")
Back to Journals » Open Access Emergency Medicine » Volume 12
The Safety of Early Thromboembolic Prophylaxis in Closed Traumatic Intracranial Hemorrhage
Authors Jamous MA
Received 25 November 2019
Accepted for publication 25 March 2020
Published 14 April 2020 Volume 2020:12 Pages 81—85
DOI https://doi.org/10.2147/OAEM.S239881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Mohammad Ahmad Jamous
Department of Neurosurgery, King Abdulla University Hospital, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Mohammad Ahmad Jamous
Department of Neurosurgery, King Abdulla University Hospital, Faculty of Medicine, Jordan University of Science and Technology, PO Box 3030, Irbid Tel +962 79 9773827
Email [email protected]
Background: Venous thromboembolism (VTE) is a major cause of morbidity and mortality in patients with traumatic brain injury (TBI); this study is testing the safety of enoxaparin use for the prevention of venous thromboembolism in this group of patients.
Patients and Methods: From January 2016 to May 2018, 46 patients (36 males, 10 females) with closed traumatic intracranial bleeding received early (ie, within 72 hours) venous thromboembolic prophylaxis with 40 mg of enoxaparin. Patients with traumatic intracranial hemorrhage were followed up both clinically and with repeated brain computed tomography to examine the safety of enoxaparin VTE prophylaxis.
Results: The age of the patients ranged from 16– 91 years (43.9± 25.8 years). Glasgow coma score ranged from 5– 15 (9.9± 4.7). Twenty patients had mild TBI (GCS 15– 13), 17 patients had moderate TBI (GCS 12– 9), and nine patients had severe TBI (GCS≤ 8). Brain computed tomography showed variable types of brain injuries. Non-surgical management was applied for 18 patients. Craniotomy and surgical evacuation of significant (≥ 1cm in maximum diameter) EDH and/or SDH was carried out in 26 patients. External ventricular drain was inserted in two patients with significant IVH. Thirty-eight patients had good overall outcome, eight patients showed poor outcome. None of the reviewed patients developed clinical deterioration and/or progression of the intracranial bleeding on follow-up brain CT scans.
Conclusion: Enoxaparin is a safe prophylaxis against venous thromboembolism in patients with traumatic closed intracranial bleeding.
Keywords: head injury, traumatic brain injury, intracranial hemorrhage, DVT prophylaxis, enoxaparin, pharmacologic thrombosis prophylaxis
Introduction
Major injury substantially increases the risk of venous thromboembolism (VTE). The incidence of DVT in multiply-injured patients ranges from 6–60%, even with the use of prophylactic measures such as pneumatic compression devices.1,2 Major trauma causes a significant increase in the markers for thrombin generation with disruptions of its regulation which, in turn, causes a hypercoagulability state. These changes occur within 24 hours after injury, remain markedly elevated for the next 5 days, and decrease by day 14 post-injury.3
Traumatic brain injury (TBI) was recognized as an independent risk factor for deep venous thrombosis (DVT), it increases the chance of venous thromboembolism by 3–4-fold.4 Praeger et al5 studied the prevalence of VTE following TBI prospectively by doing Doppler ultrasound twice weekly in isolated TBI patients, 36% of TBI patients developed venous thromboembolism. In a retrospective study, Ekeh et al6 found that 31% of patients with moderate or severe TBI developed VTE. Multiple injuries, old age, male gender, comorbidities, craniotomies, SAH, and lower limbs injury were identified as risk factors for the occurrence of VTE in patients with TBI.6,7 The use of hypertonic saline and osmotic diuresis was also identified as a risk factor for the development of VTE in TBI patients.8
The occurrence of VTE in TBI was associated with an increased mortality rate and delayed recovery;7,9,10 therefore VTE prophylaxis is essential in these critically ill patients. Low molecular weight heparin (enoxaparin) was reported to be very effective in preventing the occurrence of VTE in TBI patients; however the increasing risk of intracranial hemorrhage expansion raises the issue of its safety in this group of patients.2 Several studies that demonstrated the efficacy of low molecular weight heparin (LMWH) superiority in prophylactic anticoagulation in trauma patients had routinely excluded patients with ICH from their studies.11,12 Despite its proven efficacy for VTE prophylaxis, there is controversial data in the literature regarding the safety of early initiation of enoxaparin in this group of patients. This retrospective cohort represents the author's experience, over a 2-year period, of early DVT prophylaxis with enoxaparin in patients with intracranial hemorrhage following traumatic brain injury.
Patients and Methods
The medical records of 46 patients with isolated traumatic ICH admitted to the Neurosurgical Unit of King Abdulla University Hospital (KAUH) in Irbid, Jordan, were reviewed in the period from January, 2016 to May, 2018. The inclusion criteria for further analysis included isolated traumatic ICH on CT-imaging and early (within 72 hours) administration of VTE prophylaxis, which was continued for at least 1 week.
After the primary survey and resuscitation, emergency brain, cervical spine, chest, abdomen, and pelvic CT scans were performed for all patients. All patients were admitted to the intensive care unit at King Abdulla University Hospital. Proper management of the TBI was conducted by the neurosurgery and critical care teams based on the clinical and radiological findings; the non-surgical treatment included close clinical monitoring of vital signs and the level of consciousness in the intensive care unit and in the neurosurgical ward afterwards, mechanical ventilation, head elevation (30–45º), fluid resuscitation, sedation with either midazolam (1–2 mg/h) or fentanyl (25–100 µg/h), mild hyperventilation (PCO2 30–35 mmHg), osmotherapy (0.25 mg/kg mannitol every 4–6 h), and blood pressure support, when necessary, with dopamine (2–5 µg/kg/min). Different surgical procedures were preformed based on clinical and radiological findings. Precautionary measures included immediate access to surgery whenever deterioration occurred.
Mechanical VTE prophylaxis with a pneumatic compressive device was applied for all patients at the time of admission, additionally all patients received early (within 72 hours) chemical VTE prophylaxis with 40 mg of enoxaparin sodium injected subcutaneously every 24 hours. The administration of chemical VTE prophylaxis was not related to the type of injury, GCS on admission, or brain CT findings. Chemical VTE prophylaxis was started for the surgically managed group 24 hours after surgery. All patients were followed up both clinically and by brain CT-scan. The primary outcome measures were propagation of ICH, and/or deterioration of GCS.
Propagation of ICH was defined as an increase in the size of hemorrhage on a brain CT scan in comparison to the initial CT scan, recurrence of ICH following surgical evacuation, or the occurrence of new ICH.
Results
From January 2016 to May 2018, 46 patients (36 males, 10 females) with traumatic ICH received early (within 72 hours from TBI) thromboembolic prophylaxis with 40 mg of enoxaparin sodium injected subcutaneously every 24 hours. The age of the patients ranged from 16–91 years (43.9±25.8 years). Twenty patients had mild TBI (GCS 15–13), 17 patients had moderate TBI (GCS 12–9), and nine patients had severe TBI (GCS ≤8). GCS on admission ranged from 5–15 (9.9±4.7).
Admission Brain CT scans revealed EDH in 17 patients, SDH in 16 patients, SAH in 10 patients, IVH in five patients, brain hemorrhagic contusions in 12 patients, DAI in three patients, and skull fractures in 10 patients. Sixteen patients had more than one type of traumatic ICH.
Non-surgical management was applied for 18 patients. Craniotomy and surgical evacuation of significant (≥1 cm in maximum diameter) EDH and/or SDH was carried out in 26 patients. An external ventricular drain was inserted in two patients with significant IVH. Cranioplasty and elevation of depressed skull fracture was performed in three patients, all were done at the time of evacuation of EDH or SDH. All patients with isolated brain contusions, SAH, and DAI were managed non-surgically.
All patients in the non-surgical group received VTE prophylaxis with enoxaparin within 72 hours from the time of TBI. The initiation of prophylactic enoxaparin in patients who underwent surgery was 24 hours after surgery. All patients (surgical and non-surgical) received prophylactic enoxaparin within 72 hours from TBI. The duration of VTE prophylaxis ranged from 7–45 days (18±12). The hospital stay ranged from 7–180 days (42±36.8).
CT findings, admission GCS, clinical outcome, and type of management are shown in Table 1.
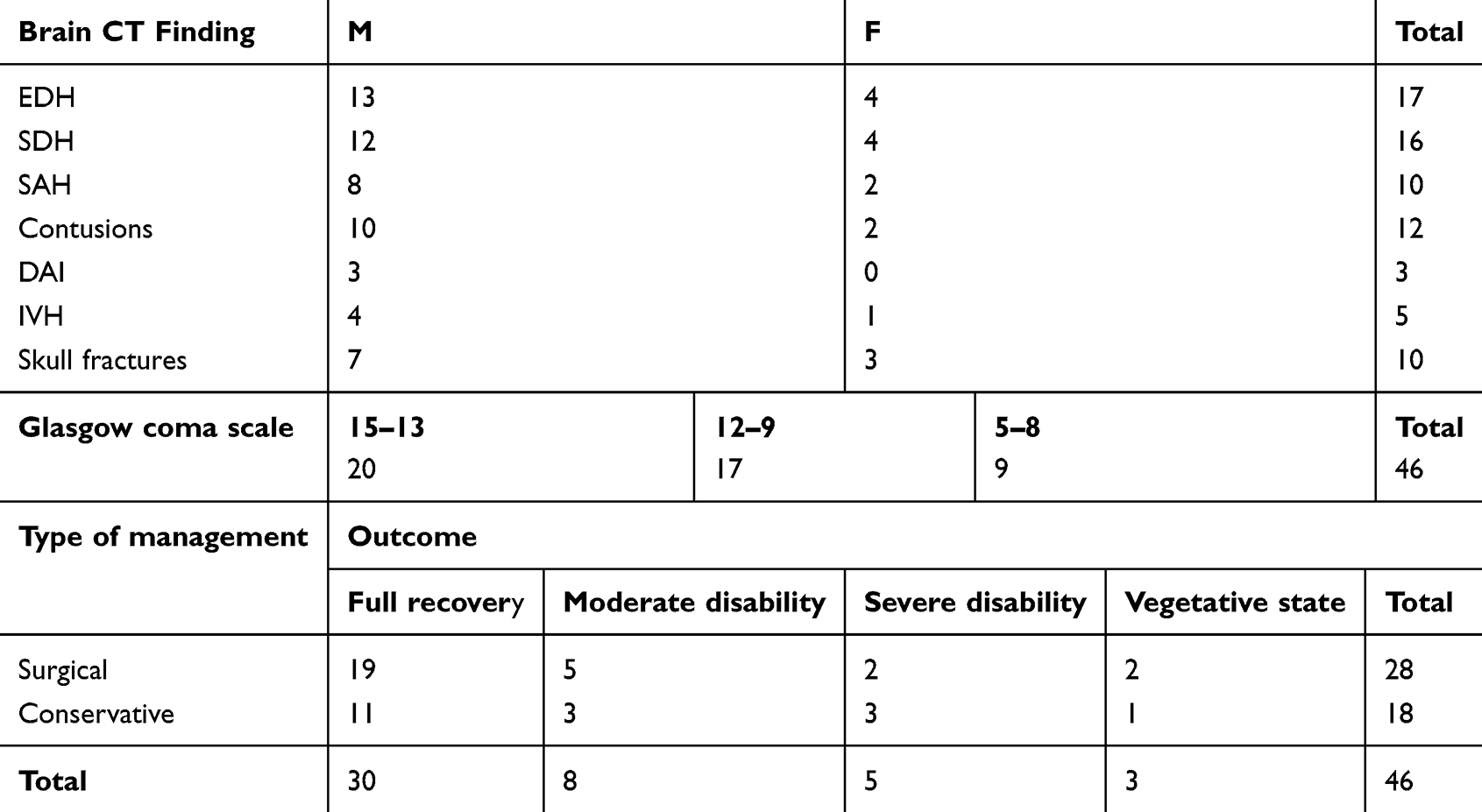 |
Table 1 Brain CT Findings, Admission GCS, Managements, and Outcome of Patients with Closed Traumatic Intracranial Hemorrhage Who Received Prophylactic Enoxaparin |
Eight patients had poor outcome (vegetative state or severe disability) due to their severe injury at presentation. Thirty-eight patients had a good outcome, defined as full recovery or mild disability. Three patients in the poor outcome group continued VTE prophylaxis after hospital discharge.
In the non-surgical group, the brain CT scan was repeated 24 hours after admission, a second follow-up brain CT scan was done within 3 days of admission, and repeated CT scans were done upon clinical need. The surgically treated patients had a follow-up brain CT scan 24 hours after surgery (before the initiation of chemical VTE prophylaxis), repeated within 3 days after initiation of prophylactic enoxaparin and upon clinical deterioration later on. The numbers of follow-up brain CT scans for each patient ranged from 4–12 exams (6±3.5).
None of the conservatively treated patients showed significant progression of the baseline ICH on follow-up brain CT scans and none of them required surgical interventions, this was also reflected by stable clinical course. Similarly, surgically treated patients did not show recurrence of ICH or the development of new ICH following surgical evacuation.
Discussion
VTE is a silent disease, with high morbidity and mortality; moreover, it can easily be missed in trauma patients as the surgeons’ attention usually moves towards more obvious injuries. Here comes the significant role of a VTE prophylaxis protocol in trauma patients. In traumatic ICH the clinical situation is more complex, as the use of anticoagulant prophylaxis may increase the risk of ICH progression; clinicians and researchers are usually avoid or delay the use of anticoagulation in this group of patients. Since the majority of VTE occurs between day 1 and day 4 in TBI patients, early VTE prophylaxis is recommended.13
Enoxaparin (ENX), a low-molecular-weight heparin, has a long established history of reducing injury-related venous thrombotic complications by blocking two key coagulation factors, factor Xa and factor II. Compared with unfractionated heparin, ENX may have superior bioavailability, a higher anti-Xa/anti-IIa ratio, and a longer half-life, making it the agent of choice following multiple injuries and TBI.14,15 It is usually given once daily (40 mg SC injection). Several reports demonstrated the occurrence of ICH expansion following enoxaparin prophylaxis in trauma patients and recommended the use of VTE prophylaxis in selected patients with multiple risk factors for VTE following TBI.7,16,17
Reiff et al4 demonstrated that isolated TBI is an independent risk factor for VTE and PE, as it increases the risk of VTE by 3–4 fold. Byrne et al9 demonstrated that the use of prophylactic enoxaparin in isolated severe TBI patients significantly reduced the risk of VTE without increasing the risk of neurosurgical procedures or death. Cote et al10 showed that death of TBI patients following VTE prophylaxis with enoxaparin was due to PE in all patients and no patients died from expansion of traumatic ICH. The majority of retrospective cohort studies of venous thromboembolic prophylaxis, with enoxaparin, in patients with traumatic intracranial hemorrhage, while biased by the starting dosage, starting time, heterogeneity of patients, and trauma type, demonstrated that the benefits of VTE prophylaxis outweigh the minimal risks of ICH expansion, which in most reports did not mandate surgical intervention or affect the outcome.
This demonstrated safety of enoxaparin was reflected on its clinical use as VTE prophylaxis following spontaneous ICH18,19 and following craniotomies for non-trauma patients.20
In this report the author used early enoxaparin prophylaxis for patient with TBI to avoid the deadly consequences of VTE, taking into consideration the chances of increasing risk for expanding ICH in this group of patients. This heterogeneous group of isolated TBI patients included different age groups (16–91 years), different severity of TBI (mild, moderate, and severe), and different types of intracranial hemorrhage. Sixteen patients had multiple types of ICH. The close monitoring of patients with TBI and frequent brain CT scans were applied for this group of patients to detect early clinical or radiological deterioration. Precautionary measures included immediate access to surgery whenever deterioration occurred.
The authors showed in this review that none of the patients that received prophylactic enoxaparin developed expansion of the primary ICH that affected the patient’s clinical course, also we demonstrated that enoxaparin was safe following craniotomy for different types of traumatic ICH; none of our patient who underwent craniotomy developed recurrence of the ICH. These findings support earlier reports concerning the safety of prophylaxis enoxaparin in patients with traumatic ICH. The main limitation of this report is its retrospective nature. Future prospective studies are needed to further explore the safety of prophylactic enoxaparin in TBI patients.
Enoxaparin prophylaxis may have an additional beneficial role by improving brain perfusion and preventing secondary hypoxic injury in patients with traumatic brain injury. Single-photon emission computed tomography (SPECT) of the brain demonstrated that enoxaparin treatment improves brain perfusion in patients with decreased brain perfusion.21 Additionally animal studies demonstrated that enoxaparin can work as a neuroprotective agent by reducing brain edema and secondary brain injury following TBI due to its anti-inflammatory effects.22,23 Recently, Baharvahdat et al,24 in a randomized double-blinded placebo-controlled pilot trial comparing the effects of high dose of enoxaparin with placebo on the clinical outcome of patients with severe TBI, demonstrated a favorable outcome in the enoxaparin group, despite the higher incidence of hematoma expansion. This first human trial supported the neuroprotective role of enoxaparin as a potential treatment of severe TBI.
Conclusion
Enoxaparin use in TBI patients is safe in not propagating ICH. Future prospective studies can include patient stratification according to specific brain injury characteristics which, in turn, help in drawing more specific prophylaxis guidelines.
Abbreviations
CT, Computed tomography; DAI, Diffuse axonal injury; DVT, Deep vein thrombosis; EDH, Extra dural hematoma; GCS, Glasgow coma scale; ICH, Intracranial hemorrhage; IVH, Intraventricular hemorrhage; LMWH, Low molecular weight heparin; PE, Pulmonary embolism; PTP, Pharmacologic thrombosis prophylaxis; SDH, Subdural hematoma; SPECT, Single photon emission computed tomography; UFH, Unfractionated heparin; VTE, Venous thromboembolism.
Ethics and Consent Statement
This article is compliant with the ethical standards. It was not funded from any source. The research was accepted by the research ethical committee at Jordan University of Science and Technology, Irbid, Jordan (proposal No 231/2017). Based on the nature of the study and the study group, patients consent form was not required by the committee. All patients data are kept confidential and in compliance with the Declaration of Helsinki.
Disclosure
The author discloses no conflicts of interest.
References
1. Knudson MM, Lewis FR, Clinton A, Atkinson K, Megerman J. Prevention of venous thromboembolism in trauma patients. J Trauma. 1994;37:480–487. doi:10.1097/00005373-199409000-00025
2. Browd SR, Ragel BT, Davis GE, Scott AM, Skalabrin EJ, Couldwell WT. Prophylaxis for deep venous thrombosis in neurosurgery: a review of the literature. Neurosurg Focus. 2004;17(4):E1. doi:10.3171/foc.2004.17.4.1
3. Selby R, Geerts W, Ofosu FA, et al. Hypercoagulability after trauma: hemostatic changes and relationship to venous thromboembolism. Thromb Res. 2009;124(3):281–287. doi:10.1016/j.thromres.2008.10.002
4. Reiff DA, Haricharan RN, Bullington NM, et al. Traumatic brain injury is associated with the development of deep vein thrombosis independent of pharmacological prophylaxis. J Trauma. 2009;66:1436–1440. doi:10.1097/TA.0b013e31817fdf1c
5. Praeger AJ, Westbrook AJ, Nichol AD, et al. Deep vein thrombosis and pulmonary embolus in patients with traumatic brain injury: a prospective observational study. Crit Care Resusc. 2012;14(1):10–13.
6. Ekeh AP, Dominguez KM, Markert RJ, McCarthy MC. Incidence and risk factors for deep venous thrombosis after moderate and severe brain injury. J Trauma. 2010;68(4):912–915. doi:10.1097/TA.0b013e3181b21cad
7. Hoffman H, Jalal MS, Chin LS. The risk factors, outcomes, and costs associated with venous thromboembolism after traumatic brain injury: a nationwide analysis. Brain Inj. 2019;16:1–8.
8. Froelich M, Ni Q, Wess C, Ougorets I, Härtl R. Continuous hypertonic saline therapy and the occurrence of complications in neurocritically ill patients. Crit Care Med. 2009;37(4):1433–1441. doi:10.1097/CCM.0b013e31819c1933
9. Byrne JP, Mason SA, Gomez D, et al. Timing of pharmacologic venous thromboembolism prophylaxis in severe traumatic brain injury: a propensity-matched cohort study. J Am Coll Surg. 2016;223(4):621–631.e5. doi:10.1016/j.jamcollsurg.2016.06.382
10. Cote LP, Greenberg S, Caprini JA, et al.; RIETE Investigators. Outcomes in neurosurgical patients who develop venous thromboembolism: a review of the RIETE registry. Clin Appl Thromb Hemost. 2014;20(8):772–778. doi:10.1177/1076029614532008
11. Geerts WH, Jay RM, Code KI, et al. A comparison of low-dose heparin with low-molecular-weight heparin as prophylaxis against venous thromboembolism after major trauma. N Engl J Med. 1996;335(10):701–707. doi:10.1056/NEJM199609053351003
12. Knudson MM, Morabito D, Paiement GD, Shackleford S. Use of low molecular weight heparin in preventing thromboembolism in trauma patients. J Trauma Acute Care Surg. 1996;41(3):446–459. doi:10.1097/00005373-199609000-00010
13. Menaker J, Stein DM, Scalea TM. Incidence of early pulmonary embolism after injury. J Trauma Acute Care Surg. 2007;63(3):620–624. doi:10.1097/TA.0b013e31812f60aa
14. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: american college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(Suppl 2):e227S–e277S. doi:10.1378/chest.11-2297
15. Dudley RR, Aziz I, Bonnici A, et al. Early venous thromboembolic event prophylaxis in traumatic brain injury with low-molecular-weight heparin: risks and benefits. J Neurotrauma. 2010;27(12):2165–2172. doi:10.1089/neu.2010.1366
16. Kimmell KT, Jahromi BS. Clinical factors associated with venous thromboembolism risk in patients undergoing craniotomy. J Neurosurg. 2015;122(5):1004–1011. doi:10.3171/2014.10.JNS14632
17. Algattas H, Kimmell KT, Vates GE, Jahromi BS. Analysis of venous thromboembolism risk in patients undergoing craniotomy. World Neurosurg. 2015;84(5):1372–1379. doi:10.1016/j.wneu.2015.06.033
18. Ianosi B, Gaasch M, Rass V, et al. Early thrombosis prophylaxis with enoxaparin is not associated with hematoma expansion in patients with spontaneous intracerebral hemorrhage. Eur J Neurol. 2019;26(2):333–341. doi:10.1111/ene.13830
19. Wu TC, Kasam M, Harun N, et al. Pharmacological deep vein thrombosis prophylaxis does not lead to hematoma expansion in intracerebral hemorrhage with intraventricular extension. Stroke. 2011;42(3):705–709. doi:10.1161/STROKEAHA.110.600593
20. Khaldi A, Helo N, Schneck MJ, Origitano TC. Venous thromboembolism: deep venous thrombosis and pulmonary embolism in a neurosurgical population. J Neurosurg. 2011;114(1):40–46. doi:10.3171/2010.8.JNS10332
21. Chazova IE, Mychka VB, Mamyrbaeva KM, Gornostaev VV, Dvoskina IM, Sergienko VB. [Cerebrovascular complications in metabolic syndrome: possible approaches to decrease risk]. Ter Arkh. 2004;76(6):74–80. Russian.
22. Li S, Eisenstadt R, Kumasaka K, et al. Does enoxaparin interfere with HMGB1 signaling after TBI? A potential mechanism for reduced cerebral edema and neurologic recovery. J Trauma Acute Care Surg. 2016;80(3):381. doi:10.1097/TA.0000000000000935
23. Li S, Marks JA, Eisenstadt R, et al. Enoxaparin ameliorates post-traumatic brain injury edema and neurologic recovery, reducing cerebral leukocyte endothelial interactions and vessel permeability in vivo. J Trauma Acute Care Surg. 2015;79:78–84. doi:10.1097/TA.0000000000000697
24. Baharvahdat H, Ganjeifar B, Etemadrezaie H, Farajirad M, Zabihyan S, Mowla A. Enoxaparin in the treatment of severe traumatic brain injury: a randomized clinical trial. Surg Neurol Int. 2019;10:10. doi:10.4103/sni.sni_112_18
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.