")
Back to Journals » Infection and Drug Resistance » Volume 15
The Sustained and Marked Elevation of Serum Procalcitonin in a Hemodialysis Patient with Tuberculous Lymphadenitis, but Without the Evidence of Sepsis: A Case Report
Authors Luo P, Long Y, Ma L , Tao Y, Gou S
Received 17 June 2022
Accepted for publication 26 August 2022
Published 2 September 2022 Volume 2022:15 Pages 5161—5166
DOI https://doi.org/10.2147/IDR.S378894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Peiyi Luo,1,2,* Yanqiong Long,1,* Liang Ma,2 Ye Tao,1 Shenju Gou1
1Department of Nephrology, West China Hospital of Sichuan University, Chengdu, People’s Republic of China; 2Kidney Research Institute, West China Hospital of Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ye Tao; Shenju Gou, Department of Nephrology, West China Hospital of Sichuan University, Chengdu, 610041, People’s Republic of China, Tel/Fax +86-28-85423341, Email [email protected]; [email protected]
Background: The elevation of serum procalcitonin (PCT) has been considered as a marker of systemic bacterial infection and sepsis. However, the marked elevation of PCT in non-sepsis conditions was rare. Here, we report a rare case of sustained markedly elevation of serum PCT in a dialysis patient with tuberculosis, but without the evidence of sepsis.
Case Presentation: A 25-year-old man on maintenance hemodialysis was admitted to the hospital for kidney transplantation. On admission, physical examination revealed multiple lymph nodes were palpable on both sides of the neck which was later confirmed as tuberculosis with biopsy pathology. On the 3rd day after admission, the patient suffered from fever with a temperature of 38.8°C. The white blood cells 12.35 × 109/L and the PCT level was 5.73 ng/mL. Lately the PCT increased to 63.10 ng/mL, and the level of C-reactive protein was 186.00 mg/L. After the antibiotics upgraded from cefmetazole to meropenem, and vancomycin was added, the body temperature dropped to the normal range on the 17th day and remained normal thereafter. The PCT level declined gradually to 4.18 ng/mL on the 21st day and an antituberculosis regimen was started. After that, the PCT levels fluctuated between 2.9 ng/mL and 94.9 ng/mL without any manifestation of sepsis. The markedly elevation of serum PCT level persisted despite normal C-reactive protein level and leukocyte counts.
Conclusion: Persistently elevated serum PCT level might occur in conditions without evidence of sepsis. Taking consideration of multiple inflammatory factors to determine infection when the markedly elevated PCT level was not correlated with the clinical manifestations.
Keywords: procalcitonin, bacterial infection, dialysis, tuberculosis
Background
As the precursor of calcitonin, procalcitonin (PCT) regulates the calcium homeostasis in organisms.1 PCT is composed of 116 amino acids. In physiological conditions, PCT was thought to be synthesized by thyroid C cells, and the blood concentration of PCT was very low (typically < 0.05 ng/mL). When bacterial infections occurred, especially for systemic infections and sepsis, an extra-thyroid synthesis of PCT will be induced in several organs, including the lung, liver, pancreas, kidney, and intestine, as well as in leukocytes. The circulating PCT could be enhanced from 100-fold to 10,000-fold over.2 The elevated PCT in plasma (generally more than 0.5 ng/mL) have been considered as a marker of systemic bacterial infection and could facilitate the differentiating bacterial from viral disease. In addition, the PCT level was found to decline during the recovery of infection. The magnitude of elevated PCT levels is often correlated with the severity of infections, where PCT was widely accepted as an indicator for antibiotic usage or early cessation in clinic.3–7 Of note, the elevated PCT may also be found in some non-infectious conditions, such as trauma, surgery, still syndrome, medullary thyroid carcinoma, and renal dysfunction. However, the PCT level in these cases was not high (often less than 10 ng/mL).8 Here, we reported a rare case of the sustained markedly elevation of PCT level in a maintained dialysis patient with tuberculosis, but without the evidence of sepsis.
Case Presentation
A 25-year-old Chinese man presented with the edema of the lower limbs and kidney dysfunction two years ago. The patient was then diagnosed as IgA nephropathy, based on the pathologic result of renal biopsy. The serum creatinine level was 222 μmol/L at that time. One year ago, the serum creatinine was increased to more than 600 μmol/L and regular hemodialysis was initiated. The patient was admitted to our hospital in August 2020 for kidney transplantation. On admission, physical examination revealed that multiple lymph nodes were palpable on both sides of the neck, which were painless and mobile. The maximal one with a size of 5 cm ×3 cm was on the right supraclavicular fossa of the neck. The tremor of the arteriovenous fistula for hemodialysis on the left forearm was well. The results of a routine peripheral blood test at the time of admission were as follows: hemoglobin 89 g/L, white blood cells 10.80 × 109/L, neutrophil percentage 83.4%, and platelets 490 × 109/L. The serum creatinine was 1429 μmol/L. The computed tomography (CT) scan of the chest and abdomen revealed two inflammatory small nodules of 0.3 cm in the lower lobes of both lungs and reduced sizes of both kidneys. Regular hemodialysis (three times per week) was performed. On the 3rd day after admission, the patient suffered from fever, with a temperature of 38.8°C. The repeated blood test results were as follows: hemoglobin 86 g/L, white blood cells 12.35 × 109/L, neutrophil percentage 77.9%, and platelets 474 × 109/L. The PCT level was 5.73 ng/mL and cefmetazole was prescribed. PCT was measured using the electrochemical luminescence method (VIDAS Brahms PCT, Mannheim, Germany) according to the manufacturer’s instructions. On the 10th day after admission, the symptom of fever was not well controlled and the patient still suffered from intermittent fever, with a maximal body temperature of 39.9°C. The PCT increased to 26.7 ng/mL. Antibiotic was upgraded to meropenem accordingly. On the 12th day after admission, although the temperature dropped to below 38°C after adjusting the antibiotic, the PCT increased to 63.10 ng/mL, and the level of C-reactive protein (CRP) was 186.00 mg/L (normal range <5 mg/L). Vancomycin was added. On the 14th day after admission, the biopsy of the lymph node on the right supraclavicular fossa of the neck was performed. On the 17th day after admission, the body temperature dropped to the normal range and remained normal in the remaining duration of the hospital stay. The histopathology result of lymph node biopsy revealed as inflammatory necrosis with granulomatous formation (Figure 1). The acid-fast staining was positive and a small number of DNA fragments of Mycobacterium tuberculosis was detected by Tuberculosis (TB)-qPCR monitoring. On the 21st day after admission, an antituberculosis regimen consisting of isoniazid, rifapentine, ethambutol, and levofloxacin was started and the surgery for kidney transplantation was canceled. The PCT declined gradually to 4.18 ng/mL on the same day and the antibiotics were downgraded to Piperacillin-tazobactam. On the 24th day after admission, the PCT level, dropped to the lowest point in admission monitoring, at 2.9 ng/mL. After that, the PCT increased gradually to 39.4 ng/mL on the 41st day after admission. There was no fever, cough, diarrhea, abdominal pain, frequent urination, and painful urination et al. The count of white blood cells was 4.58×109/L. The level of IL-6 was 8.55 pg/mL (normal range 0–7 pg/mL) and the level of CRP was 11.1 mg/L. The antibiotics were upgraded to meropenem and vancomycin again with the antituberculosis regimen continued. However, there was no marked decline of serum PCT levels. On the 51st day after admission, the PCT level was 94.9 ng/mL. The count of white blood cells was 3.8×109/L. Twice blood cultures were performed and the results were negative. The parasite antigen test was negative. The echocardiography test showed no obvious abnormalities in cardiac structure or blood flow. The thyroid function was normal. The patient was present with no complaint and in good spirit. After another 21 days course of treatment with both meropenem and vancomycin, On the 61st day after admission, the PCT level was 42.6 ng/mL. The count of white blood cells was 3.91×109/L. The levels of IL-6 and CRP were in the normal range (3.02 pg/mL and 4.27 mg/L, respectively). Without the obvious clinical manifestation of sepsis, the antibiotics meropenem and vancomycin were stopped and the patient was discharged from the hospital (Figure 2). However, the antituberculosis regimen was still going on. One month after the discharge, the patient was in a good state and complained no discomfort. He was retested with the PCT of 2.941 ng/mL and the metagenomic Next-Generation Sequencing of pathogenic microorganisms was negative.
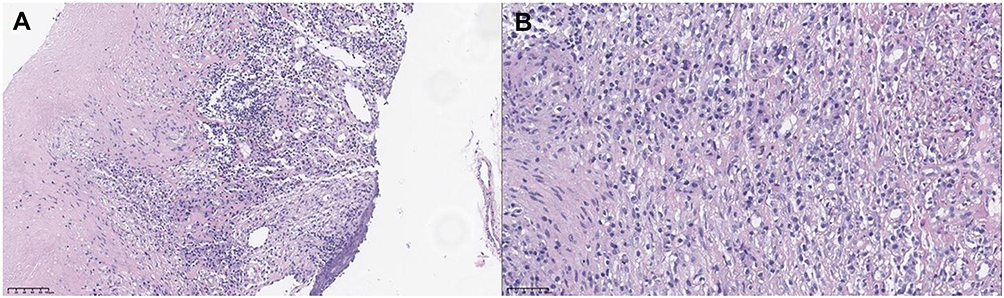 |
Figure 1 The histopathological findings of the lymph node biopsy. (A) Inflammatory necrosis with granulomatous formation. Magnification, x200. Hematoxylin and eosin staining. (B) Inflammatory necrosis with granulomatous formation. Magnification, x400. Hematoxylin and eosin staining. |
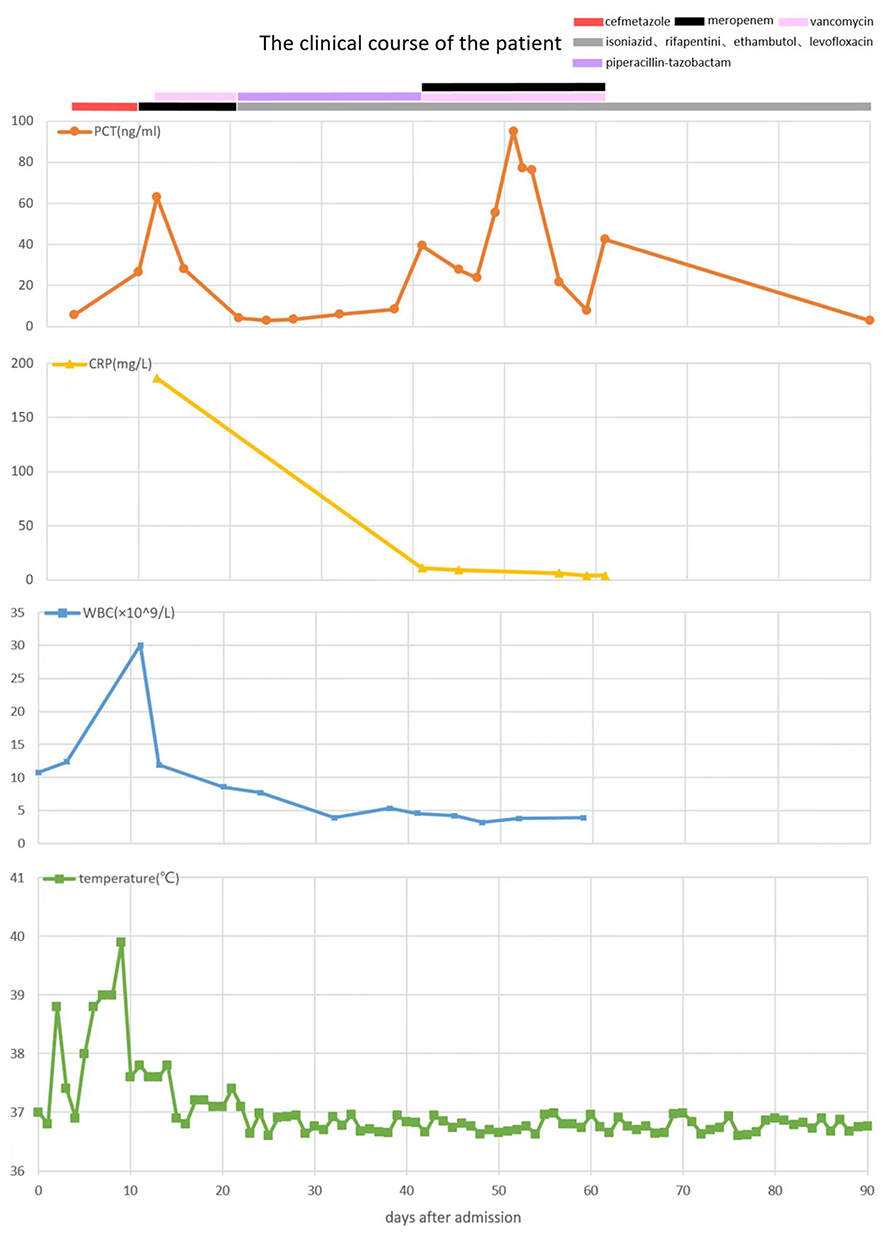 |
Figure 2 The clinical course of the present case. The X-axis shows the number of days after admission. The serum procalcitonin levels (Orange), C-reactive protein levels (yellow), white blood cells (blue), and temperature (green) variations were recorded. Multiple antimicrobials were given to the patient. Periods using cefmetazole, meropenem, vancomycin, piperacillin-tazobactam, and antituberculosis regimen consisting of isoniazid, rifapentine, ethambutol, and levofloxacin were marked by red, black, pink, purple and gray thick lines, respectively. |
Discussion and Conclusions
As a biomarker of bacterial infection, the diagnostic value of PCT for sepsis was highlighted in clinical settings. Although the mild to moderate elevation of PCT had been observed in some clinical conditions, such as surgery, shock, trauma, hepatic or renal failure, severe pancreatitis, malignancy particularly neuroendocrine neoplasm, et al,8 the marked elevation of PCT in non-sepsis condition was rare. We here reported a rare case of the sustained marked elevation of PCT level in a maintained dialysis patient with tuberculosis, but without other evidence of sepsis.
In the present case, the marked elevation of PCT occurred in a patient with the clinical setting of end-stage kidney disease. Several studies had reported that uninfected chronic kidney disease (CKD) patients had higher PCT levels than the general population.9 Furthermore, the baseline PCT levels were negatively correlated with renal function in CKD patients.10,11 Wu et al9 Enrolled the 361 CKD patients without infection and 119 healthy controls. The serum PCT level in CKD patients was significantly higher than that in healthy controls (0.44 ng/mL versus 0.04 ng/mL). In addition, the serum PCT levels increased with the CKD stages (0.50 ng/mL in CKD stage 5, 0.21 ng/mL in CKD stage 4 and 0.20 ng/mL in CKD stage 3). However, the reported baseline value of uninfected CKD patients was not very high. PCT levels could still be used as the indicators of infection with a relatively higher cut-off value in CKD patients. Lee et al12 reported that in individuals with end-stage renal disease, the PCT levels at a cut-off value of 0.75 ng/mL were an appropriate predictor of infection. Herget-Rosenthal et al13 considered that a cut-off value of PCT at 1.5 ng/mL was appropriate for determining severe infection and sepsis in hemodialytic patients. The reason why PCT mildly increase in CKD patients remains unclear. One possible explanation was that in CKD patients, renal impairment leaded to decreased glomerular clearance, consequently resulting in accumulation of low molecular weight proteins such as PCT.14 However, Meisner et al15 observed that there was no association between the PCT half-life and creatinine clearance. Another factor was micro-inflammation. Micro-inflammation referred to a disease state characterized by persistent and low-grade inflammation, which was prevalent in CKD patients. Kidney disease promoted the production and the release of inflammatory cytokines.16 In this case, the lowest PCT level after admission was 2.9 ng/mL on day 24 and the highest was 94.9 ng/mL on day 51 without manifestation of infection, which significantly exceeded the average PCT levels and cut-off values reported in previous literatures. Based on the previous studies, the markedly increased PCT levels could not be explained by CKD or dialysis in the present case.
Of note, this case was also diagnosed with tuberculosis, which might be another factor influencing the PCT levels. Studies reporting PCT levels in tuberculosis patients were limited and the PCT levels varied widely. In the study by Rasmussen et al, 218 tuberculosis patients were included.17 It was found that the PCT levels in tuberculosis patients were higher than those in healthy controls. However, the median PCT levels were less than 0.25 ng/mL in both groups. Only 5% of patients surpassed this value. Similarly, Ugajin et al18 showed an average PCT level of 0.21 ng/mL in a study of 102 patients with tuberculosis. However, the study by Huang et al19 Enrolled the 243 tuberculosis patients with an average PCT level of 0.47 ng/mL. A meta-analysis reported that the cut-off values of PCT to identify sepsis used in the tuberculosis patients were between 0.10 and 0.25 ng/mL.20 To sum up, PCT levels were only mildly elevated in tuberculosis patients overall, although some studies had found higher baseline PCT levels in tuberculosis patients than in healthy controls. The causes for the inert response of PCT in tuberculosis patients have yet to be determined. There were several possible explanations. Firstly, tuberculous infection might secrete more IFN-γ than other bacterial infections to inhibit PCT production.21,22 Secondly, PCT levels depended on the inflammatory cytokine cascade and were therefore closely related to the number of organisms that entered the systemic circulation, however, the number of organisms in tuberculosis infection was usually low.18 In this case, after the sepsis controlled, the lowest PCT level monitored was 2.9 ng/mL, significantly higher than the reported baseline PCT levels in patients with tuberculosis. Consequently, the markedly elevated PCT levels in this case could not be attributed to tuberculosis.
The potential causes leading to the significantly elevated PCT levels in non-sepsis patients like the present case were to be explored. Nowadays, the markedly elevated PCT level was an important indicator of sepsis. As mentioned above, PCT levels could also increase in some non-infectious situations, just like the patient in the present case. When the markedly elevated PCT level was not correlated with the clinical manifestations, taking the consideration of multiple inflammatory factors, such as the levels of CRP, interleukin-6, leukocyte counts, and neutrophil percentage were needed.23
In conclusion, the present case reported a rare case of sustained markedly elevation of serum PCT levels in a patient without the evidence of sepsis. This case might raise the question of PCT as a conclusive evidence of sepsis. The cause of the marked elevation of PCT in non-infectious diseases needs further exploration.
Abbreviations
PCT, procalcitonin; CRP, C-reactive protein; CKD, chronic kidney disease.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent for Publication
The patient provided written informed consent to allow the case details and any accompanying images to be published. No specific ethics committee approval was required for this study.
Acknowledgments
We thank the patient for his participation and cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by Sichuan Science and Technology Program (No.2020JDRC0022).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. MüLler B, White JC, NyléN E, et al. Ubiquitous expression of the calcitonin-i gene in multiple tissues in response to sepsis. J Clin Endocrinol Metab. 2001;86(1):396–404. doi:10.1210/jcem.86.1.7089
2. Lippi G, Sanchis-Gomar F. Procalcitonin in inflammatory bowel disease: drawbacks and opportunities. World J Gastroenterol. 2017;23(47):8283–8290. doi:10.3748/wjg.v23.i47.8283
3. Schuetz P, Raad I, Amin DN. Using procalcitonin-guided algorithms to improve antimicrobial therapy in ICU patients with respiratory infections and sepsis. Curr Opin Crit Care. 2013;19(5):453–460. doi:10.1097/MCC.0b013e328363bd38
4. Schuetz P, Wirz Y, Sager R, et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: a patient level meta-analysis. Lancet Infect Dis. 2018;18(1):95–107. doi:10.1016/s1473-3099(17)30592-3
5. de Jong E, van Oers JA, Beishuizen A, et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: a randomised, controlled, open-label trial. Lancet Infect Dis. 2016;16(7):819–827. doi:10.1016/s1473-3099(16)00053-0
6. Schuetz P, Beishuizen A, Broyles M, et al. Procalcitonin (PCT)-guided antibiotic stewardship: an international experts consensus on optimized clinical use. Clin Chem Lab Med. 2019;57(9):1308–1318. doi:10.1515/cclm-2018-1181
7. Assicot M, Gendrel D, Carsin H, et al. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 1993;341(8844):515–518. doi:10.1016/0140-6736(93)90277-n
8. Meisner M. Update on procalcitonin measurements. Ann Lab Med. 2014;34(4):263–273. doi:10.3343/alm.2014.34.4.263
9. Wu SC, Liang CX, Zhang YL, et al. Elevated serum procalcitonin level in patients with chronic kidney disease without infection: a case-control study. J Clin Lab Anal. 2020;34(2). doi:10.1002/jcla.23065
10. Sun Y, Jiang L, Shao X. Predictive value of procalcitonin for diagnosis of infections in patients with chronic kidney disease: a comparison with traditional inflammatory markers C-reactive protein, white blood cell count, and neutrophil percentage. Int Urol Nephrol. 2017;49(12):2205–2216. doi:10.1007/s11255-017-1710-z
11. Park JH, Kim DH, Jang HR, et al. Clinical relevance of procalcitonin and C-reactive protein as infection markers in renal impairment: a cross-sectional study. Crit Care. 2014;18(6). doi:10.1186/s13054-014-0640-8
12. Lee WS, Kang DW, Back JH, et al. Cutoff value of serum procalcitonin as a diagnostic biomarker of infection in end-stage renal disease patients. Korean J Intern Med. 2015;30(2):198–204. doi:10.3904/kjim.2015.30.2.198
13. Herget-Rosenthal S, Marggraf G, Pietruck F, et al. Procalcitonin for accurate detection of infection in haemodialysis. Nephrol Dial Transplant. 2001;16(5):975–979. doi:10.1093/ndt/16.5.975
14. Meisner M, Lohs T, Huettemann E, et al. The plasma elimination rate and urinary secretion of procalcitonin in patients with normal and impaired renal function. Eur J Anaesthesiol. 2001;18(2):79–87. doi:10.1046/j.0265-0215.2000.00783.x
15. Meisner M, Schmidt J, Huttner H, et al. The natural elimination rate of procalcitonin in patients with normal and impaired renal function. Intensive Care Med. 2000;26:S212–S216. doi:10.1007/s001340051146
16. Kubo S, Iwasaki M, Horie M, et al. Biological variation of procalcitonin levels in hemodialysis patients. Clin Exp Nephrol. 2019;23(3):402–408. doi:10.1007/s10157-018-1639-2
17. Rasmussen TA, Sogaard OS, Camara C, et al. Serum procalcitonin in pulmonary tuberculosis. Int J Tuberc Lung Dis. 2011;15(2):251–256.
18. Ugajin M, Miwa S, Shirai M, et al. Usefulness of serum procalcitonin levels in pulmonary tuberculosis. Eur Respir J. 2011;37(2):371–375. doi:10.1183/09031936.00011910
19. Huang CT, Lee LN, Ho CC, et al. High serum levels of procalcitonin and soluble TREM-1 correlated with poor prognosis in pulmonary tuberculosis. J Infect. 2014;68(5):440–447. doi:10.1016/j.jinf.2013.12.012
20. Huang SL, Lee HC, Yu CW, et al. Value of procalcitonin in differentiating pulmonary tuberculosis from other pulmonary infections: a meta-analysis. Int J Tuberc Lung Dis. 2014;18(4):470–477. doi:10.5588/ijtld.13.0449
21. Soderblom T, Nyberg P, Teppo AM, et al. Pleural fluid interferon-gamma and tumour necrosis factor-alpha in tuberculous and rheumatoid pleurisy. Eur Respir J. 1996;9(8):1652–1655. doi:10.1183/09031936.96.09081652
22. Ribera E, Ocana I, Martinezvazquez JM, et al. High-level of interferon-gamma in tuberculous pleural effusion. Chest. 1988;93(2):308–311. doi:10.1378/chest.93.2.308
23. England JT, Del Vecchio MT, Aronoff SC. Use of serum procalcitonin in evaluation of febrile infants: a meta-analysis of 2317 patients. J Emerg Med. 2014;47(6):682–687. doi:10.1016/j.jemermed.2014.07.034
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.