")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Role of the Integrated District Hospital Based Non Communicable Diseases’ Clinics in Cardiovascular Disease Control: Preliminary Data from Rwanda
Authors Kabakambira JD , Shumbusho P, Mujawamariya G, Rutagengwa W, Twagirumukiza M
Received 29 December 2021
Accepted for publication 13 July 2022
Published 20 July 2022 Volume 2022:15 Pages 2107—2115
DOI https://doi.org/10.2147/DMSO.S348031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Jean Damascene Kabakambira,1,2 Patrick Shumbusho,1,2 Gisele Mujawamariya,1 William Rutagengwa,3 Marc Twagirumukiza2,4
1Department of Internal Medicine, University Teaching Hospital of Kigali, Kigali, Rwanda; 2College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda; 3Department of Internal Medicine, Nyamata District Hospital, Bugesera, Rwanda; 4Faculty of Medicine and Health Sciences, Ghent University, Ghent, Belgium
Correspondence: Jean Damascene Kabakambira, Department of Internal Medicine, University Teaching Hospital of Kigali, KN 4th Avenue, P.O Box 655, Kigali, Rwanda, Tel +250 788800966, Email [email protected]
Introduction: Noncommunicable diseases (NCDs), remain the leading cause of death worldwide and represent an emerging global health threat. In Rwanda and elsewhere, the prevalence of cardiovascular diseases is increasing. To address this global health threat, Rwanda launched integrated nurse-led NCD clinics in all the forty-five District Hospitals across the country in 2006, but no evaluation study has been conducted so far for the added value of this program. The main goal of this study was to assess the impact of NCD clinics on disease control in Rwanda.
Methods: This was a retrospective ambulatory patient chart review at a rural district hospital and an urban teaching hospital; which enrolled patients with diabetes and/or hypertension who consulted in a period of 1 month with retrospective data of one year.
Results: A total of 199 patients’ electronic health records were reviewed from the University Teaching Hospital of Kigali (CHUK) (53%) and Nyamata District Hospital (47%). Among them, 31% had diabetes, 38% had hypertension and 31% had both diseases. The mean age for the total cohort was 60 years and was predominantly female at 70%. Throughout the year, about 59% patients with hypertension had blood pressure control at the district hospital as opposed to 38% at the referral hospital. The rate of diabetes control was 20% at the referral hospital, but no comparison could be established between the two health facilities as the follow up laboratory markers were not available at the district hospital.
Conclusion: There was a consistent blood pressure control at the district hospital. Diabetes control was not optimal at the referral hospital despite the presence of human resources and logistics required for diabetes care. The situation was even worse at the district hospital where the follow up markers were rarely available.
Keywords: NCD clinic, diabetes, hypertension, Rwanda
Background
Non-communicable diseases (NCDs) including hypertension and diabetes remain the leading cause of mortality worldwide.1 For instance, NCDs were responsible for 38 million (68%) of the 56 million deaths that occurred in 2012. The majority of NCD related deaths as well as the majority of premature deaths occur in low and middle income countries.1 NCDs dominate the global burden of diseases, causing a lot of economic pressure on countries struggling against poverty. Estimates show that between 2011 and 2025, NCDs will cost over US$ 50 trillion from the global economy.2 This is a loss which represents about 70% of global gross domestic product (GDP) in 2010. Fortunately, it has been proven that NCD prevention is more cost effective compared to the cost of inaction.2 Cardiovascular diseases (CVDs), diabetes, cancer and respiratory diseases are the four main NCDs and account for over 80% of NCD related deaths. Of all these conditions, diabetes is the most threatening since it is a great risk factor for cardiovascular diseases and cancer on top of traditional complications of its own.
According to the International Diabetes Federation (IDF), 10.5% of adults aged 20–79 years are estimated to have diabetes worldwide.3 In Africa, the prevalence of diabetes in adults is estimated at 4.5%.3 But at the same time Africa has the highest rate (53.6%) of undiagnosed people living with type 2 diabetes mellitus.4 This might be due to the fact that most people only consult when they feel sick, yet diabetes exhibit a progressive course without any apparent immediate effect on physiology or threat of death. In Rwanda for instance, according to the first ever national NCD risk survey conducted by the ministry of health in 2012–2013, 98% of respondents reported that they had never had their blood glucose measured, therefore a missed opportunity for early diagnosis.5
In 2006, Rwanda launched integrated nurse-led NCD clinics in all the forty-five District Hospitals (DH) across the country.6 NCD clinics provide chronic care to patients with diabetes, hypertension, asthma as well as rheumatic heart diseases. These NCD clinics are entirely managed by registered nurses who received a basic training by the ministry of health. Patients with complicated NCD conditions get referred to higher care level through established channels of patient referral in Rwanda. The model of NCD clinics has not been implemented in tertiary level teaching hospitals. In teaching hospitals, patients with NCDs are seen together with other patients with any internal medicine related conditions. Generally, consultations are undertaken by a specialist physician or a resident which means doctors undertaking a four-year postgraduate Masters program of specialization in Internal Medicine.
The main goal of this study was to assess the impact of NCD clinics healthcare delivery on hypertension and diabetes control in Rwanda.
Methods
The study’s aim was to assess the hypertension and diabetes control in sampled referral and District hospitals based on selected parameters including the blood pressure, fasting blood glucose and HbA1c. At the referral hospital, diabetes and hypertension are treated by Internal Medicine Specialists using OpenClinic as an electronic medical record. Anthropometrics, clinical information and laboratory findings are all found in patients’ electronic files. The international Classification of Diseases (ICD-10) coding is used by doctors to write patients’ diagnosis. This facilitated the task of identifying study participants. At the district hospital, diabetes and hypertension are treated by trained nurses in the NCD clinic. Anthropometrics and other clinical information are kept in a paper file but laboratory data are in OpenClinic. Files are kept in a locked room according to diagnosis. Researchers did not carry out any intervention or encounter patients, but rather accessed patients’ files to extract clinical information pertaining to blood pressure and diabetes control. At CHUK, HbA1C is performed by a biochemistry analyzer machine and by a point-of-care machine at Nyamata Hospital.
Due to the logistical constraints imposed by the COVID-19 pandemic, we only report findings from 1 referral hospital and 1 district hospital for which data were available before the pandemic.
Study Objectives
This study aimed at determining at 1 referral hospital and 1 District Hospital:
- Glycemic control among patients with diabetes as defined by HbA1C<6.5%.
- Blood pressure control among patients with hypertension as defined by systolic blood pressure <140 mmHg and diastolic blood pressure < 90 mmHg.
- Incidence of chronic kidney disease (CKD) among patients with diabetes and/or hypertension.
Study Settings
This was a retrospective chart review of ambulatory patients’ Electronic Health Records (EHRs) at a rural district hospital and an urban teaching hospital; Nyamata District Hospital (NDH) and the University Teaching Hospital of Kigali (CHUK) respectively. NDH is located in Eastern Province and has a well-organized nurse-led NCD clinic and receives mostly rural patients. CHUK is located in Kigali, the capital city and receives urban patients and patients with severe and uncontrolled diseases from district hospitals in the catchment area.
Study Population
This study enrolled patients with diabetes and/or hypertension who consulted the above mentioned health facilities in a period of one month (November 2019) with retrospective data of one year.
In the charts review we included all patients who consulted in the respective hospitals in November 2019, who had been in the program for at least one year, having either diabetes or hypertension or both and aged 18 years and above.
Convenient sampling was applied. Variables related to diabetes, hypertension and their complications were recorded at enrolment and after one year of treatment: anthropometrics, blood pressure and biological measures of blood glucose and kidney function.
Ethical Consideration
The study was approved by the University of Rwanda’s College of Medicine and Health Sciences Institution Review Board (IRB No 485/CMHS IRB/219). Data were entirely extracted from patients’ chart and there was no contact or interaction with patients. Therefore, informed consents were deemed unnecessary. The study complies with the Declaration of Helsinki.
Data Analysis
The data entry was done with Epidata 3.1 and then exported to STATA (v 15, College Station, Texas) for statistical analysis. Descriptive characteristics are presented using means. Comparison of continuous variables among hospitals were done by Student’s t-test. Comparison of categorical variables was done with Chi-square. For all the tests, a P value of ≤ 0.05 was considered as statistically significant.
Results
From 1st to 30 November 2019, we counted 199 patients with diabetes, hypertension or both who had visited the outpatient settings of CHUK or Nyamata District Hospital (NDH). CHUK accounted for 53% (106/199) while 47% of patients (93/199) were from NDH. For the total cohort, 31% patients (61/199) had diabetes, 38% (76/199) had hypertension while 31% (62/199) had both diabetes and hypertension. Men accounted for only 30% (59/199).
Population Characteristics According to Site of Care and Diagnosis
Anthropometrics
The mean age for the total cohort was 60 years. There was no age difference in two sites of study (Table 1). Patients with diabetes alone were much younger than patients with either hypertension alone or with both diseases (Table 2).
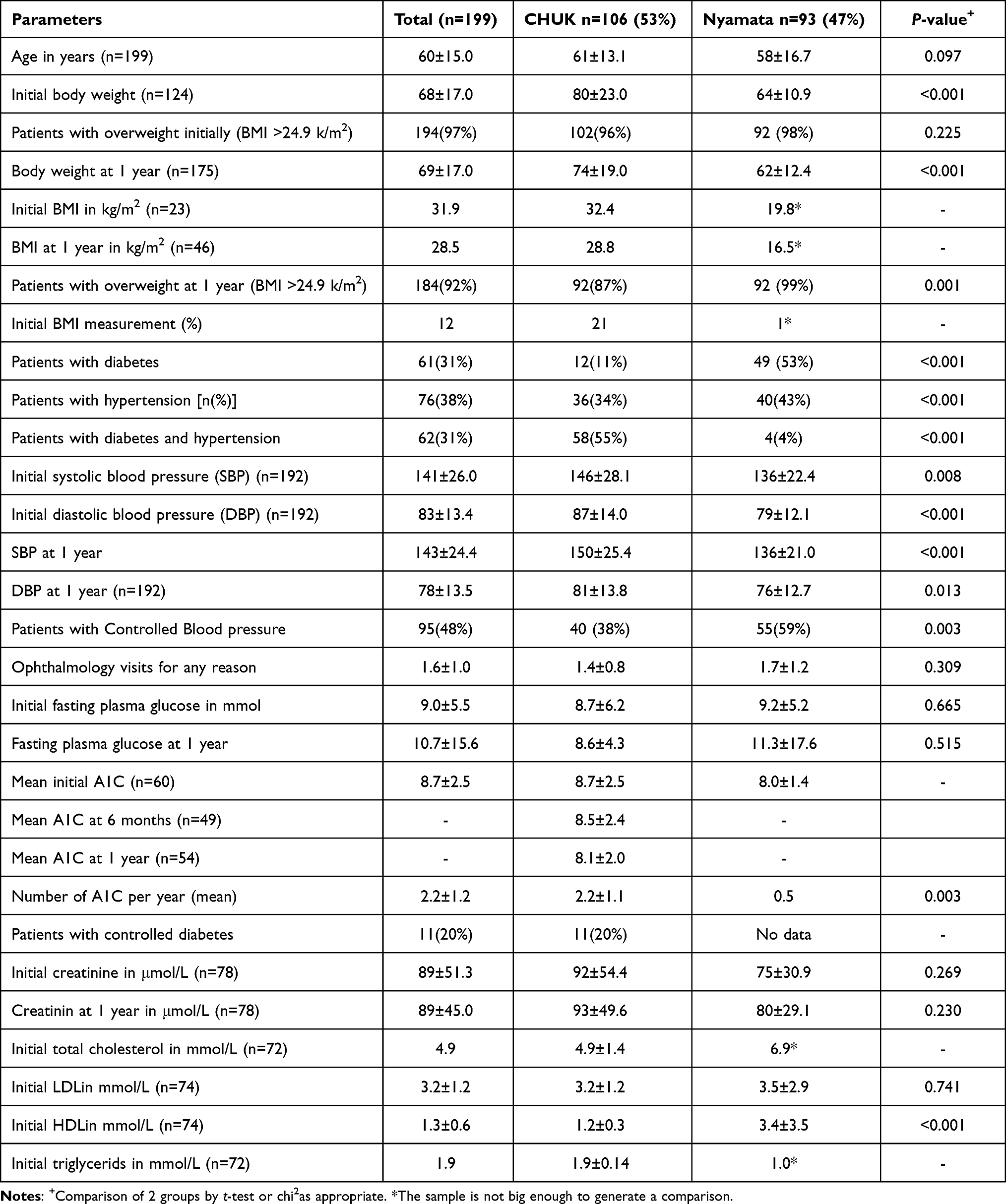 |
Table 1 Population Characteristics According to Site of Care |
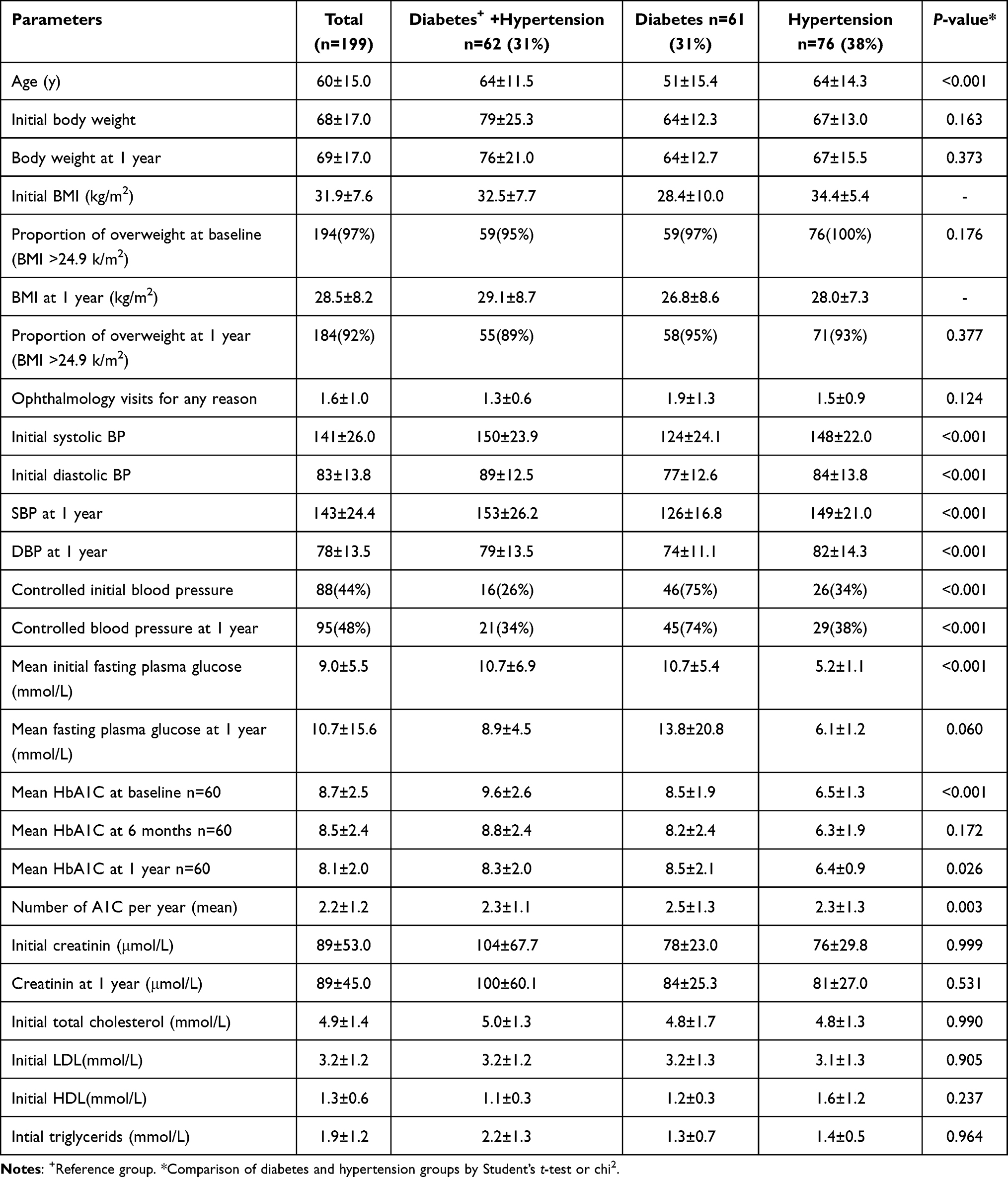 |
Table 2 Population Characteristics According to Diagnosis |
Patients at CHUK (urban area) had higher initial body weight compared to NDH which is in a rural area (80±23.0 vs 64±10.9 kg, P=0.001). The difference in body weight was maintained at the end of the year (74±19.0 vs 62±12.4 kg, P<0.001). Patients with both diagnoses had higher body weight than counterparts with either diabetes or hypertension alone both in the beginning (P<0.001) and at the end of the year (P=0.001) (Table 2).
Body mass index (BMI) was rarely calculated at CHUK (25% of patients) and almost never calculated at NDH (1% of patients). Nevertheless, the body weight was provided in most cases but the height was missing. There was no difference in BMI according to diagnosis. Waist circumference is also done in few patients at CHUK and never done at NDH (Table 1).
Blood Pressure
The initial systolic blood pressure was higher at CHUK (146±28.1 vs 136±22.4 mmHg, P=0.008) and the difference was maintained at the end of the year (150±25.4 vs 136±21.0 mmHg, P<0.001). The same difference trend was observed in diastolic pressures. Infact, upon one year, 38% patients at CHUK had normal blood pressure as opposed to 59% at NDH (P=0.003). Upon one-year follow-up, significant changes in blood pressure were only observed in diastolic blood pressure at CHUK (8713.8± mmHg vs 80±13.7, P<0.001) (Table 3).
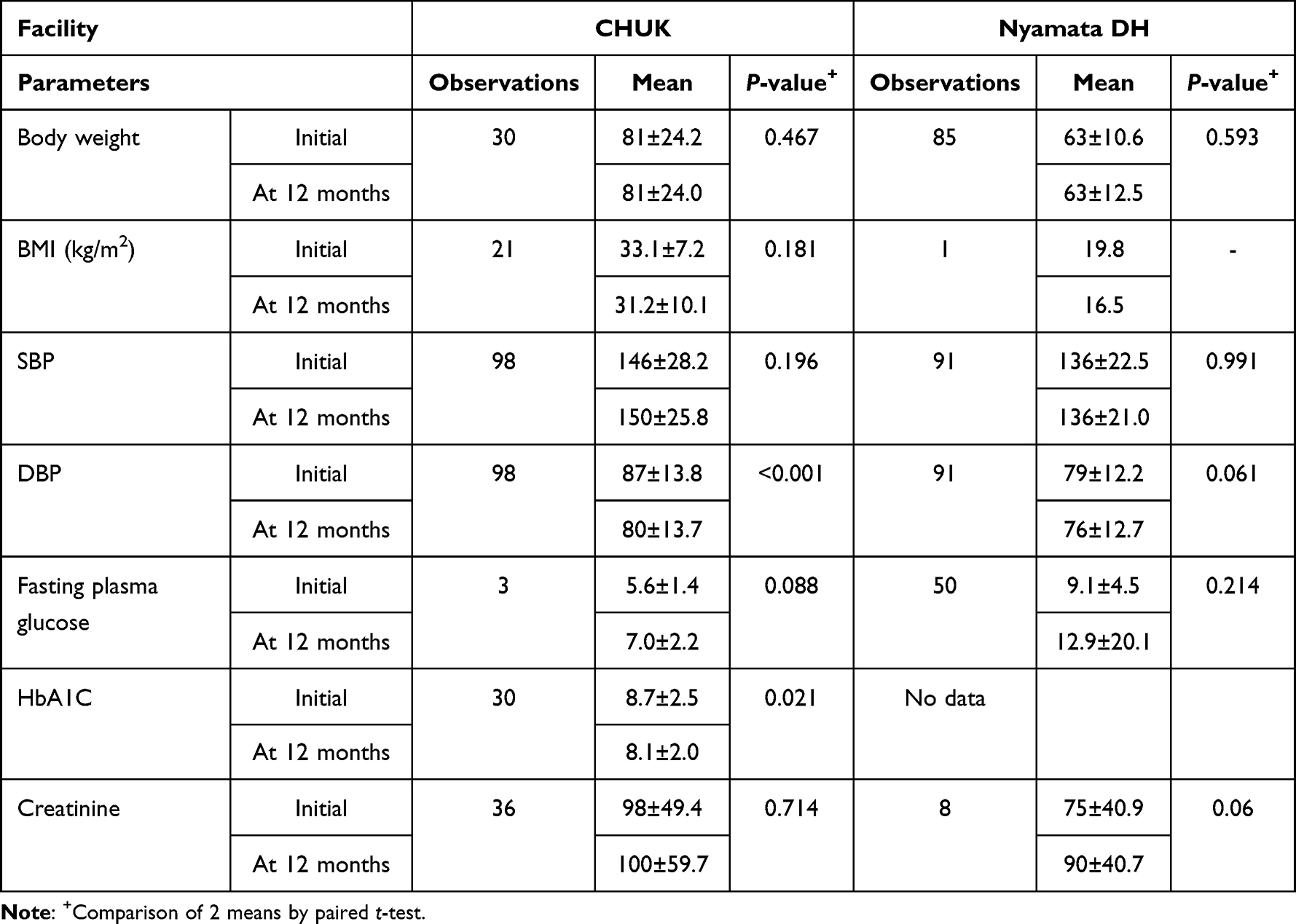 |
Table 3 Change in Metabolic Characteristics Over 1 Year |
Biological Parameters
There was no difference in fasting plasma glucose at CHUK and NDH both initially (8.7±6.2 vs 9.25.2± mmol/L, P=0.664) and after one year follow up (8.6±4.3 vs 11.3±17.6 mmol/L, P=0.515). The change in fasting plasma glucose after one year was not significant at both institutions (Table 3). The fasting plasma glucose was lower in the patients with hypertension alone but there was no difference between groups after one year of treatment. The same trend was observed in Hemoglobin A1C (HbA1C).
The mean HbA1C was 8.7% (n=60) at CHUK and 8% (n=2) at NDH. No comparison can be established between the two institutions with regards to HbA1C as it was done only in few individuals at NDH. It was observed that the frequency of measurement of HbA1C, the best treatment follow-up marker for diabetes, was not optimal at both institutions. The frequency of HbA1C measurement at CHUK was 2.2 per patient per year compared to 0.5 HbA1C measurements per patient per year at NDH. At CHUK, where HbA1C data were available, a significant change was observed after one year of follow up (8.7±2.5% vs 8.1 ±2.0%, P=0.021). Only 11 (20%) patients had good diabetes control at CHUK as defined by an HBA1C < 6.5%.
Kidney function was commonly assessed with creatinine. Creatinine was regularly measured at both institutions and no statistical difference was observed both initially and at 12 months of follow up. The change in creatinine was not statistically significant at both health facilities. Another kidney function marker, microalbuminuria, is a reliable marker of early kidney dysfunction. Unfortunately, albuminuria was only assessed in 47% of patients at CHUK but no single patient had it measured at the district hospital. Lipid profile was only evaluated in most patients at CHUK but it was measured in only one patient at NDH.
Discussion
This study intended to assess the level of non-communicable disease (NCD) control comparing an urban tertiary level hospital to a rural district hospital with an established nurse-led NCD clinic.
The mean age in the population was 60 years, which is at upper age limit of active population and falls under old population group in a Rwandan population which is rather younger in general. According to the World Health Organization, only 46% of the adult Rwandan population are above 35 years of age.5 This old age in our study suggests a late consultation at healthcare facilities within a context of scarce early disease screening and/or detection programs. However, this is in line with findings in other studies on diabetes.7 Patients from urban area had higher body weights than counterparts from rural area. The finding aligns well with the common knowledge of higher obesity rates in urban areas.8 Urban populations tend to be more exposed to unhealthy meals and lead a sedentary lifestyle.
The rates of blood pressure control among patients with hypertension in our cohort were around 30% which is similar to findings in similar studies across literature. In a study conducted in 12 countries in sub-Saharan Africa, blood pressure control was found to be around 20%9 but a systematic review revealed blood pressure control in 38% of patients.10 Blood pressure was much better controlled at NDH compared to CHUK. This could have been the effect of more rigorous and regular follow up by a permanent, assigned nurse in the NCD clinic as opposed to CHUK where physicians keep changing and have less knowledge and bonds with individual patients. On the other hand, failure to meet target blood pressure control at a tertiary hospital might be due to the complexity and severity of diseases at this level of care as the facility usually takes care of referred patients from district hospitals.
Only 20% of patients had well-controlled diabetes at CHUK which is sub-optimal. Worldwide, diabetes is notoriously known to be hard to control. Diabetes control varies widely but rates of control are less than 50% in many places across the world.11 The rates of diabetes control were not available at NDH because HBA1C is rarely performed at NDH. According to clinicians in District Hospitals, HBA1C is available in most district hospitals but not supported by the community health insurance scheme, which makes it widely financially inaccessible. Whether this challenge fully explains the reason why this important follow up biomarker is not timely performed needs to be investigated. On the other hand, a knowledge, attitude and practice study among nurses in NCDs clinics would help to rule out the knowledge gap as an alternative explanation. An alternative way to assess the level of diabetes control at the district hospital could have been the fasting plasma glucose. But given the retrospective nature of the study, this measurement was deemed unreliable and therefore was not used as it involves speaking to patients to understand what patients understand by “fasting”.
This study recorded a surprising finding. The mean HBA1C was 6.5% in the group of patients with hypertension alone. However, this value qualifies as a diagnostic cut-off for diabetes according to the American Diabetes Association.12 This finding suggests undiagnosed diabetes in this group whether incident or prevalent. The SPRINT (Systolic Blood Pressure Intervention Trial) has revealed higher incidences of diabetes among hypertensive patients than in the general population.13 This study showed 299 incident diabetes mellitus events (2.3% per year) for intensive blood pressure control (Systolic blood pressure < 120 mmHg) versus 251 events (1.9% per year) for standard blood pressure control (Systolic blood pressure < 140 mmHg). It is imperative to know if patients with hypertension are adequately screened for diabetes and treated on time since the combination of both diseases increases risks for complications.14
The lack of statistically significant changes in creatinine over one year shows a slow progress to renal impairment. However, this is a short time follow up and the retrospective nature would not allow to draw firm conclusions with regards to kidney function among patients with diabetes and/or hypertension at the two facilities. The United Kingdom Prospective Diabetes Study (UKPDS) offered a unique opportunity to observe the natural history of diabetic kidney disease in patients with type 2 diabetes from early in the course of diabetes but had to extend over decades.15 Microalbuminuria, the earliest marker of progression to kidney disease, was frequent missing in the majority of patients at both centers.
Study Limitation
This study is based on EHRs charts review and like other charts review studies, the main limitation is the data incompleteness where some variables of interest are missing like the HbA1c which was not available at one center.
Also the data gathering was not complete, the current study presents only preliminary findings. The outbreak of Coronavirus (COVID-19) pandemic in Rwanda delayed the charts review process which will resume when the situation becomes stable. It would therefore be premature to generalize findings of this study on the entire country.
Conclusions and Policy Implication
There was a great blood pressure control at the district hospital. This raises confidence in the currently existing NCDs with regards to their ability to treat hypertension. Referral hospitals should feel comfortable counter-referring stable patients with hypertension to lower levels of care. This also leaves a reflection to referral hospitals, as to whether establishing a designated facility for hypertension care or NCD clinic would have a greater impact in better control for patients with NCDs. Nonetheless, the current data are not enough to compare the two levels of care as the referral hospital tends to receive sicker patients thus harder to control.
Diabetes control was not optimal at the referral hospital despite the presence of human resources and logistics required for diabetes care. Frequent laboratory follow-ups and referrals to diabetes caregivers such ophthalmologists, podiatrists and dieticians are needed to prevent diabetes complications. Furthermore, the present study was not able to find reliable information regarding diabetes control at the district hospital level. De-escalation of diabetes care to NCD Clinics should be done with caution until necessary resources are made available.
What is Already Know on This Topic
- Cardiovascular diseases represent a major burden worldwide and particularly in countries where resources are limited.
- In Rwanda and some other parts of the world, an initiative to launch integrated nurse-led NCD clinics aimed at improving access to care while curbing NCDs to decrease the cardiovascular disease burden.
What This Study Adds
- The study suggests that the level of hypertension control is satisfactory in the NCDs clinics even though they are run by nurses with less expertise than physicians. This increases confidence in having patients with hypertension managed in NCDs Clinics which would decrease the burden of referral hospitals as they struggle with other complicated pathologies.
- The study has shown that diabetes control is still problematic at both levels of care but especially NCD Clinics are not yet ready to deal with diabetes which requires heavy and multidisciplinary resources.
Acknowledgments
We thank the clinical staff in the Outpatient Department of CHUK and NCD Clinic of Nyamata District Hospital for facilitating data collection. Our appreciation goes to Dr Vanessa Umubyeyi Mupenzi who greatly contributed to data collection along with Dr Gisele Mujawamariya and Dr Patrick Shumbusho.
Funding
The study was not funded.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. World Health Organization. Global status report on noncommunicable diseases 2014. World Health Organization. Available from: http://www.who.int/nmh/publications/ncd-status-report-2014/en/.
2. Allen LN. Financing national non-communicable disease responses. Glob Health Action. 2017;10(1326687):1326687. doi:10.1080/16549716.2017.1326687
3. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2021;183:109119. doi:10.1016/j.diabres.2021.109119
4. Ogurtsova K, Guariguata L, Barengo NC, et al. IDF Diabetes Atlas: global estimates of undiagnosed diabetes in adults for 2021. Diabetes Res Clin Pract. 2021;183:109118. doi:10.1016/j.diabres.2021.109118
5. Ministry of Health, Rwanda. Rwanda non-communicable diseases risk factors report; 2015.
6. Park PH, Pastakia SD. Access to hemoglobin A1c in Rural Africa: a difficult reality with severe consequences. J Diabetes Res. 2018;2018:1–5. doi:10.1155/2018/6093595
7. Zoungas S, Woodward M, Li Q, et al. Impact of age, age at diagnosis and duration of diabetes on the risk of macrovascular and microvascular complications and death in type 2 diabetes. Diabetologia. 2014;57(12):2465–2474. doi:10.1007/s00125-014-3369-7
8. Akhtar S, Nasir JA, Sarwar A, et al. Prevalence of diabetes and pre-diabetes in Bangladesh: a systematic review and meta-analysis. BMJ Open. 2020;10(e036086):e036086. doi:10.1136/bmjopen-2019-036086
9. Antignac M, Diop IB, Macquart de Terline D, et al. Socioeconomic status and hypertension control in sub-Saharan Africa: the Multination EIGHT study (Evaluation of Hypertension in Sub-Saharan Africa). Hypertension. 2018;71(4):577–584. doi:10.1161/HYPERTENSIONAHA.117.10512
10. Addo J, Smeeth L, Leon DA. Hypertension in sub-saharan Africa: a systematic review. Hypertension. 2007;50(6):1012–1018. doi:10.1161/HYPERTENSIONAHA.107.093336
11. Mainous AG, King DE, Garr DR, Pearson WS. Race, rural residence, and control of diabetes and hypertension. Ann Fam Med. 2004;2(6):563–568. doi:10.1370/afm.119
12. Arslanian S, Bacha F, Grey M, et al. Evaluation and management of youth-onset type 2 diabetes: a position statement by the American Diabetes Association. Diabetes Care. 2018;41(12):2648–2668. doi:10.2337/dci18-0052
13. Cushman WC, Whelton PK, Fine LJ, et al. SPRINT trial results: latest news in hypertension management. Hypertension. 2016;67(2):263–265. doi:10.1161/HYPERTENSIONAHA.115.06722
14. Bell DS. Hypertension and diabetes—a toxic combination. Endocr Pract. 2008;14(8):1031–1039. doi:10.4158/EP.14.8.1031
15. Adler AI, Stevens RJ, Manley SE, et al. Development and progression of nephropathy in type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS 64). Kidney Int. 2003;63(1):225–232. doi:10.1046/j.1523-1755.2003.00712.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.