")
Back to Journals » Journal of Pain Research » Volume 11
The rs4846049 polymorphism in the 3’UTR region of the MTHFR gene increases the migraine susceptibility in an Iranian population
Authors Salehi M, Amin-Beidokhti M, Safarpour Lima B, Gholami M , Javadi G, Mirfakhraie R
Received 29 September 2017
Accepted for publication 29 November 2017
Published 5 January 2018 Volume 2018:11 Pages 145—149
DOI https://doi.org/10.2147/JPR.S152930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Mohaddeseh Salehi,1,* Mona Amin-Beidokhti,2,* Behnam Safarpour Lima,3 Milad Gholami,2 Gholam-Reza Javadi,1 Reza Mirfakhraie2,4
1Department of Biology, Islamic Azad University, Science and Research Branch, 2Department of Medical Genetics, 3Department of Neurology, School of Medicine, 4Genomic Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran
*These authors contributed equally to this work
Introduction: Migraine is a painful complex neurovascular disease characterized by recurrent moderate-to-severe headaches. Increased level of homocysteine is related to dilation of cerebral vessels and endothelial injury that could trigger migraine attacks. Functional polymorphisms in the MTHFR gene affect homocysteine metabolism and, therefore, play an important role in the etiology of the disease.
Objectives: We aimed to investigate the possible association between MTHFR gene rs4846049, C677T, and A1298C polymorphisms and the risk of migraine in Iranian population.
Methods: In this genetic association study, 498 individuals were enrolled, including 223 migraine patients and 275 healthy controls. Genotyping was performed using tetra-primer ARMS-PCR for rs4846049 and PCR-restriction fragment length polymorphism for C677T and A1298C polymorphisms.
Results: The association between rs4846049 and C677T polymorphisms and migraine was observed. For the rs4846049 polymorphism, the association was detected under a dominant model (P=0.007; odds ratio [OR] =0.60; 95% confidence interval [CI], 0.41–0.87), and for the C677T polymorphism, the TT genotype frequency was significantly different in the studied groups (P=0.009; OR =2.48; 95% CI, 1.25–4.92). No significant differences in the genotype or allele frequencies were found for the A1298C polymorphism between the migraineurs and controls.
Conclusion: Present data provide evidence for the association of rs4846049 and C677T polymorphisms in the MTHFR gene and migraine. Further studies are required to validate the significance of the studied genetic variations in diverse ethnic populations.
Keywords: migraine, genetic association study, MTHFR, single nucleotide polymorphism
Introduction
Migraine is a recurrent unilateral pulsatile headache with a significant negative effect on the quality of life. The clinical manifestations of migraine are nausea, vomiting, photophobia, and phonophobia and sometimes, transient neurologic attacks known as “aura”.1–3 Based on the presence or absence of aura, migraine is classified into two particular subtypes, such as migraine without aura (MO) and migraine with aura (MA).4 Several factors including genetic, environment, hormonal factors, and neurotransmitters play roles in the disease etiology.5–7 Among the genetic factors, MTHFR gene can be studied in more detail due to its effect on the plasma level of homocysteine. MTHFR is a key enzyme in folate metabolism, which converts 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate that is required for the remethylation of homocysteine to methionine.8–11 Therefore, reduction in the MTHFR enzymatic activity results in hyperhomocysteinemia that is usually accompanied by spontaneous trigeminal cell firing, one of the possible reasons for headache and pain in migraine.12,13 Genetic polymorphisms in the MTHFR gene could lead to alteration in the enzyme activity. Previous studies have revealed that two common nonsynonymous single-nucleotide polymorphisms (SNPs), C677T (Ala > Val; rs1801133) and A1298C (Glu > Ala; rs1801131), affect the enzyme activity.8 It is suggested that the 677TT and 1298CC genotypes are associated with higher plasma homocysteine level.8,14 However, the results concerning the association between these polymorphisms and susceptibility to migraine were conflicting. Furthermore, SNPs in the 3′UTR region of the genes may affect mRNA-binding affinity for microRNAs, small molecules that play important roles in several complex diseases including cancer, inflammatory diseases, cardiovascular diseases, and atherosclerosis. Emerging data also suggest that miRNAs are regulators of key processes in the nervous and inflammatory systems and, therefore, are likely to be involved in pain signaling and migraine.15 Therefore, the aim of this study was to investigate the association between the MTHFR SNPs including rs4846049 (located in the MTHFR 3′UTR region), C677T, and A1298C with the risk of migraine in Iranian patients.
Subjects and methods
Subject selection
In this case–control study, 498 individuals were enrolled including 223 patients (158 MO patients and 65 MA patients) who suffered from migraine as the case group and 275 healthy controls. Diagnosis of migraine was confirmed based on the results of neurological examination and brain imaging studies in accordance with the International Headache Society (HIS) criteria.16 Control subjects had no personal history or family history of chronic headache and neurological diseases. The samples were obtained between October 2014 and December 2015 from Imam Hossain Hospital, Tehran, Iran. All of the subjects were of Iranian descent and shared common ethnogeographic origin. Patients and controls were matched in age and gender. The mean age of the patients and controls was 33.69±8.92 (range 18–57) and 34.5±10.03 (range 17–58) years, respectively. Written informed consent was obtained from all individual participants included in the study or their parents. The ethics committee of the Shahid Beheshti University of Medical Sciences (SBMU) approved the study protocol (code no: IR.SBMU.MSP.REC.1395.527).
Genotyping of rs4846049 polymorphism
Peripheral blood samples were collected from the study participants in ethylenediaminetetraacetic acid (EDTA) tubes, and genomic DNA was extracted by using the M&D DNA Extraction kit (SBMU, Tehran, Iran) according to the manufacturer’s protocol. Primers were designed using the Primer1 online software for genotyping with tetra primer-amplification refractory mutation system-polymerase chain reaction method.17 The primers used in the PCR included one pair of outer primers, FO 5′TATAACATCTCTTCTACGATGCCACCAGTG3′ and RO 5′ATATACTCTTTTGGTGGGGAGCACTTGC3′, and one pair of inner primers, Fi 5′TTTATATGTACTGCACGGGCTCCAGGT3′ and Ri 5′TATACTGGGACTCCCAGTGAACTTGCC3′. PCR amplification was carried out in a total volume of 25 μL containing genomic DNA (100 ng), 5 pmol/L of outer primers, 10 pmol/L of inner primers, and 12.5 μL of Taq DNA Polymerase 2X Master Mix RED (Ampliqon, Odense M, Denmark). Amplifications were carried out on a FlexCycler (Analytik Jena, Jena, Germany). The PCR program consisted of an initial denaturation step at 94°C for 5 minutes followed by 32 cycles including denaturation at 94°C for 30 seconds, annealing at 63°C for 1 minute, and extension at 72°C for 30 seconds. Finally, one cycle of extension at 72°C for 5 minutes was performed. PCR products were subjected to 2% agarose gel prepared in 0.5× tris/borate/EDTA. The 2572G allele generated a 101 bp band, the T allele generated a 177 bp band, and a common 224 bp band was amplified by the outer primers. Ten percent of the genotypes revealed by TP-ARMS-PCR were further confirmed by sequencing using an ABI 3730xl DNA analyzer (Macrogen, Seoul, Korea).
Genotyping of C677T (rs1801133) polymorphism
The C677T variant was determined by PCR-restriction fragment length polymorphism (RFLP) using the following primers: 677-forward 5′AGCTTTGAGGCTGACCTGAAG3′ and 677-reverse 5′AGGACGGTGCGGTGAGAGTG3′. PCR amplification was carried out in a total volume of 25 μL reaction containing genomic DNA (100 ng), 5 pmol/L of each primer, and 12.5 μL Taq DNA Polymerase 2X Master Mix RED. Amplifications were carried out on a FlexCycler. The PCR program consisted of an initial denaturation step at 94°C for 5 minutes, followed by 32 cycles including denaturation at 94°C for 30 seconds, annealing at 60°C for 1 minute, and extension at 72°C for 30 seconds. Finally, one cycle of extension at 72°C for 5 minutes was performed. PCR amplicons were digested with Hinf I restriction enzyme. Digested products were subjected to 2% agarose gel prepared in 0.5× TBE. The T variant was digested by the enzyme; therefore, wild-type homozygote (CC), heterozygote (CT), and mutant homozygote (TT) showed one band (223 bp), three bands (223, 172, and 51 bp), and two bands (172 and 51 bp), respectively. For further confirmation, 10% of the samples were sequenced by using an ABI 3730xl DNA analyzer.
Genotyping of A1298C (rs1801131) polymorphism
For genotyping A1298C polymorphism, we performed PCR-RFLP by using proposed primers by Anna-Liisa Lorenz et al.18 PCR amplification was carried out in a total volume of 25 μL reaction containing genomic DNA (100 ng), 5 pmol/L of each primer, and 12.5 μL of Taq DNA Polymerase 2X Master Mix RED. Amplifications were carried out on a FlexCycler. The PCR program was the same as the PCR program for genotyping C677T polymorphism with the exception that annealing temperature was 63°C. PCR amplicons were digested with MboII restriction enzyme. Digested products were subjected to 8% polyacrylamide gel electrophoresis (PAGE) prepared in 0.5× TBE and stained with silver nitrate. Three genotypes including AA, AC, and CC showed four bands (22, 28, 30, and 176 bp), five bands (22, 28, 30, 176, and 204 bp), and three bands (22, 30, and 204 bp), respectively. For further confirmation, 10% of the samples were sequenced by using an ABI 3730xl DNA analyzer.
Statistical analysis
Allele and genotype frequencies and the Hardy–Weinberg equilibrium were calculated by chi-squared test using the SNPStats online software available from http://bioinfo.iconcologia.net/SNPstats.19 The association of all polymorphisms with migraine was studied using recessive and dominant models. The strength of association between selected polymorphisms and susceptibility to migraine was evaluated by odds ratios (ORs) and 95% confidence intervals (CIs). A P-value of <0.05 was considered statistically significant.
Results
The results obtained from genotyping using TP-ARMS-PCR and PCR-RFLP was in 100% concordance with the sequencing results. The genotype distribution in the patients and controls were in complete Hardy–Weinberg equilibrium for all studied polymorphisms. Table 1 lists the genotype and allele frequencies of the studied polymorphisms for the migraine patients and the control group. For the rs4846049, the frequency of the G allele was significantly higher in the case group compared with the controls (P=0.01; OR =1.38; 95% CI, 1.07–1.78). The analysis of the rs4846049 genotype frequencies showed that the frequency of the GT and TT genotypes was significantly different between the studied groups (P=0.01; OR =0.61; 95% CI, 0.41–0.91 and P=0.02; OR =0.57; 95% CI, 0.34–0.94, respectively). Moreover, a significant difference under dominant model was observed between the studied case and control groups (P=0.007; OR =0.60; 95% CI, 0.41–0.87).
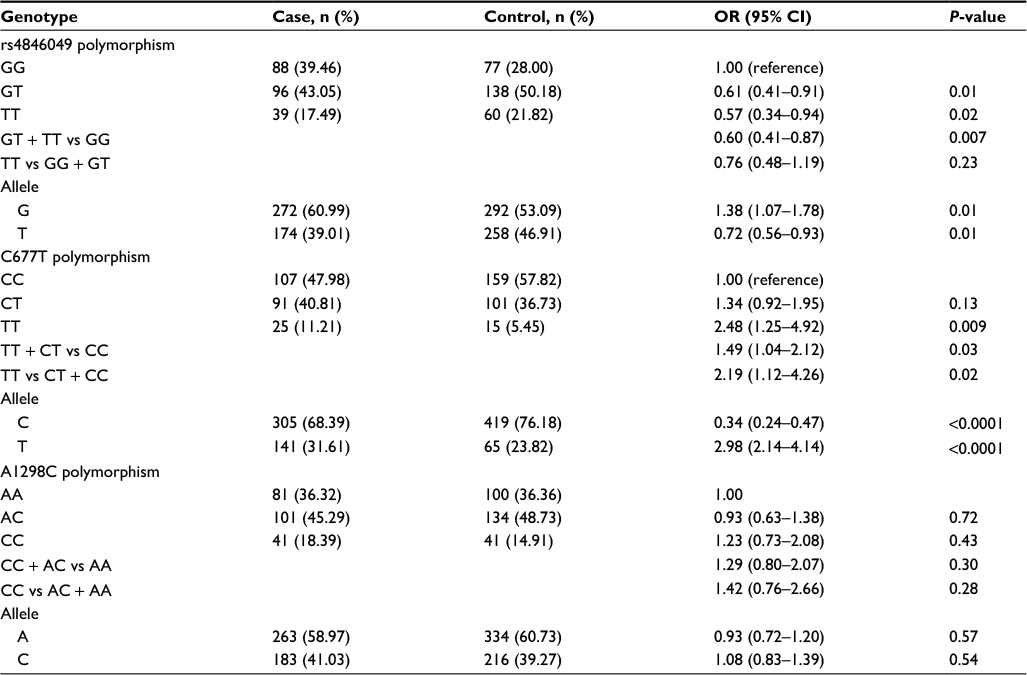 | Table 1 Genotype and allele frequencies of the MTHFR gene rs4846049, C677T, and A1298C polymorphisms in case and control groups Abbreviations: CI, confidence interval; OR, odds ratio. |
For the C677T polymorphism, the frequency of the T allele was significantly higher in the case group compared with the controls (P<0.0001; OR =2.98; 95% CI, 2.14–4.14). The frequency of the TT genotype was significantly different in the studied groups (P=0.009; OR =2.48; 95% CI, 1.25–4.92). Moreover, significant differences were observed under dominant and recessive models between the studied case and control groups (P=0.03; OR =1.49; 95% CI, 1.04–2.12 and P=0.02; OR =2.19; 95% CI, 1.12–4.26).
No significant differences were detected for A1298C genotype and allele frequencies or any of the genetic models between cases and controls (Table 1).
Discussion
In the present study, we investigated possible association between rs4846049, C677T, and A1298C polymorphisms in the MTHFR gene and migraine in Iranian patients. We observed that the rs4846049 polymorphism increases the susceptibility to migraine in the studied population. The rs4846049 polymorphism exists on the 3′UTR of the MTHFR gene and is a potential binding site for microRNA-149 (miR-149).20,21 SNPs located in the 3′UTR region of the genes could change the genes’ expression regulation due to their effect on the binding of miRNAs. According to the literature, the effectiveness of miR-149 binding to the rs4846049 T allele is more than wild-type G allele. Furthermore, the TT genotype has a reduced MTHFR protein level in peripheral blood mononuclear cells compared to the GG genotype, although interestingly, the MTHFR mRNA expression level is not significantly different between the mentioned genotypes.22
Several studies have proved the role of vascular dysfunction in migraine pathophysiology. For instance, the association of migraine with the risk of ischemic stroke was confirmed in two meta-analysis studies.23,24 In addition, Wu et al22 reported that rs4846049 polymorphism increases coronary heart disease risk through modifying miR-149 binding. Considering the results obtained from Wu et al and the present study, we may hypothesize that the regulatory role of miR-149 on MTHFR expression via rs4846049 polymorphism may explain the vascular dysfunction in migraine. However, further functional studies are required to confirm this hypothesis.
There are several association studies concerning the role of C677T MTHFR polymorphism in migraine that showed conflicting results. Most of the studies suggested the association of 677 T allele with increased risk of migraine, although some suggest no association.8,25–28 In order to prove the exact role of C677T polymorphism in migraine, several meta-analyses were performed. Schurks8 confirmed the positive association between C677T polymorphism and migraine among non-Caucasian populations. However, Rubino et al29 reported no overall association of C677T polymorphism with migraine. The same result was obtained from the meta-analysis conducted by Liu et al28 in Caucasian populations.
In this study, we found that the frequency of the TT genotype was significantly different in the studied groups (Table 1).
The 677T allele decreases MTHFR enzymatic function, and the reduction of enzymatic capacity was previously reported in TT genotypes.9 As it was mentioned previously, failure of activity of MTHFR enzyme could led to hyperhomocysteinemia and reduction in the folate plasma levels that induce dilation of cerebral vessels. These alterations result in an increased risk for coronary heart disease, peripheral vascular and cerebrovascular disease, and inflammation in the meninges that could be involved in the migraine pain.9,12,30 In a recent study in the Turkish population, it was shown that the CT genotype was significantly higher in the migraine patients.26 Our finding is in concordance with the result of the Turkish study which may be explained by the similarity in the genetic background. An et al25 also showed evidence of an association between MTHFR C677T polymorphism and risk of migraine. They observed significantly higher frequency of the T allele in the MO migraine patients than in the controls. The same association between the T allele and migraine was reported by Azimova et al. 27 They mentioned that TT and CT genotypes were significantly associated with sensitivity to migraine attack triggers. Furthermore, the TT genotype was accompanied by photophobia symptom more than in other genotypes.
Previous studies concerning the association of the A1298C polymorphism with migraine showed conflicting results.16,31 Anna-Liisa Lorenz et al18 showed no association between A1298C polymorphism and the risk of migraine. However, Kara et al31 suggested that the 1298C allele was significantly higher in migraine patients than in controls. Our data were consistent with the negative association of A1298C polymorphism with migraine.
Conclusion
This study suggests the association of rs4846049 and C677T polymorphisms with the risk of migraine in Iranian population. To the best of our knowledge, this is the first study to investigate the association between rs4846049 polymorphism and migraine. Further studies are required to validate the significance of the studied genetic variations in diverse ethnic populations.
Acknowledgments
We would like to thank all the participants of the study. This study was financially supported by the “Research Department of the School of Medicine Shahid Beheshti University of Medical Sciences” (grant no 10175).
Disclosure
The authors report no conflicts of interest in this work.
References
Haut SR, Bigal ME, Lipton RB. Chronic disorders with episodic manifestations: focus on epilepsy and migraine. Lancet Neurol. 2006;5(2):148–157. | ||
Menken M, Munsat TL, Toole JF. The global burden of disease study: implications for neurology. Arch Neurol. 2000;57(3):418–420. | ||
Silberstein SD. Migraine. Lancet. 2004;363(9406):381–391. | ||
Fang J, An X, Chen S, Yu Z, Ma Q, Qu H. Case-control study of GRIA1 and GRIA3 gene variants in migraine. J Headache Pain. 2015;17:2. | ||
Ates O, Kurt S, Altinisik J, Karaer H, Sezer S. Genetic variations in tumor necrosis factor alpha, interleukin-10 genes, and migraine susceptibility. Pain Med. 2011;12(10):1464–1469. | ||
Charbit AR, Akerman S, Goadsby PJ. Dopamine: what’s new in migraine? Curr Opin Neurol. 2010;23(3):275–281. | ||
Ghosh J, Pradhan S, Mittal B. Multilocus analysis of hormonal, neurotransmitter, inflammatory pathways and genome-wide associated variants in migraine susceptibility. Eur J Neurol. 2014;21(7):1011–1020. | ||
Schurks M. Genetics of migraine in the age of genome-wide association studies. J Headache Pain. 2012;13(1):1–9. | ||
Frosst P, Blom HJ, Milos R, et al. A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nat Genet. 1995;10(1):111–113. | ||
Graham IM, O’Callaghan P. Vitamins, homocysteine and cardiovascular risk. Cardiovasc Drug Ther. 2002;16(5):383–389. | ||
Stuart S, Cox HC, Lea RA, Griffiths LR. The role of the MTHFR gene in migraine. Headache. 2012;52(3):515–520. | ||
Parsons AA, Strijbos PJ. The neuronal versus vascular hypothesis of migraine and cortical spreading depression. Curr Opin Pharmacol. 2003;3(1):73–77. | ||
Pizza V, Agresta A, Agresta A, et al. Migraine and genetic polymorphisms: an overview. Open Neurol J. 2012;6:65–70. | ||
Kumar J, Das SK, Sharma P, Karthikeyan G, Ramakrishnan L, Sengupta S. Homocysteine levels are associated with MTHFR A1298C polymorphism in Indian population. J Hum Genet. 2005;50(12):655–663. | ||
Tana C, Giamberardino MA, Cipollone F. microRNA profiling in atherosclerosis, diabetes, and migraine. Ann Med. 2017;49(2):93–105. | ||
Headache Classification Committee of the International Headache S. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808. | ||
Ye S, Dhillon S, Ke X, Collins AR, Day IN. An efficient procedure for genotyping single nucleotide polymorphisms. Nucleic Acids Res. 2001;29(17):E88. | ||
Anna-Liisa Lorenz AL, Kahre T, Mihailov E, et al. Are methylenetetrahydrofolate reductase (MTHFR) gene polymorphisms C677T and A1298C associated with higher risk of pediatric migraine in boys and girls? JBiSE. 2014;7(8):464–472. | ||
Sole X, Guino E, Valls J, Iniesta R, Moreno V. SNPStats: a web tool for the analysis of association studies. Bioinformatics. 2006;22(15):1928–1929. | ||
Chen K, Song F, Calin GA, Wei Q, Hao X, Zhang W. Polymorphisms in microRNA targets: a gold mine for molecular epidemiology. Carcinogenesis. 2008;29(7):1306–1311. | ||
Ryan BM, Robles AI, Harris CC. Genetic variation in microRNA networks: the implications for cancer research. Nat Rev Cancer. 2010;10(6):389–402. | ||
Wu C, Gong Y, Sun A, et al. The human MTHFR rs4846049 polymorphism increases coronary heart disease risk through modifying miRNA binding. Nutr Metab Cardiovasc Dis. 2013;23(7):693–698. | ||
Colson NJ, Lea RA, Quinlan S, Griffiths LR. The role of vascular and hormonal genes in migraine susceptibility. Mol Genet Metab. 2006;88(2):107–113. | ||
Spector JT, Kahn SR, Jones MR, Jayakumar M, Dalal D, Nazarian S. Migraine headache and ischemic stroke risk: an updated meta-analysis. Am J Med. 2010;123(7):612–624. | ||
An XK, Lu CX, Ma QL, et al. Association of MTHFR C677T polymorphism with susceptibility to migraine in the Chinese population. Neurosci Lett. 2013;549:78–81. | ||
Bahadir A, Eroz R, Dikici S. Investigation of MTHFR C677T gene polymorphism, biochemical and clinical parameters in Turkish migraine patients: association with allodynia and fatigue. Cell Mol Neurobiol. 2013;33(8):1055–1063. | ||
Azimova JE, Sergeev AV, Korobeynikova LA, et al. Effects of MTHFR gene polymorphism on the clinical and electrophysiological characteristics of migraine. BMC Neurol. 2013;13:103. | ||
Liu R, Geng P, Ma M, et al. MTHFR C677T polymorphism and migraine risk: a meta-analysis. J Neurol Sci. 2014;336(1–2):68–73. | ||
Rubino E, Ferrero M, Rainero I, Binello E, Vaula G, Pinessi L. Association of the C677T polymorphism in the MTHFR gene with migraine: a meta-analysis. Cephalalgia. 2009;29(8):818–825. | ||
Di Minno MN, Tremoli E, Coppola A, Lupoli R, Di Minno G. Homocysteine and arterial thrombosis: challenge and opportunity. Thromb Haemost. 2010;103(5):942–961. | ||
Kara I, Sazci A, Ergul E, Kaya G, Kilic G. Association of the C677T and A1298C polymorphisms in the 5,10 methylenetetrahydrofolate reductase gene in patients with migraine risk. Brain Res Mol Brain Res. 2003;111(1–2):84–90. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.