")
Back to Journals » Cancer Management and Research » Volume 14
The Socioeconomic Impact of Cervical Cancer on Patients in Ethiopia: Evidence from Tikur Anbessa Specialized Hospital
Authors Endale H, Mulugeta T, Habte T
Received 3 December 2021
Accepted for publication 4 April 2022
Published 3 May 2022 Volume 2022:14 Pages 1615—1625
DOI https://doi.org/10.2147/CMAR.S352389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Helen Endale, Tefera Mulugeta, Teshome Habte
Department of Nursing, School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Teshome Habte, Department of Nursing, School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, PO Box: 5657, Addis Ababa, Ethiopia, Tel +251 911436150, Email [email protected]
Background: Cervical cancer is very common among women living in low-resource environments, according to the literature. About 85% of the cases and 88% of the deaths due to cervical cancer occurred in developing countries. Women in low- and middle-income countries have a 35% higher average life risk of cervical cancer than women in high-income countries. However, research on the socioeconomic impact of cervical cancer on patients is virtually absent in the country.
Objective: To assess the socioeconomic impact of cervical cancer on patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia in 2021.
Methods: Institutional based cross-sectional study design was employed. A structured and semi-structured questionnaire was used. The participants were selected using a simple random sampling technique. The collected data was entered and analyzed using the SPSS version 24 statistical software package.
Results: Out of 423 sampled respondents, 416 agreed to participate in the study and the response rate was 98%. The study revealed that cervical cancer has a social impact on patients in terms of social discrimination 61.8%, loss of body image 63%, loss of sexual functioning 78%, and loss of femininity 89%. It has also an economic impact in terms of loss of income of 45.7%, financial distress due to medical and nonmedical expenditures 71%, work and employment challenges 66.8%.
Conclusion and Recommendation: Cervical cancer has an enormous socioeconomic impact on patients in terms of social discrimination, loss of body image, loss of sexual functioning, loss of femininity, loss of income, financial distress, work and employment challenges. Hence, efforts on reduction of social discrimination, psychotherapy support, and financial support are needed to limit the socioeconomic impact of cervical cancer on patients.
Keywords: cervical cancer, social impact, economic impact
Background
Cervical cancer is the fourth most common cancer among women globally, with an estimated 604,000 new cases and 342,000 deaths in 2020. About 90% of the new cases and deaths worldwide in 2020 occurred in low- and middle-income countries.1
In Ethiopia, cervical cancer is the second most common cancer (13.6%) next to breast cancer (32.9%). The annual incidence of cervical cancer is around 6294 new cases and the annual mortality is over 4884. Therefore, given the high incidence, the disease has become a serious health concern in the country.2
Following the increase of prevalence and death caused by cervical cancer, patients have to deal with increased treatment-related expenses, loss of employment and consequent income, and changes in household responsibilities. Moreover, cervical cancer disproportionately affects women in the low socioeconomic level, and thus the disease can have dramatic consequences for the living conditions of patients, including falling into poverty or being pushed into deeper poverty.3 Cervical cancer is preventable primarily through prophylactic HPV vaccination and screening for precancerous lesions are in some instance currently practicing, but still it is a public health concern due to scarcity of resource and not widely implementing it for all women of child bearing age.1,3
Cervical cancer affects women in the time that they are critical to economic and social stability. It enforces them to reduce their work productivity while theyincur overwhelming medical costs. It also left women burdened by infertility, negative body image, and feeling flawed as a woman, and sexually undesirable. Moreover, in Ethiopia around 80% of cancer cases are already diagnosed when the case becomes worse, which make the treatment more costly and less successful, which aggravates cervical cancer to an enormous socioeconomic burden on patients.4
The economic impact of cervical cancer in the developing countries like Ethiopia highly affects the quality of life, due to medical and nonmedical costs incurred upon the individual over the course of the disease. Medical costs mainly include cost of medicine, laboratory test, and hospital admission charges. While the nonmedical costs are related with cost of travel, accommodation and other out of pocket expenses over the course of treatment.5 In addition, it has also an economic impact in terms of reduction of work hours, work interruption, work stop, loss of income, sale of property, and use of past savings.6 Furthermore, the financial impact of cervical cancer is much worse for patients in a developing country than the developed one as there is no well-established insurance system in these countries.7
Alternatively, cervical cancer has also an adverse social impact on patients. In this regard, prolonged cancer hospitalization usually alienates cancer patients from their social relationships.8 Moreover, its treatment affects a patient’s body image and sexual functioning, which negatively affects their intimate relationship and quality of sex life. Cervical cancer patients also experienced social discrimination as it is often associated a shameful disease from evil spirit and contagious. It is also a cause for loss of fertility which is particularly distressing for the women and affects their marriage and intimate relationship.9
Therefore, given the fact that cervical cancer has become a serious health problem in Ethiopia, it is expected that it has an enormous socioeconomic impact on patients. However, research conducted in Ethiopia on cervical cancer has not addressed this issue of interest, rather they focus mainly on the issue related with prevention, screening, awareness, knowledge, and attitude. Hence, to the best of the researchers' knowledge, no other study is conducted on the socioeconomic impact of cervical cancer on patients in Ethiopia so far. Therefore, the purpose of this study is to assess the socio-economic impact of cervical cancer on patients at Tikur Anbessa specialized hospital.
Methods
Study Design
Institution based cross-sectional study design was employed and the data were collected during the period from March 1–30, 2021 G.C.
Study Setting
The study was carried out in Tikur Anbessa Specialized Hospital (TASH) which is located in the capital city of Ethiopia. It provides a tertiary level referral treatment and it is the largest central referral hospital that has an oncology ward. It is also the only institute that provides radiotherapy treatments for cancer patients in Ethiopia.
Sample Size Determination and Sampling Procedure
The sample size for this study has been determined using a single population proportion formula. Hence, the final sample size obtained including 10% nonresponse rate was 423.
Eligibility Criteria
All women attended cervical cancer screening and whose had at least two or more follow-ups were included in the study and those patients critically sick and unable to communicate to provide information during the data collection period were excluded from the study.
Study Instrument
Data was collected from cervical cancer patients who attend the oncology unit of TASH using structured and semi-structured questionnaires which were translated into Amharic from its English version. The instrument consists of two parts which were sociodemographic variables and socioeconomic variables that show the impact of cervical cancer on patients.3,4,6,9 The questionnaires were translated from English to Amharic and back translated to English to conform the accuracy of the Amharic version before using for data collection.
Operational Definition
- Social impact: was defined or measured in terms of social discrimination, loss of body image, loss of sexual functioning and loss of femininity, as reported by the patients (self-report). Hence, patients were asked to reply a fixed choice answer of “Yes” or” No” on each social impact indicator variables.
- Economic impact: was defined or measured in terms of loss of income, financial challenge, work and employment challenge, as perceived by the patients (self-report). Hence, patients were asked to reply a fixed choice answer of “Yes” or” No” on each economic impact indicator variables.5,6,9
Data Analysis
The collected data was verified to ensure completeness and then coded, entered in an Excel (Microsoft Corporation) spread sheet. The data was analyzed with the help of SPSS version 24 statistical software package. Descriptive statistics such as frequency, percentages and mean were used to describe the result of the study. Bivariate and multivariate logistic regression was done to evaluate the association between independent versus outcome variable. In bivariate analysis, variables that have a P-value of less than 0.25 was included in multivariable analysis where variables that have P-value of less than 0.05 was used to determine level of statistical significance.
Data Quality Assurance
To ensure the validity and reliability of the data collection tool, pretest was done on 5% of the total sample size calculated two weeks before the actual data collection period held at Saint Paul's Referral Hospital and the questionnaire had been checked for its clarity, understand ability and simplicity. Respondents who were involved during the pretest were not included in the main study. After pretest, the questionnaires were reviewed and reformatted based on the obtained inputs and comments. The completed questionnaire was presented to the principal investigator and checked for its completeness and comprehensiveness to assure the quality of data. The principal investigator had been responsible for supportive supervision on the spot and on reviewing all completed questionnaires on a daily basis. Moreover, training was also given to data collectors to assure the quality of data.
Results
The Sociodemographic Characteristics
A total of 423 questionnaires were distributed among the study participants and 416 responded with response rate of 98%. Majority of the respondents (55.1%) were belonging to the age group of 30–50 years and most of the respondents (40.8%) were orthodox Christian. Regarding educational status, 32% of the women cannot read and write, whereas 26% had completed elementary school, and 23% had completed high school. As shown in Table 1, the majority of the respondents belong to urban areas (63%) and 47.1% were married. Most of the patients (64.7%) were found with late stage of the disease and about 50% of the respondents were employed. The treatment modality of the patients indicated that 31% of the respondents did not start cervical cancer treatment while 69% of the respondent took different types of treatments.
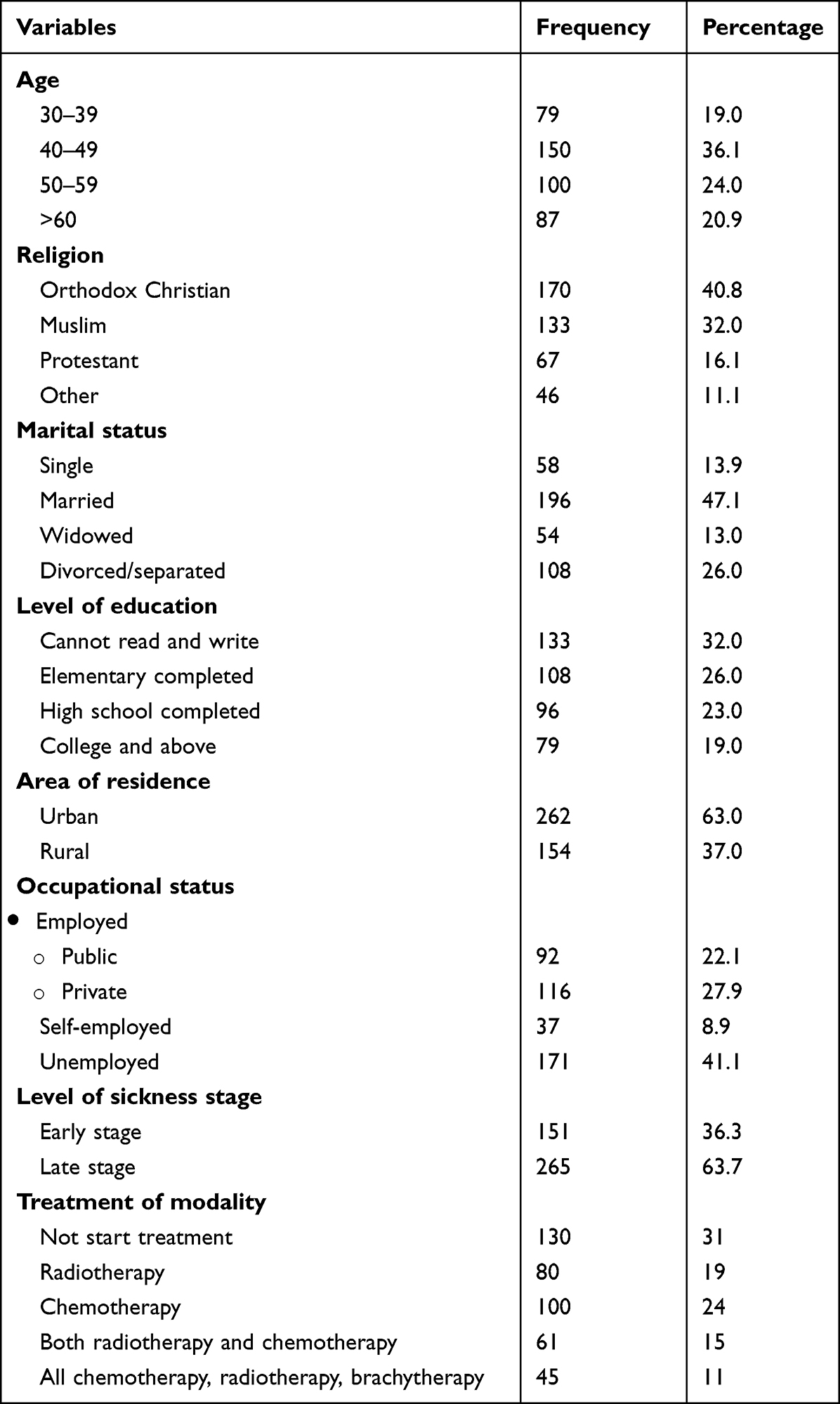 |
Table 1 Sociodemographic Characteristics of Cervical Cancer Patients at TASH, Addis Ababa, Ethiopia, March 2021 (n=416) |
Social Impact of Cervical Cancer
Social Discrimination
Majority of the respondents 256 (61.5%) revealed that they had experienced social discrimination as a result of cervical cancer while the rest 160 (38.5%) did not face social discrimination. Regarding the source of social discrimination, it mainly comes from their neighbor 167 (65%) and followed by community 146 (56.8%), close friends 131 (51%) and husband/partner 64 (24.9%). In addition to social discrimination, the result of the study also revealed that 279 (67%) of cervical cancer patient had made self-stigmatization due to bad smell of vaginal discharge 193 (69.2%) followed by cervical cancer made them feel alone 151 (54.1%), rejection by family, spouse and neighbors 131 (47%), think people do not understand them 98 (35.1%) and prolonged cancer hospitalization 70 (25.1%).
Loss of Sexual Functioning
Of the 416 respondents, 324 (78%) of the respondent mentioned that cervical cancer has a negative impact on their sexual functioning and intimate relationship while the rest 92 (22%) had not noticed its impact. This is due to, loss sexual desire 224 (69%), loss of physical strength 139 (43%), fear of sex worsened the condition 175 (54.1%), fear of pain during intercourse 230 (70.9%), loss of wholeness 214 (66.1%), loss of potential marriage opportunity 143 (44%), fear and doubt to start new relationship 126 (38.9%), make them not have sexual partner 123 (38%).
Loss of Body Image
About 262 (63%) of cervical cancer patients stated that cervical cancer treatment negatively affected their body image in terms of hair loss 220 (83.9%), feel disfigured 192 (73.1%), cannot regain the physical strength that they once had 118 (45%), decrease the attractiveness of their body 183 (70%), feeling old 131 (50%). Moreover, it also make to worry or lose confidence about their body 102 (38.9%) which in turn enforced them to use artificial hair and wear clothing to cover their body 154 (58.9%).
Loss of Femininity
Among 212 respondents who had faced infertility problems, many of them 189 (89%) reported that they lost their femininity or womanhood due to infertility. In this regard, the majority of the respondents 161 (85%) thought that fertility is a key element that made them a woman and 113 (60%) of the respondents was also thought that the culture of their society shall attest femininity via fertility.
Economic Impact of Cervical Cancer
Financial Challenge
As depicted in Figure 1, the majority of the patients (295, 71%) had faced extensive financial distress due medical and nonmedical expenditures of cervical cancer treatments while the rest (121, 29%) of the respondents reported that their expenditure is the same prior to the onset of the illness. Due to the increment of medical and nonmedical cost of cervical cancer, it forced patients to borrow money (75%), sell an asset (59.9%), use past saving (32%) and mortgage asset (35.1%). It was also quite heartening to note that only 5% of the respondents got support from an NGO.
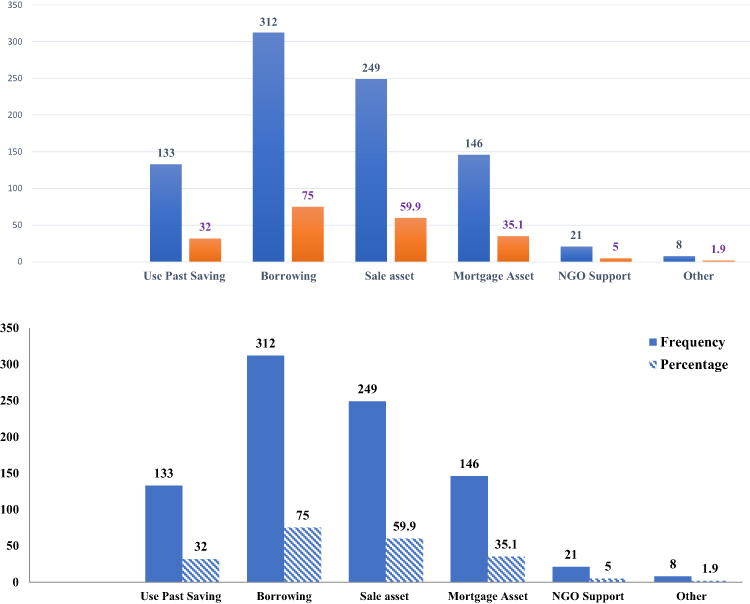 |
Figure 1 Source of financing for medical and nonmedical expenditures of cervical cancer patients at TASH, Addis Ababa, Ethiopia, March 2021. |
Work and Employment Challenge
Among the total of 208 employed cervical cancer patients who worked in public and private sectors, 66.8% of them reported that cervical cancer had affected their work and employment status. This is due to the illness make to reduce work hours (53%) and stop work (41%). Moreover, due to cervical cancer illness, 27.8% of the respondent had been forced to change their job on average once in six months.
Loss of Income
About 112 (45.7%) of the total employed respondents lost their monthly income while the rest 133 (54.3%) of the respondent did not lose their income. Regarding the amount of monthly income loss by the respondents, it was reported that the average monthly loss is Ethiopian birr (ETB) 2100 while in some case it varies with average of ETB1200 to ETB14,000.
Factors Associated with Socioeconomic Impact of Cervical Cancer
Cervical cancer patients who lived in a rural area had encountered higher social discrimination (1.9 times) compared to a study done with patients living in an urban area. In addition, women with cervical cancer who were unemployed had encountered higher social discrimination (1.2 times) compared to patients who were unemployed. And also, cervical cancer patients who were at late stage of the disease had encountered higher social discrimination, higher loss of sexual functioning, higher loss of body image, higher loss of femininity compared to patients at early stage of the disease as shown in Table 2. Further, patients who took any cervical cancer treatment had encountered higher social discrimination, loss of sexual functioning, loss of body image, loss of femininity compared to patients who did not start the treatment.
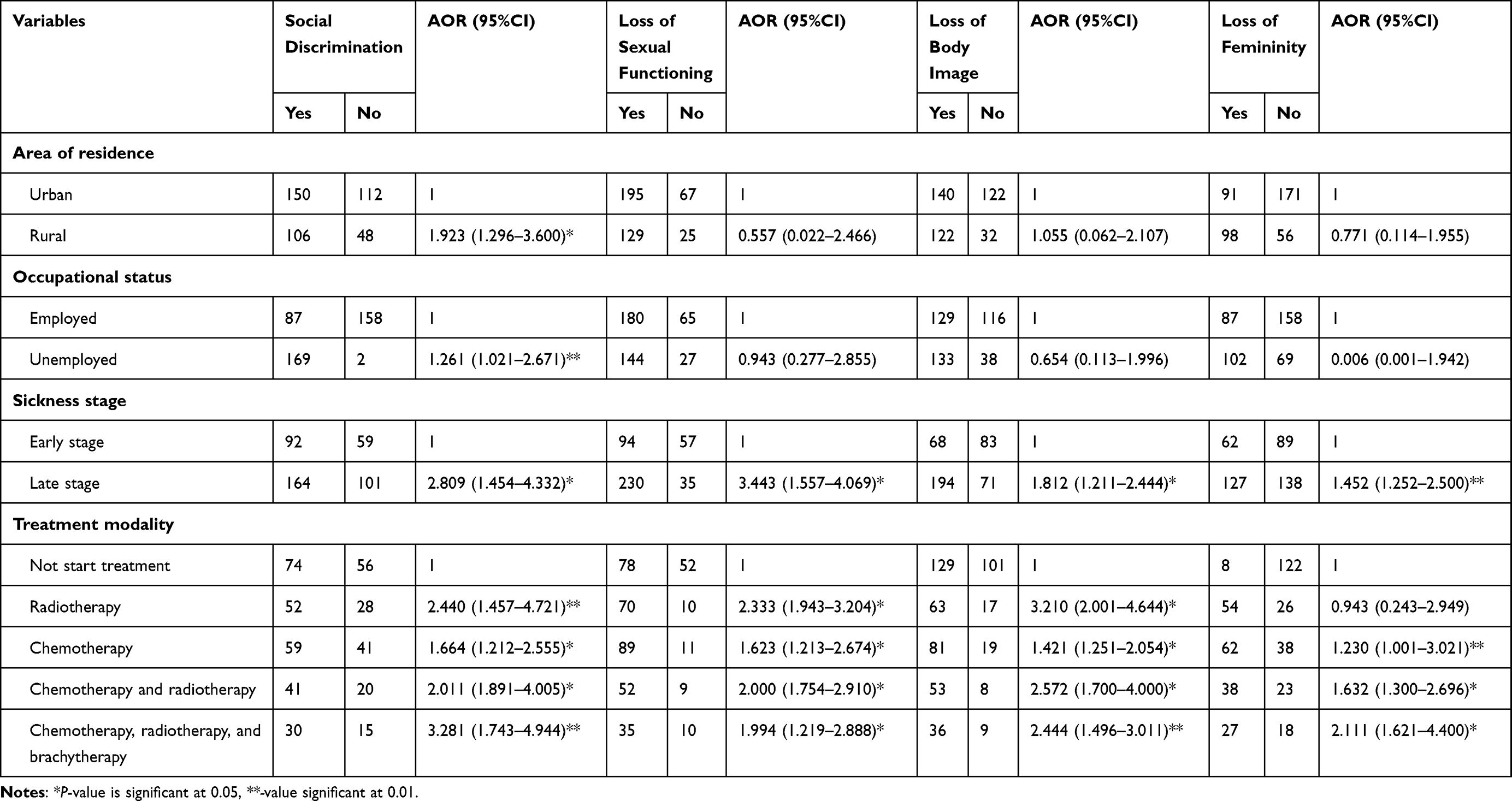 |
Table 2 Results of Multivariable Logistic Regression Analysis for the Outcome Variable “Social Impact Indicators” of Cervical Cancer at TASH, 2021 |
From an economic impact point of view, as shown in Table 3, cervical cancer patients who lived in a rural area had faced higher financial challenges (2.5 times) and higher loss of income (1.3 times) compared to patients who live in an urban area. Compared to patients at early stage of the disease, patients at late stage of the disease had encountered higher financial challenges (1.6 times more). And also, patients at late stage of the disease had encountered higher loss of income compared to patients at early stage. Cervical cancer patients who lived in a rural area had encountered less work and employment challenges (0.6 times less) as compared to patients who lived in an urban area. Moreover, cervical cancer patients who were at late stage of the disease had encountered higher work and employment challenges (3.6 times) compared to patients at early stage of the disease. Furthermore, those patients who start any type of treatment had encountered higher financial challenges, loss of income, work and employment challenges compared to patients at who did not start the treatment.
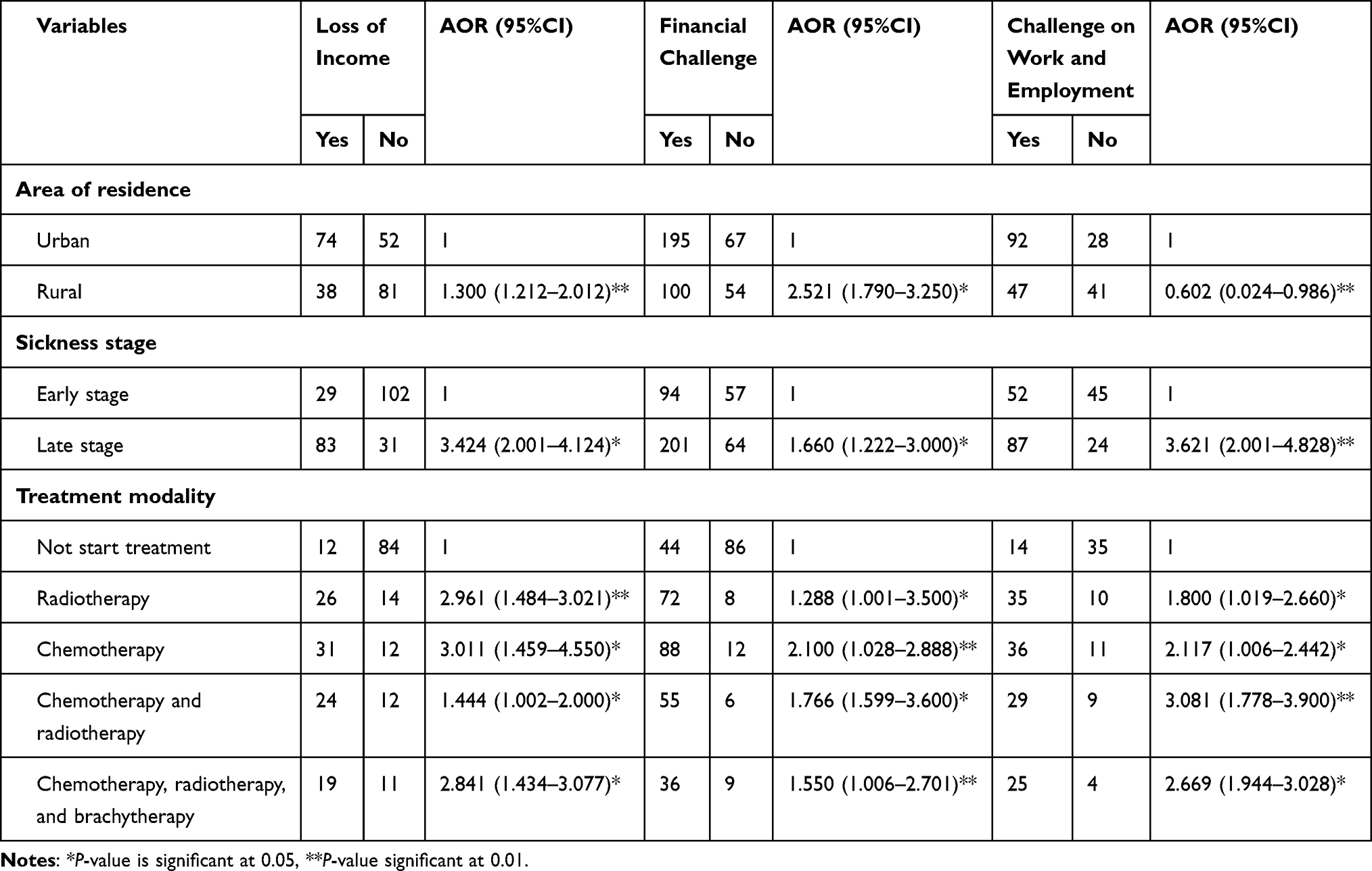 |
Table 3 Results of Multivariable Logistic Regression Analysis for the Outcome Variable “Economic Impact Indicator” of Cervical Cancer at TASH, 2021 |
Discussion
This study assessed the socioeconomic impact of cervical cancer on patients in Ethiopia. In line with this, the social impact was analyzed based on social impact indicator variables. Accordingly, the study revealed that 61.8% of the patients had faced social discrimination which is mainly from their neighbor (65%), community (56.8%), close friends (51%) and husband (24.9%). This finding is consistent with the earlier study conducted in Brazil where 53.2% of cervical cancer patients had faced social discrimination mainly by their neighbor (39%) and friends (30%) which is slightly less than the current study finding.9 This could be attributed the fact that the awareness and level of education about cervical cancer was by far better in Brazil than in Ethiopia.
This study showed that cervical cancer has a negative impact on sexual functioning of patient as reported by 78% of the respondents, which is mainly through loss of sexual desire (69%), loss of physical strength (43%), fear of relapsing (54.1%), fear of pain during intercourse (70.9%) and loss of wholeness (66.1%). This result is consistent with the studies conducted in Ireland,10 Japan,11 and USA12 where cervical cancer negatively affect the sexual functioning of 63%, 53%, and 69% of the patients, respectively. A study conducted in Croatia also found similar results to this study.13
This study revealed that cervical cancer has a negative impact on body image of patients as reported by 63% of the respondents. This study finding is lower to that reported by Irene et al (67%) in Singapore14 and Izycki et al (59%) in Poland15 but higher than that reported by Khalil et al (35%) in Morocco.6 Moreover, this study also indicated that the negative impact of cervical cancer on body image took place through hair loss (83.9%), feeling disfigured (73.1%), loss of physical strength (45%), decrease the attractiveness of the body (70%) and feeling old (50%).
In present study 51% of the patients had faced the problem of infertility due to cervical cancer treatment, which also makes 89% of them lose their femininity or womanhood. This is congruent with the studies conducted in Iran16 and Germany17 where 37% and 45% of the patients had faced loss of femininity, respectively. It is also consistent with the study conducted in USA where 70% of the patients reported that they faced loss of femininity due to cervical cancer treatment.18
Regarding the economic impact of cervical cancer on patients, it was also analyzed based on different economic impact indicator variables. Accordingly, this study found that the majority of the patients (71%) had faced extensive financial distress due medical and nonmedical expenditures of cervical cancer treatments. This finding is consistent with the study conducted in Sub-Saharan Africa where 64% of the patients had faced financial challenges due to cervical cancer.19 Previous studies in Kenya,20 and China21 correspond with this study.
The study revealed that cervical cancer patients were not in a position to finance their medical and nonmedical expenditure which forced them to borrow money (75%), sell an asset (59.9%), use past saving (32%), mortgage an asset (35.1%), get support from an NGO (5%). This finding is congruent with the study conducted in China where patients were forced to sell their assets (27%), take loans (22%), use past savings (34%) due to cervical cancer21 Moreover, a study conducted in Kenya had the same result with this study where patients were forced to use past savings (23.8%), borrowing (22.4%), and sell assets (15%).8
In the present study 66.8% of the employed patients had faced work and employment challenges due to cervical cancer. In this regard, the illness forced 53% of the patients to reduce work hours and 41% of the patients to stop work. This is congruent with the study conducted in Brazil where 15.38% of cervical cancer patients had quit their job due to cervical cancer.9 It is also consistent with the studies conducted in USA22 and South Africa23 where 59% and 60% of cervical cancer patients abandoned their work due to cervical cancer.
In the present study cervical cancer patients who lived in a rural area had encountered higher social discrimination, financial challenge and loss of income compared to patients who lived in an urban area. This might be due to the fact that there is low awareness in rural communities about the disease and they even consider the disease as an evil spirit or a result of curse of God. Alternatively, the rural community mainly focus on agricultural activity and their economic diversification is limited, which makes their source of income inadequate. Moreover, the nonmedical cost for rural patients is likely higher as they travel longer distances in search of medical service than the urban patient.
This study also revealed that cervical cancer patients who were at late stage of the disease had encountered higher social discrimination, financial challenge, loss of income, work and employment challenges compared to patients who were at an early stage of the disease. Probable reasons could be that patients at late stage could not play a significant role in society and could not participate in social gatherings. Moreover, late-stage patients could face high burden of medical costs as they came to health facilities after the advanced stage of the disease. Moreover, late-stage patients may not be effective and productive in their work area because of the illness.
Regarding modality of treatment, cervical cancer patients who took any type of treatment (chemotherapy, radiotherapy and brachytherapy) had encountered higher social and economic impact compared to patients who did not start the treatment.
Limitations of the Study
This study is conducted a single institution and not community-based study, the selected study subjects were women who visited the Tikur Anbessa Specialized Hospital for the study on socioeconomic impact of cervical cancer patients because of suspecting themselves attended hospital for screening which may lead to selection bias and the impact of the problem is higher than the general population. Another community-based large-scale study is recommended.
Conclusion and Recommendations
Conclusion
- This study indicates that most of cervical cancer patients had faced social discrimination which is mainly from their neighbors, community, close friends and husband while (69.2%) had made self-stigmatization because of bad smell of vaginal discharge, felt alone, rejection by others, and prolonged cancer hospitalization.
- Cervical cancer alters the physiological condition of the reproductive system as a result of metabolic change and self-image disturbance.
- Half of cervical cancer patients had infertility problems due to lose of their femininity and also most study participants have financial constraints due to the high cost of medical service.
- This study indicates that for patients with cervical cancer employment is very poor, even after being employed they were forced to resign due to pathological process of the disease (severity of their illness).
- Patients who lived in a rural area have higher financial challenges and social discrimination compared to patients who lived in an urban area and late stage of the disease worsen the social and financial problems.
Recommendations
On the basis of the findings of this study, the following recommendations are proposed:
- Enhance awareness of the society about the disease to reduce the social discrimination faced by cervical cancer patients.
- Health professionals need to provide psychotherapy treatment to patients and facilitate body image acceptance program that help patients to have a positive feeling about their current body image and avoid body appearance related distress.
- In order to improve the mental wellbeing of patients about their loss of femininity, health professionals need to provide advice and psychotherapy treatment for them.
- The government need to strengthen the support provided to cervical cancer patients in the form of subsidy and free treatment cost.
- Strengthen and design a strong policy that enables a health insurance scheme is implemented in the country to reduce the financial challenge that emanates from cervical cancer treatment.
- To reduce the work and employment challenge faced by cervical cancer patients, employers need to support patients by providing activities that are not stressful and physically challenging jobs.
- Enhance the availability of health-care facilities in rural parts of the country to reduce the nonmedical related cost of cervical cancer treatment.
- Researchers should conduct further studies regarding ways to reduce the negative socioeconomic impact of cervical cancer on patients.
Abbreviations
TASH, Tikur Anbessa Specialized Hospital; SPSS, Statistical Package for Social Science; AOR, adjusted odds ratio; MSC, Master of Science; RN, registered nurse; USA, United States of America.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
In line with the work experience of Department of Nursing and Midwifery, College of Health Sciences, Addis Ababa University, ethical approval and clearance were obtained from the respective Ethical Review Board and this study was passed through this channel. The study participants were described about the purpose of this study and then, verbal and written informed consent were obtained from each study participants. The collected data was checked for completeness, coded and entered in to application software for analysis. All steps of the research project process were undertaken in line with the Declaration of Helsinki (1964) guideline.
Acknowledgments
This study was conducted in collaboration with Addis Ababa University. Every step of the project was followed by Addis Ababa University, College of Health Sciences, School of Nursing and Midwifery. The university had no role in designing, analysis and writing of the study. The authors did not receive any financial support from any organization.
This article was prepared for publication directly derived from an upublished original thesis.24 We would like to extend our sincere gratitude to the data collectors, supervisors and the study participants for being involved in the study.
Author Contributions
All authors approved the manuscript for submission, made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors contributed sufficiently to the project to be included as authors and are qualified to be authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. Terefu T, Mesfin K, Gemechu K, Tagel G. Magnitude and factors associated with pre cervical cancer among screened women in Southern Ethiopia. Adv Public Health. 2019;2019:1–8.
3. World Health Organization. Accelerating cervical cancer elimination report by the director –general; 2018.
4. Zenebu B, Ramila B. Exploring barriers in health care delivery system for cancer care in Ethiopia. College of medicine and health sciences, Ambo University, Ethiopia. Int j Health Sci. 2018;8:132–142.
5. Mulugeta M, Kebede E, Mulualem E, et al. Prevalence of cervical cancer and associated factors among women attended cervical cancer screening center at Gahandi Memorial Hospital, Ethiopia. Cancer Inform. 2021;20:1–6. doi:10.1177/11769351211068431
6. Khalil J, Bellefqih S, Sahli N, Afif M, Elkacemi H. Impact of cervical cancer on quality of life: beyond the short term. Gynecol Oncol Res Pract. 2015;2 (1):1–6.
7. Wondemagegnhu T, Werissaw H, Tefera M, Mirgissa K, Wajana LL. The situation of cancer treatment in Ethiopia: challenges and opportunities. J Cancer Prev. 2019;24 (1):33.
8. Mutuma J, Wakhungu C, Mutai J. Socio economic effect of cancer on patients’ livelihoods in Kenyan house hold. Centre for disaster management and humanitarian assistance, Masinde Muliro University of Science and Technology. Bibechana. 2016;14:37–47.
9. Novaes HMD, Itria A, Silva GA, Sartori AMC, Rama CH, Soárez PC. Annual national direct and indirect cost estimates of the prevention and treatment of cervical cancer in Brazil. Clinics. 2015;70 (4):289–295. doi:10.6061/clinics/2015(04)12
10. Gilbert E, Ussher JM, Perz J. Sexuality after gynaecological cancer: a review of the material, intrapsychic, and discursive aspects of treatment on women’s sexual-wellbeing. Maturitas. 2017;70:42–57. doi:10.1016/j.maturitas.2011.06.013
11. Kamijo Y, Ichikawa M. Cost information of chemotherapy for cervical and endometrial cancer in Japan. Jpn J Nurs Sci. 2014;11:190–199. doi:10.1111/jjns.12020
12. Christina M, Deborah B, Beth L, Sarah M. Body image, sexuality, and sexual functioning in women with gynaecologic cancer: an integrative review of the literature and implications for research. Cancer Nurs. 2021;44 (5):1–17.
13. Bukovic D, Silovski H, Silovski T. Sexual functioning and body image of patients treated for ovarian cancer. Sex Disabil. 2018;26:63–73. doi:10.1007/s11195-008-9074-z
14. Irene T, Yin Bun C, Timothy Y, Rama P, Victoria L, Komal T. The relationship between symptom prevalence, body image, and quality of life in Asian gynaecologic cancer patients. Psycho-Oncol. 2018;27 (1):69–74.
15. Iżycki D, Woźniak K, Iżycka N. Consequences of gynaecological cancer in patients and their partners from the sexual and psychological perspective. Przegl Menopauz. 2016;15 (2):112–116.
16. Bakhtiyar K, Beiranvand R, Ardalan A, et al. An investigation of the effects of infertility on Women’s quality of life: a case-control. BMC Women’s Health. 2019;19:114. doi:10.1186/s12905-019-0805-3
17. Slade P. Sexual attitudes and social role orientations in infertile women. J Psychosom Res. 2019;25 (3):183–186. doi:10.1016/0022-3999(81)90031-3
18. Torre LA, Islami F, Siegel RL, et al. Global cancer in women: burden and trends. Cancer Epidemiol Biomark Prev. 2017;26:444–457. doi:10.1158/1055-9965.EPI-16-0858
19. Aniebue UU, Onyeka TC. Ethical, socioeconomic, and cultural considerations in gynecologic cancer care in developing countries. Int J Palliat Care. 2014;2014:1–31. doi:10.1155/2014/141627
20. Jane A, Owenga J, Nyambedha E. Perception of cervical cancer patients on their financial challenges in Western Kenya. BMC Health Serv Res. 2018;1–17. doi:10.1186/s12913-017-2770-6
21. Qianhui W, Manman J, Hongmin C, et al. The economic burden of cervical cancer from diagnosis to one year after final discharge in Henan Province, China: a retrospective case series study. PloS One. 2020;15 (5):1371–1389.
22. Byers TE. The impact of socioeconomic status on survival after cancer in the United States: findings from the National Program of Cancer Registries Patterns of Care Study. Cancer. 2014;113 (3):582–591. doi:10.1016/j.anai.2014.09.013
23. Cebisile N, Ellinor O, Themba G. The economic burden of cervical cancer in Eswatini: societal perspective. PLoS One. 2021;16 (4):e0250113.
24. Endale H, Mulugeta T, Habte T. The socio -economic impact of cervical cancer on patients in Ethiopia: evidence from Tikur Anbessa Specialized Hospital; 2021.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.