")
Back to Journals » Clinical Interventions in Aging » Volume 18
The Surgical Timing and Prognoses of Elderly Patients with Hip Fractures: A Retrospective Analysis
Authors Sun L, Wang C, Zhang M, Li X, Zhao B
Received 16 February 2023
Accepted for publication 17 May 2023
Published 2 June 2023 Volume 2023:18 Pages 891—899
DOI https://doi.org/10.2147/CIA.S408903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Lili Sun, Cong Wang, Mingqing Zhang, Xiang Li, Bin Zhao
Department of Emergency, Beijing Jishuitan Hospital, Beijing, People’s Republic of China
Correspondence: Bin Zhao, Department of Emergency, Beijing Jishuitan Hospital, No. 31 of Xinjiekou East Street, Xicheng District, Beijing, 100035, People’s Republic of China, Tel +86-1058516417, Fax +86-1058516931, Email [email protected]
Background: Guidelines exist for the surgical treatment of hip fractures, but the association between the surgical timing and the incidence of postoperative complications and other important outcomes in elderly patients with hip fracture remains controversial.
Objective: This study aims to explore the association between the surgical timing and the prognoses in elderly patients with hip fracture.
Methods: A total of 701 elderly patients (age ≥ 65 years) with hip fractures who were treated in our hospital from June 2020 to June 2021 were selected. Patients who underwent surgery within 2 d of admission were assigned to the early surgery group, and those who underwent surgery after 2 d of admission were assigned to the delayed surgery group. The prognosis indices of the patients in the two groups were recorded and compared.
Results: The length of postoperative hospitalisation in the early surgery group was significantly lower than that in the delayed surgery group (P < 0.001). The European quality of life questionnaire (EQ-5D) utility in the delayed surgery group was significantly lower than that in the early surgery group at 30 days and 6 months after operation (P< 0.05). Compared with the delayed surgery group, the incidence of pulmonary infection, urinary tract infection (UTI) and deep vein thrombosis (DVT) in the early surgery group were significantly lower. There were no significant differences between the two groups in terms of mortality and excellent rates of the HHS at six months after the operation. In addition, the early surgery group had a lower readmission rate than the delayed surgery group [34 (9.5%) vs 56 (16.3%), P = 0.008].
Conclusion: Earlier surgery can reduce the incidence of pulmonary infections, UTI, DVT and readmission rate among elderly patients with hip fractures, shorten postoperative hospitalisation.
Keywords: Hip fracture, elderly patients, timing of surgery, prognosis
Introduction
Hip fractures are the most common type of fracture among elderly people and have significant morbidities and possible life-threatening complications.1 Surgeries, such as total or partial hip replacements, are the common treatments for hip fractures.2 At the same time, the timing of surgery is considered to play an important role in survival. International clinical practice guidelines recommend surgical treatment of acute hip fractures within 24–48 hours after admission,3,4 but these recommendations are still controversial.5 Proponents of early treatment argue that early surgical intervention could improve the prognoses of patients and minimises the time a patient is confined to bed rest, thereby reducing the risk of associated complications, such as pressure sores, deep vein thrombosis (DVT) and urinary tract infection (UTI)6,7 However, those favouring a delay believe it provides the opportunity to optimise patients’ medical status, thereby decreasing the risk of perioperative complications.6,8 Most studies have shorter follow-up observation times and tend to pay more attention to the survival rate of patients, while ignoring the postoperative quality-of-life concerns caused by psychological changes and decreased physical and social functions.9,10 The association of the timing of surgery and the prognosis of elderly patients with hip fractures needs more research to explore these issues.
This study retrospectively analysed the clinical and six-month follow-up data of elderly patients admitted to our hospital with hip fractures. More specifically, the following question was addressed: Among patients 65 years of age or older who underwent surgery for hip fractures, what was the effect of early surgery, relative to delayed surgery, on all-cause mortality and postoperative complications?
Data and Methods
Population
A total of 701 elderly patients with hip fractures admitted to our hospital from June 2020 to June 2021 were recruited as subjects. All data collected from patients medical files retrospectively.
The inclusion criteria were as follows: (1) patients who were ≥65 years old, (2) patients with hip fractures, and (3) patients with complete preoperative examinations who had received surgical treatment.
The exclusion criteria were as follows: (1) patients with old fractures (fractures over three weeks), (2) patients with pathological fractures, (3) patients who had received conservative treatment, or (4) patients who refused follow-up and had incomplete data.
The subjects were divided into two groups according to surgical timing. Those who had received surgery within 2 d of admission were placed into the early surgery group, while those who received surgery after 2 d of admission were placed into the delayed surgery group.11–13 The patients were followed up six months later by phone or outpatient service, when they completed questionnaires used to determine the survival status and Harris Hip Scores (HHS) (Figure 1). This study was approved by our hospital ethic committee. Patients were contacted by telephone and informed consent was obtained.
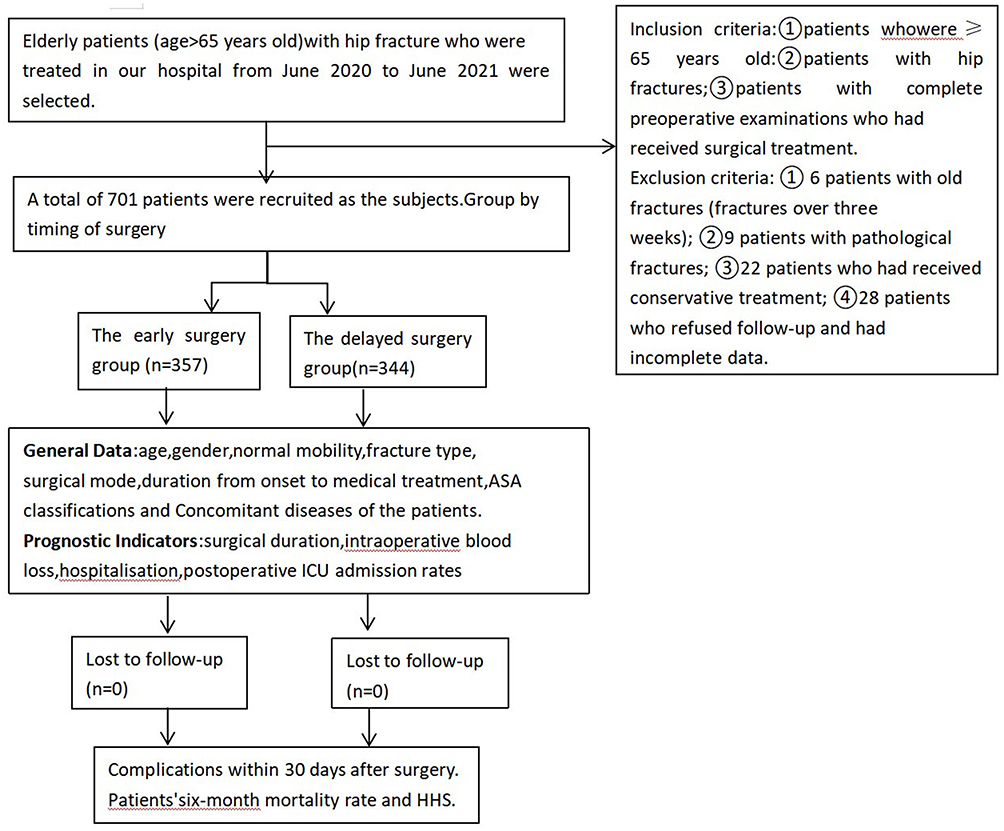 |
Figure 1 Flow Diagram of Participant Recruitment. |
Data Collection Procedures
Data were collected from all included patients included demographics (age, gender and normal mobility), fracture type (femoral neck, intertrochanteric or subtrochanteric), surgical mode (closed reduction and internal fixation of femoral neck fracture, artificial femoral head replacement, total hip arthroplasty, closed reduction and intramedullary nail of intertrochanteric fracture), duration from onset to medical treatment and American Society of Anaesthesiologists (ASA) physical status classifications of the patients.
Observations of Prognostic Indicators
Perioperative indicators were as follows: surgical duration, intraoperative blood loss, postoperative hospitalisation, and postoperative intensive care unit (ICU) admission rates (the percentage of patients admitted to ICU after surgery). Quality of life index at 30 days and 6 months after operation.In this study, the European quality of life questionnaire (EQ-5D) was used to evaluate the postoperative health status of elderly patients with hip fracture. The content includes: action ability, self-care, daily activities, pain/discomfort, anxiety/depression. The score of each item includes: 1 point (no difficulty), 2 points (moderate difficulty), and 3 points (extremely difficult). According to the choices made by the respondents in the questionnaire, the EQ-5D score is converted into the EQ-5D index through the utility value conversion table The higher the EQ-5D index, the better the quality of life. The Chinese EQ-5D score conversion system table was used.14
Complications within 30 d after surgery were as follows: pulmonary infection, UTI, cardiovascular event, cerebral infarction, delirium, DVT of the lower limbs, PE, pressure ulcer, stress ulcer with bleeding, intestinal obstruction, incision infection and others.
Prognostic indicators were as follows: patients’ six-month mortality rate and HHS. The HHS can be divided into four grades based on address pain, walking function, daily activity and range of motion, comprising excellent (90–100 points), good (80–89 points), medium (70–79 points) and poor (<70 points).15 The excellent and good rates of hip joint function were calculated as (excellent + good) cases / total cases × 100%.
Statistical Processing
The SPSS™ Statistics v26.0 software was adopted for data analysis. The measurement data were tested for normality using the Shapiro–Wilk normality test, with the results expressed as mean (standard deviation) (mean [SD]). Those conditions not aligned with the normal distribution were described with median and interquartile range (M [Q1, Q3]). The Categorical variable data were expressed as the percentage of cases (n%). Measurement variable data were compared by Student’s t-test when the distribution was normal or by the Fisher’s exact test if it the distribution was not normal. Chi-squared tests were used for categorical variable data. A P value of <0.05 was deemed statistically significant.
Results
General Clinical Data
A total of 701 patients were included in this study. Among them, 357 patients (104 male and 253 female) with an average age of 80.10 years (8.20) were placed into the early surgery group. The remaining 344 patients (97 male and 247 female) with an average age of 79.56 years (8.15) were placed into the delayed surgery group. There were no significant differences in age, gender, Body Mass Index (BMI), normal mobility, fracture type, surgical mode, duration from the onset to medical treatment, ASA physical status classification or concomitant diseases between the two groups (Table 1).
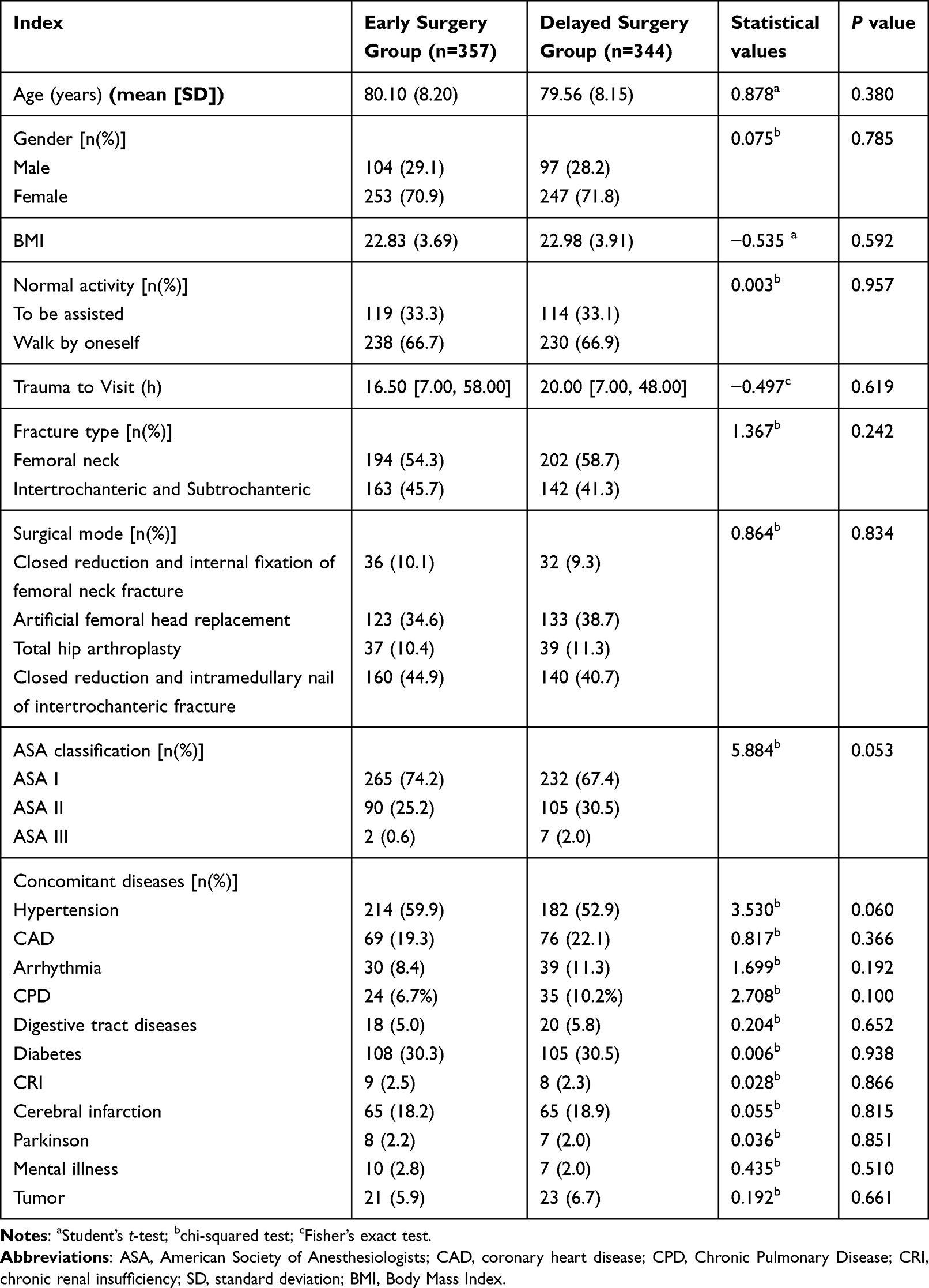 |
Table 1 Comparison of General Clinical Data Between Two Groups |
Comparison of Perioperative Indicators
The perioperative parameters between the two groups were compared and the results are presented in Table 2. There were no significant differences in surgical duration, intraoperative blood loss or postoperative ICU admission rates between the two groups. The length of postoperative hospitalisation in the early surgery group (4 [3, 5] d) was shorter than that of the delayed surgery group (5 [4, 7] d), with a significant difference (P < 0.001). The EQ-5D utility value was 0.552 (0.196) in the early operation group and 0.511 (0.195) in the delayed operation group 30 days after operation, the difference was statistically significant (P<0.05); The EQ-5D utility value was 0.707 (0.147) in the early operation group and 0.652 (0.189) in the delayed operation group 6 months after operation, with a statistically significant difference (P<0.05).
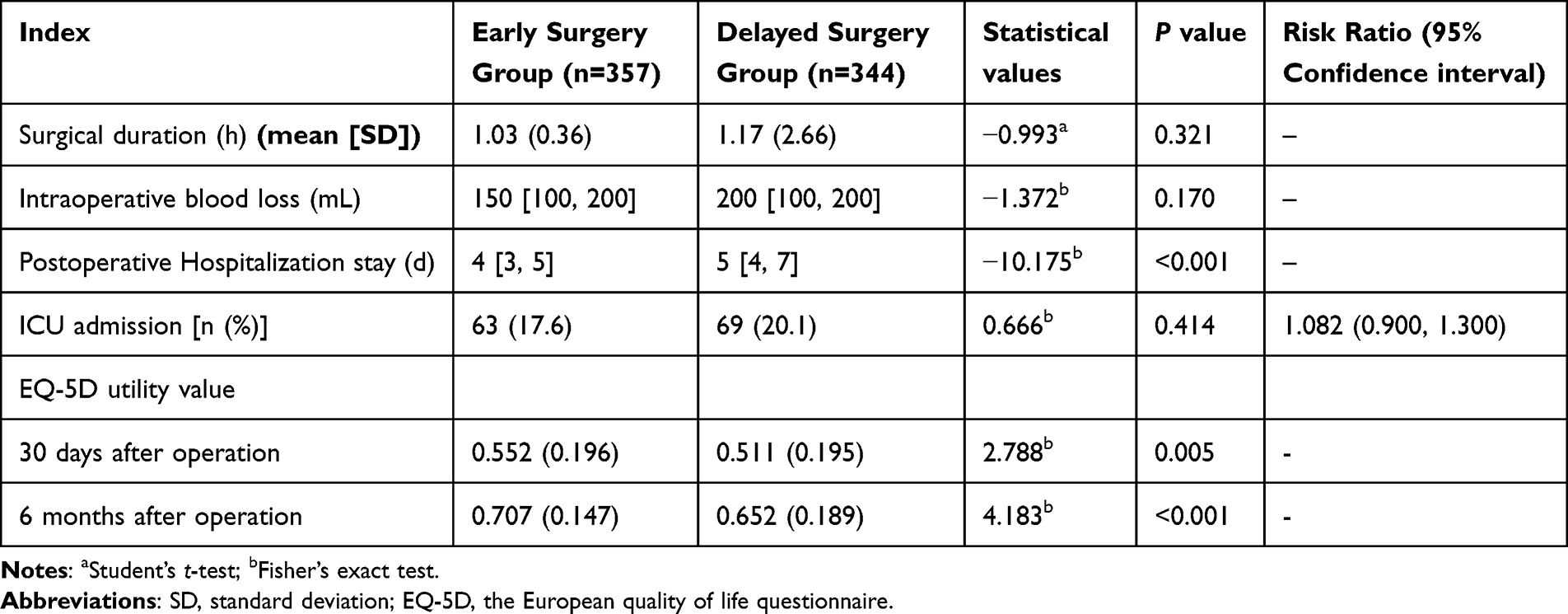 |
Table 2 Comparison of Perioperative Indicators Between the Two Groups |
Complications Within 30 Days After Surgery
The incidence of complications within 30 d after surgery were counted. The results showed that the proportion of pulmonary infections in the early surgery group was significantly lower than that in the delayed surgery group [26 (7.3%) vs 41 (11.9%), P = 0.037]. The incidence of UTIs was 17.6% in the early surgery group and 32.3% in the delayed surgery group, and the difference between the two groups was statistically significant [63 (17.6%) vs 111 (32.3%), P < 0.001]. In addition, the incidence of DVT was significantly lower in the early surgery group compared with the delayed surgery group [27 (7.6%) vs 59 (17.2%), P < 0.001]. The occurrence of other complications, such as cardiovascular events, cerebral infarction, delirium, PE, pressure ulcer, stress ulcer with bleeding, intestinal obstruction and incision infection, were not statistically significantly different between the two groups (Table 3).
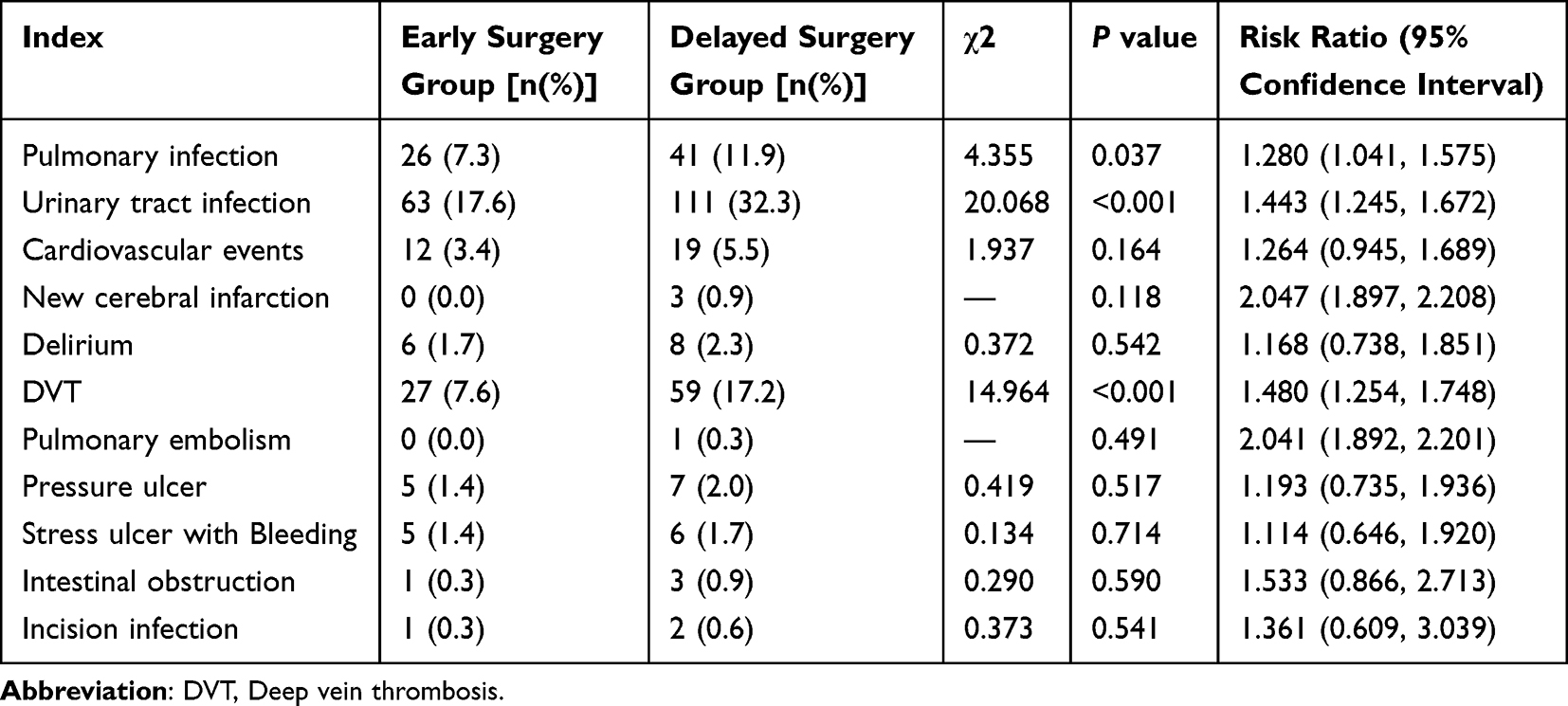 |
Table 3 Complications Within 30d After Surgery Between the Two Groups |
Prognostic Indicators Six Months After Surgery
Six months after surgery, the mortality rate was 5.9% and 6.7% in the two groups, respectively, with no significant difference. The readmission rate in the delayed surgery group was significantly higher than that in the early surgery group six months after surgery, and the difference was statistically significant [34 (9.5%) vs 56 (16.3%), P = 0.008]. According to the HHS, in the early surgery group, there were 288 cases with excellent and good scores and 62 cases with medium and poor scores, and the overall excellent and good rate was 82.3%. In the delayed surgery group, there were 259 cases with excellent and good scores and 78 cases with medium and poor scores, and the overall excellent and good rate was 76.9%. There was no significant difference in the excellent and good rate of HHS between the two groups (Table 4).
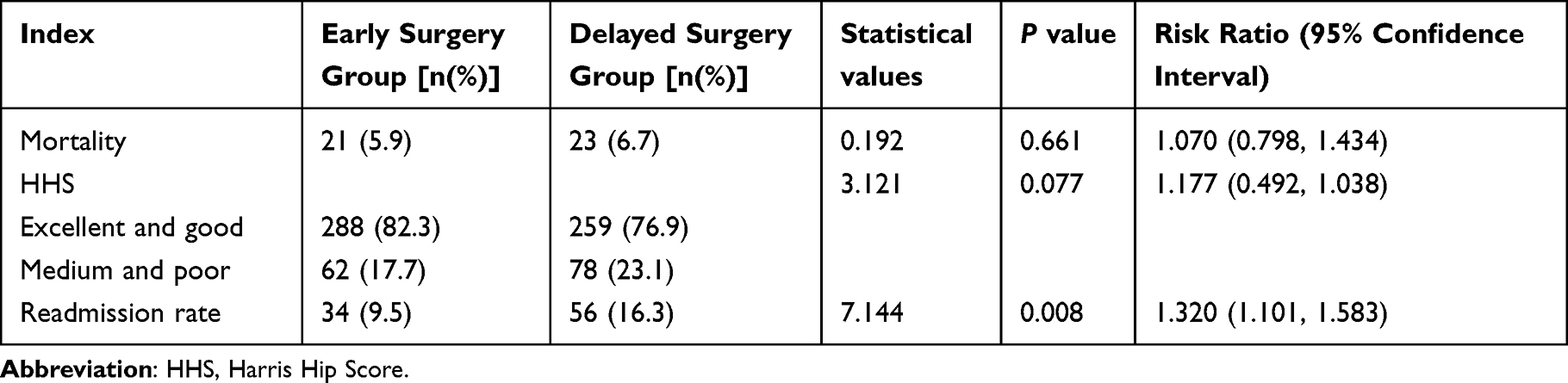 |
Table 4 Mortality, Readmission Rate and HHS Six Months After Surgery |
Complications Within Six Months After Surgery
Six months after surgery, the early surgery was associated with a lower incidence of urinary tract infection (19.6% vs 32.6%, P < 0.001), deep venous thrombosis (9.8% vs 18.3%, P < 0.001), and pressure ulcer (3.4% vs 9.6%, P < 0.001). However, there was no significant difference in the presence of other complications (Table 5).
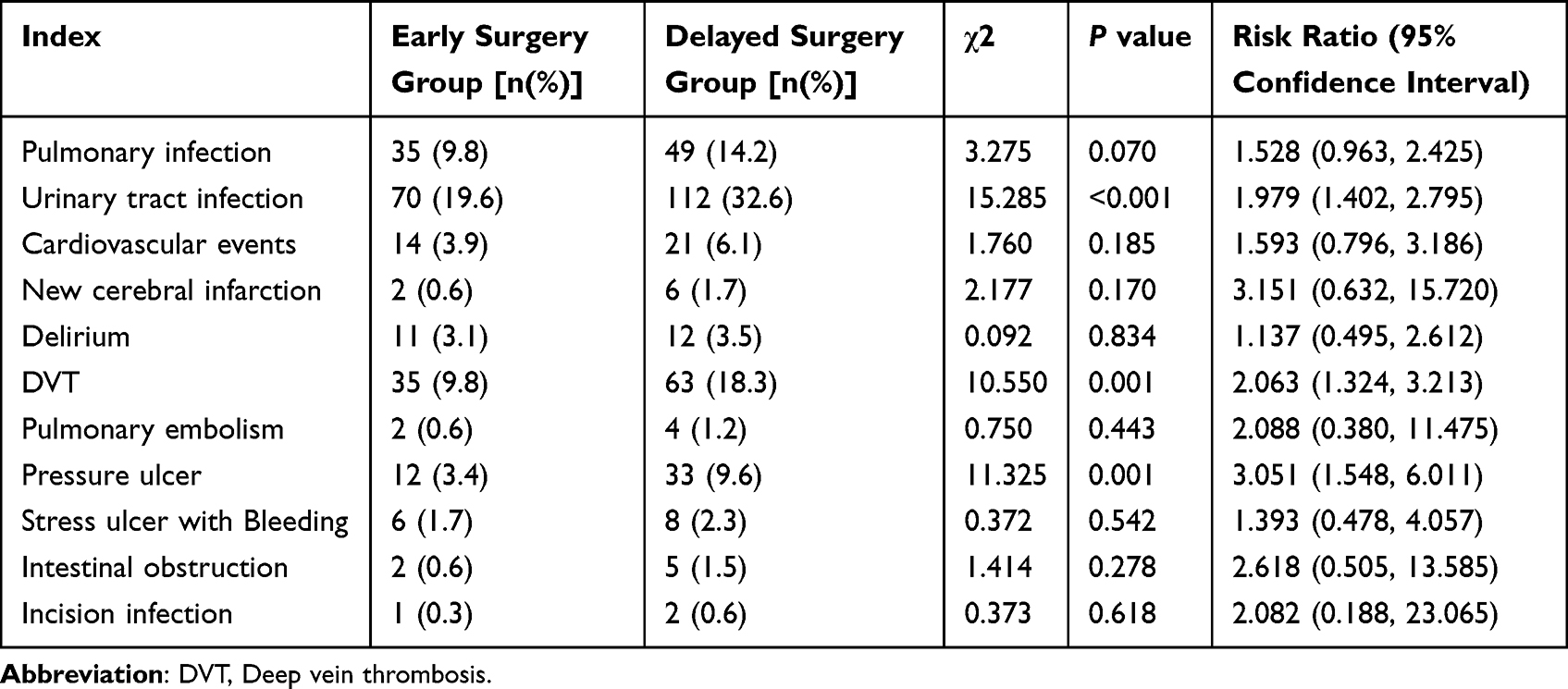 |
Table 5 Complications Within 6 Months After Surgery Between the Two Groups |
Discussion
In this study, we investigated the relationship between the surgical timing and postoperative complications, main outcomes of elderly patients with hip fracture. Compared with the delayed surgery group, the early surgery group significantly reduced the average postoperative hospital stay and the incidence of complications within 30 d after surgery, such as pulmonary infections, UTIs and DVT. In addition, at six months after surgery, although early surgery had no significant effect on patient mortality compared with delayed surgery, early surgery significantly reduced patient rehospitalisation rates.
Hip fractures are one of the deadliest fractures among the elderly. A systematic review concluded that multiple factors, such as age, pre-fracture function, health status, fracture type, pain, anaemia, muscle strength and early activity level, affect the prognoses of patients.16
In this study, it was found that the incidence of pulmonary infection, UTIs and DVT of the lower limbs within 30 d after surgery was lower in the elderly patients with hip fracture who underwent early surgery. There are many potential complications, such as Urinary retention (UR), aspiration pneumonia (AP), dislocation, surgical site infection, fractures around the prosthesis and venous embolism, which can occur after the large-scale application of hip replacement surgery, so an experienced medical staff and a proper medical environment are important determinants for ensuring appropriate prognoses.17–19 Furthermore, the results of previous studies showed that the fewer the days of hospitalisation, the lower the incidence of lung infections, because long-term bed rest could make elderly patients with weakened immune function more susceptible to infections.20,21 The orthogeriatric program succeeded in preventing and treating perioperative complications.22
Pulmonary infections are common postoperative complications in elderly patients with hip fractures.23 Research demonstrates that early surgery can mitigate the risk of pneumonia after surgery,24,25 which is consistent with the results of the present study. According to the analysis, there may be multiple reasons for early surgery to reduce the occurrence of postoperative pulmonary infections. Elderly patients often have a decreased immune capacity. When elderly patients survive for a long time in a highly pathogenic environment like a hospital, the risk of infection is greatly increased. However, early surgery reduces the length of the postoperative hospital stay and avoids prolonged exposure of elderly patients to the highly pathogenic environment of the hospital, thereby reducing the risk of pulmonary infection. Moreover, under stress conditions, such as pain and trauma, various inflammatory factors can be released and induce a systemic inflammatory response. Early surgery can shorten pain continuance, thereby reducing the release of inflammatory factors. Therefore, surgery should be performed at the earliest opportunity to reduce the incidence of postoperative pulmonary infection.
The most common infectious complication in patients with hip fractures is UTI.20 This complication may be related to bed rest, urinary retention, indwelling catheters and other factors. Rodriguez–Fernandez et al26 reported that delayed surgery increases the incidence of UTIs, which is consistent with the results of the present study. Therefore, early surgery is recommended to shorten the bed rest period and reduce the incidence of UTIs.
Additionally, there is also a high incidence of DVT of the lower limbs during the perioperative period for elderly patients with hip fractures.27 This may be related to the following factors: swelling soft tissues around the area of the incision compresses veins, impacting blood flow; bed rest is required after the onset of a fracture; and traumatic stress increases blood viscosity. It has been suggested in some studies27,28 that prolonged preoperative waiting time is one of the most important risk factors for DVT. Therefore, the incidence of DVT for elderly patients with hip fractures can be effectively reduced by conducting early surgery, ending bed rest and implementing early ground activities and functional exercises.
Postoperative complications significantly influence the length of the postoperative hospital stay.28 Studies29 have concluded that early surgery can shorten hospitalisation for patients with hip fractures, which is consistent with the results of the present study. In the present study, patients in the early surgery group have shorter postoperative hospital stay. Therefore, it is proposed that early surgery can shorten the length of the postoperative hospital stay, which would reduce the burden on families and also help conserve limited medical resources.
Postoperative mortality is one of the most important prognostic criteria. There are still controversies regarding the influence of surgical timing on postoperative mortality of elderly patients with hip fractures. According to some studies,30,31 surgical timing is intricately linked to postoperative mortality, which can be reduced by prompt surgery. However, Bretherton et al9 reported that delayed surgery would significantly increase the incidence of postoperative complications but has no influence on the three-month and one-year mortality rate after surgery. A potential reason for this conclusion may be that the sample size was not large enough to show the difference in mortality rates. Some elderly patients have numerous comorbidities, and they lose their mobility after the onset of fractures. Traumatic surgery can induce serious complications, which would require intensive care after surgery. In the present study, the surgical timing was found to exert no influence on the postoperative ICU transfer rate and short-term mortality. This indicates that early surgery should be performed after a thorough assessment. For patients suffering from concomitant diseases and unstable conditions, and for those with high surgical risks, surgery should be delayed appropriately to allow them to actively adjust their state.
The HHS and EQ-5D are an important indicator for evaluating the efficacy of hip joint surgery. In the present study, medical follow-up continued for six months. There was no significant difference in the HHS between the two groups, indicating that surgical timing has little influence on the short-term recovery of hip joint function after surgery. But the EQ-5D utility in the delayed surgery group was significantly lower than that in the early surgery group at 30 days and 6 months after operation. The recovery of hip joint function after surgery may be mainly related to the extent of the fracture, general condition and postoperative rehabilitation exercise, amongst other factors. Moreover, there were no significant differences in the intraoperative blood loss and surgical duration between the two groups, indicating that surgical timing would not affect the surgical course.The results are consistent with previous studies.32,33
This study encountered limitations. First, it was a single-centre retrospective analysis, which may have encompassed selection bias and overlooked some clinically significant data. Therefore, a multicentre, large sample and strictly designed clinical study is required for further exploration. Second, the impact of some other variables on the prognosis of elderly patients, such as the type of fracture, the impact of comorbidities, and differences between genders, were not addressed. Third, the present study was constrained by the available resources and timeframes of the research project, and multivariate analysis was not performed. In future studies, multiple variables should be considered, multivariate analysis implemented, and rigorous clinical studies designed to further investigate the factors affecting the prognosis of elderly patients with hip fractures.
Conclusion
Early surgery is associated with a lower rate of perioperative complications in elderly patients with hip fractures. Early surgery can shorten the length of the postoperative hospitalisation and bed rest for patients and reduce complications such as pulmonary infections, UTIs, and lower extremity DVT associated with bed rest. There were no significant differences between the two groups in terms of mortality and excellent rates of the HHS at six months after the operation.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Beijing Jishuitan Hospital. No identifiable participant information (such as patients’ images, faces, or names) was disclosed in the study.
Acknowledgments
No funding or sponsorship was received for this study or publication of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was available for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang X, Zhao BJ, Su Y. Can we predict postoperative complications in elderly Chinese patients with Hip fractures using the surgical risk calculator? Clin Interv Aging. 2017;12:1515–1520. doi:10.2147/CIA.S142748
2. Wolf M, Bäumer P, Pedro M, et al. Sciatic nerve injury related to Hip replacement surgery: imaging detection by MR neurography despite susceptibility artifacts. PLoS One. 2014;9(2):e89154. doi:10.1371/journal.pone.0089154
3. Bhatti UF, Shah AA, Williams AM, et al. Delay in hip fracture repair in the elderly: a missed opportunity towards achieving better outcomes. J Surg Res. 2021;266:142–147. doi:10.1016/j.jss.2021.03.027
4. Quinn RH, Murray JN. Members of the writing and voting panels of the AUC on the treatment of hip fractures in the elderly and the AUC on postoperative rehabilitation of low energy hip fractures in the elderly. The American Academy of orthopaedic surgeons appropriate use criteria for management of hip fractures in the elderly. J Bone Joint Surg Am. 2016;98(14):1222–1225. doi:10.2106/JBJS.16.00260
5. Moja L, Piatti A, Pecoraro V, et al. Timing matters in Hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175. doi:10.1371/journal.pone.0046175
6. Orosz GM, Magaziner J, Hannan EL, et al. Association of timing of surgery for Hip fracture and patient outcomes. JAMA. 2004;291(14):1738–1743. doi:10.1001/jama.291.14.1738
7. Kostuj T, Smektala R, Schulze-Raestrup U, Müller-Mai C. Einfluss des Operationszeitpunkts und -verfahrens auf Mortalität und Frühkomplikationen der Schenkelhalsfraktur: eine Analyse von 22.566 Fällen der verpflichtenden externen Qualitätssicherung [The influence of timing of surgery on mortality and early complications in femoral neck fractures, by surgical procedure: an analysis of 22,566 cases from the German external quality assurance program]. Unfallchirurg. 2013;116(2):131–137. German. doi:10.1007/s00113-011-2071-1
8. Rai SK, Varma R, Wani SS. Does time of surgery and complication have any correlation in the management of Hip fracture in elderly and can early surgery affect the outcome? Eur J Orthop Surg Traumatol. 2018;28(2):277–282. doi:10.1007/s00590-017-2047-0
9. Bretherton CP, Parker MJ. Early surgery for patients with a fracture of the Hip decreases 30-day mortality. Bone Joint J. 2015;97-B(1):104–108. doi:10.1302/0301-620X.97B1.35041
10. Carretta E, Bochicchio V, Rucci P, Fabbri G, Laus M, Fantini MP. Hip fracture: effectiveness of early surgery to prevent 30-day mortality. Int Orthop. 2011;35(3):419–424. doi:10.1007/s00264-010-1004-x
11. Kostuj T, Smektala R, Schulze-Raestrup U, Müller-Mai C. Pertrochantäre Frakturen. Welchen Einfluss haben Operationszeitpunkt und Implantatwahl auf das Outcome? [Pertrochanteric fractures. What impact do surgical timing and implant choice have on the outcome?]. Unfallchirurg. 2013;116(1):53–60. German. doi:10.1007/s00113-011-2092-9
12. Leslie WD, Brennan SL, Prior HJ, Lix LM, Metge C, Elias B. The contributions of First Nations ethnicity, income, and delays in surgery on mortality post-fracture: a population-based analysis. Osteoporos Int. 2013;24(4):1247–1256. doi:10.1007/s00198-012-2099-2
13. Marsland D, Chadwick C. Prospective study of surgical delay for Hip fractures: impact of an orthogeriatrician and increased trauma capacity. Int Orthop. 2010;34(8):1277–1284. doi:10.1007/s00264-009-0868-0
14. Li N, Song JF, Zhang MZ, Lv XM, Hua HL, Chang YL. Impact of medication therapy management (MTM) service model on multi-morbidity (MMD) patients with hypertension: a pilot RCT. BMC Geriatr. 2023;23(1):10. doi:10.1186/s12877-023-03725-4
15. Luo J, Dong X, Hu J. Effect of nursing intervention via a chatting tool on the rehabilitation of patients after Total Hip Arthroplasty. J Orthop Surg Res. 2019;14(1):417. doi:10.1186/s13018-019-1483-4
16. Kristensen MT. Factors affecting functional prognosis of patients with Hip fracture. Eur J Phys Rehabil Med. 2011;47(2):257–264.
17. Higashikawa T, Shigemoto K, Goshima K, et al. Urinary retention as a postoperative complication associated with functional decline in elderly female patients with femoral neck and trochanteric fractures: a retrospective study of a patient cohort. Medicine. 2019;98(24):e16023. doi:10.1097/MD.0000000000016023
18. Petis S, Howard JL, Lanting BL, Vasarhelyi EM. Surgical approach in primary total Hip arthroplasty: anatomy, technique and clinical outcomes. Can J Surg. 2015;58(2):128–139. doi:10.1503/cjs.007214
19. Higashikawa T, Shigemoto K, Moriyama M, et al. Orthogeriatric co-management at a regional core hospital as a new multidisciplinary approach in Japanese Hip fracture operation. J Orthop Sci. 2022;S0949–S02658(22):314. doi:10.1016/j.jos.2022.11.002
20. Wang JH, Liu SX, Chen YQ, Ning XJ, Wang RR, Zhang YP. Changes of pulmonary infection and serum inflammatory factors in elderly patients after total Hip arthroplasty. Chin J Nosocomiol. 2019;29(09):1396–1399.
21. Lu KQ, Yang LJ, Sun HH, Xu Y, Zhang CY. Analysis of intervention measures for prevention of pulmonary infection after total hip replacement in elderly patients. Chin J Nosocomiol. 2016;26(10):2317–2319.
22. Higashikawa T, Shigemoto K, Goshima K, et al. Risk factors for the development of aspiration pneumonia in elderly patients with femoral neck and trochanteric fractures: a retrospective study of a patient cohort. Medicine. 2020;99(7):e19108. doi:10.1097/MD.0000000000019108
23. Chen J, Wang X, Qian H, Ye J, Qian J, Hua J. Correlation between common postoperative complications of prolonged bed rest and quality of life in hospitalized elderly Hip fracture patients. Ann Palliat Med. 2020;9(3):1125–1133. doi:10.21037/apm-20-891
24. Chechik O, Amar E, Khashan M, Kadar A, Rosenblatt Y, Maman E. In support of early surgery for Hip fractures sustained by elderly patients taking clopidogrel: a retrospective study. Drugs Aging. 2012;29(1):63–68. doi:10.2165/11598490-000000000-00000
25. Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after Hip fracture on mortality and complications: systematic review and meta-analysis. CMAJ. 2010;182(15):1609–1616. doi:10.1503/cmaj.092220
26. Rodriguez-Fernandez P, Adarraga-Cansino D, Carpintero P. Effects of delayed Hip fracture surgery on mortality and morbidity in elderly patients. Clin Orthop Relat Res. 2011;469(11):3218–3221. doi:10.1007/s11999-010-1756-z
27. Zhang BF, Wei X, Huang H, et al. Deep vein thrombosis in bilateral lower extremities after Hip fracture: a retrospective study of 463 patients. Clin Interv Aging. 2018;13:681–689. doi:10.2147/CIA.S161191
28. Van den Belt L, Van Essen P, Heesterbeek PJ, Defoort KC. Predictive factors of length of hospital stay after primary total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015;23(6):1856–1862. doi:10.1007/s00167-014-3313-x
29. Choi HJ, Kim E, Shin YJ, Choi BY, Kim YH, Lim TH. The timing of surgery and mortality in elderly Hip fractures: a retrospective, multicenteric cohort study. Indian J Orthop. 2014;48(6):599–604. doi:10.4103/0019-5413.144232
30. Collin PG, D’Antoni AV, Loukas M, Oskouian RJ, Tubbs RS. Hip fractures in the elderly-: a Clinical Anatomy Review. Clin Anat. 2017;30(1):89–97. doi:10.1002/ca.22779
31. Maheshwari K, Planchard J, You J, et al. Early surgery confers 1-year mortality benefit in hip-fracture patients. J Orthop Trauma. 2018;32(3):105–110. doi:10.1097/BOT.0000000000001043
32. Deutschbein J, Lindner T, Möckel M, et al. Health-related quality of life and associated factors after Hip fracture. Results from a six-month prospective cohort study. PeerJ. 2023;11:e14671. doi:10.7717/peerj.14671
33. Han J, Kim CH, Kim JW. Handgrip strength effectiveness and optimal measurement timing for predicting functional outcomes of a geriatric Hip fracture. Sci Rep. 2022;12(1):20600. doi:10.1038/s41598-022-25177-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.