")
Back to Journals » Journal of Pain Research » Volume 14
The Transformation of the Balloon Shape in Percutaneous Balloon Compression for Trigeminal Neuralgia
Authors Sun C, Zheng W , Zhu Q, Du Q , Yu W
Received 21 October 2021
Accepted for publication 6 December 2021
Published 14 December 2021 Volume 2021:14 Pages 3805—3814
DOI https://doi.org/10.2147/JPR.S343783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Chenglong Sun,1 Wenhao Zheng,2 Qiang Zhu,1 Quan Du,1 Wenhua Yu1,3
1Department of Neurosurgery, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2The Fourth Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Neurosurgery, Hangzhou Ninth People’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Wenhua Yu
Department of Neurosurgery, Affiliated Hangzhou First People’s Hospital, Zhejiang University School of Medicine, No. 261, Huansha Road, Hangzhou, People’s Republic of China
Email [email protected]
Background: The pear shape of an inflated balloon is thought to be a gold standard of successful percutaneous balloon compression (PBC). However, neither how nor why it changes in that way (the anatomic basis) has not yet been fully described.
Aim: In this article, we try to describe how the balloon in Meckel’s cave (MC) should appear and why; and identify which shapes are good pear shapes, which shapes are not good pear shapes, and which shapes are intermediate.
Methods: Radiographs from over 150 percutaneous balloon compression (PBC) cases were thoroughly evaluated. We proposed a model of changing balloon shape in MC and 70 cases were followed up over two years, in which therapeutic effect was measured.
Results: We found that the balloon changed stereotypically in MC. The model that we proposed is consistent with the description of MC’s structures and its’ surroundings in the literature. The distinct pear (pear in MC) brought about a far better surgical result than other shapes (p < 0.01).
Conclusion: Our study showed how and why the balloon shape changed during PBC surgery. The model provides clear guidance for PBC surgery.
Keywords: percutaneous balloon compression, balloon shape transformation, trigeminal neuralgia, Meckel’s cave
Introduction
In 1983, a novel percutaneous technique for trigeminal ganglion compression (percutaneous balloon compression, PBC) was described.1 The percutaneous approach through the foramen ovale had been well developed long before this time (eg, Harris in 1910 and Härtel’s work published in German in 1914). The idea of balloon “compression” was thought to be a percutaneous modification of Taarnhoj and Shelden’s “decompression” craniotomy operation. Shelden first proposed compression, and he pointed out that it was not decompression but the compression that alleviated the pain.2,3 Mullan’s great invention ingeniously combined those two aspects using a No. 4 Fogarty balloon catheter as a percutaneous compression carrier. Since then, this approach has survived the test of time and is still popular worldwide.
After Mullan’s proposal of the PBC technique, Urculo et al studied the balloon’s macroscopic changes on cadavers, providing solid evidence that a good balloon shape is an ideal pear shape in Meckel’s cave (MC).4 Although there are studies about the balloon’s shape in PBC surgery, there is no thorough investigation about how and why the balloon shape changes during PBC.5–7 During PBC, inflated balloons may form many shapes other than a typical pear shape. In this article, we try to describe how the balloon in the MC should appear and why; and identify which shapes are good pear shapes, which shapes are not good pear shapes, and which shapes are intermediate.
Methods
Preparation and Equipment
Patients with supine positions were subject to light general anesthesia. Patients’ heads and trunks were in an anatomical position and with no head rotation or flexion. The endotracheal tube was used to carry out anesthesia.
Patients’ vital signs should be closely monitored, especially during puncture and compression. In case of bradycardia or cardiac arrest, 0.5 mg atropine was prepared for IV push. Nicardipine or Urapidil was administered for high blood pressure induced by puncture or compression.
C-arm X-ray was used after general anesthesia to obtain patients’ lateral projection. The patients’ position and the C-arm were kept still during the whole process.
The study was approved by the Institutional Review Board of Hangzhou First People’s Hospital, China (IRB No. 2020-240-01) and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Surgical Material and Puncturing Technique
The liver-biopsy needle with a blunted head was used to perform a puncture (Figure 1A and B). Another two longer wires with different diameters were used to perform further cannulation. We preferred modified Härtel’s pathway similar to that described by De Cordoba et al (proposed by Henderson).8,9
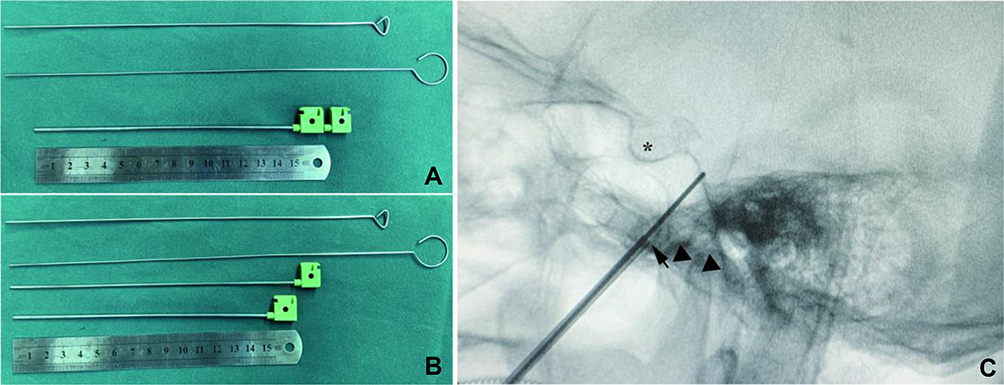 |
Figure 1 Puncture kits and a lateral projection of a PBC surgery. (A) PBC Puncture kits. From bottom to top: ruler (as scale), a head-blunted liver-biopsy needle with stylet in, a thinner needle with blunted head, a needle of larger diameter. (B) PBC Puncture kits with the stylet out. (C) Lateral projection cannulation: The puncture needle (cannula) tip is at the foramen ovale (arrow) but does not penetrate. The thinner needle tip comes across the clivus on the projection; the puncture sets are between the mandibular condyles (black triangle) and hypophysial fossa (*). |
On lateral projection, the puncture needle appears between the mandibular condyle and hypophysial fossa. When the blunt-head needle with stylet impacts the cranial bone, the foramen ovale is identified as a soft spot in the bone. After stylet withdrawal, a thinner wire and then a larger wire is employed to perform the cannulation (as shown in Figure 1C). A popping sensation can be felt with the wire during cannulation. When the tip of the puncture needle is positioned at the foramen ovale, we are careful not to penetrate the structure (Figure 1C).
Balloon Volume and Compression Time
According to intraoperative pressure and the balloon’s shape, a balloon volume of 0.35 to 0.5 mL, with a mean value of 0.4 mL, and compression time of 3.5 to 5 min, with a mean time of 4 min, were sufficient to achieve an excellent functional outcome. Before ensuring that the balloon was in the proper position (MC), we used a 0.15 to 0.2 mL balloon volume projection to find the proper position. Reinforced compression was performed for 1 to 2 mins for the 1st or the 3rd branch pain (see below). Radiographs were taken to record every balloon inflation. We deflated the balloon before balloon adjustment.
Image Processing
The radiographs of over 150 cases were reviewed. The figures were processed or drawn by Photoshop and Adobe Illustrator.
Patient Selection and Follow-Up
Indications for PBC surgery were insufficient pain relief or unacceptable side effects from medication. Older people over 70 years old accounted for most of the cases. Most of them had previous failed surgeries or could not endure microvascular decompression (MVD) surgery. After PBC surgery, follow-up was accomplished through telephone interviews. Pain relief was defined as no trigeminal pain in patients who were not on medication.
Result
Transformation of the Balloon Shape
During adjustment of balloon positions, we found the balloon changing in a stereotypical way. Before entering MC, the inflated balloon initially had a cucumber-like shape in the lateral projection (Figure 2A1). In practice, after the balloon inflated into a pear shape, the cucumber shape would appear by deflating, pulling backward, and reinflating the catheter. Afterward, when the catheter was pushed forward, it would undergo a series of consecutive shape transformations: almost round (Figure 2A2 and B1), pear (Figure 2A3, B2, C1), dumbbell (Figure 2B3, C2), mirror pear (Figure 2A4, B4), down head balloon (Figure 2C3), and balloon (Figure 2C4). There was no smooth transition between “cucumber” and “almost round”. The punctured entry point in MC could be different among cases, but the balloon could only change in a fixed pattern after it entered into MC (Figure 3b2–b4). The descriptive words (such as “cucumber”, etc.) are from here on used as the exclusive identifiers of shapes in this manuscript.
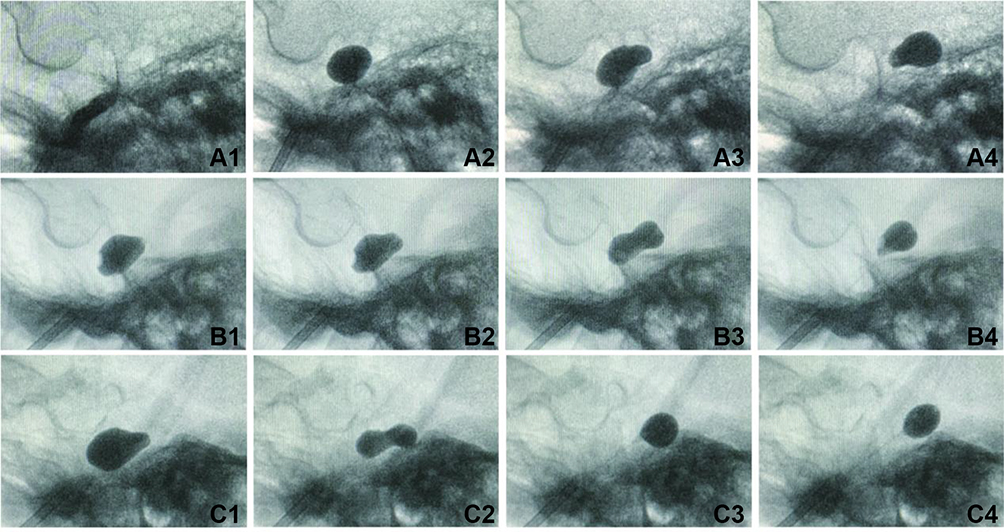 |
Figure 2 Transformation of the balloon shape in MC. For each row (A–C), the figures are from the same patients. As when pushing the balloon catheter forward, the balloon shape changed stereotypically: cucumber (A1), almost round (A2, B1), pear (A3, B2, C1), dumbbell (or hourglass, B3, C2), mirror pear (A4, B4), down-head balloon (C3), balloon (C4). (Note that the balloon may not change in that order in the actual procedure.). |
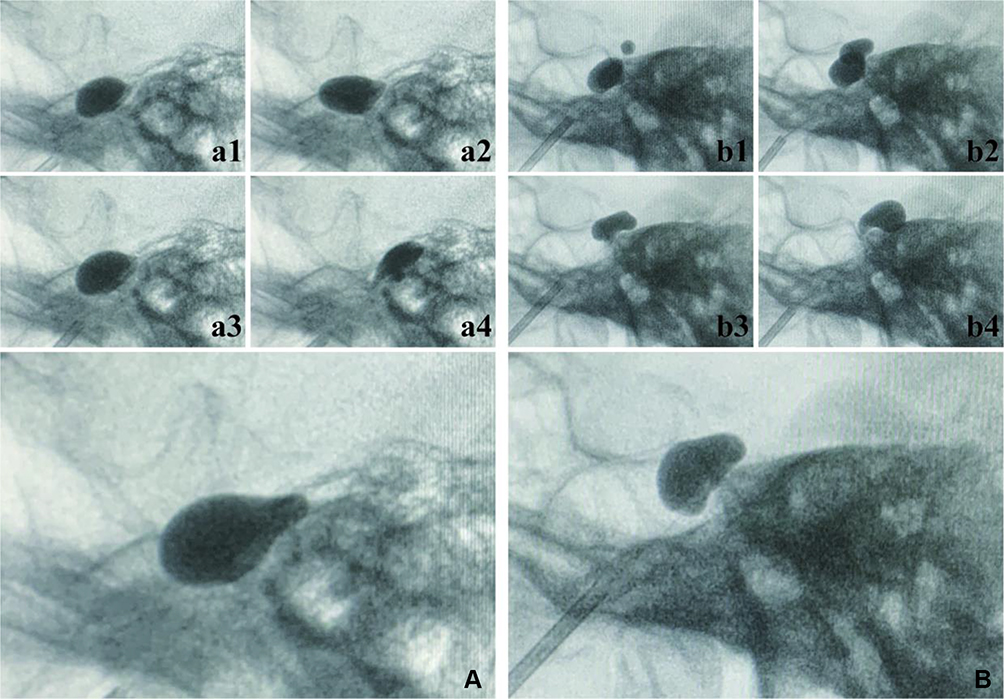 |
Figure 3 An incorrectly placed balloon resulted in unsatisfactory pear shapes. Set A (a) was from one PBC patient. a1 to a4 are not correct pears (although a3 looks pretty likely to be right, it camouflaged with a distorted end), A is the correct pear shape of the patient. Set B (b) is another patient. b1 is not correct. The upper part of the balloon of b2 is in the correct space, so the following b3 (dumbbell) and b4 (mirror pear) change in a correct mode (because the entry point was in the middle of the MC (b2), one could not get a correct pear shape by adjusting the catheter). B is the correct pear of the case. |
Selective Numbness
Different balloon shapes may act on different parts of the trigeminal ganglion. It was found occasionally that a more dumbbell-shaped balloon (nearer to the outlet of the MC, Figure 4a1) and a more cucumber-shaped balloon (near the entrance of the MC, Figure 4b2) could numb the first (ophthalmic division) or the third (mandibular division) branch (Figure 4) respectively. There was a numbest point after the surgery, usually not the most painful point (Figure 4A and B).
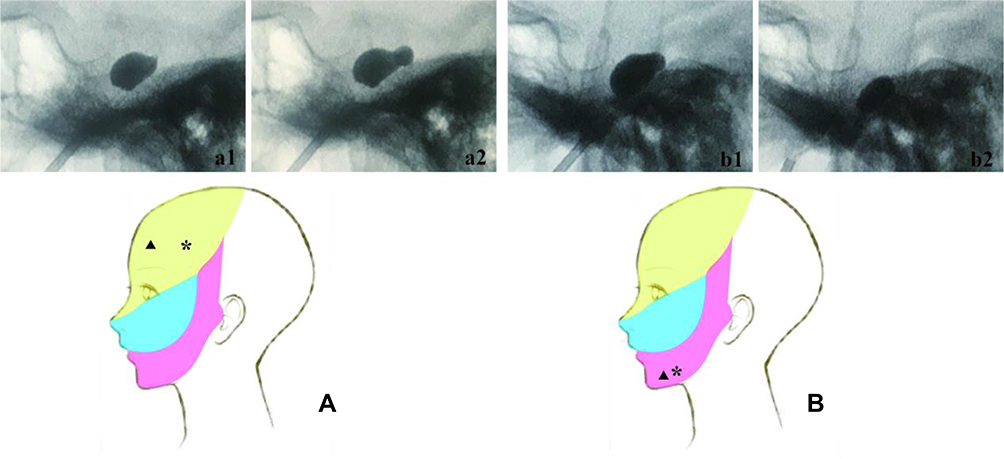 |
Figure 4 Selective numbness. After we performed the routine pear shape (a1, b1) compression (3–4 min): (A) For the first branch pain (marked with ▲), the more dumbbell-shaped balloon (a2) reinforced compression (1–2 min) could give the selective effect of the first branch numbness (marked with *). (B) The cucumber-shaped balloon (b2) reinforced compression (1–2 min) could contribute to selective numbness of the third branch (*). The pain region (▲) and the numbness region (*) did not overlap. |
A Continuous Space: From MC to Porus Trigeminus
When the balloon is in MC, if the balloon volume is large enough, the balloon would assume the shape of an enlarged MC and its outlet, the porus trigeminus (Figure 5e or A). As the volume or the position of the balloon changed within the range (Figure 5a–i), the overlap of the two ends (Figure 5B) or the whole series (Figure 5C) would appear like the largest one (Figure 5e or A).
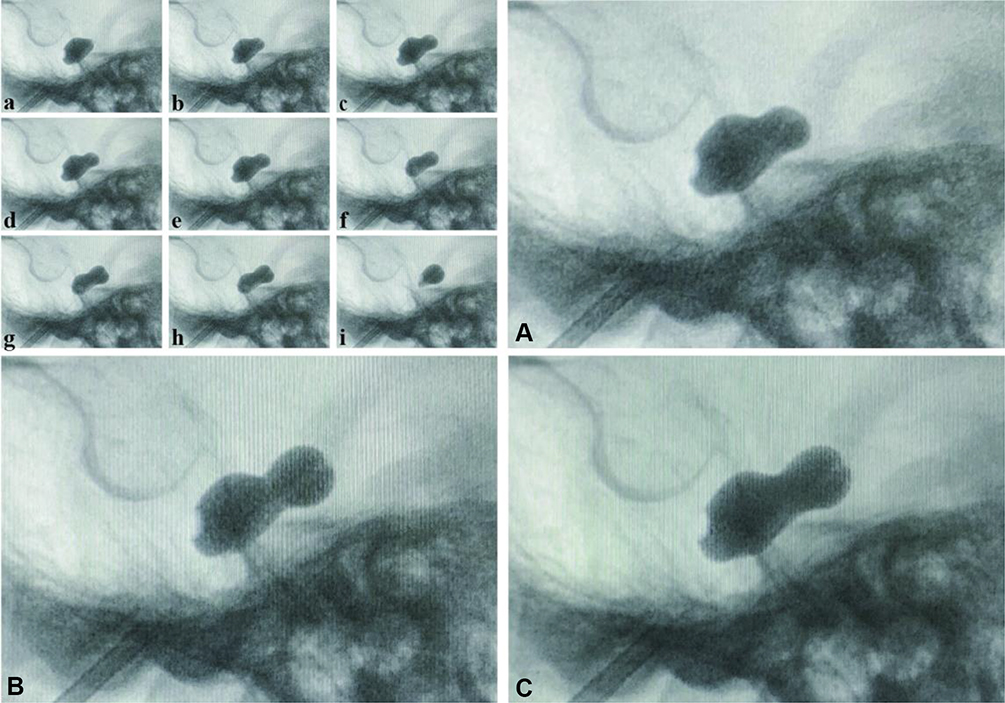 |
Figure 5 MC and its outlet is a continuous space. a to i are a consecutive series of pictures during a PBC surgery (From the same patient of Figure 2B). (A) is an enlargement of e; (B) is an overlap of a and i; (C) is an overlap of a to i. Note that (A–C) are almost the same. |
The Space Holding the Third Branch Was Inconsecutive with MC
In most cases, standard cucumber shapes were failed to achieve. Typically, if the balloon became almost round, the catheter would be pulled backward slightly, and it would slip out of the foramen ovale. Fortunately, in the three cases presented, uncommon radiographs were observed. The balloon was pulled back slightly and inflated after standard pear shapes were achieved (Figure 6A1, B1, and C1). It seemed that something prevented the balloon from entering the rear space (Figure 6B2, C2) or separated the space from MC (Figure 6A2).
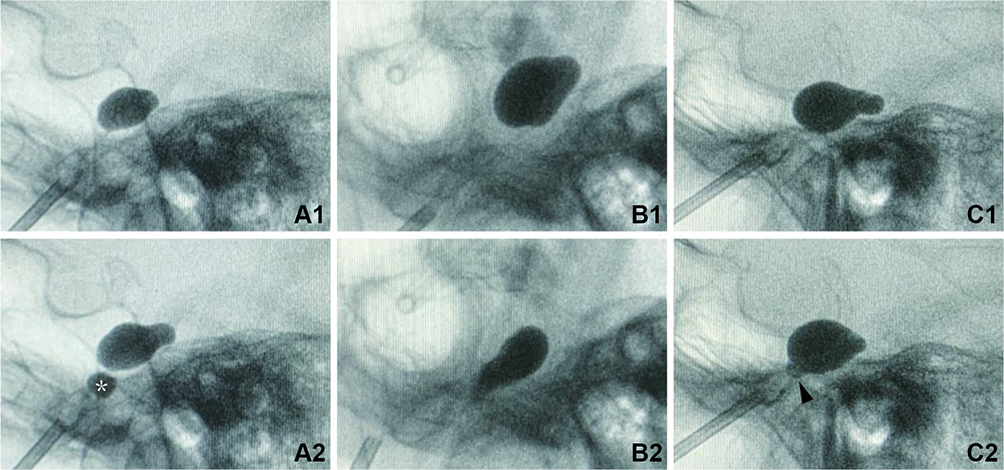 |
Figure 6 The space that is accommodating the third branch is not contiguous with MC. The sets (A–C) are from three patients. A1, B1 and C1 are standard pear shapes. For the third branch reinforced compression: When inflated, A2 had a disconnected tail (*). When pulled back and reinflated, B2 had a sharp triangle tail; C2 only got a tiny butt (arrowhead). |
There Should Be Always a Pear Shape
The abnormal pear shapes (Figure 7a1–a4) did not change in a fixed pattern, and the incorrectly placed balloon would not assume the shape of MC (Figure 7A1 and A2). In contrast, after re-puncture (which may be performed repeatedly), the good pear shapes change in a normal manner (Figure 7b1–b4) and assume the shape of MC after being inflated (Figure 7B1 and B2).
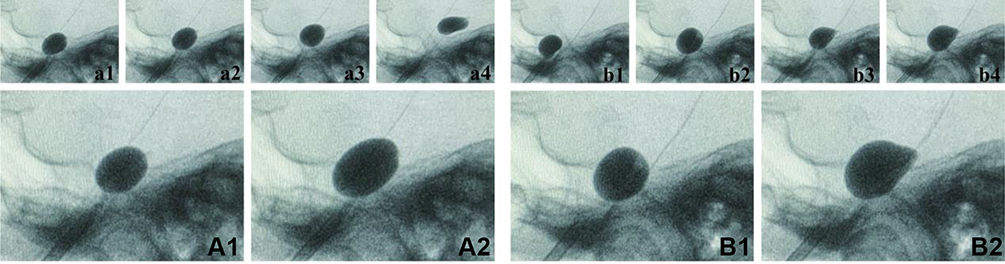 |
Figure 7 There should be always a pear shape. Both set A (a) and set B (b) are from the same patient during one PBC surgery. Set A (a). The balloon catheter was not in the correct anatomic space (MC); when push forward the catheter, the balloon did not change in a standard mode (a1 to a4). When inflated, the balloon just got larger but did not assume a correct shape (A1 to A2). In contrast, set B (b) was in the correct position, the balloon changed in a correct manner (b1 to b4) and inflated to a correct shape (B1 to B2). |
An Incorrectly Placed Balloon May Produce Different Shapes
In the case of incorrect balloon position, the catheter’s tip may be restricted and distorted by the surroundings. The inflated balloon will present numerous odd shapes (Figure 3a1–a4, b1). Some odd shapes may appear similar to ideal shapes (Figure 3a3). When the catheter enters halfway into the MC, the balloon’s shape could initially be half correct (Figure 3b2) before taking on correct shapes (Figure 3b3 and b4). Note that most cases result in good pear shapes after re-puncturing, and they may be different from each other (Figure 3A and B).
Outcome and Complications
70 out of 150 cases were successfully followed up over 24 months. Patients’ characteristics are presented in Table 1. Most of the patients (66/70) had previous operative histories (minimal invasive or craniotomy). 59 out of 70 cases got distinct pear shapes (Table 2). A distinct pear is defined as a balloon that locates in MC and will stereotypically transform as described above. The patients’ result with distinct pear was significantly better than those without (p < 0.01). No serious complication was observed. Ipsilateral facial numbness was the most common complication (37/70), and other complications are listed in Table 3.
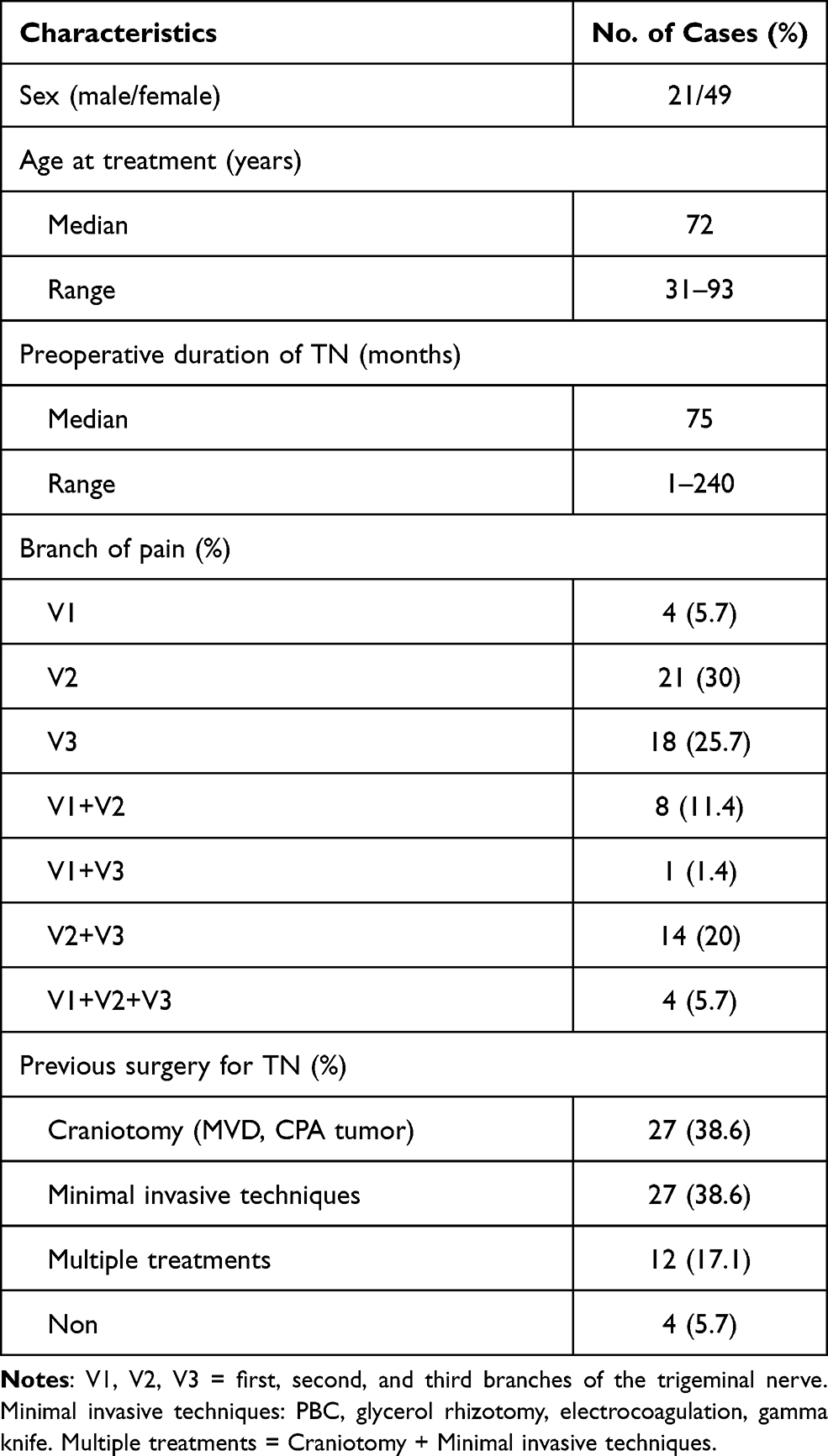 |
Table 1 Patient Characteristics of 70 Patients Undergoing PBCs |
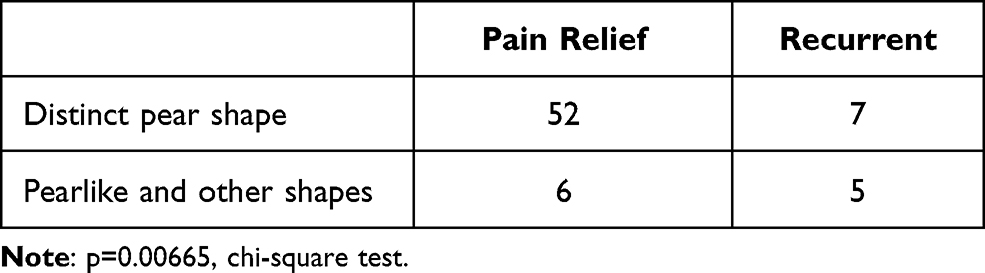 |
Table 2 Results of 70 Patients After PBC |
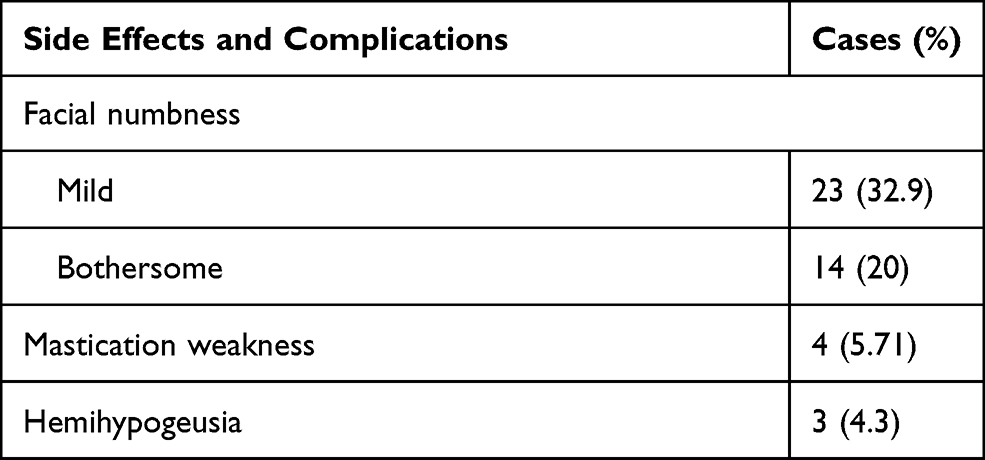 |
Table 3 Side Effects and Complications in 70 Patients After PBC |
Discussion
The radiographs were carefully selected from over 150 PBC cases. Most of the cases that resulted in the optimal pear shape were successes at the first attempt and of no reference value. The cases presented here mainly required much more adjustment. Commonly, if a non-pear-shaped balloon had not been achieved, another puncture would be immediately performed again (sometimes the puncture might be repeated several times), which has been proven to be a safe approach. That is different from that described by Mullan and may not be the policy for most physicians, who “repeated a few days later.”1,6
A lower volume of 1.5–2 mL was used to test the position of the balloon. In previous reports, most often, the volume of injected contrast was 0.7 mL. In Mullan’s original article, the volume was 0.75 mL. In our view, that is more than enough. In our cases, the average inflated volume of 0.4 mL is much lower than what was generally reported.1,6,10 Sometimes, the numbness is devastating even with a small volume. The procedure, including balloon volume combined with compression time, was acceptable over one-year of follow-up. According to the stature, balloon pressure, and other variables, the balloon volume should differ from person to person. This observation is beyond the scope of this study.
The dural structure of the trigeminal nerve delineates the contour of the MC and its potential connection. MC is formed by a continuous dura mater, which isolates its contents from the middle cranial fossa below and the temporal lobe above.11–13 The dural sheaths cover the three major divisions of the trigeminal nerves and extend far beyond the points that the divisions join the ganglion. For the mandibular branch, the dural sheath leaves the middle fossa through the foramen ovale and fuses with the epineurium extracranially (Figure 8A).11,12
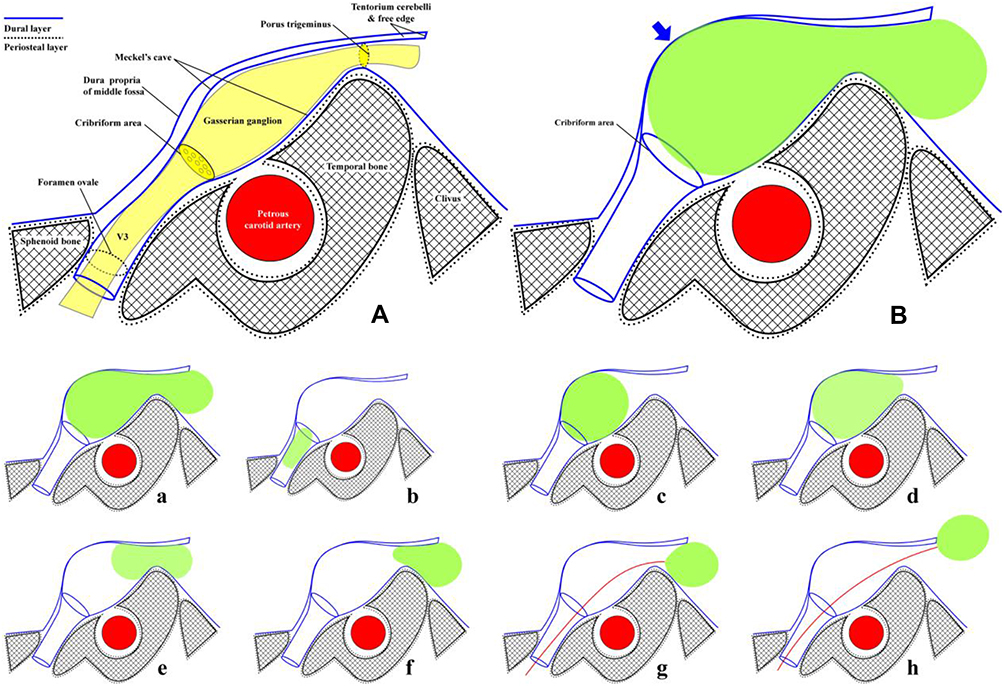 |
Figure 8 Schematic showing of MC and balloon changes (Redrawn with data from Joo et al. Based on the work of Joo et al, Li et al and Janjua et al11,12,14) (A) Oblique coronal section between the porous trigeminus and the foramen ovale. Meckel’s cave’s superior surface is formed by double layers of dura matter: meningeal dura (dura propria of middle fossa) and periosteal dura (inner layer of MC). The periosteal dura can be seen lining the bone intra- and extracranially and forms nerve branches’ sheaths. Cribriform separates MC from the peripheral nerve sheaths. (B) A balloon fully inflated in MC. (the enormous belly of the balloon, blue arrow). a: a miniature version of B. b: cucumber. c: almost round. d: pear. e: dumbbell (or hourglass). f: mirror pear. g: down head balloon (as a result of the block of tentorium cerebelli). h: balloon. Refer to Figure 2. Redline for the balloon catheter. |
For correct placement, a fully inflated balloon should include two tunnel-like ends and one large belly. One tunnel end should target the sheath of the mandibular branch, and the other should target the porus trigeminus, while the large belly should target the central part of the MC. However, all of the fully inflated balloons we have observed have never assumed that kind of shape. It seemed there was a septum between the sheath of the third branch and MC. As a result, the fully inflated balloon can only take on the shape of one large belly (MC) and one tunnel end (porus trigeminus, Figure 8B). Indeed, there is such a septum named the cribriform area by Li et al.12 The cribriform area also explains why the space accommodating the third branch is difficult to enter (Figure 6). There is no smooth transition between a cucumber and an almost round shape (Figures 8b, c and 2A1 and A2).
For partially inflated balloons, they assumed the shape of the space holding them. Therefore, there was cucumber, almost round, pear, and dumbbell (or hourglass) shapes in the cavity. Except for the cucumber, the last three shapes can smoothly change from one to another by adjusting the catheter. The mandibular branch, the ganglion, and the nerve root share space in the MC. The last two have much less effect on the balloon shape; however, the mandibular branch would interact with the balloon to deforms its shape. As a result, the cucumber shape is not such a typical shape. Furthermore, the dural structure of the third branch, whether or not the dural sheath stretches out of the foramen ovale, is still controversial.11,12,14
The forepart of the tentorium and the dural band superior to the MC’s opening (that is, the porus trigeminus) stretches out into the subarachnoid cisternal space. Suppose the balloon catheter goes beyond the porus trigeminus and partially enters the subarachnoid space. In that case, the dura will bend the head of the balloon downward.14,15 At this position, part of the balloon is still in MC, so the inflated balloon looks like a mirrored pear shape (a mirror image of the right pear, Figure 8f). If the balloon completely exits the porus trigeminus, dura’s obstruction would cause a down-head balloon (Figure 8g), followed by a balloon (Figure 8h).
Based on a thorough literature review, a model of MC’s dural architectures and its potential connection were proposed to explain the variations of the balloon shape (Figure 8). The model could explain the balloon shape’s variation and transformation in the MC. It is an informative reference for balloon adjustment. For example, if someone intends to achieve a standard pear shape, but the inflated balloon is an hourglass shape or a mirror pear shape (Figure 8e and f), the balloon must be deflated, followed by slightly removing the catheter backward, and then reinflate the balloon. If an almost round shape (Figure 8c) is achieved, the balloon should be reinflated in a forward position.
Surprisingly, we found that balloon compression towards the two ends selectively numbs the third branch (the proximal end, towards the cucumber) and the first branch (the distal end, towards the dumbbell). Because we always perform standard pear compression before cucumber shapes or dumbbell shapes as reinforcements, most patients would still complain of hemifacial numbness instead of localized numbness. The numbness was acceptable for most patients, so it is not a good option to perform selective compression alone. However, for this study, good pear compression is a necessity for a PBC. Brown, J. A. described a method specialized for different divisions of pain: on anteroposterior view and using the trigeminal impression as a reference, for first, second (or multidivisional), or third division pain, the stylet should be aimed at the trigeminal impression medially, centrally and laterally, respectively.16 This method of using different MC entry points (for different angles) to realize the selectivity was very likely to be the same as what we used different balloon shapes. Teo et al did the same as we do for lower divisional pain.17 The affecting points also coincide with the anatomical structures of the trigeminal nerve.8,18
As mentioned above, the cucumber shape was usually challenging to obtain. If a cucumber shape was failed to achieve, the catheter would be pulled backward and maintain a little tension when the balloon was almost round. This method was used as an alternative to reinforcing the compression of the pain from the third division. For pain from the first division, we would slightly push forward the catheter, and when a good pear shape was achieved, a more “hourglass” pear shape would immediately appear.
There are articles identifying correlations between different balloon shapes and the patients’ prognosis,6,10 but we believe there should be always a pear shape and only one true pear shape (because there is a MC for each trigeminal ganglion). The pears’ shapes may be subtly different from one another, but proper pear shapes change stereotypically. Parts of the dura mater around MC could be easily detached from its surroundings, so the incorrectly placed balloon would assume many peculiar shapes. However, fake pear shapes that were quite similar to standard pear shapes did not change stereotypically; in many instances, they had twisted balloon ends (Figure 3a3).
We have given a far more detailed description of the balloon shape-changing in PBC. A good outcome of PBC had long been related to a pear shape balloon, so was our study. The model we presented here was based on circumstantial evidence from fluoroscopy. There are still shapes that we were unable to classify positively. MC’s dural structure (may rupture as a result of puncture) and the petrous ridge and angulation of the trigeminal nerve could lead to the variation in the balloon shape that cannot be directly observed during PBC.19 Sometimes, the experience of the physician remains the determining factor.
Conclusions
Meckel’s cave, its inlet, and its outlet force the inflated balloon to take on various shapes. When pushing forward the catheter, the shapes are as follows: cucumber, almost round, pear, dumbbell, mirror pear, down-head balloon, and balloon. Different balloon shapes may act on different parts of the trigeminal ganglion and cause selective numbness. These findings offer a good reference for PBC surgery in clinical events.
Acknowledgments
This research was supported by Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2021KY229).
Disclosure
The authors declare no conflicts of interest.
References
1. Mullan S, Lichtor T. Percutaneous microcompression of the trigeminal ganglion for trigeminal neuralgia. J Neurosurg. 1983;59:1007–1012. doi:10.3171/jns.1983.59.6.1007
2. Shelden CH, Pudenz RH, Freshwater DB, Crue BL. Compression rather than decompression for trigeminal Neuralgia. J Neurosurg. 1955;12:123. doi:10.3171/jns.1955.12.2.0123
3. TaarnhØJ P. Decompression of the trigeminal root and the posterior part of the ganglion as treatment in trigeminal neuralgia; preliminary communication. J Neurosurg. 1952;9:288–290. doi:10.3171/jns.1952.9.3.0288
4. Urculo E, Martinez L, Arrazola M, Ramirez R. Macroscopic effects of percutaneous trigeminal ganglion compression (Mullan’s technique): an anatomic study. Neurosurgery. 1995;36:776–779. doi:10.1227/00006123-199504000-00019
5. Park SS, Lee M-K, Kim J-W, et al. Percutaneous balloon compression of trigeminal ganglion for the treatment of idiopathic trigeminal neuralgia: experience in 50 patients. J Korean Neurosurg Soc. 2008;43:186–189. doi:10.3340/jkns.2008.43.4.186
6. Asplund P, Linderoth B, Bergenheim AT. The predictive power of balloon shape and change of sensory functions on outcome of percutaneous balloon compression for trigeminal neuralgia. J Neurosurg. 2010;113:498–507. doi:10.3171/2010.2.JNS091466
7. Kouzounias K, Schechtmann G, Lind G, Winter J, Linderoth B. Factors that influence outcome of percutaneous balloon compression in the treatment of trigeminal neuralgia. Neurosurgery. 2010;67:
8. Henderson WR. The anatomy of the gasserian ganglion and the distribution of pain in relation to injections and operations for trigeminal neuralgia. Ann R Coll Surg Engl. 1965;37:346–373.
9. De Cordoba JL, Garcia Bach M, Isach N, Piles S. Percutaneous balloon compression for trigeminal neuralgia: imaging and technical aspects. Reg Anesth Pain Med. 2015;40:616–622. doi:10.1097/AAP.0000000000000292
10. Lobato RD, Rivas JJ, Sarabia R, Lamas E. Percutaneous microcompression of the gasserian ganglion for trigeminal neuralgia. J Neurosurg. 1990;72:546–553. doi:10.3171/jns.1990.72.4.0546
11. Janjua RM, Al-Mefty O, Densler DW, Shields CB. Dural relationships of Meckel cave and lateral wall of the cavernous sinus. Neurosurg Focus. 2008;25:E2. doi:10.3171/FOC.2008.25.12.E2
12. Li Y, Zhang XA, Qi S. Anatomic characteristics of the dural sheath of the trigeminal nerve. Head Neck. 2016;38 Suppl 1:E185–E188. doi:10.1002/hed.23968
13. Schwadron L, Moffett BC. Relationships of cranial nerves to Meckel’s cave and the cavernous sinus. Anat Rec. 1950;106:131–139. doi:10.1002/ar.1091060204
14. Joo W, Yoshioka F, Funaki T, Mizokami K, Rhoton AL
15. Malis LI. Petrous ridge compression and its surgical correction. J Neurosurg. 1967;26, Suppl:163–167. doi:10.3171/jns.1967.26.1part2.0163
16. Brown JA, Pilitsis JG. Percutaneous balloon compression for the treatment of trigeminal neuralgia: results in 56 patients based on balloon compression pressure monitoring. Neurosurg Focus. 2005;18:E10. doi:10.3171/foc.2005.18.5.11
17. Teo MK, Suttner NJ. Effective management of lower divisional pain in trigeminal neuralgia using balloon traction. Br J Neurosurg. 2015;29:343–346. doi:10.3109/02688697.2014.990419
18. Zdilla MJ, Hatfield SA, Mangus KR. Angular relationship between the foramen ovale and the trigeminal impression: percutaneous cannulation trajectories for trigeminal neuralgia. J Craniofac Surg. 2016;27:2177–2180. doi:10.1097/scs.0000000000003138
19. Brinzeu A, Dumot C, Sindou M. Role of the petrous ridge and angulation of the trigeminal nerve in the pathogenesis of trigeminal neuralgia, with implications for microvascular decompression. Acta neurochirurgica. 2018;160:971–976. doi:10.1007/s00701-018-3468-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.