for evaluating satisfaction with treatments for erectile dysfunction. Urology. 1999;53:793–799.
16. Carson C, Giuliano F, Goldstein I, et al. The ‘effectiveness’ scale--therapeutic outcome of pharmacologic therapies for ED: an international consensus panel report. Int J Impot Res. 2004;16:207–213.
17. Fisher WA, Rosen RC, Eardley I, Sand M, Goldstein I. Sexual experience of female partners of men with erectile dysfunction: the female experience of men’s attitudes to life events and sexuality (FEMALES) study. J Sex Med. 2005;2:675–684.
18. Vinay J, Moreno D, Rajmil O, Ruiz-Castañe E, Sanchez-Curbelo J. Penile low intensity shock wave treatment for PDE5I refractory erectile dysfunction: a randomized double-blind sham-controlled clinical trial. World J Urol. 2021;39:2217–2222.
19. Chung E, Cartmill R. Evaluation of long-term clinical outcomes and patient satisfaction rate following low intensity shock wave therapy in men with erectile dysfunction: a minimum 5-year follow-up on a prospective open-label single-arm clinical study. Sex Med. 2021;9:100384.
20. Qiu X, Lin G, Xin Z, et al. Effects of low-energy shockwave therapy on the erectile function and tissue of a diabetic rat model. J Sex Med. 2013;10:738–746.
21. Fojecki GL, Tiessen S, Osther PJ. Effect of low-energy linear shockwave therapy on erectile dysfunction-A double-blinded, sham-controlled, randomized clinical trial. J Sex Med. 2017;14:106–112.
22. Yamaçake KGR, Carneiro F, Cury J, et al. Low-intensity shockwave therapy for erectile dysfunction in kidney transplant recipients. A prospective, randomized, double blinded, sham-controlled study with evaluation by penile Doppler ultrasonography. Int J Impot Res. 2019;31:195–203.
23. Kalyvianakis D, Memmos E, Mykoniatis I, Kapoteli P, Memmos D, Hatzichristou D. Low-intensity shockwave therapy for erectile dysfunction: a randomized clinical trial comparing 2 treatment protocols and the impact of repeating treatment. J Sex Med. 2018;15:334–345.
24. Hausner T, Pajer K, Halat G, et al. Improved rate of peripheral nerve regeneration induced by extracorporeal shock wave treatment in the rat. Exp Neurol. 2012;236:363–370.
25. Peng D, Tan Y, Reed-Maldonado AB, Lin G, Lue TF. Molecular mechanism of action of low-intensity extracorporeal shockwave therapy for regenerating penile and peripheral nerves. Turk J Urol. 2020;2020:1.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.