")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
The Swedish Version of the TeamSTEPPS® Teamwork Perceptions Questionnaire (T-TPQ): A Validation Study
Authors Hall-Lord ML , Skoogh A, Ballangrud R, Nordin A, Bååth C
Received 8 May 2020
Accepted for publication 23 July 2020
Published 19 August 2020 Volume 2020:13 Pages 829—837
DOI https://doi.org/10.2147/JMDH.S261768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marie Louise Hall-Lord,1,2 Annika Skoogh,1 Randi Ballangrud,2 Anna Nordin,1 Carina Bååth1,3
1Department of Health Sciences, Faculty of Health, Science and Technology, Karlstad University, Karlstad, Sweden; 2Department of Health Science, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Gjøvik, Norway; 3Faculty of Health and Welfare, Østfold University College, Fredrikstad, Norway
Correspondence: Carina Bååth
Department of Health Sciences, Faculty of Health, Science and Technology, Karlstad University, Universitetsgatan 2, Karlstad 651 88, Sweden
Tel +46 54 7002089
Email [email protected]
Purpose: The delivery of effective and safe healthcare to patients is highly dependent on careful collaboration between healthcare professionals. Although teamwork is an important component for patient safety, effective teamwork is not always carried out in hospital wards, leading to negative consequences for the patients. Teamwork measurements can be used to evaluate and provide feedback to healthcare professionals to support team performance and to identify areas for improvement. The TeamSTEPPS® Teamwork Perceptions Questionnaire (T-TPQ) evaluates Team Structure and four core competences of teamwork (Leadership, Situation Monitoring, Mutual Support, and Communication) among healthcare professionals in various healthcare settings. The questionnaire was judged to be relevant in a Swedish healthcare context and was translated into Swedish. This study aimed to test the reliability and construct validity of the Swedish version of the T-TPQ.
Methods: A total of 450 (of 1176) frontline healthcare professionals working at four hospitals responded to the questionnaire. A confirmatory factor analysis was carried out to test the factor structure. Cronbach’s alpha was used to measure internal consistency.
Results: The hypothesized five-factor model of the five dimensions showed acceptable goodness-of-fit indexes. Cronbach’s alpha coefficient for the total T-TPQ was 0.94, and the Cronbach’s alpha coefficients for the dimensions ranged from 0.79 to 0.92. The intercorrelation coefficients ranged from 0.27 to 0.74.
Conclusion: The Swedish version of the T-TPQ showed acceptable reliability and validity for measuring healthcare professionals’ individual perceptions of teamwork at the group level. Due to the low response rate, further studies are required to test the validity of the Swedish T-TPQ.
Keywords: healthcare professionals, perceptions, questionnaire, teamwork performance, validation study
Introduction
Healthcare organizations operate in a complex context of conflicting demands and objectives. Healthcare is multifaceted and it has challenging tasks and many different professions.1 The delivery of effective and safe healthcare to patients is highly dependent on careful collaboration between healthcare professionals.2 The process of providing healthcare is interdisciplinary and requires people in various professions, such as physicians, nursing staff and allied health professionals, to work in teams.3 A team can be described as two or more individuals who work together to achieve specified and shared goals, have task-specific competencies and specialized work roles, use shared resources, and communicate to coordinate and adapt to change.4 Teamwork is a critical component of patient safety and is described in terms of behavior, cognitions and attitudes that make interdependent performance possible.5 Xyrichis and Ream defined teamwork as
A dynamic process involving two or more health professionals with complementary backgrounds and skills, sharing common health goals and exercising concerted physical and mental effort in assessing, planning or evaluating patient care. This is accomplished through interdependent collaboration, open communication and shared decision-making. (p.238)6
A meta-analysis found that teamwork had a medium-sized effect on clinical performance in various healthcare settings.7 Effective teamwork contributes to fewer medical errors,3 decreased mortality,8 higher patient satisfaction, higher nurse retention, lower hospital cost,9 and improved job satisfaction.10,11 Insufficient interprofessional communication is the most frequent cause of unsatisfactory teamwork12 and contributes to patients being less likely to receive appropriate care,13 and contributes to harm among patients.14 Furthermore, teamwork without common health goals, open communication and information sharing is correlated with reduced organizational performance.15 Hence, teamwork, communication, collaboration16,17 and patient safety culture18,19 have been shown to be improved by team training.
Although it is known that team training improves teamwork, team training has not routinely been implemented in clinical practice. To improve the quality and safety in health care in the US, the Department of Defense and the Agency for Healthcare Research and Quality (AHRQ) developed the Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS®), which is an evidence-based program. TeamSTEPPS was developed according to the framework of the “Big Five”, including the core components of effective teamwork: team leadership, mutual performance monitoring, backup behavior, adaptability and team orientation.20
As a part of TeamSTEPPS, the American Institute of Research developed two questionnaires: the TeamSTEPPS® Teamwork Attitudes Questionnaire (T-TAQ) and the TeamSTEPPS® Teamwork Perceptions Questionnaire (T-TPQ). The T-TAQ measures individuals’ general attitudes about teamwork and the T-TPQ was designed to measure individuals’ perceptions of teamwork in their workplace. Both questionnaires are related to the five dimensions of teamwork, namely, Team Structure, Leadership, Situation Monitoring, Mutual Support and Communication, which represent the core teamwork competencies that mostly affect team performance.21 In the current study, the results of a validation of the T-TPQ are reported, while validation of the T-TAQ is planned to be performed in another study. The original English version of the T-TPQ has been psychometrically validated.21,22 Furthermore, the T-TPQ has been tested among healthcare professionals in Norway23 and among nurses in Korea.24 The questionnaire, which is not limited to specific departments or specialties, measures how healthcare professionals perceive the present state of teamwork.21 The T-TPQ can be used to evaluate and provide feedback to managers and personnel to support team performance.25 As we did not find any Swedish questionnaire measuring perceptions of teamwork and because the T-TPQ seemed to be relevant for a Swedish healthcare context, the questionnaire was translated into Swedish. When a questionnaire is translated into another language and is to be used in another culture, measurement equivalence is required.26 The aim of this study was to test the reliability and construct validity of the Swedish version of the TeamSTEPPS® Teamwork Perceptions Questionnaire (T-TPQ).
Methods
The Questionnaire
The T-TPQ was translated with the permission of the United States AHRQ from the TeamSTEPPS 2.0 National Implementation (accessible at http://teamstepps.ahrq.gov/). The T-TPQ consists of 35 items with seven items in each of the following five dimensions: Team Structure, Leadership, Situation Monitoring, Mutual Support and Communication. Each item has five response options on a Likert scale ranging from 1 = strongly disagree with the statement to 5 = strongly agree with the statement. The scores for the total scale and for each dimension were calculated by adding all items and dividing the score by the number of items in each dimension and in the total scale.21,22
Translation Procedures
The model of Brislin27 inspired the translation of the T-TPQ into Swedish. A professional bilingual translator with Swedish as her native language conducted the forward translation of the original English version of the T-TPQ into Swedish. The research group reviewed the translated version of the T-TPQ, resulting in some semantic and conceptual adjustments. Another professional bilingual translator with English as her native language who was “blinded” to the original English version conducted back-translation of the reviewed Swedish version to English. Members of the research group compared the original version and the back-translated version of the T-TPQ. Few discrepancies were revealed, leading to some minor revisions to the Swedish T-TPQ. To establish semantic equivalence, the translated version was pilot-tested among 15 healthcare professionals working in clinical practice (3 physicians, 8 registered nurses, 2 midwives, 1 nursing assistant and 1 physiotherapist). For each item, the participant had the opportunity to comment on the language, understandability and clarity. A review of the participants’ responses led to some changes to clarify the language and the concepts in the questionnaire. Table 1 shows the Swedish version of the questionnaire.
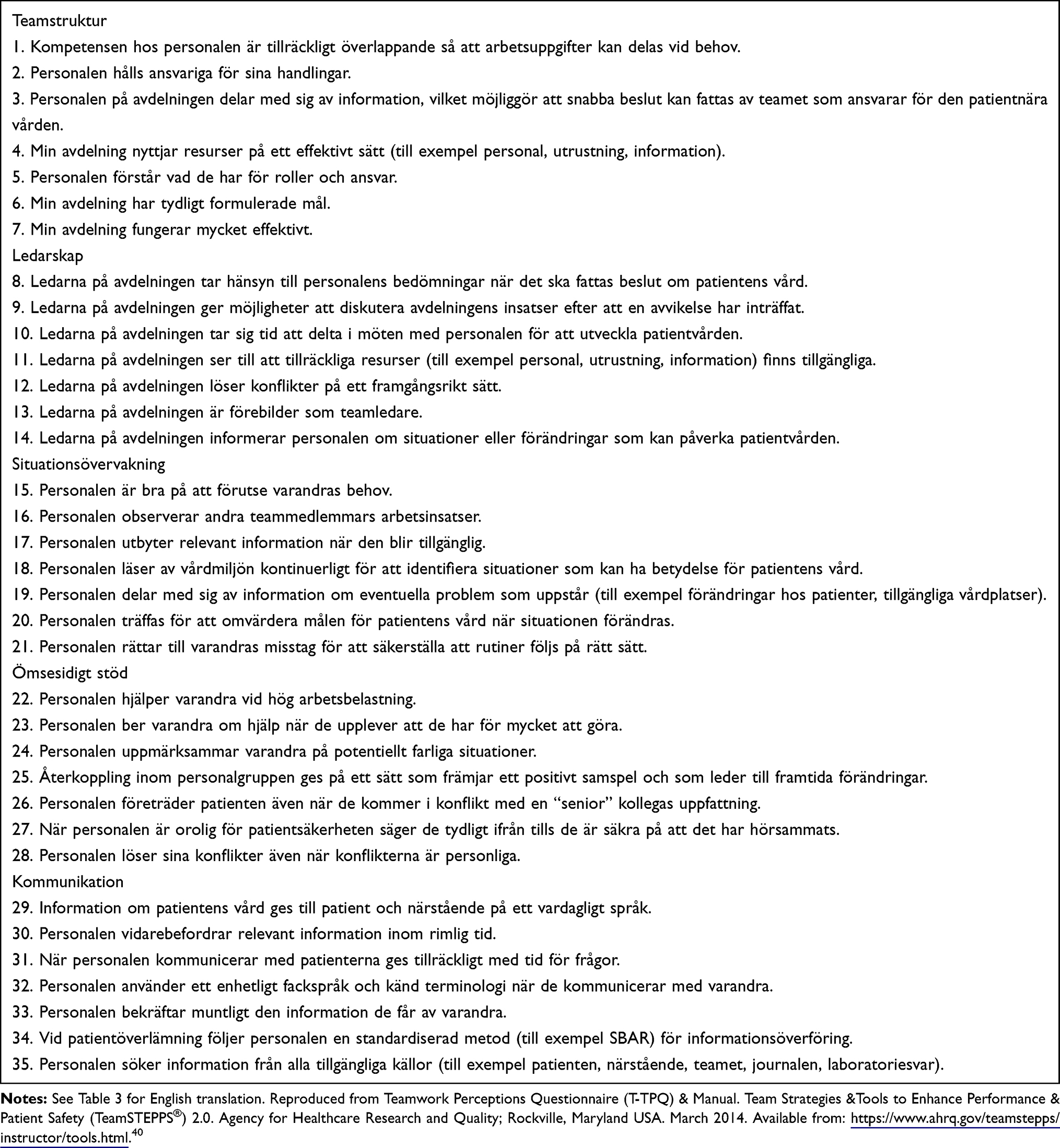 |
Table 1 The Swedish Version of the T-TPQ |
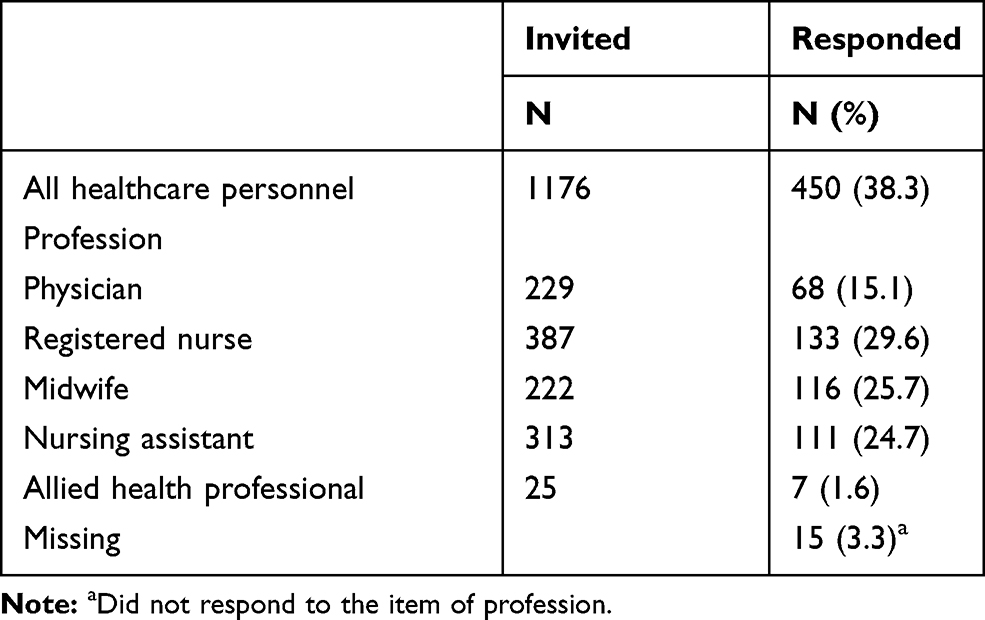 |
Table 2 The Healthcare Professionals |
 |
Table 3 Median, Range, Mean and Standard Deviation for the Total Questionnaire, The Five Dimensions and the Items (T-TPQ) (n = 450) |
Design
The study had a cross-sectional design.
Setting and Sample
Frontline healthcare professionals (physicians, registered nurses, midwives, nursing assistants and allied health professionals) working at four hospitals (Hospital A, Hospital B, Hospital C, and Hospital D) in three healthcare regions in Sweden were included (N = 1176). They were employed in medical wards (Hospital A and Hospital B), emergency rooms (Hospital B), obstetric care wards (Hospital A, Hospital C and Hospital D), gynecological and intensive care wards, and anesthesia and operating rooms (Hospital A). In total, 450 healthcare professionals (38.3%) responded to the T-TPQ. The numbers and percentages of the different healthcare professions who were invited to the study and responded to the questionnaire are shown in Table 2.
Data Collection
A paper version of the T-TPQ with an information letter about the study was distributed to the healthcare professionals between September and December 2018. The chief managers provided information to the healthcare professionals about the study. They also reminded the healthcare professionals to respond to the questionnaire via e-mail or during reports. Completed questionnaires were returned anonymously in self-addressed envelopes.
Data Analysis
Descriptive statistics were analyzed with IBM SPSS statistics, version 25, to describe the median, range, mean, and standard deviation of the scores of the total questionnaire, the teamwork dimensions and the individual items. SPSS was also used to obtain the Cronbach’s alpha coefficients to assess the reliability of the total questionnaire and each of the five teamwork dimensions. Cronbach’s alpha coefficients equal to or greater than 0.70 are considered acceptable.26 Finally, construct interdependence was examined based on the intercorrelations between the five dimensions using Pearson’s r.
The construct validity, ie, the hypothesized five-factor model, was tested in two models (Model 1 and Model 2) by confirmatory factor analysis (CFA) in IBM AMOS, version 25. CFA indicates whether the dimensionality of a construct is similar between an adapted measure and the original measure.26 Data from the respondents who answered all items were included in the CFA (n = 416). CFA provides goodness-of-fit indexes, which show how well the factor pattern complies with the hypothesized model.26 Starting with Model 1, we used the goodness-of-fit indexes to evaluate how well the data fit the hypothesized five-factor model. In accordance with the study by Keebler et al22 who examined the construct validity (via CFA) of the original version of the T-TPQ, we decided to analyze a second model (Model 2).
To assess the strength of the two models, goodness-of-fit indexes were calculated. We included the chi-square goodness of fit (x2), for which the p-value should exceed 0.05; the normed chi-square (chi-square/df), which should be <3; the root-mean-square error of approximation (RMSEA), for which a value of <0.06 indicates a good fit;28 the Tucker-Lewis index (TLI) and the comparative fit index (CFI), which both should exceed 0.95.26 The RMSEA takes into account the error of the approximation in the population,29 and the TLI and CFI evaluate the goodness of fit of a hypothesized model in comparison with a null model.26,29
Results
Table 3 presents the median, range, mean, and standard deviation for the total questionnaire, the five teamwork dimensions and the 35 items. At the dimension level, the highest mean score was found for the Communication dimension, and the lowest mean score was obtained for the Leadership dimension. Items 22, 35, 23, and 19 demonstrated the strongest agreement, while items 28 and 12 showed the strongest disagreement.
For reliability, the Cronbach’s alpha coefficient for the total T-TPQ was 0.94, and the Cronbach’s alpha coefficient for each dimension ranged from 0.79 to 0.92 (Table 4).
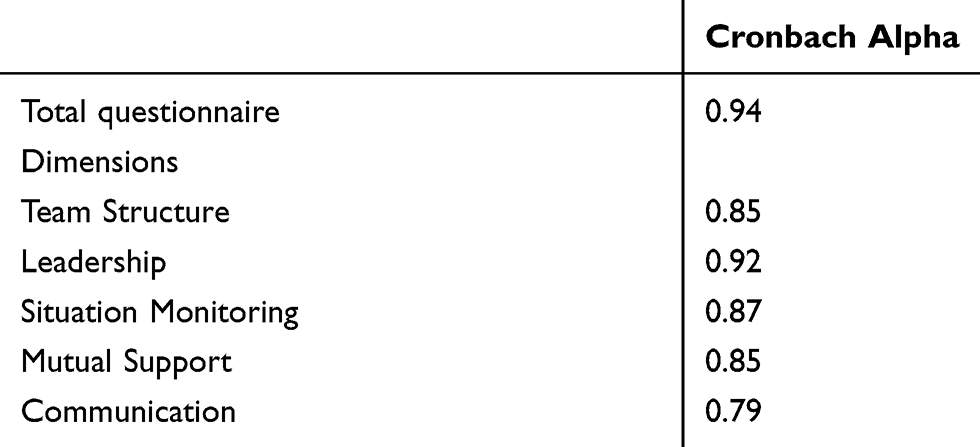 |
Table 4 Internal Consistency for the T-TPQ Total Scale and the Dimensions |
The intercorrelation coefficients of the five teamwork dimensions ranged from 0.27 to 0.74 (Table 5).
 |
Table 5 Intercorrelations of the T-TPQ Dimensions |
The construct validity of the T-TPQ was confirmed by goodness-of-fit indexes. The CFA (Model 1) showed a moderate fit with the data: x2 (df) 1402 (550), p < 0.001, normed chi-square = 2.54, RMSEA = 0.061, TLI = 0.877, CFI = 0.758. To improve the fit of the model, post-hoc modifications (Model 2) according to Keebler et al22 were made, which concerned four sets of items with high modification indexes. This included two items in the Leadership dimension (12 and 13), four items (22 and 23; and 26 and 27) in the Mutual Support dimension, and two items (29 and 31) in the Communication dimension. Model 2 showed that the hypothesized model of the five dimensions fit the data adequately: x2 (df) 1230 (546), p < 0.001, normed chi-square = 2.25, RMSEA = 0.055, TLI = 0.901, CFI = 0.909 (Table 6).
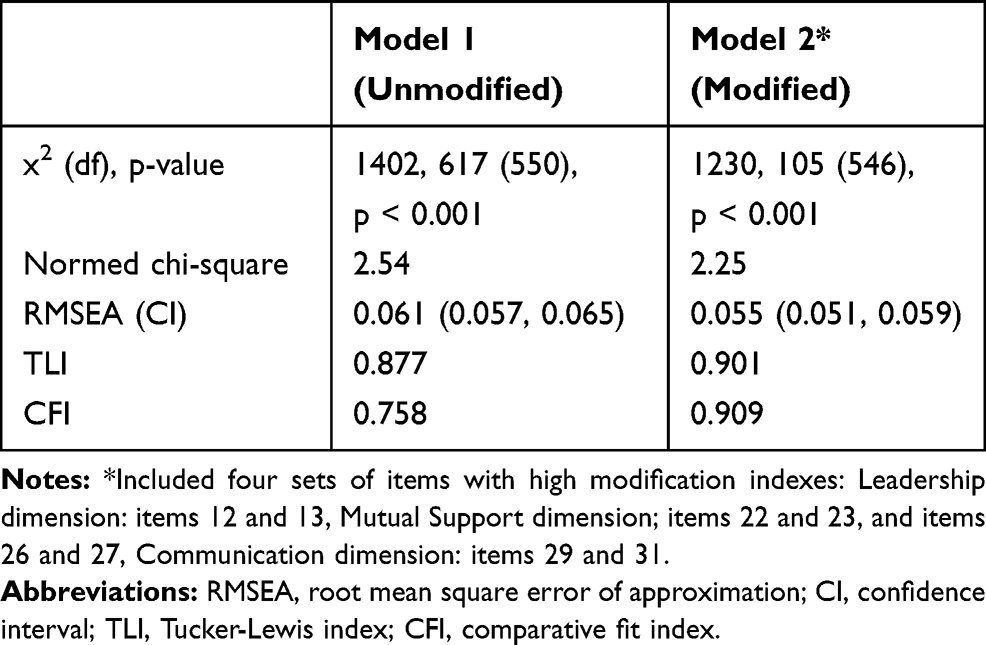 |
Table 6 Confirmatory Factor Analysis Fit Indexes for Each Model (N = 416) |
Discussion
The results of the present study demonstrated that the reliability of the total questionnaire and each of the dimensions were considered acceptable. Other studies also showed acceptable Cronbach’s alpha values for this questionnaire.21,23 Compared to our study, the studies by Battles and King21 and Keebler et al22 demonstrated slightly higher values on all the dimensions, while that of Ballangrud et al23 showed somewhat lower values in all dimensions except for Communication.
The hypothesized five-factor model of Team Structure, Leadership, Situation Monitoring, Mutual Support and Communication had acceptable goodness-of-fit indexes, indicating that this questionnaire can be used to measure teamwork perceptions among healthcare professionals in a hospital setting in Sweden. We conducted the CFA with post hoc modifications in accordance with the study by Keebler et al.22 Post hoc modification may improve the fit due to high modification indexes, which was the case with four pairs of items in three of the five dimensions of the T-TPQ.22 When modifications are used with CFA, it is important that the final model does not deviate from the theoretical model.30 Although each of the four sets of correlated items contained similar content, the items in one dimension showed low correlation with the items in the other dimensions, which indicates that none of the items measures more than one dimension.22
The RMSEA, which is recognized as one of the most informative criteria in CFA,29 had an acceptable fit after the post hoc modification (Model 2). The RMSEA value in this study was almost identical to those reported in the previous research conducted with healthcare personnel.22,23 Hwang and Ahn,24 who performed CFA, demonstrated an RMSEA just below 0.7, which can be explained by the fact that only nurses were included in their sample. The confidence interval in our study was narrow, which could indicate the high precision of the RMSEA in reflecting the model fit in the population.29 Both the CFI and TLI had values below the recommended value (>0.95) in the present study. The values were lower than those in the study by Keebler et al,22 but slightly higher than in the other two studies that conducted CFA.23,24 The better outcome in the study by Keebler et al22 can be explained by the large sample of 1700 staff members. Hu and Bentler28 suggested a TLI close to 0.95 for large samples and noted that when the sample size is small, both the RMSEA and TLI tend to overreject true population models. A sample size of at least 10 cases for each variable is desirable,30 which means a minimum of 350 cases in the analyses in our study. However, even though we had a sample size of 416 for our CFA, larger samples are preferable.26 On the other hand, the chi-square goodness-of-fit (x2) index was significant, probably due to the sample size. The x2 index is sensitive to sample size and therefore seldom used as the only criterion for model fit.26 It is desirable for the normed chi-square value to be less than 3, which was achieved in the present study.
The fit indexes for the final model provide support for the hypothesized theoretical model showing that the five dimensions of the T-TPQ are important components for measuring individual perceptions of teamwork in healthcare settings. We do not recommend changes to the questionnaire. No changes were made after the validation of the original English version of the T-TPQ22 and the T-TPQ manual states that items in the T-TPQ should not be modified.21
The T-TPQ can be used as an assessment of teamwork perceptions to identify areas for improvement and can be administered before and after the implementation of a team training program for comparison and follow-up. In previous studies, the questionnaire was used to evaluate the implementation of the TeamSTEPPS program within various health care specialties19,31-33 and the implementation of other teamwork improvement initiatives.34,35 The T-TPQ was also used to evaluate learning interventions for undergraduate students.36,37 The T-TPQ has the advantage of being sensitive to changes in teamwork perceptions. It is important, however, to be aware of that the T-TPQ is designed to measure perceptions of the five teamwork dimensions and may not be appropriate for the assessment of other aspects of teamwork or objective measures of teamwork behaviors.22 Further efforts to advance research about teamwork may include analyses of the relationship between teamwork perceptions and other outcome measures, such as organizational (eg patient safety culture), professional (eg job satisfaction) and patient outcomes (eg quality of care).
Limitations
The study has several limitations. The sample size was considered sufficient to perform CFA,30 however, the response rate was low and the risk of bias may, therefore, have influenced the external validity.38 The response rate varied somewhat among the profession groups. Midwives had the highest response rate, while physicians and allied health professionals had the lowest response rate. High workload, time pressure and the possibility that teamwork was not a fully known concept for everyone may have influenced the motivation to answer the questionnaire. Since the questionnaire was answered anonymously, it was not possible to carry out a dropout analysis of those who did not reply, which is also a limitation.
Conclusion
The Swedish version of the T-TPQ showed acceptable reliability and construct validity to measure healthcare professionals’ individual perceptions of teamwork at the group level. Teamwork is an important component of patient safety and a core element of highly reliable organizations.39 In hospital settings, measuring teamwork as one component of patient safety can be valuable. Since the T-TPQ is a reasonable time- and cost-effective survey, it can be used in addition to objective measures of teamwork behaviors to evaluate healthcare professionals’ perceptions of teamwork. Due to low response rates and varying response rates in the different profession groups in the current study, further studies are necessary to test the reliability and validity of the Swedish T-TPQ.
Ethics
The Research Ethics Committee at Karlstad University approved the study (C2018/50) and the head manager at each division gave permission to conduct the study. By completing and returning the questionnaire, the healthcare professionals consented to participate in the study.
Acknowledgments
The authors want to thank the healthcare professionals who participated in the study. We also want to thank Jari Appelgren, Karlstad University, Sweden, for statistical support.
Author Contributions
All authors made substantial contributions to the conception and design, data acquisition, or data analysis and interpretation; drafted or written, or substantially revised or critically reviewed the article; agreed on the journal to which the article was submitted, reviewed and agreed on all versions of the article before submission, and during revision; and agreed to be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ramanujam R, Rousseau DM. The challenges are organizational not just clinical. J Organiz Behav. 2006;27:811–827. doi:10.1002/job.411
2. World Health Organization. Framework for Action on Interprofessional Education & Collaborative Practice. Geneva, Switzerland: Health Professions Networks Nursing & Midwifery, Human Resources for Health, Department of Human Resources for Health; 2010. Available from: https://apps.who.int/iris/bitstream/handle/10665/70185/WHO_HRH_HPN_10.3_eng.pdf;jsessionid=5A3D1A8E39A8760F9D797BFA1AF747F6?sequence=1.
3. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol. 2009;53:143–151. doi:10.1111/j.1399-6576.2008.01717.x
4. Brannick MT, Prince C. An overview of team performance measurements. In: Brannick MT, Salas E, Prince C, editors. Team Performance Assessment and Measurement Theory, Research and Applications. New York: Psychology Press, Taylor & Francis Group; 1997:3–10.
5. Salas E, Cooke NJ, Gorman JC. The science of team performance progress and the need for more. Hum Factors. 2010;52(2):344–346. doi:10.1177/0018720810374614
6. Xyrichis A, Ream E. Teamwork: a concept analysis. J Adv Nurs. 2008;61(2):232–241. doi:10.1111/j.1365-2648.2007.04496.x
7. Schmutz JB, Meier LL, Manser T. How effective is teamwork really? The relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open. 2019;9:e028280. doi:10.1136/bmjopen-2018-028280
8. Neily J, Mills PD, Young-Xu Y, et al. Association between implementation of a medical team training program and surgical mortality. JAMA. 2010;304(15):1693–1700. doi:10.1001/jama.2010.1506
9. O’Leary KJ, Sehgal NL, Terrell G, Williams MV. Interdisciplinary teamwork in hospitals: a review and practical recommendations for improvement. J Hosp Med. 2012;7(1):48–54. doi:10.1002/jhm.970
10. Buttigieg SC, West MA, Dawson JF. Well-structured teams and the buffering of hospital employees from stress. Health Serv Manage Res. 2011;24:203–212. doi:10.1258/hsmr.2011.011013
11. Ajeigbe DO, McNeese-Smith D, Phillips LR, Leach LS. Effect of nurse-physician teamwork in the emergency department nurse and physician perception of job satisfaction. J Nurs Care. 2014;3(1):148. doi:10.4172/2167-1168.1000141
12. Kishimoto M, Noda M. The difficulties of interprofessional teamwork in diabetes care: a questionnaire survey. J Multidiscp Healthc. 2014;7:333–339. doi:10.2147/JMDH.566712
13. Scott AM, Li J, Oyewole-Eletu S. Understanding facilitators and barriers to care transitions: insights from Project ACHIEVE site visits. Jt Comm J Qual Patient Saf. 2017;43(9):433–447. doi:10.1016/j.jcjq.2017.02.012
14. Stead K, Kumar S, Schultz TJ, et al. Teams communicating through STEPPS. Med J Aust. 2009;190(Suppl 11):128–132. doi:10.5694/j.1326-5377.2009.tb02619.x
15. West MA, Guthrie JP, Dawson JF, et al. Reducing patient mortality in hospitals: the role of human resource management. J Organiz Behav. 2006;27:983–1002. doi:10.1002/job.396
16. Gillespie BM, Chaboyer W. Enhancing communication in surgery through team training interventions: a systematic literature review. AORN. 2010;92(6):642–657. doi:10.1016/j.aorn.2010.02.015
17. Brock D, Abu-Rish E, Chiu C, et al. Interprofessional education in team communication: working together to improve patient safety. BMJ Qual Saf. 2013;22:414–423. doi:10.1136/bmjqs-2012-000952
18. Jones KJ, Skinner AM, High R, et al. A theory-driven, longitudinal evaluation of the impact of team training on safety culture in 24 hospitals. BMJ Qual Saf. 2013;22:394–404. doi:10.1136/bmjqs-2012-000939
19. Aaberg OR, Ballangrud R, Husebø SE, et al. An interprofessional team training intervention with an implementation phase in a surgical ward. A controlled quasi-experimental study. J Interprof Care. 2019:1–10. doi:10.1080/13561820.2019.1697216.
20. Salas E, Sims DE, Burke CS. Is there a “Big Five” in teamwork? Small Group Res. 2005;36(5):555–599. doi:10.1177/1046496405277134
21. Battles J, King HB. TeamSTEPPS Teamwork Perceptions Questionnaire (T-TPQ) Manual. Washington, DC: American Institutes Research; 2010. Available from: https://www.ahrq.gov/sites/default/files/wysiwyg/teamstepps/instructor/reference/teamperceptionsmanual.pdf.
22. Keebler JR, Dietz AS, Lazzara EH, et al. Validation of a teamwork perception measure to increase patient safety. BMJ Qual Saf. 2014;13:1–9. doi:10.1136/bmjqs-2013-001942
23. Ballangrud R, Husebø SE, Hall-Lord ML. Cross-cultural validation and psychometric testing of the Norwegian version of the TeamSTEPPS® teamwork perceptions questionnaire. BMC Health Serv Res. 2017;17:799. doi:10.1186/s12913-017-2733-y
24. Hwang J-I AJ. Teamwork and clinical error reporting among nurses in Korean hospitals. Asian Nurs Res. 2015;9(1):14–20. doi:10.1016/j.anr.2014.09.002
25. Rosen MA, DiazGranados D, Dietz AS. Teamwork in healthcare: key discoveries enabling safer, high quality care. Am Psychol. 2018;73(4):433–450. doi:10.1037/amp0000298
26. Polit DF, Yang FM. Measurement and the Measurement of Change. A Primer for Health Professions. Philadelphia: Wolters Kluwer; 2016.
27. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1:185–216. doi:10.1177/135910457000100301
28. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
29. Byrne BM. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming.
30. Schreiber JB, Nora A, Stage F, et al. Reporting structural equation modeling and confirmatory factor analysis results: a review. J Educ Res. 2006;99(6):323–338. doi:10.3200/JOER.99.6.323-338
31. Dodge LE, Nippita S, Hacker MR, et al. Impact of teamwork improvement training on communication and teamwork climate in ambulatory reproductive health care. J Healthc Risk Manag. 2018;38(4):44–54. doi:10.1002/jhrm.21353
32. Gaston T, Short N, Ralyea C, et al. Promoting patient safety. Results of a TeamSTEPPS® initiative. J Nurs Adm. 2016;46(4):201–207. doi:10.1097/NNA.0000000000000333
33. Obenrader C, Broome ME, Yap TL, et al. Changing team member perceptions by implementing TeamSTEPPS in an emergency department. JEN. 2019;45(1):31–37. doi:10.1016/j.jen.2018.08.006
34. Tibbs MS, Moss J. Promoting teamwork and surgical optimization: combining TeamSTEPPS with a specialty team protocol. AORN. 2014;100(5):477–488. doi:10.1016/j.aorn.2014.01.028
35. Weaver A, Hernandez S, Olson DM. Clinician perceptions of teamwork in the emergency department: does nurse and medical provider workspace placement make a difference? J Nurs Adm. 2017;47(1):50–55. doi:10.1097/NNA.0000000000000436
36. Carson OM, Laird EA, Reid BB, et al. Enhancing teamwork using a creativity-focussed learning intervention for undergraduate students – a pilot study. Nurse Educ Pract. 2018;30:20–26. doi:10.1016/j.nepr.2018.02.008
37. Fowler TO, Wise HH, Mauldin MP, et al. Alignment of an interprofessional student learning experience wit a hospital quality improvement initiative. J Interprof Care. 2018;11:1–10. doi:10.1080/13561820.2018.1455649
38. Polit DF, Beck CT. Nursing Research: Generating and Assessing Evidence for Nursing Practice.
39. Baker DP, Day R, Salas E. Teamwork is an essential component of high-reliability organizations. Health Serv Res. 2006;41(4):1576–1598. doi:10.1111/j.1475-6773.2006.00566.x
40. Teamwork Perceptions Questionnaire (T-TPQ) & Manual Team Strategies & Tools to Enhance Performance & Patient Safety (Teamstepps®) 2.0. Rockville, Maryland USA: Agency for Healthcare Research and Quality; March 2014. Available from: https://www.ahrq.gov/teamstepps/instructor/tools.html.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.