")
Back to Journals » Patient Preference and Adherence » Volume 14
The Translation, Reliability and Validity of the Chinese Version of the Hill–Bone Compliance to High Blood Pressure Therapy Scale in Adults with Hypertension
Authors Pan J , Hu B, Wu L, Wang H, Lei T, Liu Z
Received 22 June 2020
Accepted for publication 2 September 2020
Published 9 October 2020 Volume 2020:14 Pages 1853—1860
DOI https://doi.org/10.2147/PPA.S268031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Jingjing Pan,1 Bin Hu,1 Lian Wu,2 Huichuan Wang,1 Tao Lei,3 Zhiyu Liu4
1Department of Pharmacy, Xi’an Fourth Hospital, Xi’an, People’s Republic of China; 2Department of Ophthalmology, Xi’an Fourth Hospital, Xi’an, People’s Republic of China; 3Department of Neurology, Xi’an Fourth Hospital, Xi’an, People’s Republic of China; 4Department of Orthopedics, Xi’an Fourth Hospital, Xi’an, People’s Republic of China
Correspondence: Bin Hu
Department of Pharmacy, Xi’an Fourth Hospital, 21 JieFang Road, Xi’an 710004, People’s Republic of China
Tel +86 29 87401581 Ext 029
Email [email protected]
Lian Wu
Department of Ophthalmology, Xi’an Fourth Hospital, Xi’an, People’s Republic of China
Tel +86 29 87480843 Ext 029
Email [email protected]
Objective: To assess the reliability and validity of the Chinese version of the Hill–Bone compliance to high blood pressure therapy scale (HBTS) for use in adults with hypertension in China.
Methods: To develop a Chinese version of the study scale, it was translated into Chinese then back-translated into English. The final version was used in a survey conducted between Jan and June 2019 in a hospital in Xi’an, China. Reliability was assessed by using the Cronbach’s alpha as a measure of analyzing the internal consistency. Exploratory factor analysis (EFA) was performed to assess the validity of the Chinese scale.
Results: The EFA revealed a four-component structure representing two of medication taking; appointment keeping and reduced sodium intake. Percentages of explained variance were 37.55%, 52.77%, 65.24% and 73.97%, respectively. All questions have factor loadings > 0.4. The Cronbach’s alpha score for the entire questionnaire was 0.857.
Conclusion: The Chinese Hill–Bone scale (HBTS-C) is a valid and reliable instrument for measuring adherence among Chinese with hypertension. Use of this screening tool for the assessment of adherence to hypertension treatment is recommended.
Keywords: Hill–Bone scale, hypertension, adherence, psychometrics
Introduction
High blood pressure (HBP) is considered one of the most significant public health problems worldwide and reported as the major risk factor for a number of serious health conditions, including cardiovascular disease,1,2 stroke,3,4 and chronic kidney disease.5,6 According to the World Health Organization (WHO), hypertension affects 1.13 billion people around the world (20% of women and 24% of men).7 We estimated that between 2000 and 2010, the global age-standardized prevalence of hypertension in adults aged ≥20 years increased by 5.2%. The prevalence of hypertension is high and increasing, whereas awareness, treatment and control of hypertension are unacceptably low worldwide, particularly in low and middle-income countries. The most recent global estimates suggest that in 2010, only 45.6% of people with hypertension were aware of their condition, only 36.9% were receiving treatment and only 13.8% had achieved BP control (defined as systolic BP <140 mmHg and diastolic BP <90 mmHg).8 In China, one-third of adults were diagnosed with hypertension, however, the control rate was low.9
The influence of non-adherence to treatment regimens is the most important reason for uncontrolled blood pressure.10 Treatment adherence is defined as the process by which patients follow the agreed treatment regimens with their physician.11 Several methods are available for the assessment of adherence behaviors in hypertensive patients, which are categorized as direct and indirect methods. Direct methods include pill counting, reminder packaging, mobile health, electronic medication monitoring, measurement of drug concentrations in bodily fluids, etc.12–18 Indirect methods mainly include self-reported questionnaires and scales. Although each available method has its own advantages and disadvantages, the self-reported method is the the most commonly used method to assess adherence behaviors, because it is economical and simple to gather information.19 There are a variety of self-reported scales used to measure adherence in hypertensive patients.20–22 The most commonly used self-reported scale is the Morisky Medication Adherence Scale (MMAS),23 however, it has limitations because it does not include items related with lifestyle modifications. Furthermore, it’s difficult to access the MMAS questionnaires because of the high price of its license.
The Hill–Bone compliance to high blood pressure therapy scale (HBTS) is also one of the most broadly used adherence scales. In addition to measuring medication adherence, it also measures lifestyles (salt intake) and appointment keeping in contrast to the MMAS.21 HBTS has passed validation and psychometric evaluation in various populations and cultures including Polish, Turkish and Korean-Americans.24–26 Currently the Chinese Hill–Bone scale (HBTS-C) does not exist. The aim of the present research was to develop and assess the reliability and validity of the HBTS-C in order to use it in Chinese hypertension patients in future studies.
Materials and Methods
Study Objectives
We set out to translate the English-language version of the Hill–Bone scale into Chinese and conduct psychometric validation to assess its potential applicability in Chinese patients. Therefore, reliability was estimated, and construct validity based on the results of the expolatory factor analysis (EFA) were performed.
Questionnaire
HBTS was developed by Kim and tested among patients with hypertension. The 14 items included in the final questionnaire comprise three subscales: 1) medication taking (9 items); 2) appointment keeping (2 items); and 3) reduced sodium intake (3 items). Each item is a four point Likert type scale. The score ranged from 1 (all the time) to 4 (none of the time). Item 6 needed reverse coding on analysis. Item scores are summed to produce an overall adherence score of 14–56, with higher scores indicating better adherence.21
Translation and Cultural Adaptation
Permission for translation of the HBTS into Chinese was obtained from the original developer of the English version of the HBTS (Table 1). It was then translated into Chinese language and back-translated into English. The translation process was based on the five-stage process and proceeded as follows: 1) forward translation; 2) synthesis of translated versions (target language); 3) backward translation (blind); 4) synthesis of translated versions (original language); 5) pretest of synthesized translated version: cognitive debriefing and cultural equivalence.27 Forward translation of the questionnaire from English to Chinese was conducted by two bilingual individuals. One of the translators was an English teacher and was not aware of the goal of the questionnaire while the other translator had a medical background and was familiar with the study. They independently translated the original English measures into Chinese, and then a third translator synthesized the two translated versions into one, discussing and resolving any discrepancies. The approved version was then translated back into English by another two bilingual translators who had no knowledge of the original questionnaire. This back-translated version was then reviewed and compared with the original version by the research team, and all differences were discussed and reconciled. A pilot study was carried out to verify patients’ understanding of the Chinese version of the HBTS questionnaire. Each participant was asked to express his/her opinions regarding the clarity of the scale and to provide further suggestions. This pilot study included 30 hypertension patients hospitalized in the department of neurology of the Xi’an Fourth Hospital, China. All patients completed the questionnaire on their own, and reported no difficulties in understanding or responding to any of the items. The pretested version of the HBTS was used as the final version for psychometric testing in Chinese hypertensive patients.
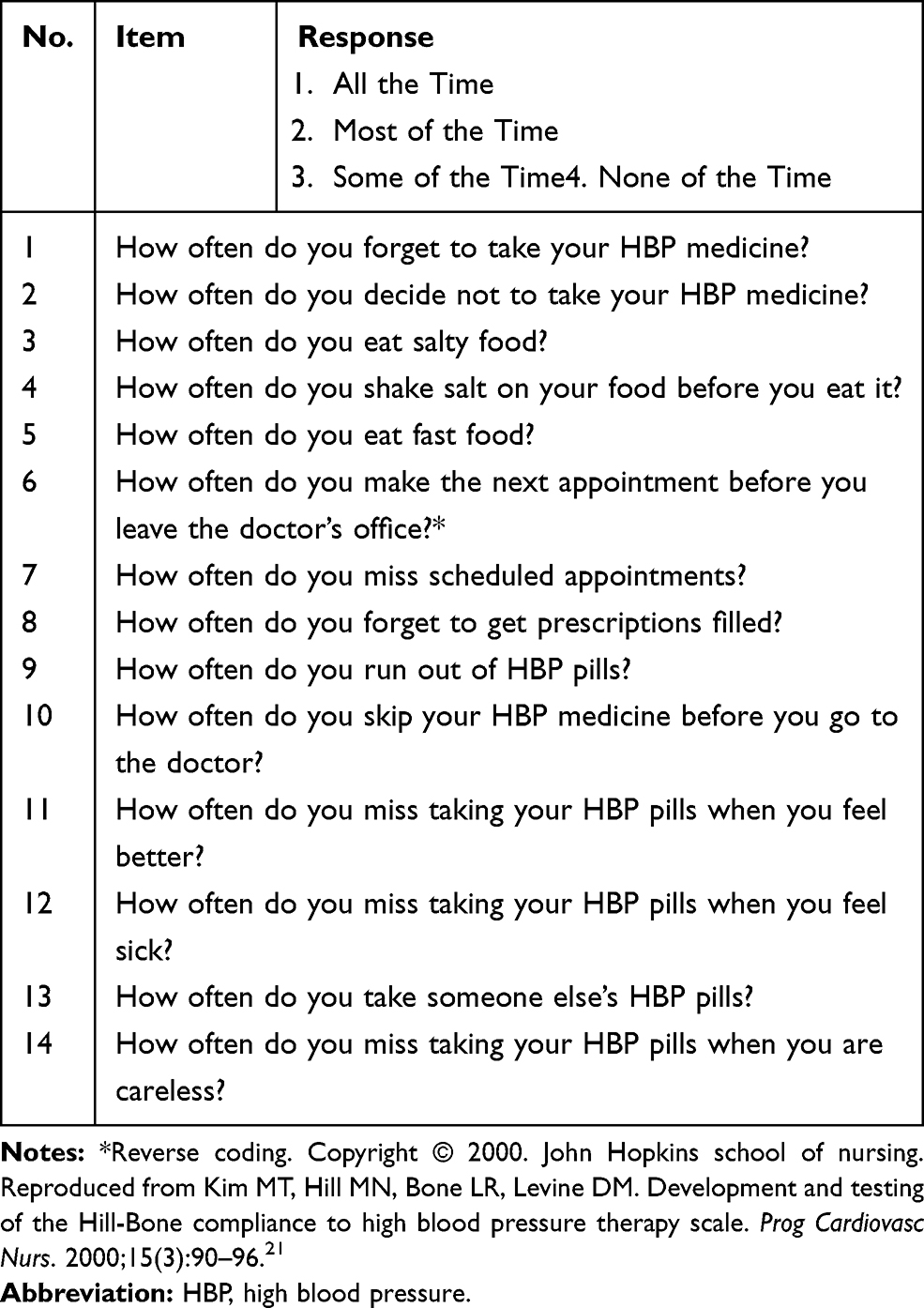 |
Table 1 The Original English Version of the Hill–Bone Compliance to High Blood Pressure Therapy Scale |
Study Sample and Data Collection
To assess its reliability and validity, the final version of the HBTS-C was used in a survey in Xi’an Fourth Hospital, China between Jan and June 2019. The verbal informed consent was approved by the ethics committee of Xi’an Fourth Hospital, and also that this study was conducted in accordance with the Declaration of Helsinki. All patients who participated in the study gave verbal informed consent.
Sample size of the study was calculated on the basis of item-to-subject ratio. Based on evidence from previous research, a subject-item ratio of 15 was used to calculate the sample size.28 Since the Hill–Bone scale contains 14 questions, a minimum sample size of 210 patients was required. Finally, 234 hypertensive patients satisfying the inclusion/exclusion criteria were recruited. Trained clinical pharmacists qualified the patients according to the inclusion/exclusion criteria.
The inclusion criteria were as follows: 1) aged at least 18 years and who agreed to attend the study; 2) diagnosis of primary hypertension; 3) undergoing anti-hypertensive drug therapy. Exclusion criteria were: 1) patients with severe complications of hypertension (eg stroke and severe heart failure); 2) cannot communicate due to physical or mental problems; 3) unable to read or understand Chinese language; 4) pregnant women. 234 patients were randomly selected from the database of the hospital. These patients were hospitalized in the department of neurology and cardiology during the period from Jan to June, 2019.
The patient data regarding socio-demographic factors were collected by reviewing the electronic medical records of every patient. Clinical data, including duration of HBP, duration of anti-hypertensive drugs used, etc., were collected face to face by trained clinical pharmacists. HBTS-C was given to the recruited patients for self-completion. For illiterate patients, the questions were read by clinical pharmacists to facilitate survey completion.
Statistical Analysis
Socio-demographic data and clinical characteristics of HBP patients in the study were analyzed using descriptive statistics. To assess the internal consistency, Cronbach’s alpha was utilized. Cronbach’s alpha is a statistic for investigating the internal consistency or reliability of a questionnaire. Alpha was developed by Cronbach and was originally used to measure the reliability of a psychometric instrument.29,30 Cronbach’s alpha ranges from 0 to 1.0 and a value of >0.7 was considered as acceptable.31 Item-total correlation (ITC) was also examined. ITC with a value of >0.3 was considered acceptable. EFA using principal component extraction was used to confirm the construct validity. Both the Kaiser-Meyer-Olkin (KMO) test and the Bartlett’s test of sphericity were estimated to confirm the appropriateness of performing EFA. Factors were extracted based on eigenvalues greater than 1. Items with loading >0.40 within one factor were retained. All statistical analyses were performed using SPSS version 19 (IBM Corp., Armonk, NY, USA). P<0.05 was considered to be statistically significant.
Results
The socio-demographic and clinical characteristics of the 234 patients are summarized in Table 2. In the group of 234 patients, 47.01% were female and most of them (91.88%) were middle and old age with an age above 50 years. 27 (11.54%) patients were illiterate and 48 (20.51%) patients had a college or university degree. Most of them (64.10%) were retired. 198 (84.62%) patients were urban people, of whom 197 patients had urban medical insurance, while 36 (15.38%) patients were rural people and only 20 patients had rural medical insurance. Most of them (61.97%) were diagnosed with stage III HBP. Most of the patients (60.69%) had suffered HBP for more than 10 years. 82 (35.04%) patients took anti-hypertensive drugs for less than 5 years, 120 (51.28%) patients took antihypertensive drugs for more than 10 years. 21 patients (8.97%) took more than 3 anti-HBP medicines every day. 87 (37.18%) patients had no other chronic diseases and 30 (12.82%) patients had more than 2 other chronic diseases.
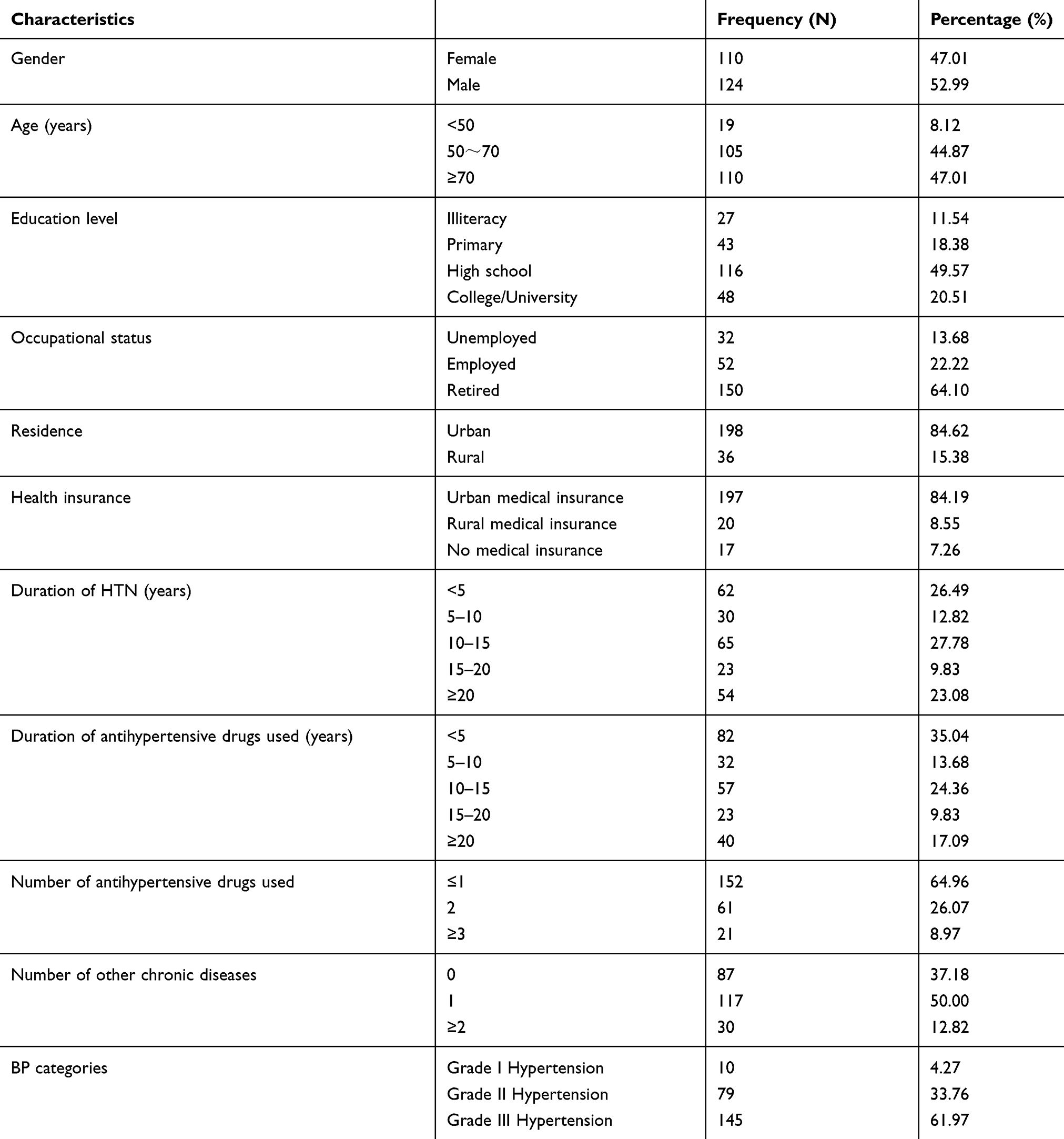 |
Table 2 Socio-Demographic Characteristics and Clinical Characteristics of Hypertension Patients (n=234) |
In the adherence assessment (n=234), the mean score was 41.91±9.27 (14–56) points. All the items except item 5 and item 6 had the highest proportion of respondents who answered never. The reverse coded item 6 “How often do you make the next appointment before you leave the doctor’s office?” had the highest proportion of respondents who answered all the time (35.47%). Item 5 “How often do you eat fast food?” had the highest proportion of respondents who answered sometimes (49.15%). Descriptive statistics from the HBTS-C questionnaire in the studied group are shown in Table 3.
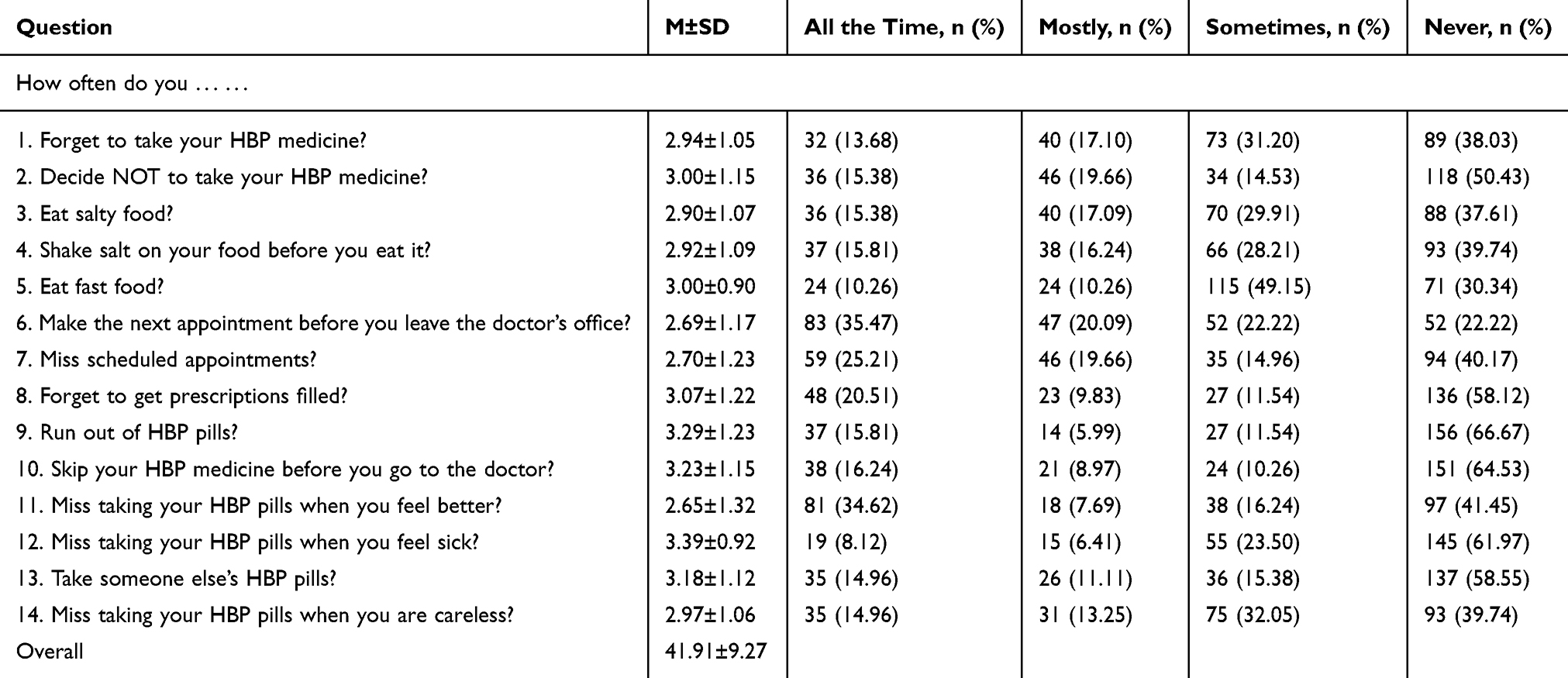 |
Table 3 Scores and Distribution of Answers to the Chinese Version of HBTS |
Internal consistency was tested using Cronbach’s alpha, and the item-total correlation coefficient was determined. The Cronbach’s alpha score for the whole questionnaire was 0.857. The item-total-correlation coefficients ranged from 0.332 to 0.822 (mean, 0.595) with all items satisfying the criterion of >0.30. Reliability analysis results are displayed in Table 4.
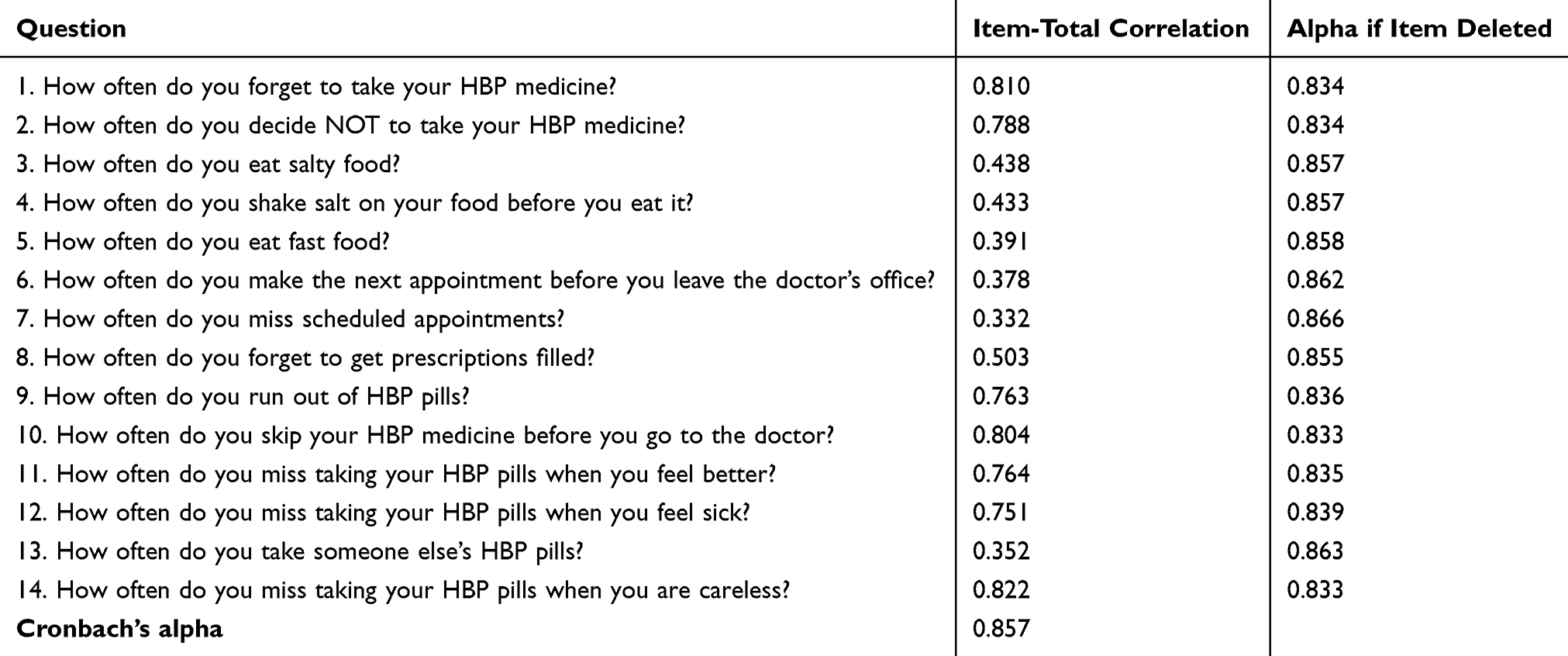 |
Table 4 Reliability Analysis of the Chinese Version of HBTS |
The Kaiser-Meyer-Olkin statistic was 0.825, and Bartlett’s test of sphericity was significant (p < 0.01) with a value of 2259.08 denoting adequate sample size for EFA. Factors were extracted based on Eigenvalues >1.0. The EFA revealed a four-component structure (factor 1 and factor 3: medication taking; factor 2: reducing sodium intake; factor 3: appointment keeping) with eigenvalue (% variance explained) of 5.258 (37.554%), 2.130 (52.769%), 1.746 (65.238%) and 1.223 (73.97%). All questions had factor loadings >0.4. The first seven items were loaded on factor 1, the next three on factor 2, the next two on factor 3, the last two on factor 4 (Table 5).
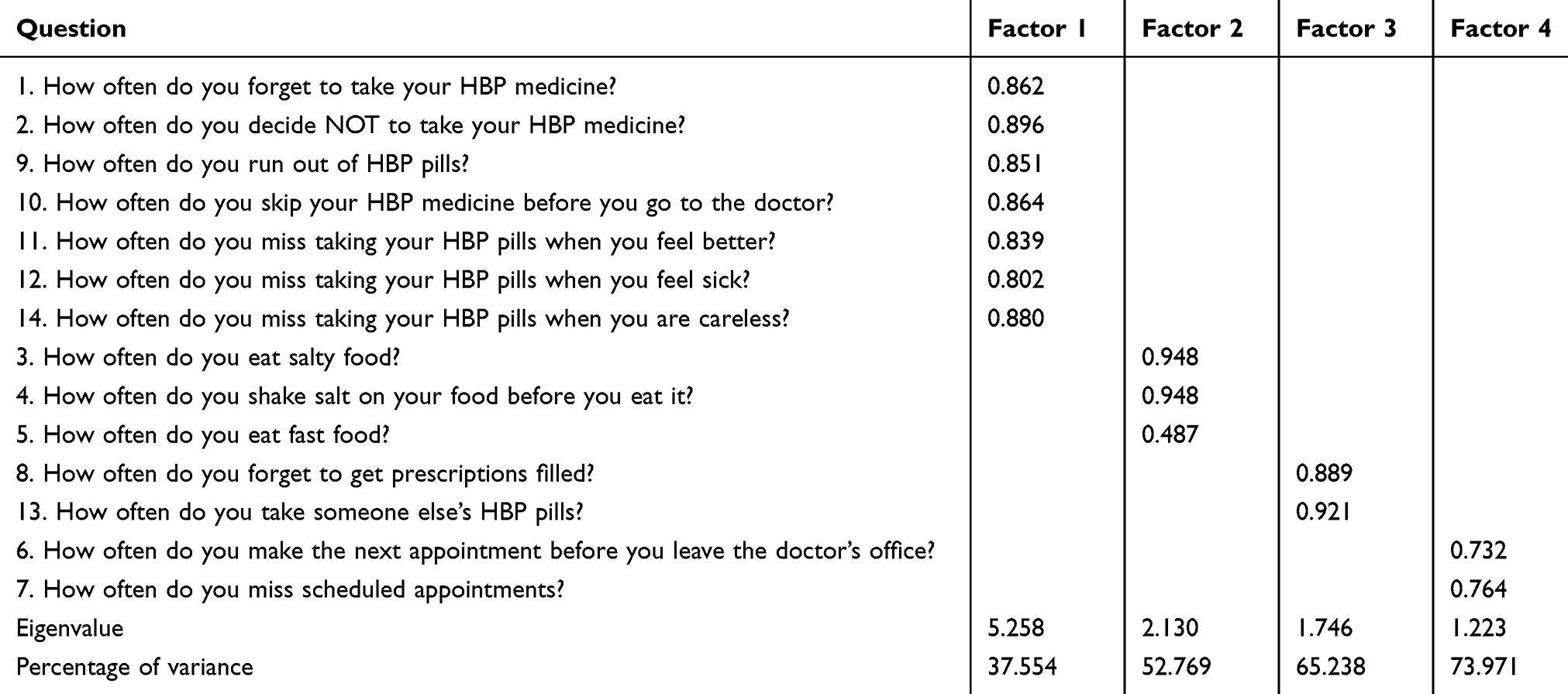 |
Table 5 Factor Loadings for Each Question in the Questionnaire |
Discussion
Poor adherence is a major problem in hypertension care. Questionnaires are the most accessible tools to assess adherence in daily clinical practice. There are several Chinese versions of questionnaires used to assess the adherence of hypertension patients, however, to our knowledge, no Chinese translations and psychometric assessment of the HBTS have been described in the literature. The purpose of this study was to prepare a Chinese adaptation of HBTS and to assess the construct validity and reliability for future use for hypertension patients in China.
The psychometric assessment in the study supports the validity and reliability of a 14-item HBTS-C scale. The HBTS-C scale demonstrated adequate internal consistency, with a Cronbach’s alpha of 0.857, which is slightly higher compared to other language versions such as Polish (0.851),24 Turkish (0.72)25 and Korean Americans (0.80).26 EFA was used to explore the structure of a construct and revealed there were four factors that may explain the interrelations among a set of items.
The 14-item HBTS-C showed reasonable internal consistency and construct validity for use to assess hypertensive treatment adherence in China. However, the Hill–Bone scale was unable to produce satisfactory results in some populations. For example, the Germany version32 and Malay version33 of the Hill–Bone scale has shown an insufficient psychometric quality in the aspects of reliability and validity. The psychometric assessment in this study supported the validity and reliability of a 14-item HBTS-C. It is similar to the study conducted in the population of Poland, which also supported the validity and reliability of the scale with all items included. However, in the adaptation by Krauser-Wood et al it was found that the scale had sufficient internal consistency and construct validity only for the 9-item medication-taking subscale.34 The Turkish HBTS with 12 items regarding medication and salt intake, especially the 9 medication compliance questions, presented a consistent structure with the original HBTS.25 The psychometric assessment in the study conducted in the Korean population supported the validity and reliability of the one factor model with an 8-item HBTS subscale.26 Thus, psychometric properties of HBTS are different from population to population.
The original HBTS has three components including medication adherence, salt intake and appointment keeping, whereas, our study showed four components, that is two components for medication adherence, one component for salt intake and one component for appointment keeping. Although the two components of medication adherence were identified through factor analysis in the study, a meaningful concept could not be rationalized. The Turkish version of HBTS also has two components for medical adherence, which found that the two factors related to the medication adherence scale were unintentional medication non-adherence and intentional medication non-adherence. However, in our study the theoretical concepts underlying each concept of the two components could not be identified, which is similar to the result reported in the Malay version of HBTS.33 In the study, very few patients had the situation mentioned in item 8 and item 13, therefore, the two items are poorly differentiated among The Chinese population. It was implied that the existence of item 8 and item 13 in this scale was of little significance. It may be the reason why the two items are independent from the medication adherence component and form another component. However, in order to maintain the integrity of the scale, this component has not been deleted. Further studies need to be conducted to find the deeper reasons.
This study has some limitations. First, questionnaires are a self assessment method and may not accurately assess the actual level of adherence. Therefore, it is worth conducting a comparative analysis and comparing the obtained results with the values and clinical parameters of disease control. Second, most of the study samples are the local residents, who live in the north of China, so cultural and region bias could have existed. Cultural and economic factors are crucial factors which could explain different levels of adherence in different countries even in different regions of a country.35 The imbalanced economic and cultural development in the southern and northern regions of China leads to differences in compliance of hypertension. While the analysis demonstrates the reliability and validity of this instrument in adults in the north of China, the ultimate usefulness in all the Chinese population groups will need to be determined through further investment. Third, the HBTS-C scale does not provide a cutoff point as compared to some other hypertension questionnaires such as the Morisky scale and TASHP scale.36 The cutoff point for a scale may help to predict clinical outcomes. Fourth, although the HBTS-C scale includes items related to lifestyle modifications, it only focuses on the salt intake. Several evidence-based recommendations for the control of HBP, including reducing weight, engaging in physical activities, and moderating alcohol intake, were not included. Further studies are needed to develop a scale that can contain the multidimensional behaviors related to BP control. Fifth, we did not carry out a re-test analysis, which would certainly improve the quality of the work. Finally, the sample size was small, larger scale studies should be carried out in the future.
Conclusions
Considering the good construct validity and internal consistency of the HBTS-C Scale, we expect that the HBTS-C Scale can be used to evaluate the treatment adherence of patients with hypertension in clinical fields in China.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Barrera L. High blood pressure prevention and control: from evidence to action. Colomb Med. 2018;49(2):137–138.
2. Patel P, Ordunez P, DiPette D, et al. Improved blood pressure control to reduce cardiovascular disease morbidity and mortality: the standardized hypertension treatment and prevention project. J Clin Hypertens (Greenwich). 2016;18(12):1284–1294. doi:10.1111/jch.12861
3. Grassi G, Quarti F, Mancia G. Hypertension, antihypertensive treatment and stroke prevention. Neurol Sci. 2005;26(Suppl 1):S22–S23.
4. Aronow WS. Hypertension-related stroke prevention in the elderly. Curr Hypertens Rep. 2013;15(6):582–589. doi:10.1007/s11906-013-0384-x
5. Hamrahian SM, Falkner B. Hypertension in chronic kidney disease. Adv Exp Med Biol. 2017;956:307–325.
6. Pugh D, Gallacher PJ, Dhaun N. Management of hypertension in chronic kidney disease. Drugs. 2019;79(4):365–379. doi:10.1007/s40265-019-1064-1
7. Gavrilova A, Bandere D, Rutkovska I, et al. Knowledge about disease, medication therapy, and related medication adherence levels among patients with hypertension. Medicina (Kaunas, Lithuania). 2019;55(11).
8. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
9. Zhou Y, Jia L, Lu B, et al. Updated hypertension prevalence, awareness, and control rates based on the 2017ACC/AHA high blood pressure guideline. J Clin Hyperten. 2019;21(6):758–765.
10. Yang Q, Chang A, Ritchey MD, Loustalot F. Antihypertensive medication adherence and risk of cardiovascular disease among older adults: a population-based cohort study. J Am Heart Assoc. 2017;6(6). doi:10.1161/JAHA.117.006056
11. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
12. Shehab A, Elnour AA, Swaidi SA, et al. Evaluation and implementation of behavioral and educational tools that improves the patients’ intentional and unintentional non-adherence to cardiovascular medications in family medicine clinics. Saudi Pharm J. 2016;24(2):182–188. doi:10.1016/j.jsps.2015.02.022
13. Akhu-Zaheya LM, Shiyab WY. The effect of short message system (SMS) reminder on adherence to a healthy diet, medication, and cessation of smoking among adult patients with cardiovascular diseases. Int J Med Inform. 2017;98:65–75. doi:10.1016/j.ijmedinf.2016.12.003
14. Christensen A, Osterberg LG, Hansen EH. Electronic monitoring of patient adherence to oral antihypertensive medical treatment: a systematic review. J Hypertens. 2009;27(8):1540–1551. doi:10.1097/HJH.0b013e32832d50ef
15. Hou MY, Hurwitz S, Kavanagh E, Fortin J, Goldberg AB. Using daily text-message reminders to improve adherence with oral contraceptives: a randomized controlled trial. Obstet Gynecol. 2010;116(3):633–640. doi:10.1097/AOG.0b013e3181eb6b0f
16. Piette JD, Datwani H, Gaudioso S, et al. Hypertension management using mobile technology and home blood pressure monitoring: results of a randomized trial in two low/middle-income countries. Telemed e-Health. 2012;18(8):613–620. doi:10.1089/tmj.2011.0271
17. Mudhune V, Gvetadze R, Girde S, et al. Correlation of adherence by pill count, self-report, MEMS and plasma drug levels to treatment response among women receiving ARV therapy for PMTCT in Kenya. AIDS Behav. 2018;22(3):918–928. doi:10.1007/s10461-017-1724-7
18. Sandbaumhüter FA, Haschke M, Vogt B, Bohlender JM. Indexed plasma drug concentrations for drug adherence screening in hypertensive patients. Ann Cardiol Angeiol. 2018;67(3):119–126. doi:10.1016/j.ancard.2018.04.020
19. He W, Bonner A, Anderson D. Patient reported adherence to hypertension treatment: A revalidation study. Eur J Cardiovasc Nurs. 2016;15(2):150–156. doi:10.1177/1474515115603902
20. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hyperten. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
21. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone compliance to high blood pressure therapy scale. Prog Cardiovasc Nurs. 2000;15(3):90–96. doi:10.1111/j.1751-7117.2000.tb00211.x
22. Lomper K, Chabowski M, Chudiak A, Białoszewski A, Dudek K, Jankowska-Polańska B. Psychometric evaluation of the polish version of the adherence to refills and medications scale (ARMS) in adults with hypertension. Patient Prefer Adherence. 2018;12:2661–2670. doi:10.2147/PPA.S185305
23. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
24. Uchmanowicz I, Jankowska-Polańska B, Chudiak A, Szymańska-Chabowska A, Mazur G. Psychometric evaluation of the polish adaptation of the Hill-Bone compliance to high blood pressure therapy scale. BMC Cardiovasc Disord. 2016;16:87. doi:10.1186/s12872-016-0270-y
25. Karademir M, Koseoglu IH, Vatansever K, Van Den Akker M. Validity and reliability of the Turkish version of the Hill-Bone compliance to high blood pressure therapy scale for use in primary health care settings. Eur J Gen Pract. 2009;15(4):207–211. doi:10.3109/13814780903452150
26. Song Y, Han HR, Song HJ, Nam S, Nguyen T, Kim MT. Psychometric evaluation of hill-bone medication adherence subscale. Asian Nurs Res (Korean Soc Nurs Sci). 2011;5(3):183–188. doi:10.1016/j.anr.2011.09.007
27. Efstathiou G. Translation, adaptation and validation process of research instruments. Individualized Care. 2019;2019:65–78.
28. Anthoine E, Moret L, Regnault A, Sébille V, Hardouin JB. Sample size used to validate a scale: a review of publications on newly-developed patient reported outcomes measures. Health Qual Life Outcomes. 2014;12:176. doi:10.1186/s12955-014-0176-2
29. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):297–334. doi:10.1007/BF02310555
30. Bujang MA, Omar ED, Baharum NA. A review on sample size determination for cronbach’s alpha test: a simple guide for researchers. Malays J Med Sci. 2018;25(6):85–99. doi:10.21315/mjms2018.25.6.9
31. Streiner D, Norman G,Cairney J. Health Measurement Scales: A practical Guide to Their Development and use. 5th ed. Oxford University Press; 2015. Available from: https://oxfordmedicine.com/view/10.1093/med/9780199685219.001.0001/med-978019968521. Accessed September 29, 2020.
32. Koschack J, Marx G, Schnakenberg J, Kochen MM, Himmel W. Comparison of two self-rating instruments for medication adherence assessment in hypertension revealed insufficient psychometric properties. J Clin Epidemiol. 2010;63(3):299–306. doi:10.1016/j.jclinepi.2009.06.011
33. Cheong AT, Tong SF, Sazlina SG. Validity and reliability of the Malay version of the Hill-Bone compliance to high blood pressure therapy scale for use in primary healthcare settings in Malaysia: a cross-sectional study. Malays Fam Physician. 2015;10(2):36–44.
34. Krousel-Wood M, Muntner P, Jannu A, Desalvo K, Re RN. Reliability of a medication adherence measure in an outpatient setting. Am J Med Sci. 2005;330(3):128–133. doi:10.1097/00000441-200509000-00006
35. Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky Medication Adherence Scale. PLoS One. 2013;8(4):e62775. doi:10.1371/journal.pone.0062775
36. Pan J, Wu L, Wang H, et al. Determinants of hypertension treatment adherence among a Chinese population using the therapeutic adherence scale for hypertensive patients. Medicine. 2019;98(27):e16116.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.