")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 8
The treatment of type 2 diabetes in the presence of renal impairment: what we should know about newer therapies
Authors Davies M, Chatterjee S, Khunti K
Received 5 January 2016
Accepted for publication 3 March 2016
Published 23 June 2016 Volume 2016:8 Pages 61—81
DOI https://doi.org/10.2147/CPAA.S82008
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Video abstract presented by Sudesna Chatterjee.
Views: 2185
Melanie Davies,1,2 Sudesna Chatterjee,1,2 Kamlesh Khunti1,2
1Diabetes Research Centre, University of Leicester, 2Leicester Diabetes Centre, University Hospitals of Leicester NHS Trust, Leicester, UK
Abstract: Worldwide, an estimated 200 million people have chronic kidney disease (CKD), the most common causes of which include hypertension, arteriosclerosis, and diabetes. Importantly, ~40% of patients with diabetes develop CKD, yet evidence from major multicenter randomized controlled trials shows that intensive blood glucose control through pharmacological intervention can reduce the incidence and progression of CKD. Standard therapies for the treatment of type 2 diabetes include metformin, sulfonylureas, meglitinides, thiazolidinediones, and insulin. While these drugs have an important role in the management of type 2 diabetes, only the thiazolidinedione pioglitazone can be used across the spectrum of CKD (stages 2–5) and without dose adjustment; there are contraindications and dose adjustments required for the remaining standard therapies. Newer therapies, particularly dipeptidyl peptidase-IV inhibitors, glucagon-like peptide-1 receptor agonists, and sodium-glucose cotransporter-2 inhibitors, are increasingly being used in the treatment of type 2 diabetes; however, a major consideration is whether these newer therapies can also be used safely and effectively across the spectrum of renal impairment. Notably, reductions in albuminuria, a marker of CKD, are observed with many of the drug classes. Dipeptidyl peptidase-IV inhibitors can be used in all stages of renal impairment, with appropriate dose reduction, with the exception of linagliptin, which can be used without dose adjustment. No dose adjustment is required for liraglutide, albiglutide, and dulaglutide in CKD stages 2 and 3, although all glucagon-like peptide-1 receptor agonists are currently contraindicated in stages 4 and 5 CKD. At stage 3 CKD or greater, the sodium-glucose cotransporter-2 inhibitors (dapagliflozin, canagliflozin, and empagliflozin) either require dose adjustment or are contraindicated. Ongoing trials, such as CARMELINA, MARLINA, CREDENCE, and CANVAS-R, will help determine the position of these new therapy classes and if they have renoprotective effects in patients with CKD.
Keywords: DPP-IV inhibitor, GLP-1RA, SGLT-2 inhibitor, PK, chronic kidney disease, renal impairment
Introduction
Chronic kidney disease (CKD) can adversely affect the pharmacokinetics (PK) or pharmacodynamics (PD) of some therapies.1 Thus, in order for clinicians to make informed choices, it is important to understand how: 1) the use of glucose-lowering therapies is affected by renal impairment; 2) treatment regimens may need to be modified and how these treatments may impact on CKD outcomes; and 3) the importance of safety across the spectrum of CKD.
Worldwide, an estimated 200 million people have CKD,2 a long-term condition that may lead to renal failure and, if left untreated, to premature death. CKD is characterized by the presence of kidney damage, indicated by albuminuria and/or a gradual loss of kidney function (estimated glomerular filtration rate [eGFR]) over time.2 Common causes of CKD include hypertension,3 atheriosclerosis,4 and diabetes.5 Furthermore, CKD is associated with an elevated risk of death from cardiovascular (CV) disease.6 Kidney Disease: Improving Global Outcomes criteria and associated CKD stages are summarized in Tables 1 and 2, respectively.7
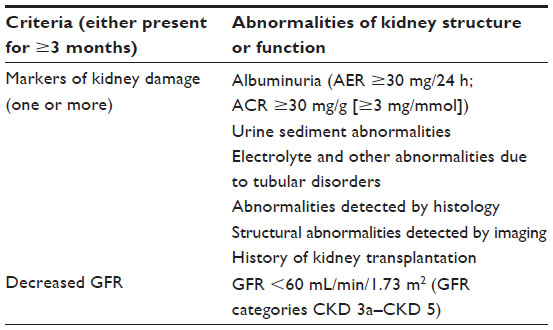 | Table 1 National Kidney Foundation criteria for CKD |
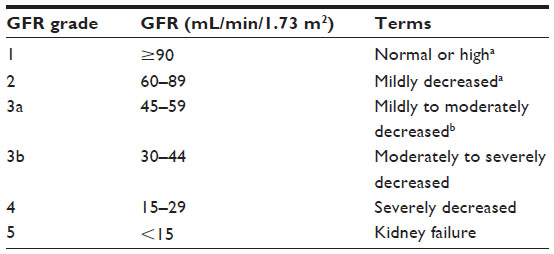 | Table 2 Staging of CKD |
Approximately 40% of patients with diagnosed or undiagnosed diabetes have CKD8 and, in the absence of monitoring for and effective treatment of renal function, CKD can develop insidiously.9 Pathological changes in the kidney include increased glomerular basement membrane thickness, formation of microaneurysms, and mesangial nodules.10 The current estimates show a global prevalence of 415 million adults with diabetes,11 with type 2 diabetes (T2D) accounting for ~90% of these patients;12 CKD in diabetes is, thus, a significant health problem. Atherosclerosis is also an associated condition, leading to narrowing of arterial walls and subsequent high blood pressure.10 Diabetic nephropathy is generally, but not always, preceded by albuminuria, defined as proteinuria of >500 mg/day.10 In fact, there is evidence that intensively improving blood glucose control through pharmacological intervention can reduce the incidence and progression of CKD in people with diabetes. The UK Prospective Diabetes Study found a reduced risk of progressive kidney disease with intensive glycemic control, apparent from a 34% reduction in albuminuria, 67% reduction in the proportion of patients who had a twofold increase in plasma creatinine, and 74% reduction in the proportion of patients who had doubling of plasma urea.13 In addition, the Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation trial determined that intensive glucose control significantly reduced the risk of progression to stage 5 CKD by 65%, microalbuminuria by 9%, and macroalbuminuria by 30%.14 In the Steno-2 study, patients with T2D and microalbuminuria receiving intensive therapy (compared with conventional therapy) had a significantly lower risk of nephropathy (hazard ratio: 0.39, 95% confidence interval [CI]: 0.17–0.87; P<0.003).15
A recent meta-analysis demonstrated that combination therapies are effective in improving glycemic control, with some combinations of metformin and newer drug classes (specifically, dipeptidyl peptidase-IV [DPP-IV] inhibitors, glucagon-like peptide-1 receptor agonists [GLP-1RAs], and sodium-glucose cotransporter-2 [SGLT-2] inhibitors) providing glycemic control without increasing the risk of hypoglycemia or weight gain.16 Indeed, many current treatment guidelines now advocate the use of these newer therapies in multiple stepwise combinations.17
As previous reviews have already investigated the impact of conventional glucose-lowering therapies on CKD,18,19 this review will primarily focus on the newer therapies (DPP-IV inhibitors, GLP-1RAs, and SGLT-2 inhibitors), mechanisms by which CKD affects the use of T2D therapies, place of these therapies in CKD treatment, and their potential renoprotective effects.
T2D therapies and CKD
Conventional glucose-lowering therapies
Conventional glucose-lowering therapies include metformin, sulfonylureas, thiazolidinediones, meglitinides, and insulin.
Apart from pioglitazone, a thiazolidinedione,20 other conventional therapies must be reduced or withdrawn as eGFR declines due to increased risk of lactic acidosis (in the case of metformin) and hypoglycemia (in the case of sulfonylureas, meglitinides [such as repaglinide], and insulin).21–33 Their use in CKD is described below and summarized in Table 3.
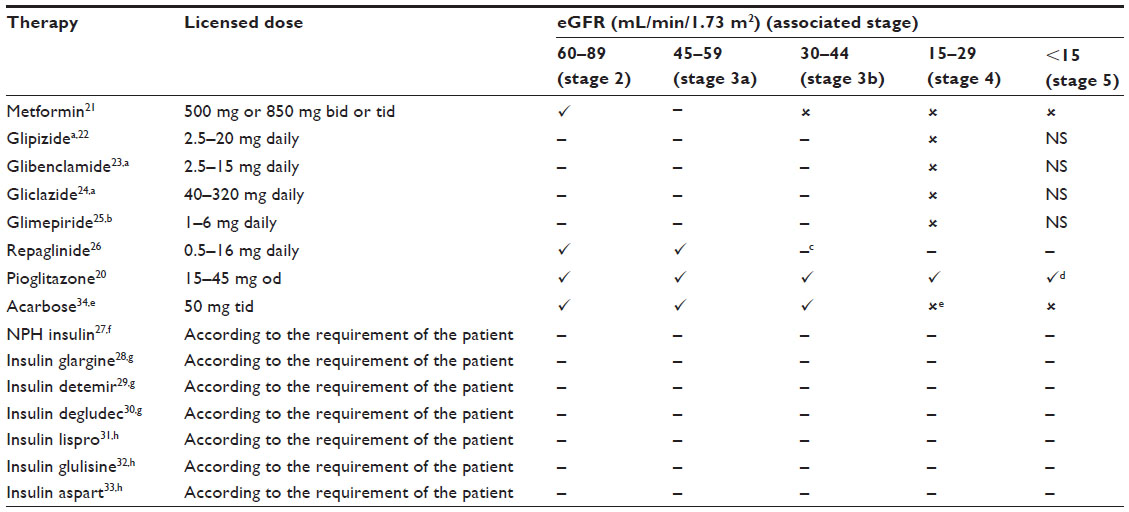 | Table 3 The use of conventional glucose-lowering therapies in chronic kidney disease (based on European Union label) |
Metformin
Metformin may be used without dose adjustment in patients with stage 2 CKD. With dose adjustment, metformin may be used in patients with stage 3a CKD, but only in the absence of other conditions, such as liver dysfunction,35 CV disease,36 and renal disease,36 which may increase the risk of lactic acidosis. Renal function must be closely monitored every 3–6 months and, if eGFR falls to <45 mL/min/1.73 m2, metformin administration must be stopped.21 Current UK National Institute for Health and Care Excellence guidelines suggest stopping if eGFR falls to <30 mL/min/1.73m2.37 Clinical data on the risk of lactic acidosis in metformin-treated patients with CKD are currently limited.38
Sulfonylureas
Patients with CKD who are treated with glipizide, glibenclamide, gliclazide, and glimepiride require careful monitoring. Moreover, these sulfonylureas are contraindicated in patients with stage 4 CKD.22–25 The PK and/or PD of glipizide may be altered in patients with impaired renal function; initial and maintenance dosing should, therefore, be conservative to avoid hypoglycemic episodes.22 Glibenclamide should be used cautiously in patients with stages 2 and 3 CKD; however, in long-term clinical trials, patients with renal impairment have been treated adequately at reduced doses with frequent monitoring.23 Likewise, in long-term clinical trials, patients with renal impairment have also been treated adequately using gliclazide at reduced doses with frequent monitoring.24 In the case of glimepiride, in patients with low creatinine clearance (CrCl), there is a trend for glimepiride clearance to elevate and serum concentrations to diminish.25
Meglitinides
The meglitinides, such as repaglinide, are short-acting. Patients with CKD ranging from stages 3b to 5 require careful management.26 Repaglinide is mostly metabolized by the liver and, with dose adjustment, may be used in patients with CKD.26 In a clinical trial, after 5 days of treatment with repaglinide, there was a twofold increase in exposure (area under the curve [AUC]) and half-life in patients with stage 4 CKD compared with individuals with normal renal function.26
Thiazolidinediones
Of the thiazolidinedione family, only pioglitazone is generally available due to safety concerns with other agents in this class. No dose adjustment is required with impaired renal function (stages 2–5 CKD), as pioglitazone is metabolized mainly by the liver.20,39 No information is available for patients undergoing dialysis; therefore, pioglitazone should not be used in this setting. Plasma concentrations of pioglitazone and its metabolites in patients with CKD are lower than those observed in individuals with normal renal function, but the parent compound shows comparable apparent clearance.20 Edema occurs in ~5% of patients treated with pioglitazone in monotherapy or combination therapy.40 Although there have been concerns over CV risk,41 a recent study showed that pioglitazone was not associated with any increase in CV adverse events (AEs).41
Alpha-glucosidase inhibitors
The alpha-glucosidase inhibitor acarbose has gastrointestinal side effects associated with its use, including flatulence, soft stools, and abdominal discomfort.34,42 Acarbose is excreted unaltered by the renal system and should not be initiated in patients with stage 4 CKD.34
Amylin analogs
Amylin analogs, such as pramlintide, are commonly used in the US. Pramlintide has limited side effects but a small proportion of patients may have intolerable nausea despite receiving the lowest doses.43 The dosing requirements for pramlintide are not altered in patients with stages 2–4 CKD.43 Pramlintide has not been studied in patients with stage 5 CKD.43
Dopamine agonists
Dopamine agonists, such as bromocriptine, are commonly used in the US. Common side effects of bromocriptine include nausea, asthenia, constipation, dizziness, and rhinitis.44 No PK studies have been conducted in patients with renal impairment.45 Although the kidney is a minor pathway for elimination of bromocriptine, careful monitoring should be undertaken in patients with renal impairment.45
Insulin
Classes of insulin include intermediate-acting (neutral protamine Hagedorn insulin, indicated for basal coverage), long-acting (glargine 100 units/mL28 and 300 units/mL [U300],46 detemir29 and degludec30 indicated for basal coverage), and fast-acting (lispro,47 glulisine,48 and aspart,49 indicated for prandial coverage). CKD may reduce insulin requirements dramatically and increase the risk for hypoglycemia in patients.50 Insulin dose, therefore, needs to be adjusted on an individual basis.
In patients with CKD, glargine requirements may be diminished because of reduced insulin metabolism;28,46 the high concentration of insulin (U300) results in different PK and PD profiles, but both concentrations have been shown to be safe in patients with renal failure.46,51,52 In a clinical study, the PK of detemir did not significantly differ in patients with stages 3–4 CKD compared with healthy individuals.53 Likewise, in one clinical study, renal impairment did not have a significant effect on maximum concentration (Cmax), apparent clearance, or AUC0–120 h of single-dose degludec.30,54
The glucodynamic response to insulin lispro is not affected by renal impairment.31,47 Glulisine requirements may be reduced in the presence of renal impairment.32 In patients with type 1 diabetes, renal impairment (stages 2–5 CKD) did not affect the PK of aspart in a clinically significant manner.33,55
Newer therapies
DPP-IV inhibitors, GLP-1RAs, and SGLT-2 inhibitors are the most recent classes of agents licensed for use in T2D in Europe. The use of newer therapies in CKD is described below and summarized in Table 4.
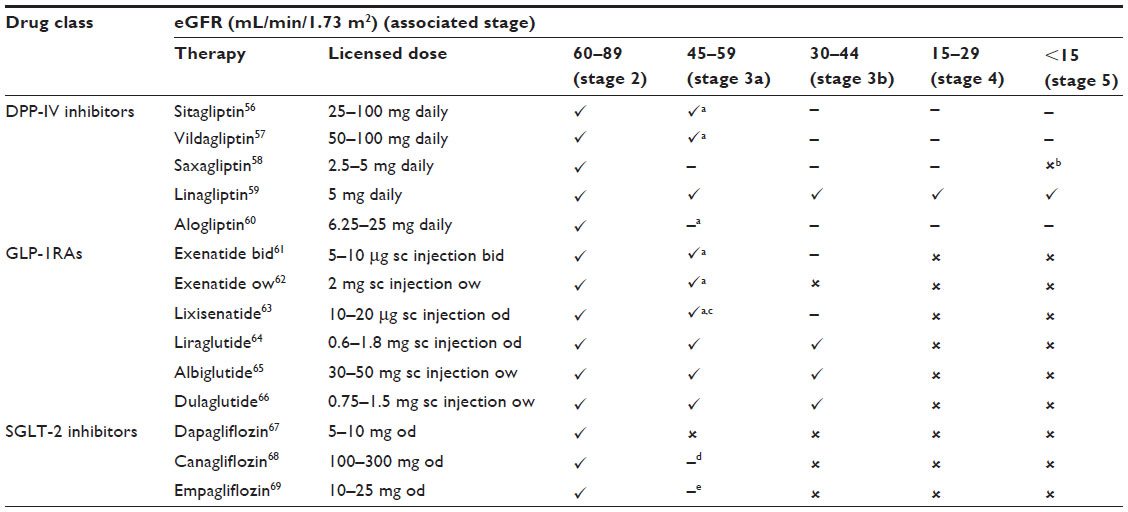 | Table 4 Newer glucose-lowering therapies and data regarding their use in CKD (based on European Union label) |
DPP-IV inhibitors
DPP-IV inhibitors, such as sitagliptin, vildagliptin, saxagliptin, alogliptin and linagliptin, reduce the physiological breakdown of native GLP-1, which increases the secretion of insulin and promotes satiety, effectively decreasing blood glucose levels.70 A meta-analysis has shown that DPP-IV inhibitors are effective in lowering glycated hemoglobin (HbA1c) in patients with T2D and stages 3–4 CKD (−0.52%, 95% CI: –0.64 to –0.39).71 Despite associations with AEs that include nasopharyngeal symptoms, headaches, angioedema,72,73 and pancreatitis,72 meta-analyses showed low prevalence of such AEs.74,75
DPP-IV inhibitors are metabolized and eliminated in a number of different ways. Their mode of action (MOA) and elimination, as well as PK and safety, are described in Table 5.
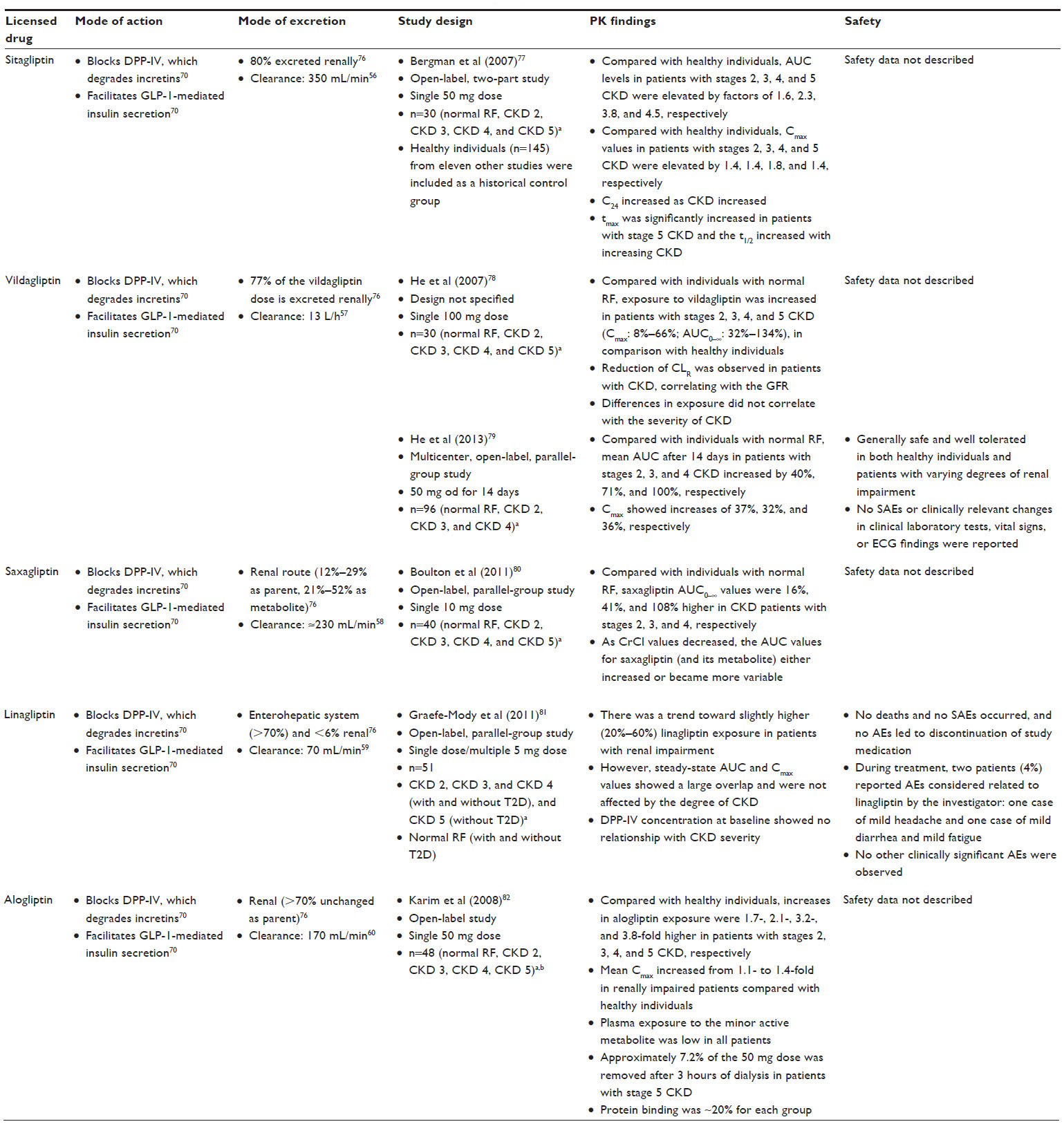 | Table 5 DPP-IV inhibitors: modes of action, modes of excretion, and studies investigating PK |
Sitagliptin
Sitagliptin undergoes limited hepatic metabolism; ~80% of the dose is excreted renally, and there is a low, reversible protein binding in the plasma (38%).76
The TECOS study showed that sitagliptin was noninferior to placebo for the primary composite CV outcome of CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for unstable angina (hazard ratio 0.98, 95% CI: 0.88–1.09; P<0.001).83 In addition, no significant differences between the placebo and sitagliptin group in incidences of pancreatic cancer (P=0.32), acute pancreatitis (P=0.07), or hospitalization for heart failure (P=0.98) were reported.83 In T2D patients, sitagliptin has also been shown to reduce significantly urinary albumin excretion (P<0.0001).84
One PK study in patients without T2D showed that, compared with healthy controls, plasma sitagliptin AUC levels in patients with stages 2–5 CKD were increased by factors of 1.6–4.5.77 Cmax was moderately increased, and concentration at 24 hours increased as severity of CKD increased. Time to Cmax was significantly increased in patients with stage 5 CKD, and the half-life increased with increasing severity of CKD. For patients with stages 2–4 CKD, clearance rates were 0.18–0.71 mL/min.77
In treatment, patients with stage 2 CKD and stage 3 CKD (if eGFR is ≥50 mL/min) require no dose adjustment. For stage 3 CKD and an eGFR of <50 mL/min, the sitagliptin dose should be reduced to 50 mg once daily (od). For patients with stages 4–5 CKD, including those undertaking hemodialysis or peritoneal dialysis, the dose should be decreased to 25 mg od. Treatment can be administered regardless of dialysis time.56
Vildagliptin
Vildagliptin is metabolized via four metabolic pathways before excretion.85 Overall, 77% of the vildagliptin dose is excreted renally (22% as parent, 55% as primary metabolite). In the plasma, vildagliptin shows low (10%), reversible protein binding.76 In patients in early stages of nephropathy, vildagliptin significantly decreased albumin concentrations.86
In a PK study, patients with stages 2–5 CKD, systemic exposure to vildagliptin was increased (Cmax: 8%–66%; AUC extrapolated to infinity: 32%–134%) compared with healthy individuals.78 Changes in exposure to vildagliptin showed no relationship with severity of CKD. No safety data were reported.78 A later study showed that the mean AUC of vildagliptin after 14 days in patients with stages 2–4 CKD increased by 40%–100%. Vildagliptin Cmax increased by 32%–37%.79 Vildagliptin was generally safe and well tolerated in both healthy individuals and patients with different stages of CKD.
In treatment, no dose adjustment of vildagliptin is required in patients with stage 2 CKD. In patients with stages 3–5 CKD, for safety, the recommended dose is 50 mg od.57
Saxagliptin
Saxagliptin is metabolized in the liver, producing an active metabolite. It is eliminated via the kidney (12%–29% as parent, 21%–52% as metabolite).76 In the plasma, saxagliptin shows negligible protein binding.76
The Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus – Thrombolysis in Myocardial Infarction 53 (SAVOR-TIMI 53) trial confirmed that the CV safety of saxagliptin met US Food and Drug Administration requirements.87 Patients with no renal impairment or stage 2 CKD (P<0.0001) and stages 3–4 CKD (P=0.041) randomized to saxagliptin had greater improvement and less worsening of urine albumin-to-creatinine ratio (UACR) than patients randomized to placebo. Indeed, the relative risk of hospitalization for heart failure was comparable among patients with normal renal impairment or stage 2 CKD and patients with stages 3 and 4 CKD (P=0.43).
One PK study showed that, compared with patients with normal renal function, saxagliptin AUC extrapolated to infinity values were 16%–108% increased in those with stages 2–4 CKD.80 In addition, as CrCl values decreased, AUC values either increased or became more variable.
In treatment, no dose adjustment of saxagliptin is recommended for patients with stage 2 CKD;58 however, to keep the plasma concentration comparable to individuals with normal renal function, the dose should be reduced to 2.5 mg od in patients with stages 3–4 CKD. However, saxagliptin is contraindicated in patients with stage 5 CKD requiring hemodialysis.58
Linagliptin
Linagliptin is metabolized by the liver and does not have active metabolites. It is eliminated by the enterohepatic system (>70% unchanged as parent) and the kidney (<6%).76 Linagliptin binds extensively to plasma proteins in a concentration-dependent manner and it has been calculated that, at the therapeutic dose (5 mg), most of the drug is protein-bound.76 In a study in which linagliptin was administered to patients with T2D and renal dysfunction, there was a significant reduction in albuminuria.88
In one PK study, although there was a trend toward slightly higher (20%–60%) linagliptin exposure in patients with CKD, steady-state AUC and Cmax values showed a substantial overlap and were unaffected by the degree of CKD.81 No deaths or serious AEs occurred, and no AEs led to discontinuation. During treatment, two patients reported AEs considered related to linagliptin by the investigator. No other clinically significant AEs were observed.81
In treatment, in patients with CKD, no dose adjustment is required, and it can be administered across the CKD spectrum.59
Alogliptin
Alogliptin is eliminated slowly, primarily via renal excretion (>70% unchanged as parent).76 After oral administration, alogliptin is absorbed with 100% bioavailability and undergoes ~20% protein binding and limited hepatic metabolism.89 In a study by Sakata et al,90 alogliptin reduced UACR following 12 weeks of treatment.
In a PK study involving patients with various degrees of renal impairment (not stated whether any patients had T2D), Karim et al82 determined that, compared with healthy individuals, increases in alogliptin exposure were 1.7–3.8-fold higher in patients with stages 2–5 CKD. The range of alogliptin AUC was comparable in healthy individuals and patients with stage 2 CKD. Cmax increased from 1.1- to 1.4-fold in patients with CKD compared with healthy individuals. Plasma exposure suggested no accumulation of this metabolite in patients with increasing CKD. Approximately 7.2% of the 50 mg dose was eliminated after 3 hours of dialysis in patients with stage 5 CKD. Protein binding was ~20% for each CKD group.82
In patients with stage 2 CKD (in the CrCl range >50 to ≤80 mL/min), no alogliptin dose adjustment is required. For patients with stage 3 CKD (in the CrCl range ≥30 to ≤50 mL/min), half of the recommended dose should be administered (12.5 mg od) to keep the plasma concentration comparable to healthy individuals.60 Likewise, for patients with stages 4–5 CKD requiring dialysis, administration of a quarter of the recommended dose is advised (6.25 mg od).60
Summary of DPP-IV inhibitor use in renal impairment
DPP-IV inhibitors can be used at all stages of CKD with dose reduction, except for linagliptin, which can be used without dose adjustment.56–60 A potential renoprotective effect (reduction in albuminuria) has been observed with all DPP-IV inhibitors.84,86–88,90 It is not clear whether this renoprotective effect is independent of changes in blood pressure and glycemic markers.
GLP-1 receptor agonists
GLP-1RAs function as incretin mimetics, which enhance the action of the endogenous incretin GLP-1, thereby controlling glycemia via several pathways, including enhancement of insulin secretion, inhibition of glucagon secretion, delay of gastric emptying, and induction of satiety.91 GLP-1RAs reduce HbA1c by 0.55%–1.90%72,92 and have low rates of hypoglycemia,93 with the advantage of promoting weight loss as well as controlling blood glucose.91 Owing to the effect of these agents on gastric emptying, AEs are typically gastrointestinal, that is, nausea and vomiting.91 However, gradually increasing the dose over a few weeks helps build a tolerance to such side effects. One possible, but infrequent, AE is pancreatitis. Available evidence suggests that the rate of pancreatitis among patients using GLP-1RAs is low;94 however, these data are not definitive and ongoing analysis is needed.94
The short-acting compounds (short-lived receptor activation) consist of exenatide twice daily (bid) and lixisenatide od; the longer-acting compounds, which continuously activate receptors at their recommended dose, consist of liraglutide od and once weekly (ow) formulations of exenatide, albiglutide, and dulaglutide.95 Exenatide96 and liraglutide97 have been shown to reduce albuminuria and proteinuria, respectively. A summary of the MOAs, elimination, PK, and safety of the GLP-1RAs is provided in Table 6.
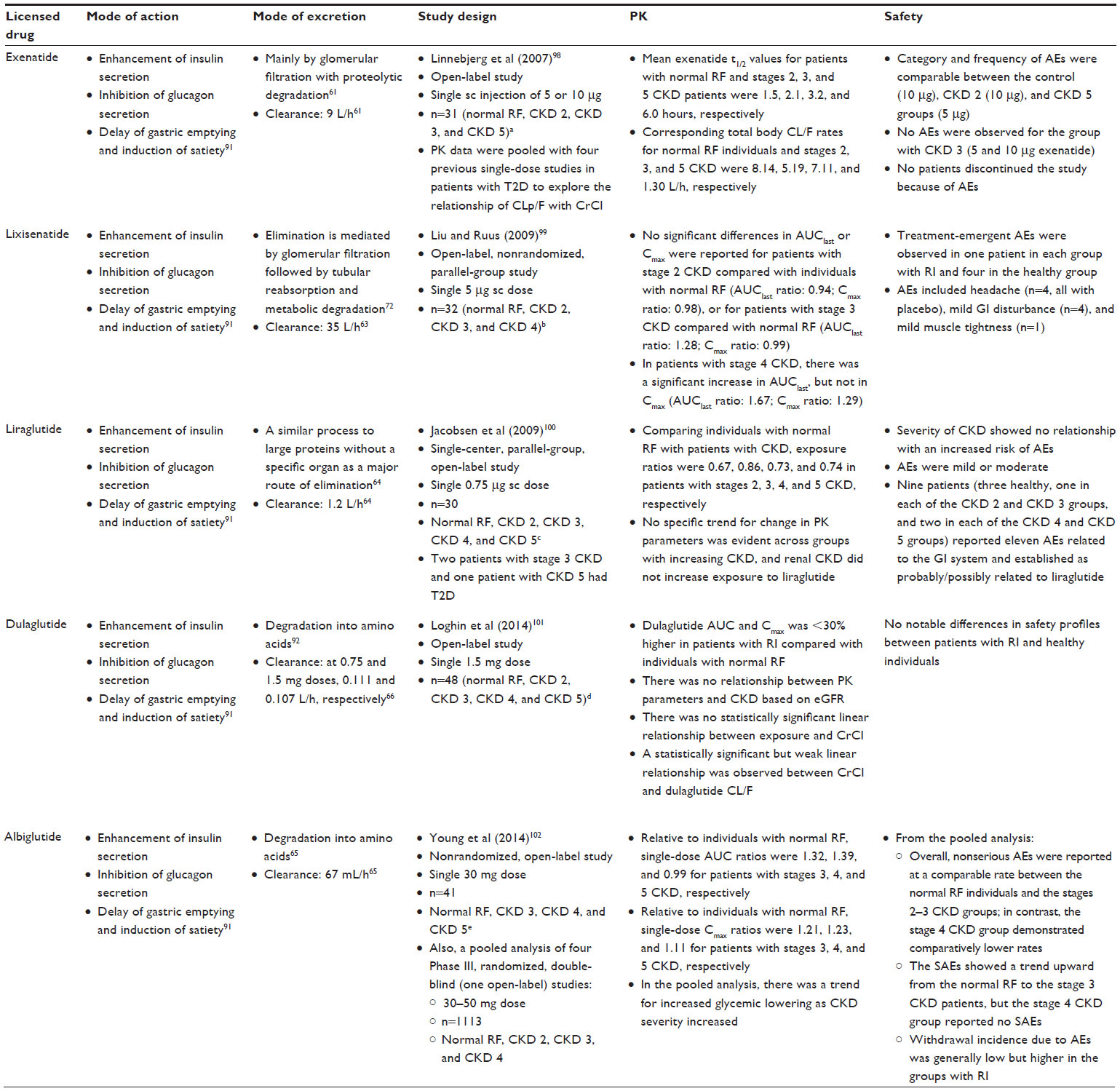 | Table 6 GLP-1RAs: modes of action, modes of excretion, and studies investigating PK |
Exenatide
Exenatide is a synthetic analog of exendin-4, which is extracted from the saliva of Heloderma suspectum.103 Exenatide bid and ow are both eliminated mainly by glomerular filtration with subsequent proteolytic degradation. In addition, Zhang et al96 reported decreased levels of 24-hour urinary albumin after 16 weeks of exenatide treatment (P<0.01).
In a study by Linnebjerg et al,98 exenatide (5 or 10 μg) was injected subcutaneously in 31 patients (including one patient with T2D) stratified by renal function (CrCl): normal and stages 2–5 CKD. PK data were then combined with four previous single-dose studies in patients with T2D to determine the relationship of exenatide clearance and CrCl. The half-life for patients with normal renal function and stages 2–5 CKD groups was 1.5–6.0 hours. After pooling data from several studies, least-squares geometric mean for exenatide clearance in individuals with normal renal function and patients with stages 2–4 CKD were 5.19–8.14 L/h.98 Similar category and incidence of AEs were reported between the healthy and stages 2 and 5 CKD groups. No AEs were reported for the group with stage 3 CKD and no patients discontinued because of AEs.98
No dose adjustment is required at stage 2 CKD to preserve therapeutic exposure. Dose adjustment is required in exenatide bid if CrCl in the patient is in the range 30–50 mL/min, which falls within the definition of stages 3a and 3b CKD;61 within the same CrCl range, exenatide ow is contraindicated.62 However, both exenatide bid and ow are contraindicated in patients with stages 4–5 CKD.61,62
Lixisenatide
As with exenatide, lixisenatide is a synthetic version of exendin-4,104 with resistance to physiological degradation by DPP-IV as a result of C-terminal modification.104 Elimination occurs through glomerular filtration followed by tubular reabsorption and subsequent metabolic degradation.72
A study has shown that stage 2 CKD does not influence lixisenatide PK;63 however, in patients with stages 3–4 CKD, the AUC was increased by 24%–46%.63 In an open-label, nonrandomized, parallel-group study by Liu and Ruus,99 no significant differences in AUC up to the last measurable concentration or Cmax were observed for patients with stage 2 CKD compared with individuals with normal renal function or, indeed, for patients with stage 3 CKD versus normal function. However, in patients with stage 4 CKD, there was a significant increase in AUC up to the last measurable concentration, but not in Cmax.99 Treatment-emergent AEs were reported for one patient in each CKD group and four in the group of patients with normal renal function. AEs included headache (n=4; all with placebo), mild gastrointestinal disturbance (n=4), and mild muscle tightness (n=1).99
No dose adjustment is required at stage 2 CKD to maintain therapeutic exposure. In treatment, monitoring is required with lixisenatide in patients whose CrCl is in the range 30–50 mL/min (which falls within the definition of stages 3a and 3b CKD).63 Additionally, lixisenatide is contraindicated in patients with stages 4 and 5 CKD.63
Liraglutide
Liraglutide has 97% sequence homology to GLP-1.63 Liraglutide is endogenously metabolized in a similar process to large proteins with no specific organ established as a major route of elimination.64 Zavattaro et al have shown a decrease in the proportion of patients with microalbuminuria; five patients in the study had microalbuminuria at baseline, but at 12 months, the levels in three of the patients had returned to normal (P<0.006). Total microalbuminuria levels were improved in patients with normal renal function and stage 2 CKD (P<0.02).105 Investigating the superiority of liraglutide 1.8 mg versus placebo as an add-on to existing oral glucose-lowering agents with T2D and stage 3 CKD, the LIRA-RENAL study showed that liraglutide did not affect renal function and demonstrated better glycemic control (estimated treatment difference in HbA1c from baseline was −0.66% [95% CI: –0.90 to –0.43; P<0.0001]). Moreover, no difference in hypoglycemic AEs was reported between treatment groups; common AEs were gastrointestinal (liraglutide, 35.7%; placebo, 17.5%).106
Jacobsen et al100 investigated the effect of renal impairment on the PK of liraglutide in patients with T2D and normal renal function or stages 2–5 CKD. No defined relationship for change in PK parameters was evident across groups with increasing severity of CKD, and CKD did not increase exposure to liraglutide. Headache and gastrointestinal symptoms were the most commonly reported AEs. Reported AEs were mild to moderate in severity.100
In treatment, no dose adjustment is necessary for patients with stages 2–3 CKD. As there is no therapeutic knowledge in patients with stages 4–5 CKD, liraglutide is contraindicated for use in patients with these diagnoses.64
Dulaglutide
Dulaglutide has 90% sequence homology to GLP-1,92 with the GLP-1 portion of the molecule fused to an immunoglobulin 4 molecule, limiting renal clearance.92 Elimination occurs through degradation into amino acids.92
Loghin et al101 assessed the PK of dulaglutide 1.5 mg in renal impairment compared to healthy individuals. The study included stages 2–5 CKD populations. There was no correlation between PK parameters and renal function based on eGFR. Also, there was no statistically significant correlation between exposure and CrCl. A weak, statistically significant linear correlation was established between CrCl and dulaglutide clearance. There were no prominent differences in safety profiles between patients with CKD and healthy individuals.101
In treatment, no dose adjustment of dulaglutide is necessary in patients with stages 2–3 CKD, but there is still limited experience in patients with stages 4–5 CKD; consequently, dulaglutide is contraindicated in these populations.66
Albiglutide
Albiglutide shares 95% sequence homology with native GLP-1.107 It is composed of a GLP-1 dimer fused to an albumin molecule.108 The expected metabolic pathway for albiglutide is degradation to small peptides and individual amino acids by ubiquitous proteolytic enzymes.65
In their investigation of the PK of albiglutide in patients with T2D stages 2–5 CKD groups, Young et al102 determined modest increases in plasma albiglutide concentration with increased severity of renal impairment and a trend for greater glycemic reductions as eGFR decreased, indicating no need for a dose adjustment. Overall, the incidences of nonserious AEs were comparable in the normal, and stages 2 and 3 CKD groups, whereas the stage 4 CKD group demonstrated lower rates. The serious AEs increased with increasing renal dysfunction up to stage 3 CKD, but the stage 4 CKD group reported no serious AEs.102
In treatment, no dose adjustment of albiglutide is required for patients with stages 2–3 CKD. There is limited experience in patients with stages 4–5 CKD, and, therefore, albiglutide is contraindicated in these patients.65
Summary of GLP-1RA use in renal impairment
Dose adjustment is required in exenatide bid in patients whose CrCl is in the range 30–50 mL/min, which falls within the definition of stages 3a and 3b CKD;56,61 within the same CrCl range, exenatide ow is contraindicated.62 Also, within the same range, monitoring is necessary when dosing lixisenatide.63 By contrast, no dose alteration is necessary for liraglutide, albiglutide, and dulaglutide in stages 2, 3a, and 3b CKD.64–66 All GLP-1RAs are currently contraindicated in stages 4–5 CKD.61–66
SGLT-2 inhibitors
SGLT-2 inhibitors inhibit glucose reabsorption and induce excretion of glucose in the urine.109 Treatment with SGLT-2 inhibitors is associated with reductions in HbA1c levels of 0.4%–1.5% and weight of up to 4.7 kg.110,111
SGLT-2 inhibitors carry a low risk of hypoglycemia, unless combined with sulfonylureas or insulin.112 AEs include urinary and genital tract infections (which are usually not severe), especially in female patients.112 SGLT-2 inhibitors appear to be associated with a small increased risk of euglycemic diabetic ketoacidosis and ketosis.112,113
As their efficacy is reliant on renal function, SGLT-2 inhibitors are generally contraindicated in patients with eGFR <60 mL/min/1.73 m2, mainly because of reduced efficacy.72 A summary of their MOAs, elimination, PK, and safety is provided in Table 7.
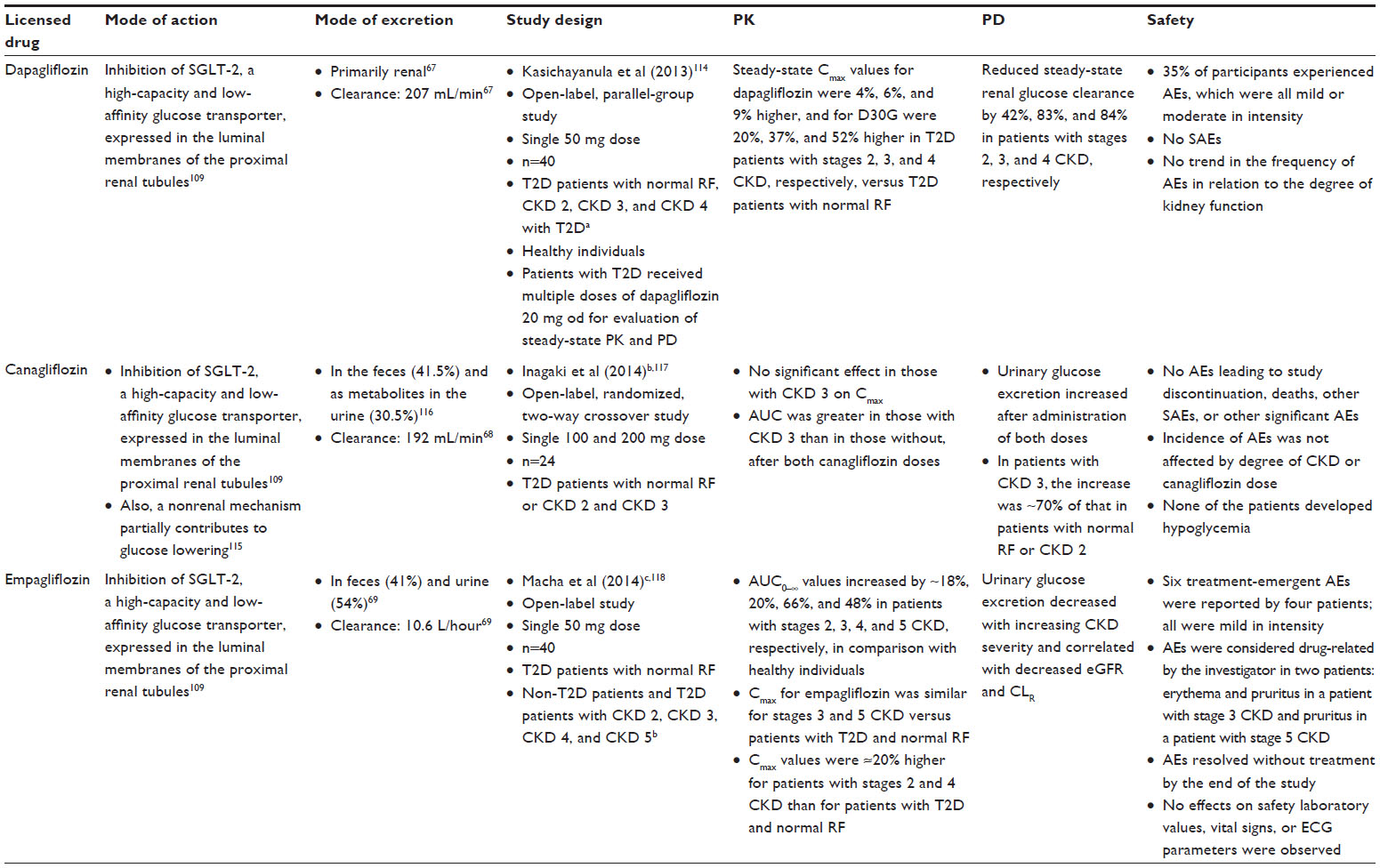 | Table 7 SGLT-2 inhibitors: modes of action, modes of excretion, and studies investigating PK and PD |
Dapagliflozin
Dapagliflozin is metabolized in both the kidney and the liver, with active metabolites generated at doses of >50 mg.119 It is primarily eliminated via the renal pathway.67
Assessment of PK by Kasichayanula et al114 in healthy individuals and patients with T2D with normal renal function and stages 2–4 CKD showed that dapagliflozin plasma concentrations and its inactive metabolite dapagliflozin 3-O-glucuronide increased with increasing CKD severity. Steady-state Cmax values for dapagliflozin were 4%–9% higher, and for dapagliflozin 3-O-glucuronide were 20%–52% higher in T2D patients with stages 2–4 CKD, compared with patients with T2D and normal renal function.114 Steady-state renal glucose clearance was reduced by 42%–84% in patients with stages 2–4 CKD, thereby also reducing its efficacy.114
In treatment, dapagliflozin is not recommended for use in patients with stages 3–5 CKD.67 However, no dosage adjustment is suggested in patients with stage 2 CKD.
Canagliflozin
Canagliflozin is primarily metabolized by O-glucuronidation.116 It is eliminated largely unchanged in the feces (41.5%) and as metabolites in the urine (30.5%). Recent clinical data suggest that, in addition to the renal mechanism of action, a nonrenal mechanism partially contributes to glucose lowering for canagliflozin 300 mg but not 150 mg.115 Data from a substudy of the CANagliflozin cardioVascular Assessment Study (CANVAS) showed that 100 and 300 mg doses of canagliflozin significantly reduced the primary outcome of HbA1c levels relative to placebo at week 18 (both P<0.001).120
A study examining the impact of CKD on the PK and PD of canagliflozin 100 and 200 mg in Japanese patients with T2D found no significant effect of stage 3 CKD on the Cmax of either canagliflozin dose.121 The canagliflozin AUC values were higher in patients with stage 3 CKD than in patients with T2D and normal renal function or stage 2 CKD. Changes from baseline in 24-hour urinary glucose excretion increased after administration but, in patients with stage 3 CKD, the increases were ~70% of those in patients with stage 2 CKD or normal.
In treatment, in patients with stage 2 CKD, no dose adjustment is needed.68 Canagliflozin should not be initiated in patients with eGFR <60 mL/min/1.73 m2, but in patients tolerating canagliflozin whose eGFR falls continuously below 60 mL/min/1.73 m2, the dose of canagliflozin should be reduced to or managed at 100 mg od. Canagliflozin is contraindicated in patients with stages 3b–5 CKD, and in patients undertaking dialysis.
Empagliflozin
Empagliflozin is metabolized by glucuronidation without generation of active metabolites and eliminated in feces (41%) and urine (54%).69
In a study comparing patients with normal renal function (and T2D), stage 2 CKD (and T2D), stage 3 CKD (and T2D), stage 4 CKD (four patients with T2D and four without), and stage 5 CKD (without T2D), Macha et al118 showed that the Cmax for empagliflozin was similar for stages 3 and 5 CKD and with normal renal function (and T2D). However, empagliflozin Cmax values were ~20% higher for patients with stages 2 and 4 CKD than for patients with normal renal function.118
In treatment, no dose adjustment of empagliflozin is necessary for patients with stage 2 CKD, but empagliflozin treatment should not be administered in patients with eGFR <60 mL/min/1.73 m2. In patients tolerating empagliflozin whose eGFR falls continuously beneath 60 mL/min/1.73 m2, the dose of empagliflozin should be altered or managed at 10 mg od and stopped when eGFR is continuously beneath 45 mL/min/1.73 m2. Empagliflozin is contraindicated in patients with stages 3b to 5 CKD.69
SGLT-2 effect on proteinuria
Many studies have shown evidence of renoprotection with use of SGLT-2 inhibitors in patients with CKD.120,122–124 SGLT-2 inhibition may mediate their renoprotective effects by decreasing intra-glomerular pressure.125 Indeed, inhibition of SGLT-2 can normalize the NaCl concentration at the macula densa and lower glomerular hyperfiltration, thereby lowering glomerular hyperfiltration and albuminuria.125 This MOA could explain the reduction of albuminuria with SGLT-2 (dapagliflozin, canagliflozin, and empagliflozin) treatment described in clinical studies.120,122–124
In a study by Kohan et al, 122 UACR values of >1,800 mg/g during the 104-week treatment period were reported in a higher percentage of patients receiving placebo (13.3%) than patients receiving dapagliflozin 5 (10.8%) or 10 mg (9.5%), indicating decreased albuminuria with dapagliflozin. In Phase III studies, canagliflozin treatment was also associated with decreased albuminuria and an early decrease in eGFR.120,124 Yale et al124 determined a lower proportion of subjects in the canagliflozin 100 and 300 mg groups progressing from normoalbuminuria to micro- or macroalbuminuria, or from micro- to macroalbuminuria compared to those in the placebo group (5.1%, 8.3%, and 11.8%, respectively); likewise, the CANVAS substudy reported decreases in UACR from baseline at canagliflozin 100 mg (−9.6, 95% CI: −13.0 to −6.1) and 300 mg doses (−9.5, 95% CI: −12.9 to −6.1).120
In the Efficacy and Safety of Empagliflozin (BI 10773) in Patients With Type 2 Diabetes and Renal Impairment (EMPA-REG RENAL) placebo-controlled trial, small decreases in eGFR and albuminuria were shown in empagliflozin-treated T2D patients with stages 2–3 CKD.123 UACR was enhanced with empagliflozin (10 and 25 mg) after 52 weeks in patients with stage 2 CKD (empagliflozin 10 mg placebo adjusted mean difference: –184.59, P=0.0831; at 25 mg: –235.86, P=0.0257) and stage 3 CKD (empagliflozin 25 mg placebo adjusted mean difference: –183.78, P=0.0031). Moreover, greater proportions of patients with stage 3 CKD shifted from macroalbuminuria at baseline to microalbuminuria, or from microalbuminuria to no albuminuria with empaglifozin compared to placebo (32.6% vs 8.6% and 27.5% vs 21.4%, respectively).
Summary of SGLT-2 inhibitor use in renal impairment
For patients with stage 3 CKD or greater, SGLT-2 inhibitors (dapagliflozin, canagliflozin, and empagliflozin) either require dose adjustment or are contraindicated.67–69 However, a renoprotective effect has been observed with all SGLT-2 inhibitors.120,122–124
Impact of CKD on treatment algorithm
Leading on to the impact of CKD on the T2D treatment algorithm, examples of the dose maintenance and withdrawal of glucose-lowering therapies in the American Diabetes Association/European Association for the Study of Diabetes 2015 guidelines are described in Figure 1.
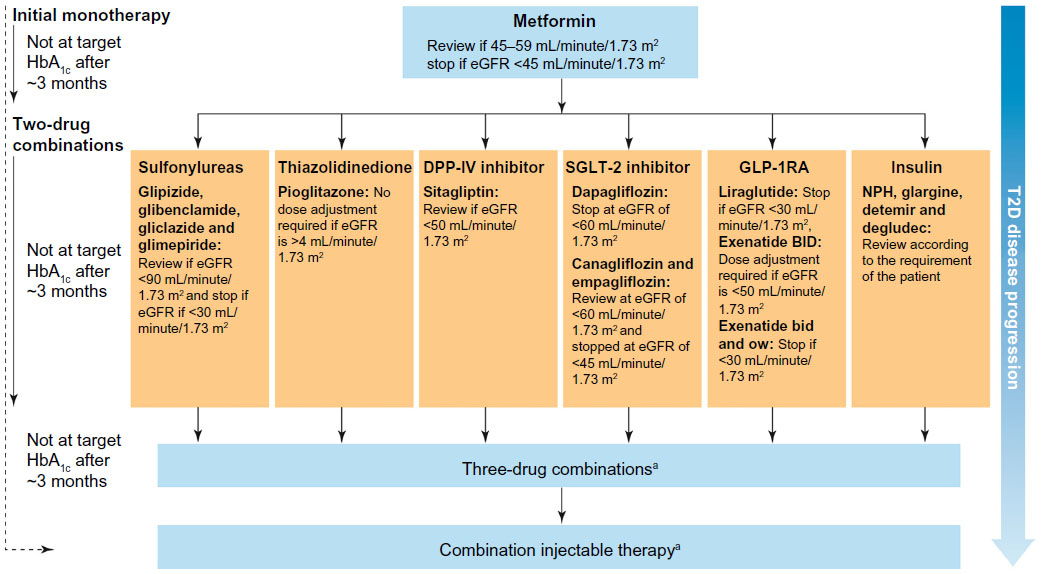 | Figure 1 The effect of CKD in the European Association for the Study of Diabetes/American Diabetes Association (EASD/ADA) treatment algorithm. |
Ongoing or data pending studies
Clinical investigations of DPP-IV inhibitor, GLP-1RA, and SGLT-2 inhibitor therapies in renal impairment or protection are being carried out in several ongoing studies. A summary is provided in Table 8.
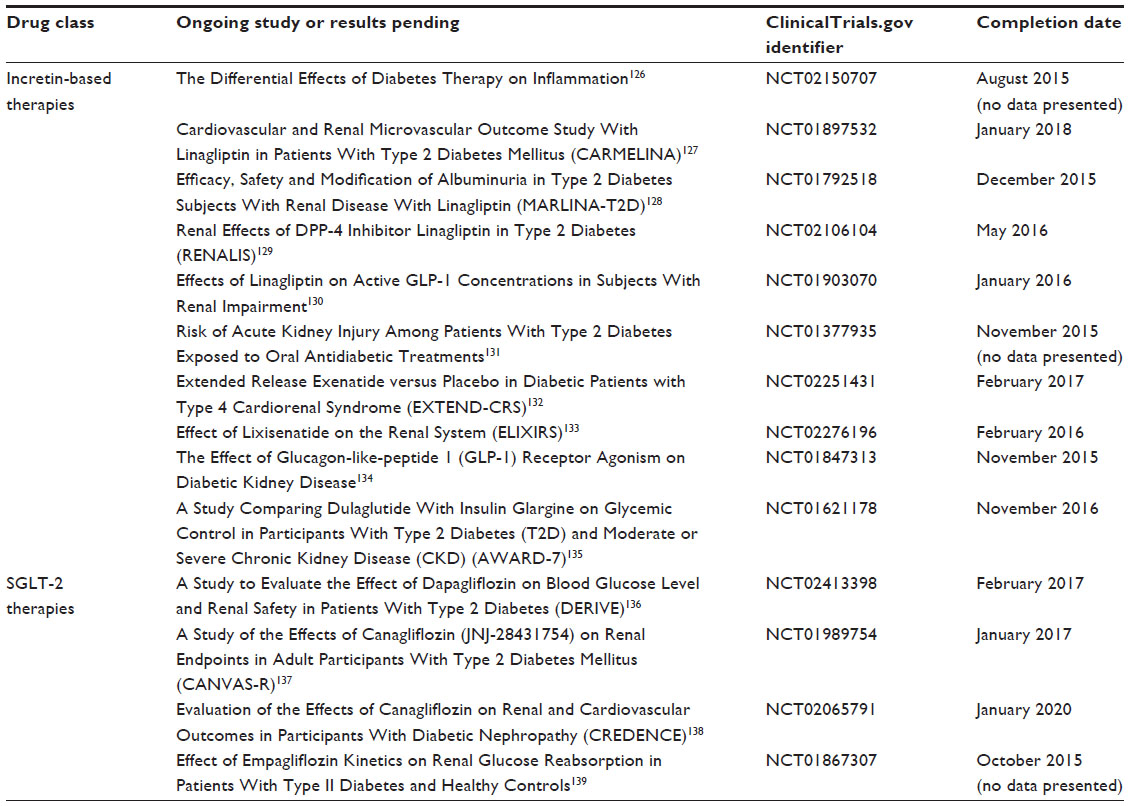 | Table 8 Ongoing or data pending studies |
Incretin-based therapies
The Differential Effects of Diabetes Therapy on Inflammation study aims to determine whether different diabetes treatments have different effects on inflammation, particularly in the kidney, and includes126 patients who need additional glycemic therapy and who are prescribed a DPP-IV inhibitor, GLP-1RA, or insulin.126
Given the relationship between CV safety and T2D and the uncertainty surrounding the CV risk of some therapies, the Cardiovascular and Renal Microvascular Outcome Study with Linagliptin in Patients With Type 2 Diabetes Mellitus (CARMELINA) will compare the CV and renal safety of linagliptin versus placebo, when added to standard care in ~8,000 patients with T2D at high CV risk.127 Clinical data have previously shown that linagliptin reduces albuminuria.88,140 The Efficacy, Safety and Modification of Albuminuria in Type 2 Diabetes Subjects with Renal Disease with Linagliptin (MARLINA) study will investigate this renoprotective effect.128 The Renal Effects of DPP-IV Inhibitor Linagliptin in Type 2 Diabetes (RENALIS) study will further investigate this drug’s action on renal physiology.129 In addition, delayed elimination of GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) in renal insufficiency may influence the PK and PD of linagliptin;141 consequently, another study will investigate the effects of linagliptin on active GLP-1 concentrations in patients with renal impairment.130 Examining the safety of a DPP-IV inhibitor in a real-world setting, a postmarketing study will compare the rates of hospitalization for acute kidney injury among patients with T2D who are new initiators of saxagliptin and those patients who are new initiators of other T2D therapies.131
Several studies are currently examining the safety and renoprotective effects of GLP-1RAs. Cardiorenal syndrome type IV is impaired cardiac function due to CKD and is characterized by ventricular hypertrophy, diastolic dysfunction, and/or increased risk of CV AEs.142 The Extended Release Exenatide versus Placebo in Diabetic Patients with Type IV Cardiorenal Syndrome study is evaluating the quantitative impact of 38 weeks of treatment on cardiac biomarkers in patients at high risk of developing cardiorenal syndrome type IV.132 Additionally, the mechanistic and clinical effects of lixisenatide on renal physiology and biomarkers in T2D patients are being explored in the Effect of LIXIsenatide on the Renal System (ELIXIRS) study.133 Meanwhile, the effect of liraglutide on CKD and kidney function in diabetes is being assessed in the Effect of Glucagon-like-peptide 1 (GLP-1) Receptor Agonism on Diabetic Kidney Disease study.134 Dulaglutide has been shown to have similar efficacy and safety to other agents in its class and provide better glycemic control than placebo,92 but there is little experience with its use in populations with renal impairment. The AWARD-7 study will provide important information in this regard by comparing the efficacy and safety of dulaglutide with insulin glargine on glycemic control in patients with T2D and stages 3–4 CKD.135
SGLT-2 inhibitors
Glycemic control and renal safety are being investigated in the Effect of Dapagliflozin on Blood Glucose Level and Renal Safety in Patients With Type 2 Diabetes study.136 In Phase III studies, canagliflozin treatment was also associated with decreased albuminuria and an early decrease in eGFR;120,124 the Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy (CREDENCE) trial is a randomized, double-blind, placebo-controlled trial intended to assess whether canagliflozin can delay the development of diabetic nephropathy.138 The renoprotective effect of canagliflozin relative to placebo will be assessed by the composite endpoint of reduction in progression to stage 5 CKD, doubling of serum creatinine, and renal or CV death. Further assessing CV risk, the Effects of Canagliflozin on Renal Endpoints in Adult Participants with Type 2 Diabetes Mellitus (CANVAS-R) study will recruit 5,875 individuals with T2D.137
The EMPA-REG RENAL trial showed that albuminuria decreased in T2D patients with stages 2–3 CKD treated with empagliflozin.123 To further investigate the impact of empagliflozin on renal kinetics, The Effect of Empagliflozin Kinetics on Renal Glucose Reabsorption in Patients with Type II Diabetes and Healthy Controls study, which has no current published data, investigated the change from baseline of renal tubular maximum reabsorptive capacity for glucose at end of empagliflozin treatment.139
Conclusion
Improved blood glucose control through pharmacological intervention can reduce the incidence and progression of CKD.8,13,14 CKD is a common complication of T2D and should inform the choice of initial and subsequent drug therapy based on individualized glycemic targets.
Apart from the thiazolidinedione pioglitazone,20 which can be used across the spectrum of CKD, there are contraindications and dose adjustments required for all the remaining conventional therapies, including metformin, sulfonylureas, meglitinides, and insulin.21–33 The inclusion of several newer therapy classes in treatment guidelines increases the likelihood that T2D will be well managed,17 with the attendant positive impact on the long-term incidence and progression of renal impairment.
Clinical studies suggest that reductions in albuminuria may be renoprotective and have been observed with all DPP-IV inhibitors,76,84,86,88,90 all SGLT-2 inhibitors, as demonstrated in the EMPA-REG study,120,122,123 and the GLP-1RAs liraglutide and exenatide.96,105 However, as with conventional therapies, not all of these newer therapies can be used when CKD is present, and some require dose adjustment with incident CKD.56–58,60–63,68,69 In contrast to other DPP-IV inhibitors,56–58,60 linagliptin can be used across the spectrum of CKD with no dose adjustment.59 No dose adjustment is required for liraglutide, albiglutide, and dulaglutide in stages 2–3 CKD;64–66 however, they are all currently contraindicated in CKD stages 4–5.61–66 At CKD stages of 3 or more, the SGLT-2 inhibitors dapagliflozin, canagliflozin, and empagliflozin either require dose adjustment or are contraindicated.67–69
Data from ongoing clinical trials with larger populations are awaited to further determine the safety and efficacy profile of DPP-4 inhibitors, GLP-1RAs, and SGLT-2 inhibitors in patients with T2D and CKD.126–139 Ongoing trials, such as CARMELINA, MARLINA, ELIXIRS, A Study Comparing Dulaglutide With Insulin Glargine on Glycemic Control in Participants With Type 2 Diabetes (T2D) and Moderate or Severe Chronic Kidney Disease (CKD) (AWARD-7), CREDENCE, and CANVAS-R, in particular, will help to confirm the position of these new therapy classes in patients with CKD.
Acknowledgments
The authors acknowledge support from the UK National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care – East Midlands (NIHR CLAHRC – EM), the Leicester Clinical Trials Unit, and the NIHR Leicester-Loughborough Diet, Lifestyle and Physical Activity Biomedical Research Unit, which is a partnership between University Hospitals of Leicester NHS Trust, Loughborough University, and the University of Leicester. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. The authors thank Watermeadow Medical for assistance with preparation of this manuscript (funded by Novo Nordisk).
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
Professor Melanie Davies has acted as a consultant, advisory board member, and speaker for Novo Nordisk, Sanofi-Aventis, Eli Lilly, Merck Sharp and Dohme, Boehringer Ingelheim, AstraZeneca, and Janssen, and as a speaker for Mitsubishi Tanabe Pharma Corporation and Takeda. She has received grants in support of investigator-initiated trials from Novo Nordisk, Sanofi-Aventis, and Eli Lilly. Dr Sudesna Chatterjee has received speaker fees and educational funding from Janssen, Eli Lilly, Novo Nordisk, Astra Zeneca, and Boehringer Ingelheim. Professor Kamlesh Khunti has received funds for research and honoraria for speaking at meetings from, and served on advisory boards for, Astra Zeneca, Boehringer Ingelheim, Lilly, Novartis, Roche, Servier, Sanofi Aventis, MSD, Janssen, and Novo Nordisk. The authors report no other conflicts of interest in this work.
References
Olyaei AJ, Steffl JL. A quantitative approach to drug dosing in chronic kidney disease. Blood Purif. 2011;31(1–3):138–145. | |
Ojo A. Addressing the global burden of chronic kidney disease through clinical and translational research. Trans Am Clin Climatol Assoc. 2014;125:229–243; discussion 243–246. | |
Tedla FM, Brar A, Browne R, Brown C. Hypertension in chronic kidney disease:navigating the evidence. Int J Hypertens. 2011;2011:132405. | |
Olechnowicz-Tietz S, Gluba A, Paradowska A, Banach M, Rysz J. The risk of atherosclerosis in patients with chronic kidney disease. Int Urol Nephrol. 2013;45(6):1605–1612. | |
Tuttle KR, Bakris GL, Bilous RW, et al. Diabetic kidney disease:a report from an ADA Consensus Conference. Diabetes Care. 2014;37(10):2864–2883. | |
Savarese G, Dei Cas A, Rosano G, et al. Reduction of albumin urinary excretion is associated with reduced cardiovascular events in hypertensive and/or diabetic patients. A meta-regression analysis of 32 randomized trials. Int J Cardiol. 2014;172(2):403–410. | |
Kidney Disease:Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl. 2013;3(1):1–163. | |
Plantinga LC, Crews DC, Coresh J, et al. Prevalence of chronic kidney disease in US adults with undiagnosed diabetes or prediabetes. Clin J Am Soc Nephrol. 2010;5(4):673–682. | |
Hippisley-Cox J, Coupland C. Predicting the risk of chronic kidney disease in men and women in England and Wales:prospective derivation and external validation of the QKidney Scores. BMC Fam Pract. 2010;11:49. | |
Fowler MJ. Microvascular complications of diabetes. Clin Diabetes. 2008;26(2):77–82. | |
International Diabetes Federation. IDF Diabetes Atlas. 7th edn. Brussels, Belgium:International Diabetes Federation; 2015. | |
Lyssenko V, Laakso M. Genetic screening for the risk of type 2 diabetes:worthless or valuable? Diabetes Care. 2013;36(Suppl 2):S120–S126. | |
Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–853. | |
Perkovic V, Heerspink HL, Chalmers J, et al. Intensive glucose control improves kidney outcomes in patients with type 2 diabetes. Kidney Int. 2013;83(3):517–523. | |
Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348(5):383–393. | |
McIntosh B, Cameron C, Singh SR, et al. Second-line therapy in patients with type 2 diabetes inadequately controlled with metformin monotherapy:a systematic review and mixed-treatment comparison meta-analysis. Open Med. 2011;5(1):e35–e48. | |
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015:a patient-centered approach:update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. | |
Yale JF. Oral antihyperglycemic agents and renal disease:new agents, new concepts. J Am Soc Nephrol. 2005;16(Suppl 1):S7–S10. | |
Cavanaugh K. Diabetes management issues for patients with chronic kidney disease. Clin Diabetes. 2007;25(3):90–97. | |
Takeda. Actos (pioglitazone) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/4236. Accessed November 2015. | |
Merck Serono. Glucophage (metformin) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/1043. Accessed November 2015. | |
Pfizer Limited. Minodiab (glipizide) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/ 9851. Accessed November 2015. | |
Wockhardt UK Limited. Glibenclamide Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/30411. Accessed November 2015. | |
Wockhardt UK Limited. Gliclazide Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/ 27762. Accessed November 2015. | |
Accord Healthcare Limited. Glimepiride Summary of Product Characteristics. 2014. Available from: https://www.medicines.org.uk/emc/medicine/25813. Accessed November 2015. | |
Novo Nordisk Limited. Prandin (repaglinide) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/18980. Accessed November 2015. | |
Eli Lilly and Company Limited. Humulin I (isophane insulin) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/3425. Accessed November 2015. | |
Sanofi-aventis. Lantus (insulin glargine) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/25506. Accessed November 2015. | |
Novo Nordisk Limited. Levemir (insulin detemir) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/14584. Accessed November 2015. | |
Novo Nordisk Limited. Tresiba (insulin degludec) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/27360. Accessed November 2015. | |
Eli Lilly and Company Limited. Humalog (insulin lispro) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/30005. Accessed November 2015. | |
Sanofi. Apidra (insulin glulisine) Summary of Product Characteristics; 2013. Available from: https://www.medicines.org.uk/emc/medicine/26476. Accessed November 2015. | |
Novo Nordisk Limited. NovoMix (insulin aspart) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/8591. Accessed November 2015. | |
Actavis UK Ltd. Acarbose Summary of Product Characteristics; 2013. Available from: https://www.medicines.org.uk/emc/medicine/27829. Accessed February 2016. | |
Brown JB, Pedula K, Barzilay J, Herson MK, Latare P. Lactic acidosis rates in type 2 diabetes. Diabetes Care. 1998;21(10):1659–1663. | |
Rojas LB, Gomes MB. Metformin:an old but still the best treatment for type 2 diabetes. Diabetol Metab Syndr. 2013;5(1):6. | |
National Institute for Health and Care Excellence (NICE). [The management of type 2 diabetes (CG87)]. London: National Institute for Clinical Excellence [Published May 2009]. Available from: http://guidance.nice.org.uk/cg87. Accessed June 16, 2015. | |
Inzucchi SE, Lipska KJ, Mayo H, Bailey CJ, McGuire DK. Metformin in patients with type 2 diabetes and kidney disease: a systematic review. JAMA. 2014;312(24):2668–2675. | |
National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850–886. | |
Kasliwal R, Wilton LV, Shakir SA. Monitoring the safety of pioglitazone: results of a prescription-event monitoring study of 12,772 patients in England. Drug Saf. 2008;31(10):839–850. | |
Shaya FT, Lu Z, Sohn K, Weir MR. Thiazolidinediones and cardiovascular events in high-risk patients with type-2 diabetes mellitus: a comparison with other oral antidiabetic agents. P T. 2009;34(9):490–501. | |
Rosak C, Mertes G. Critical evaluation of the role of acarbose in the treatment of diabetes:patient considerations. Diabetes Metab Syndr Obes. 2012;5:357–367. | |
AstraZeneca AB. Symlin (pramlintide acetate) Prescribing Information; 2014. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/021332s025lbl.pdf. Accessed February 2016. | |
Defronzo RA. Bromocriptine:a sympatholytic, d2-dopamine agonist for the treatment of type 2 diabetes. Diabetes Care. 2011;34(4):789–794. | |
VeroScience. Cycloset (bromocriptine) Prescribing Information; 2016. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2016/020866s009lbl.pdf. Accessed February 2016. | |
Sanofi. Toujeo (insulin glargine) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/30586. Accessed November 2015. | |
Simpson D, McCormack PL, Keating GM, Lyseng-Williamson KA. Insulin lispro:a review of its use in the management of diabetes mellitus. Drugs. 2007;67(3):407–434. | |
Dreyer M, Prager R, Robinson A, et al. Efficacy and safety of insulin glulisine in patients with type 1 diabetes. Horm Metab Res. 2005;37(11):702–707. | |
Owens D, Vora J. Insulin aspart:a review. Expert Opin Drug Metab Toxicol. 2006;2(5):793–804. | |
Duckworth WC, Bennett RG, Hamel FG. Insulin degradation:progress and potential. Endocr Rev. 1998;19(5):608–624. | |
Goykhman S, Drincic A, Desmangles JC, Rendell M. Insulin glargine:a review 8 years after its introduction. Expert Opin Pharmacother. 2009;10(4):705–718. | |
Iglesias P, Diez JJ. Insulin therapy in renal disease. Diabetes Obes Metab. 2008;10(10):811–823. | |
Jacobsen L, Popescu G, Plum A. Pharmacokinetics of insulin detemir in subjects with renal or hepatic impairment. Diabetologia. 2002;45:A259–A260. | |
Kiss I, Arold G, Roepstorff C, Bottcher SG, Klim S, Haahr H. Insulin degludec:pharmacokinetics in patients with renal impairment. Clin Pharmacokinet. 2014;53(2):175–183. | |
Holmes G, Galitz L, Hu P, Lyness W. Pharmacokinetics of insulin aspart in obesity, renal impairment, or hepatic impairment. Br J Clin Pharmacol. 2005;60(5):469–476. | |
Merck Sharp and Dohme Limited. Januvia (sitagliptin) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/19609. Accessed November 2015. | |
Novartis Pharmaceuticals UK Ltd. Galvus (vildagliptin) Summary of Product Characteristics; 2016. Available from: https://www.medicines.org.uk/emc/medicine/20734. Accessed January 2016. | |
AstraZeneca UK Limited. Onglyza (saxagliptin) Summary of Product Characteristics. 2015; Available from: https://www.medicines.org.uk/emc/medicine/22315. Accessed February 2016. | |
Boehringer Ingelheim Limited. Trajenta (linagliptin) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/25000. Accessed November 2015. | |
Takeda UK Ltd. Vipidia (alogliptin) Summary of product characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/28513. Accessed November 2015. | |
AstraZeneca UK Limited. Byetta (exenatide) Summary of Product Characteristics. 2016. Available from: https://www.medicines.org.uk/emc/medicine/19257. Accessed January 2016. | |
AstraZeneca UK Limited. Bydureon (exenatide) Summary of Product Characteristics; 2016. Available from: https://www.medicines.org.uk/emc/medicine/24665. Accessed February 2016. | |
Sanofi-aventis. Lyxumia (lixisenatide) Summary of Product Characteristics; 2014. Available from: https://www.medicines.org.uk/emc/medicine/27405. Accessed November 2015. | |
Novo Nordisk Limited. Victoza (liraglutide) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/21986. Accessed November 2015. | |
GlaxoSmithKline Trading Services Limited. Eperzan (albiglutide) Summary of Product Characteristics; 2016. Available from: https:// www.medicines.org.uk/emc/medicine/31399. Accessed February 2016. | |
Eli Lilly and Company Limited. Trulicity (dulaglutide) Summary of Product Characteristics; 2016. Available from: https://www.medicines.org.uk/emc/medicine/29747. Accessed February 2016. | |
AstraZeneca UK Limited. Forxiga (dapagliflozin) Summary of Product Characteristics; 2014 Available from: https://www.medicines.org.uk/emc/medicine/27188. Accessed November 2015. | |
Janssen-Cilag Ltd. Invokana (canagliflozin) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/28400. Accessed February 2016. | |
Boehringer Ingelheim Limited. Jardiance (empagliflozin) Summary of Product Characteristics; 2015. Available from: https://www.medicines.org.uk/emc/medicine/28973. Accessed November 2015. | |
Muskiet MH, Smits MM, Morsink LM, Diamant M. The gut-renal axis:do incretin-based agents confer renoprotection in diabetes? Nat Rev Nephrol. 2014;10(2):88–103. | |
Cheng D, Fei Y, Liu Y, et al. Efficacy and safety of dipeptidyl peptidase-4 inhibitors in type 2 diabetes mellitus patients with moderate to severe renal impairment:a systematic review and meta-analysis. PLoS One. 2014;9(10):e111543. | |
Game F. Novel hypoglycaemic agents:considerations in patients with chronic kidney disease. Nephron Clin Pract. 2014;126(1):14–18. | |
Amori RE, Lau J, Pittas AG. Efficacy and safety of incretin therapy in type 2 diabetes:systematic review and meta-analysis. JAMA. 2007;298(2):194–206. | |
Tricco AC, Antony J, Khan PA, et al. Safety and effectiveness of dipeptidyl peptidase-4 inhibitors versus intermediate-acting insulin or placebo for patients with type 2 diabetes failing two oral antihyperglycaemic agents: a systematic review and network meta-analysis. BMJ Open. 2014;4(12):e005752. | |
Brown NJ, Byiers S, Carr D, Maldonado M, Warner BA. Dipeptidyl peptidase-IV inhibitor use associated with increased risk of ACE inhibitor-associated angioedema. Hypertension. 2009;54(3):516–523. | |
Deacon CF. Dipeptidyl peptidase-4 inhibitors in the treatment of type 2 diabetes:a comparative review. Diabetes Obes Metab. 2011;13(1):7–18. | |
Bergman AJ, Cote J, Yi B, et al. Effect of renal insufficiency on the pharmacokinetics of sitagliptin, a dipeptidyl peptidase-4 inhibitor. Diabetes Care. 2007;30(7):1862–1864. | |
He YL, Flannery B, Wang Y et al. The influence of renal impairment on pharmacokinetics of vildagliptin (Abstract PIII-86). Clin Pharmacol Ther. 2007;81(Suppl 1):S113. | |
He YL, Kulmatycki K, Zhang Y, et al. Pharmacokinetics of vildagliptin in patients with varying degrees of renal impairment. Int J Clin Pharmacol Ther. 2013;51(9):693–703. | |
Boulton DW, Li L, Frevert EU, et al. Influence of renal or hepatic impairment on the pharmacokinetics of saxagliptin. Clin Pharmacokinet. 2011;50(4):253–265. | |
Graefe-Mody U, Friedrich C, Port A, et al. Effect of renal impairment on the pharmacokinetics of the dipeptidyl peptidase-4 inhibitor linagliptin(*). Diabetes Obes Metab. 2011;13(10):939–946. | |
Karim A, Fleck P, Hetman L, et al. Single-dose pharmacokinetics of the dipeptidyl peptidase-4 inhibitor alogliptin in subjects with renal impairment (Abstract 538-P). Diabetes. 2008;57(Suppl 1):A160. | |
Green JB, Bethel MA, Armstrong PW, et al. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232–242. | |
Mori H, Okada Y, Arao T, Tanaka Y. Sitagliptin improves albuminuria in patients with type 2 diabetes mellitus. J Diabetes Investig. 2014;5(3):313–319. | |
He H, Tran P, Yin H, et al. Absorption, metabolism, and excretion of [14C]vildagliptin, a novel dipeptidyl peptidase 4 inhibitor, in humans. Drug Metab Dispos. 2009;37(3):536–544. | |
Watanabe M, Furuya F, Kobayashi T. DPP-4 inhibitor vildagliptin reduces urinary albumin excretion in type 2 diabetic patients with microalbuminuria. Endocrine Abstracts. 2012;29:P687. | |
Udell JA, Bhatt DL, Braunwald E, et al. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes and moderate or severe renal impairment:observations from the SAVOR-TIMI 53 Trial. Diabetes Care. 2015;38(4):696–705. | |
Groop PH, Cooper ME, Perkovic V, Emser A, Woerle HJ, von Eynatten M. Linagliptin lowers albuminuria on top of recommended standard treatment in patients with type 2 diabetes and renal dysfunction. Diabetes Care. 2013;36(11):3460–3468. | |
Dineen L, Law C, Scher R, Pyon E. Alogliptin (nesina) for adults with type-2 diabetes. P T. 2014;39(3):186–202. | |
Sakata K, Hayakawa M, Yano Y, et al. Efficacy of alogliptin, a dipeptidyl peptidase-4 inhibitor, on glucose parameters, the activity of the advanced glycation end product (AGE) – receptor for AGE (RAGE) axis and albuminuria in Japanese type 2 diabetes. Diabetes Metab Res Rev. 2013;29(8):624–630. | |
Ahren B. The future of incretin-based therapy: novel avenues – novel targets. Diabetes Obes Metab. 2011;13(Suppl 1):158–166. | |
Kuritzky L, Umpierrez G, Ekoe JM, Mancillas-Adame L, Lando LF. Safety and efficacy of dulaglutide, a once weekly GLP-1 receptor agonist, for the management of type 2 diabetes. Postgrad Med. 2014; 126(6):60–72. | |
Trujillo JM, Nuffer W, Ellis SL. GLP-1 receptor agonists:a review of head-to-head clinical studies. Ther Adv Endocrinol Metab. 2015;6(1):19–28. | |
Li L, Shen J, Bala MM, et al. Incretin treatment and risk of pancreatitis in patients with type 2 diabetes mellitus: systematic review and meta-analysis of randomised and non-randomised studies. BMJ. 2014;348:g2366. | |
Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol. 2012;8(12):728–742. | |
Zhang H, Zhang X, Hu C, Lu W. Exenatide reduces urinary transforming growth factor-beta1 and type IV collagen excretion in patients with type 2 diabetes and microalbuminuria. Kidney Blood Press Res. 2012;35(6):483–488. | |
Imamura S, Hirai K, Hirai A. The glucagon-like peptide-1 receptor agonist, liraglutide, attenuates the progression of overt diabetic nephropathy in type 2 diabetic patients. Tohoku J Exp Med. 2013;231(1):57–61. | |
Linnebjerg H, Kothare PA, Park S, et al. Effect of renal impairment on the pharmacokinetics of exenatide. Br J Clin Pharmacol. 2007; 64(3):317–327. | |
Liu Y, Ruus P. Pharmacokinetics and safety of the GLP-1 agonist AVE0010 in patients with renal impairment (abstract). Diabetes. 2009;59:A149–A150. | |
Jacobsen LV, Hindsberger C, Robson R, Zdravkovic M. Effect of renal impairment on the pharmacokinetics of the GLP-1 analogue liraglutide. Br J Clin Pharmacol. 2009;68(6):898–905. | |
Loghin C, de la Peña A, Cui X, Zhang X, Geiser JS, Chien JY. Pharmacokinetics of once weekly dulaglutide in special populations. Diabetologia. 2014;57:(Suppl 1):S349. | |
Young MA, Wald JA, Matthews JE, Yang F, Reinhardt RR. Effect of renal impairment on the pharmacokinetics, efficacy, and safety of albiglutide. Postgrad Med. 2014;126(3):35–46. | |
Gedulin BR, Nikoulina SE, Smith PA, et al. Exenatide (exendin-4) improves insulin sensitivity and {beta}-cell mass in insulin-resistant obese fa/fa Zucker rats independent of glycemia and body weight. Endocrinology. 2005;146(4):2069–2076. | |
Barnett AH. Lixisenatide:evidence for its potential use in the treatment of type 2 diabetes. Core Evid. 2011;6:67–79. | |
Zavattaro M, Caputo M, Sama MT, et al. One-year treatment with liraglutide improved renal function in patients with type 2 diabetes: a pilot prospective study. Endocrine. 2015;50(3):620–626. | |
Davies MJ, Bain SC, Atkin SL, et al. Efficacy and safety of liraglutide versus placebo as add-on to glucose-lowering therapy in patients with type 2 diabetes and moderate renal impairment (LIRA-RENAL):A randomized clinical trial. Diabetes Care. 2016;39(2):222–230. | |
Garber AJ. Long-acting glucagon-like peptide 1 receptor agonists: a review of their efficacy and tolerability. Diabetes Care. 2011;34(Suppl 2):S279–284. | |
Matthews JE, Stewart MW, De Boever EH, et al. Pharmacodynamics, pharmacokinetics, safety, and tolerability of albiglutide, a long-acting glucagon-like peptide-1 mimetic, in patients with type 2 diabetes. J Clin Endocrinol Metab. 2008;93(12):4810–4817. | |
Bays H. From victim to ally:the kidney as an emerging target for the treatment of diabetes mellitus. Curr Med Res Opin. 2009; 25(3):671–681. | |
Chao EC. SGLT-2 inhibitors: A new mechanism for glycemic control. Clin Diabetes. 2014;32(1):4–11. | |
Ferrannini E, Solini A. SGLT2 inhibition in diabetes mellitus:rationale and clinical prospects. Nat Rev Endocrinol. 2012;8(8):495–502. | |
Nauck MA. Update on developments with SGLT2 inhibitors in the management of type 2 diabetes. Drug Des Devel Ther. 2014;8:1335–1380. | |
Peters AL, Buschur EO, Buse JB, Cohan P, Diner JC, Hirsch IB. Euglycemic diabetic ketoacidosis: A potential complication of treatment with sodium-glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1687–1693. | |
Kasichayanula S, Liu X, Pe Benito M, et al. The influence of kidney function on dapagliflozin exposure, metabolism and pharmacodynamics in healthy subjects and in patients with type 2 diabetes mellitus. Br J Clin Pharmacol. 2013;76(3):432–444. | |
Stein P, Berg JK, Morrow L, et al. Canagliflozin, a sodium glucose co-transporter 2 inhibitor, reduces post-meal glucose excursion in patients with type 2 diabetes by a non-renal mechanism:results of a randomized trial. Metabolism. 2014;63(10):1296–1303. | |
Sarnoski-Brocavich S, Hilas O. Canagliflozin (Invokana), a novel oral agent for type-2 diabetes. P T. 2013;38(11):656–666. | |
Inagaki N, Kondo K, Yoshinari T, et al. Pharmacokinetic and pharmacodynamic profiles of canagliflozin in Japanese patients with type 2 diabetes mellitus and moderate renal impairment. Clin Drug Investig. 2014;34(10):731–742. | |
Macha S, Mattheus M, Halabi A, Pinnetti S, Woerle HJ, Broedl UC. Pharmacokinetics, pharmacodynamics and safety of empagliflozin, a sodium glucose cotransporter 2 (SGLT2) inhibitor, in subjects with renal impairment. Diabetes Obes Metab. 2014;16(3):215–222. | |
Komoroski B, Vachharajani N, Boulton D, et al. Dapagliflozin, a novel SGLT2 inhibitor, induces dose-dependent glucosuria in healthy subjects. Clin Pharmacol Ther. 2009;85(5):520–526. | |
Neal B, Perkovic V, de Zeeuw D, et al. Efficacy and safety of canagliflozin, an inhibitor of sodium-glucose cotransporter 2, when used in conjunction with insulin therapy in patients with type 2 diabetes. Diabetes Care. 2015;38(3):403–411. | |
Inagaki N, Kondo K, Yoshinari T, et al. Pharmacokinetic and pharmacodynamic profiles of canagliflozin in Japanese patients with type 2 diabetes mellitus and moderate renal impairment. Clin Drug Investig. 2014;34(10):731–742. | |
Kohan DE, Fioretto P, Tang W, List JF. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. 2014;85(4):962–971. | |
Barnett AH, Mithal A, Manassie J, et al; EMPA-REG Renal Trial investigators. Efficacy and safety of empagliflozin added to existing antidiabetes treatment in patients with type 2 diabetes and chronic kidney disease:a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014;2(5):369–384. | |
Yale JF, Bakris G, Cariou B, et al. Efficacy and safety of canagliflozin in subjects with type 2 diabetes and chronic kidney disease. Diabetes Obes Metab. 2013;15(5):463–473. | |
Vallon V. The mechanisms and therapeutic potential of SGLT2 inhibitors in diabetes mellitus. Annu Rev Med. 2015;66:255–270. | |
University College Dublin. The differential effects of diabetes therapy on inflammation. Available from: https://clinicaltrials.gov/ct2/show/NCT02150707?term=NCT02150707&rank=1. NLM identifier: NCT02150707. Accessed September 30, 2015. | |
Boehringer Ingelheim. Cardiovascular and Renal Microvascular Outcome Study With Linagliptin in Patients With Type 2 Diabetes Mellitus (CARMELINA). Available from: https://clinicaltrials.gov/ct2/show/NCT01897532?term=NCT01897532&rank=1. NLM identifier: NCT01897532. Accessed September 30, 2015. | |
Boehringer Ingelheim. MARLINA – T2D :Efficacy, Safety and Modification of Albuminuria in Type 2 Diabetes Subjects With Renal Disease With LINAgliptin. Available from: https://clinicaltrials.gov/ct2/show/record/NCT01792518. NLM identifier: NCT01792518. Accessed November 30, 2015. | |
VU University Medical Center. Renal Effects of DPP-4 Inhibitor Linagliptin in Type 2 Diabetes (RENALIS). Available from: https://clinicaltrials.gov/ct2/show/NCT02106104?term=NCT02106104& rank=1. NLM identifier: NCT02106104. Accessed November 30, 2015. | |
Profil Institut für Stoffwechselforschung GmbH. Effects of Linagliptin on Active GLP-1 Concentrations in Subjects With Renal Impairment. Available from: https://clinicaltrials.gov/ct2/show/NCT01903070?term=NCT01903070&rank=1. NLM identifier: NCT01903070. Accessed November 30, 2015. | |
Bristol-Myers Squibb. Risk of Acute Kidney Injury Among Patients With Type 2 Diabetes Exposed to Oral Antidiabetic Treatments. Available from: https://clinicaltrials.gov/ct2/show/NCT01377935?term=Comparison+of+Risk+of+Hospitalization+for+Acute+Kidney+Injury+Between+Patients+With+Type+2+Diabetes+Initiating+Saxagliptin&rank=1. NLM identifier: NCT01377935. Accessed November 30, 2015. | |
Baylor Research Institute. Extended Release Exenatide Versus Placebo In Diabetic Patients With Type 4 Cardiorenal Syndrome. Available from: https://clinicaltrials.gov/ct2/show/NCT02251431. NLM identifier: NCT02251431. Accessed November 30, 2015. | |
VU University Medical Center. Effect of LIXIsenatide on the Renal System (ELIXIRS). Available from: https://clinicaltrials.gov/ct2/show/NCT02276196. NLM identifier: NCT02276196. Accessed November 30, 2015. | |
Karl Neff, University College Dublin. The Effect of Glucagon-like-peptide 1 (GLP-1) Receptor Agonism on Diabetic Kidney Disease. Available from: https://clinicaltrials.gov/ct2/show/NCT01847313?term=The+Effect+of+Glucagon-like-peptide+1+%28GLP-1%29+Receptor+Agonism+on+Diabetic+Kidney+Disease&rank=1. NLM identifier: NCT01847313. Accessed November 30, 2015. | |
Madiraju AK, Erion DM, Rahimi Y, et al. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature. 2014;510(7506):542–546. | |
AstraZeneca AB. Study to Evaluate the Effect of Dapagliflozin on Blood Glucose Level and Renal Safety in Patients With Type 2 Diabetes (DERIVE). Available from: https://clinicaltrials.gov/ct2/show/NCT02413398?term=Study+to+Evaluate+the+Effect+of+Dapagliflozin+on+Blood+Glucose+Level+and+Renal+Safety+in+Patients+With+Type+2+Diabetes&rank=1. NLM identifier: NCT02413398. Accessed November 30, 2015. | |
Janssen Research and Development, LLC. A Study of the Effects of Canagliflozin (JNJ-28431754) on Renal Endpoints in Adult Participants With Type 2 Diabetes Mellitus (CANVAS-R). Available from: https://clinicaltrials.gov/ct2/show/record/NCT01989754. NLM identifier: NCT01989754. Accessed November 30, 2015. | |
Janssen Research and Development, LLC. Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy (CREDENCE). Available from: https://clinicaltrials.gov/ct2/show/NCT02065791?term=NCT02065791&rank=1. NLM identifier: NCT02065791. Accessed November 30, 2015. | |
Boehringer Ingelheim. Effect of Empagliflozin Kinetics on Renal Glucose Reabsorption in Patients With Type II Diabetes and Healthy Controls. Available from: https://clinicaltrials.gov/ct2/show/NCT01867307?term=Effect+of+Empagliflozin+Kinetics+on+Renal+Glucose+Reabsorption+in+Patients+With+Type+II+Diabetes+and+Healthy+Controls&rank=1. NLM identifier: NCT01867307. Accessed November 30, 2015. | |
Groop PH, Del Prato S, Taskinen MR, et al. Linagliptin treatment in subjects with type 2 diabetes with and without mild-to-moderate renal impairment. Diabetes Obes Metab. 2014;16(6):560–568. | |
Meier JJ, Nauck MA, Kranz D, et al. Secretion, degradation, and elimination of glucagon-like peptide 1 and gastric inhibitory polypeptide in patients with chronic renal insufficiency and healthy control subjects. Diabetes. 2004;53(3):654–662. | |
Clementi A, Virzi GM, Goh CY, et al. Cardiorenal syndrome type 4: a review. Cardiorenal Med. 2013;3(1):63–70. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.