")
Back to Journals » Psychology Research and Behavior Management » Volume 14
The Role of Stress Perception and Coping with Stress and the Quality of Life Among Multiple Sclerosis Patients
Authors Kołtuniuk A , Kazimierska-Zając M, Cisek K, Chojdak-Łukasiewicz J
Received 12 March 2021
Accepted for publication 17 May 2021
Published 18 June 2021 Volume 2021:14 Pages 805—815
DOI https://doi.org/10.2147/PRBM.S310664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Aleksandra Kołtuniuk,1 Magdalena Kazimierska-Zając,1 Kinga Cisek,1 Justyna Chojdak-Łukasiewicz2
1Department of Nervous System Diseases, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland; 2Department of Neurology, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Aleksandra Kołtuniuk
Department of Nervous System Diseases, Faculty of Health Sciences, Wroclaw Medical University, Bartla 5, 51-618, Wroclaw, Poland
Tel +48 71 7841805
Fax +48 71 3459324
Email [email protected]
Purpose: Multiple sclerosis (MS) is one of the most common neurological disorders and a cause of disability in young adults. Adequate stress management in MS patients may merit the benefits of both physical and psychological well-being. This study aimed to evaluate the quality of life in MS patients and its correlation with stress levels and coping strategies.
Methods: This descriptive and correlational study was conducted among 109 patients diagnosed with relapsing-remitting MS (RRMS). The study was based on a questionnaire designed by the authors and the following standardized questionnaires: the Perceived Stress Scale (PSS-10), the Inventory for Measuring Coping with Stress (Mini-COPE), and the Multiple Sclerosis International Quality of Life Questionnaire (MusiQoL).
Results: Data analysis showed that 47.71% of the patients experienced a high level of stress, and the most often used strategies under challenging situations included seeking emotional support (2.11) and active coping (1.96). Also, it showed that when the level of stress is higher, the QOL in all domains is lower. Coping strategies such as sense of humor, turning to religion, self-distraction, denial, venting, substance use, behavioral disengagement, and self-blame are negatively correlated with the quality of life of MS.
Conclusion: Quality of life in MS patients is negatively affected by a higher level of perceived stress. The use of coping strategies such as active coping, positive reframing, acceptance, and seeking emotional and instrumental support is positively correlated with the quality of life of MS patients.
Keywords: multiple sclerosis, stress perception, coping with stress, quality of life
Introduction
Multiple sclerosis (MS) is one of the most common neurological disorders and a cause of disability for young adults. It is a chronic, progressive, inflammatory, and demyelinating disease of the central nervous system that increases incidence and prevalence globally.1,2 Based on the third edition of Atlas Reports is estimated that in the world live over 2.8 million patients with MS (35.9 per 100,000 population). Most people with MS are diagnosed between the age of 20 and 40.3 Pediatric MS is rare and makes up approximately 2–10% of total patients with MS.4 The disease affects women two to three times more than men.5,6
The etiology of MS is still unknown.7 A genetic predisposition with specific HLA-DRB1*15 region and many factors are involved in the pathogenesis of the disease.6,8–10 The pathology of MS is characterized by two main processes inflammation and neurodegeneration.11 The symptoms of the disease are varied and depend on which areas of the brain or spinal cord are affected.12,13 Typical signs of MS include loss of motor and sensory function, the problem with bowel or bladder control, sexual dysfunction, fatigue, blindness due to optic neuritis, diplopia, imbalance, cognitive impairment, and emotional changes. The most common subtype of MS is a relapsing-remitting form (RRMS), which accounts for approximately 80% of all MS cases. The RRMS is characterized by relapse (acute neurological symptoms) and periods of relative clinical stability (remissions).14,15
The patients with MS have a lower quality of life (QOL) comparing to a healthy population.16,17 The low QOL depends on multiple factors, especially chronic disease, fatigue, pain, and cognitive impairments. One of the factors that play a primary role in the quality of life is stress.18 Based on the probably first definition proposed by Hans Selye, stress is a non-specific response of the body to any demand.19,20 Cohen et al21 defined stress as a process in which environmental factors strain an organism’s adaptive capacity resulting in both psychological demands and biological changes. Stressors factors can be different, including an event in the environment or psychological consequences. Stress is every fact of life or disease that we must all deal with. According to the DSM-IV definition, acute stress occurs after months of exposure to a traumatic event and has a significant impact on the person.22
The stress is chronic when the exposure to stressor factors continues above 48 hours. Responses to stress are ultimately based on the predispositions of the individual organism. The connection between stress and MS is well known and complex.23–26 Many studies suggest that stress is more common in patients with MS than in the general population.27 Firstly, newly diagnosed MS patients commonly experience increased levels of psychological distress. During the disease, patients are exposed to many stressors, such as the unpredictability of disease, symptoms, the risk of relapse, the side effects of treatment, changes in interpersonal relationships, daily activities, and employment.28 Some studies demonstrated that patients with MS with higher levels of disability had higher stress intensity29,30 Some symptoms (like pain, fatigue) are not visible to other people and can cause people with MS to feel misunderstood by others. These problems in daily life can lead to anxiety and depression symptoms and affect the quality of life.17,31,32 Many patients with MS feel a connection between stress life and the course of the disease.
Most patients believe that stress can cause exacerbations.33 Some studies showed the association between stress and worsening disease34,35 The association between stress and the exacerbation of neurological symptoms is well documented. Golan et al36 demonstrated that war stress was associated with increased risk for MS exacerbations. Also, Mohr et al33 suggest that is an association between MS exacerbation and stressful life events. Some studies report exacerbations after several weeks after the onset of stress.24,37,38 Stressful events or perceived stress may be linked to the development of new Gd+ MR lesions.39 In the study of Burns et al40 showed that major negative, stressful events were associated with increased risk for subsequent Gd+ and new or enlarging T2 lesions, while positive stressful events were associated with decreased.
This relationship is followed by stress-induced inflammatory factors (eg, TNFa, IFNg), which influence the nerve conductance of demyelinated axons.35,41 The influence of stress on the disease course could be explained by alterations in the stress-response systems of the hypothalamic-pituitary-adrenal axis and autonomic nervous system.42,43 In MS, the hypothalamic-pituitary-adrenal axis hyperactivity is observed, reducing the sensitivity of lymphocytes on glucocorticoid.44 The research suggests that psychological and neural stress impact neurodegeneration and may lead to atrophy of grey matter in MS patients. In the study Meyer-Arnst45 based on results of functional MRI, the stress was negatively related to brain atrophy. Some studies have shown that disease-related chronic stressors do not increase the possibility of attacks in MS patients than acute stressors, creating more pressure and having a more significant impact.46 Also, in contrast to other publication Nisipeanu et al47 found that stress was connected with decreased risk of exacerbation.
Patients with MS have developed a lot of techniques and strategies for taming stress. Adequate stress management in MS patients may merit benefits of both physical and psychological well-being. The ability of a patient to control the stress by leading a healthy life and avoiding stressful situations, and modify their behavior and reaction to stressors is crucial.48 Much sleep, physical activity (like yoga, tai chi), thinking patterns, relaxation, deep breathing are the stress reducers.49 The ability to relax during exposition on stress factors is connected with higher QOL and lower level of anxiety and depression in patients with MS50,51 Some studies showed evidence of these strategies having a positive impact on the physical and mental health of patients with MS.52–55 Progressive muscle relaxation (PMR) and autogenic training, reflexology has a good influence on the health-related quality of life and well-being in MS.56–58 Also, a variety of psychological interventions ranging from mindfulness-based and cognitive-behavioral approaches can improve the quality of life and mental health of patients with MS.59 Patients who use less emotional coping strategies assess their HRQoL highly.60
The factors that contribute to HRQoL in MS are both disease-related and person-specific. High levels of perceived stress and use some coping strategies are the factors that are negatively affecting QoL in MS.61 Their identification is essential; therefore, the aim of the study was the assessment of the quality of life in patients with MS by different independent variables (sex, age, place of residence, marital status, education, the time since the diagnosis) and its association with the level of stress and its management techniques.
Methods
Study Participants
A cross-sectional descriptive design with a questionnaire survey was used. The study included 109 patients with a relapsing-remitting form of MS (RRMS), with a mean age of 37.45 years, treated at a neurological health center in Wroclaw, Poland. Data were collected between December 2019 and March 2020. The study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations for observational studies reporting.
The inclusion criteria were as follows: (1) a confirmed diagnosis of MS based on McDonald Criteria 2010 or 2017 (depending on the time of diagnosis), (2) a stable MS disease without any episodes of relapse within 30 days before the study, (3) being over 18 years old, (4) being treated with a disease-modifying therapy (DMT) (5) written informed consent to participate in the study. The exclusion criteria were as follows: (1) participants without a confirmed diagnosis of MS, (2) participants with a confirmed diagnosis of RRMS but without treatment with first-line DMT, (3) patients unable to follow the test instructions, (4) psychiatric comorbidities, and (5) lack of written consent to participate in the study.
Ethical Considerations
The research project was approved by the Bioethics Committee of Wroclaw Medical University, Poland (permission no. KB–10/2020). Participation in the study was anonymous and voluntary. All patients were informed about the study, and their written consent to participate in the study was required. The study was carried out following the Declaration of Helsinki and Good Clinical Practice guidelines.
Data Collection
The respondents were qualified to participate in this study based on the inclusion and exclusion criteria during each check-up visit to the neurological center, where they received their DMTs for the next month. Afterward, they received traditional self-administered pencil-and-paper questionnaires, designed to be completed in approximately 20 minutes. Researchers also gained access to the complete medical records of the patients. A total of 125 surveys were returned, but only 109 were completed correctly.
Research Tools
In the study, the diagnostic survey method was used, along with the authors’ questionnaire (AQ), as well as the following standardized questionnaires: the 10-item Perceived Stress Scale (PSS-10),62 the Inventory for Measuring Coping with Stress (Mini-COPE),63 and the Multiple Sclerosis International Quality of Life Questionnaire (MusiQoL).64
Authors’ Questionnaire (AQ)
The questionnaire included a survey designed by the authors, which comprised questions concerning socio-demographic data (ie, sex, age, place of residence, marital status, education) and clinical data (ie, time from the diagnosis and duration of DMT).
10-Item Perceived Stress Scale (PSS-10)
In the Polish adaptation,62 it is a research tool that employs self-report to measure the degree to which situations in one’s life are considered stressful. The scale consists of 10 questions describing subjective feelings related to personal problems, emotional states, current levels of experienced stress, and possibilities of controlling one’s own life. Individual scores on the PSS range from 0 to 40, with higher scores indicating greater perceived stress. After transformation into standardized sten scores, results from 1 to 4 sten scores are considered low perceived stress, from 7 to 10 as high, and 5 and 6 as average perceived stress. Cronbach’s alpha for the Polish version is 0.86, and for the original PSS-10, 0.84.
Inventory for Measuring Coping with Stress (Mini-COPE)
In order to determine stress-coping strategies, the Polish version of the MiniCOPE was applied.63 The Mini-COPE consists of 28 statements, which are divided into 14 categories of coping with stress: active coping, planning, positive reframing, acceptance, sense of humor, turning to religion, seeking emotional support, seeking instrumental support, self-distraction, denial, venting, substance use, behavioral disengagement, and self-blame.
Multiple Sclerosis International Quality of Life Questionnaire (MusiQoL)
The MusiQoL is a research tool aimed at assessing the quality of life of MS patients. It contains 31 questions concerning the patient’s life during the last four weeks, with the following verbal answers: never, rarely, sometimes, often, always, not applicable. The MusiQoL questionnaire makes it possible to assess the quality of life of MS patients in 10 domains: ADL – activities of daily living, PWB – psychological well-being, RFr – relationships with friends, SPT – symptoms, RFa – family relationships, RHCS – satisfaction with the healthcare system, SSL – sentimental and sexual life, COP – coping, REJ – rejection, and Total – overall quality of life.
The quality of life in each domain is expressed by a number, ranging from 0 to 100—the higher the number, the better the quality of life. No norms exist in the case of MusiQoL, and as such, it is impossible to say whether the respondents’ results indicate high or low quality of life; one can only compare the individual domains with each other to identify the areas of the high and low quality of life. The dimensions of the scale exhibited high internal consistency (Cronbach’s alpha between 0.67 and 0.90 for the Polish version).64
Data Analysis
The analysis of quantitative variables (ie, expressed numerically) was conducted by calculating the mean, standard deviation, median, quartiles, minimum, and maximum. The analysis of qualitative variables (ie, not expressed numerically) was performed by calculating the number and percentage of occurrences of each value. The comparison of the values of quantitative variables in the two groups was performed using the Mann–Whitney test. The comparison of the values of quantitative variables in three and more groups was performed using the Kruskal–Wallis test. A post-hoc Dunn’s test was performed to identify statistically significantly different groups when statistically significant differences were detected. Correlations between quantitative variables were analyzed using Spearman correlation coefficient. A significance level of 0.05 was assumed in the analysis. Thus, all p values below 0.05 were interpreted as indicating significant correlations.
Results
Participants’ Characteristics
A total of 109 participants with RRMS took part in the study to evaluate the relationship between stress intensity and coping methods and the quality of life. The most numerous group was composed of females, namely 64.22%, persons aged 31–40 (35.78%), with secondary education (44.04%). The average time from MS diagnosis was 9.63 years, while the drug program participation was 4.71 years. As many as 68.81% of patients declared that they know support groups, while 27.52% regularly use this form of assistance. Detailed characteristics of the study group are presented in Table 1.
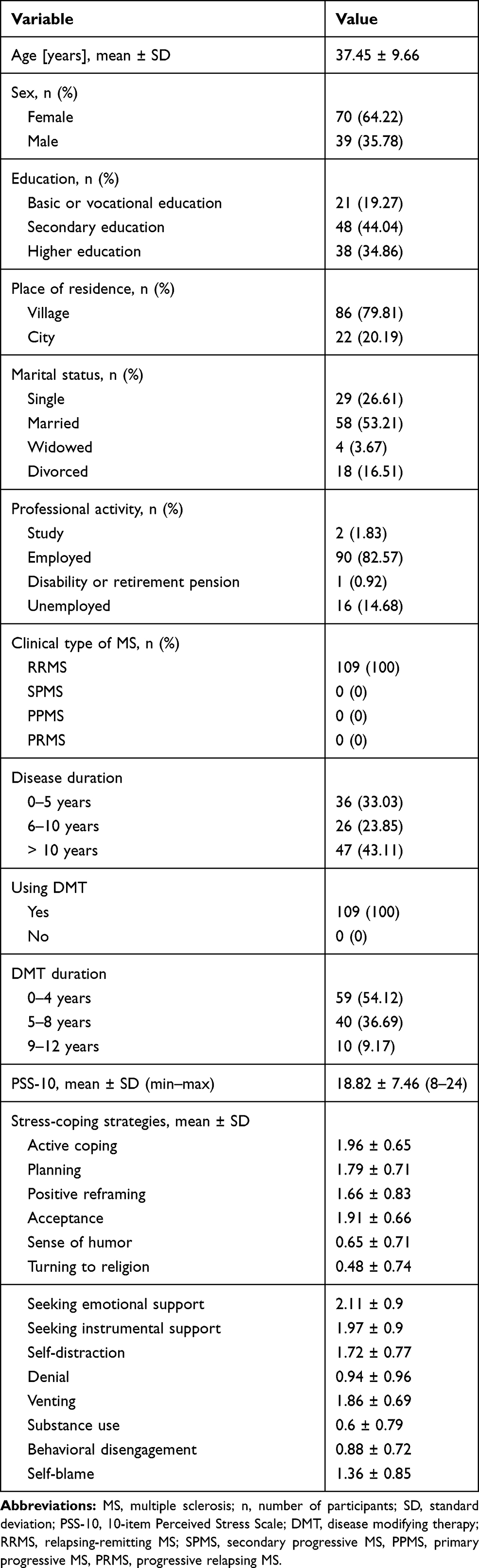 |
Table 1 Characteristics of the Study Group |
Stress Level
Analysis of the obtained data showed that 47.71% of the patients experienced high-stress levels, 34.86% had low-stress levels, and 17.43% experienced moderate stress. We also found that stress level was significantly higher among divorced and widowed individuals (24.77) than singles (18.38) or married persons (17.03) (p=0.001). Non-working individuals experienced more severe stress (22.21) than working ones (18.27); however, the difference was on the borderline of significance (p=0.05). There were no statistically significant differences in the level of stress intensity due to other socio-demographic characteristics.
Stress-Coping Strategies
Analysis of the obtained data showed that under challenging conditions, MS patients most often used the strategies of seeking emotional support (2.11) and active coping (1.96). On the other hand, the least frequently used coping mechanisms included turning to religion (0.48) and substance use (0.6). We also found that: (1) with age, the strategies of positive reframing, sense of humor, turning to religion, seeking instrumental support, denial, venting, substance use, and behavioral disengagement are used more frequently; (2) with more time following the diagnosis, patients are less likely to use the planning strategy; (3) with longer treatment time, patients are more likely to use positive reframing, sense of humor, and seeking instrumental support; (4) females use planning, positive reframing, turning to religion, seeking instrumental support, self-distraction, and venting significantly more often than males; (5) individuals with primary, lower secondary, and vocational education are considerably more likely than those with higher education to turn to substance use; (6) married individuals were significantly more likely to use positive reframing and seeking emotional support than individuals in other groups; (7) residents of rural areas were significantly more likely to turn to substance use than those living in large cities; and (8) professionally inactive individuals were significantly more likely to employ sense of humor, denial, venting, substance use, behavioral disengagement, and self-blame as stress coping strategies (Table 2 and Supplementary Table 1).
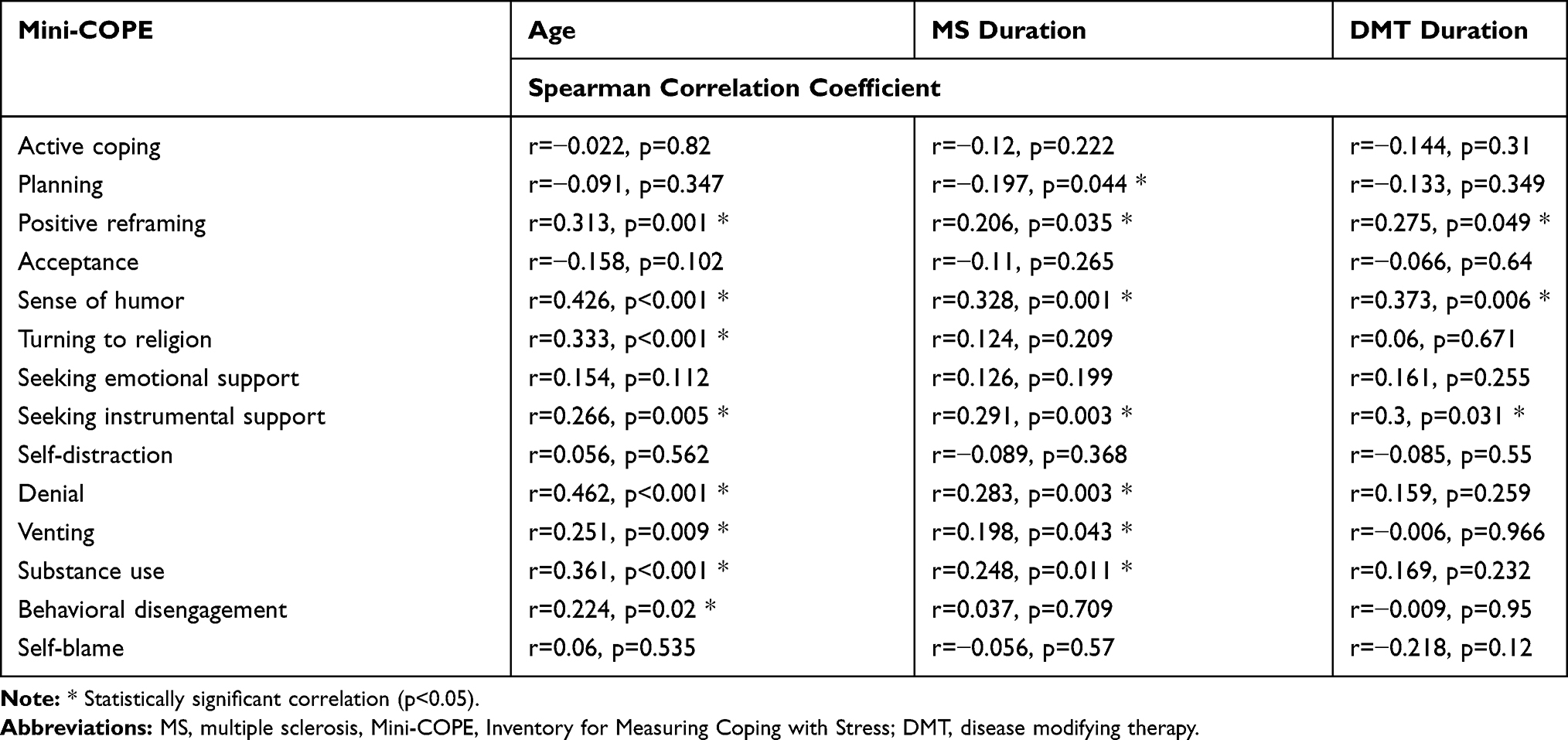 |
Table 2 Correlations Between Age, Disease Duration, DMT Duration and Coping Strategies in MS Patients |
Quality of Life
The overall quality of life index in the study group averaged 65.39 points out of 100 and ranged from 27.43 to 96.18 points (MusiQol). The highest self-rated quality of life included RFa (81.37), RFr (69.83), and REJ (69.04) domains. The lowest quality of life was reported in COP (51.72) and PWB (55.67).
In psychological well-being (PWB) and coping (COP), males reported a higher quality of life than females (64.9 vs 50.45, p=0.001, and 62.18 vs 45.89, p<0.001). Also, age correlates with quality of life scores - the older the patient the lower the quality of life in the MusiQoL total score (r=−0.338, p<0.001), with ADL (r=−0, 3, p=0.002), PWB (r=−0.315, p=0.001), RFr r=−0.369, p<0.001), SPT (r=−0.403, p<0.001), RHCS r=−0.342, p<0.001), and SSL r=−0.268, p=0.005). The quality of life in the domain of sentimental and sexual life (SSL) is significantly higher in those with higher education compared to those with secondary education (72.04 vs 57.29, p=0.038). In all domains except for rejection (REJ), it was significantly higher in unmarried and married individuals than in divorced and widowed persons. Subjects from large cities rated their quality of life in terms of relationships with friends (RFr) (88.1 vs 69.3, p=0.027), family relationships (RFa) (77.68 vs 66.67, p=0.003), satisfaction with the healthcare system (RHCS) (70.83 vs 62.5, p=0.028), and sentimental and sexual life (SSL) (69.64 vs 42.5, p=0.021) significantly higher than those living in rural areas. Quality of life in total MusiQoL (67.37 vs 55.23, p=0.005), ADL (66.42 vs 53.78, p=0.034), PWB (57.44 vs 47.37, p=0.029), RFr (72.13 vs 58.33, p=0.023), SPT (65.1 vs 55.9, p=0.038), RFa (84.47 vs 66.2, p=0.008), and SSL (66.99 vs 44.74, p=0.018) was significantly higher in the professionally active group. We also found that the longer the time from MS diagnosis, the higher the quality of life in REJ (r=0.223, p=0.022) and lower in RFr (r=−0.27, p0.006) and SPT (r=−0.32, p=0.001). Also, the longer the participation in a drug program, the higher the patients rated their quality of life in REJ (r=0.344, p=0.012).
Variable Correlations
The correlations between the PSS 10 questionnaire results and all MusiQoL, Mini COPE questionnaire domains were shown in Table 3. The patients, who more frequently employed active coping, seeking emotional support, and seeking instrumental support, reported a higher quality of life (MusiQoL total). In contrast, patients, who were more likely to use coping strategies such as sense of humor, turning to religion, denial, venting, substance use, behavioral disengagement, and self-blame rated their quality of life lower (MusiQoL total). Detailed data are presented in Supplementary Table 2.
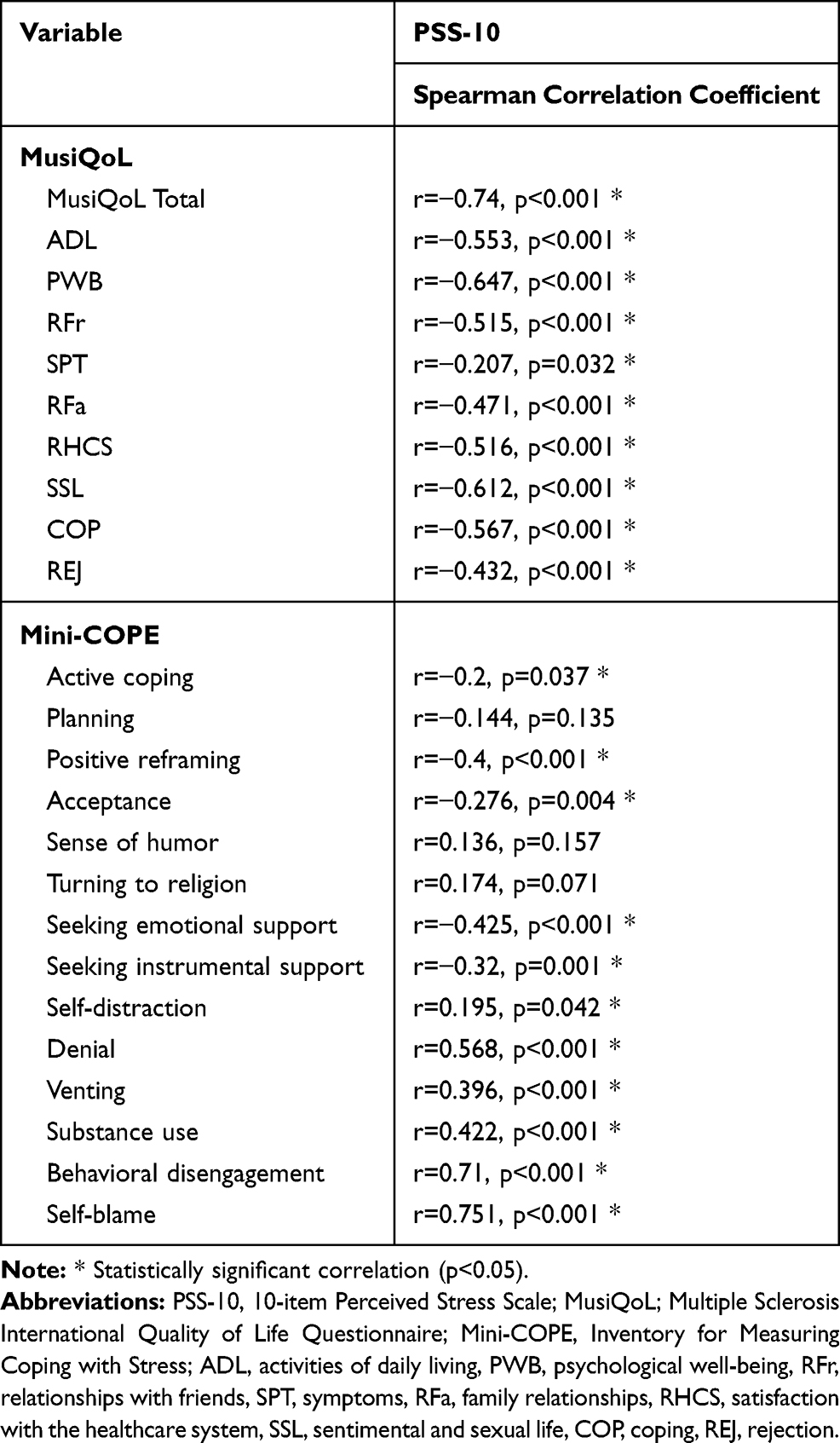 |
Table 3 Correlations Between Stress Intensity Levels and Domains of Quality of Life and Coping Strategies in MS Patients |
Discussion
We investigated whether perceived stress and emotion-related coping strategies may indicate a poor adjustment to MS.65 Patients with MS appear unable to integrate peripheral stress signals into their perception of relaxation.66 Blunted neural and psychological stress processing have a detrimental effect on the course of MS45 and, consequently, can decrease quality of life.
In this study, the mean stress level was 18.88, consistent with the results reported by other authors.67–71 Ifantopoulou72 showed that elderly individuals more often than younger ones and MS patients with tertiary education more frequently than those with secondary education reported significantly higher stress levels. However, this was not confirmed in our study. Among the socio-demographic variables, only marital status and occupational status significantly differentiated the respondents regarding the level of perceived stress.
The data analysis showed that MS patients most often used the strategies of seeking emotional support (2.11) and active coping (1.96). The studies by Holland et al73 and Cornero Contentti et al74 show that the most commonly applied strategies included acceptance and active coping. On the other hand, the least frequently used mechanisms were turning to religion (0.48) and substance use (0.6), which was confirmed in studies by other authors.73,74
The overall quality of life index in the study group averaged 65.39 points out of 100 (MusiQol) and is similar to the results obtained by Farran et al and Nickel et al.77 In contrast, Beltrán et al78 reported a significantly higher score (84.1), and this difference may be since the participants in the Colombia study were characterized by good functional status (low EDDS scores) and short disease duration (average 4.8 years). In our study, the highest self-rated quality of life concerned RFa (81.37), RFr (69.83), and REJ (69.04) domains. In contrast, the lowest quality of life was reported regarding COP (51.72) and PWB (55.67), which is consistent with the results obtained by Koltuniuk et al79 among female MS patients and Farran et al.76 On the other hand, in the validation study of the Polish version of the MusiQoL questionnaire, MS patients scored significantly lower on average – 42.5 points, and they rated their quality of life highest in terms of SPT and lowest in RFa. This difference is likely because all patients included in our study suffered from RRMS and were participating in a drug program that translates into better functional ability and the capacity to participate in family and work-life more actively. Previous studies have also shown a link between socio-demographic variables and specific domains of quality of life in MS patients.64,76,77 For instance, age is negatively correlated with the MusiQoL total score,76 which was also confirmed in our study. Jamroz-Wisniewska et al64 and Nickel et al77 showed that males rated the quality of life in PWB higher than females, which was also confirmed by our study. Our subjects from large cities rated their quality of life in terms of RFr, RFa, RHC, and SSL significantly higher than those living in rural areas. In the study by Jamroz-Wisniewska et al,64 city-dwelling patients had higher scores than their counterparts who lived in rural areas in ADL, PWB, and SPT.
Our study also indicated that the level of perceived stress negatively correlates with the level of quality of life, which is consistent with the results of Senders et al,69 Bishop et al,80 Wollin et al,81 and Strober et al.61
Previous studies have shown that in MS patients, emotion-oriented coping has a negative impact on the quality of life.60,82,83 and was associated with more significant disability.73 Strategies such as behavioral disengagement,61,84 denial,84 self-controlling,75 escape avoidance,75 distancing,75 social withdrawal,85 and wishful thinking85 were also associated with a lower QoL. Our study showed that denial, venting, substance use, and behavioral disengagement strategies were also associated with a lower QoL in MS patients across domains. In contrast, the use of mechanisms based on acceptance and active engagement, such as active coping,61 planning,61 humor,61 problem resolution,85 emotional and instrumental social support,61 and acceptance61,84 were associated with a higher QoL in MS, which was also confirmed in our study.
Frequent use of denial-based coping predicted significantly higher stress severity,84 consistent with our research and research by Somer et al,86 who found that denial coping was related to higher perceived stress and psychological distress. In contrast, higher mental disengagement predicted a higher frequency of stressful events. Also, venting-based coping was significantly correlated with stress severity,84 which was reflected in our research.
Study Limitations
The study group could be more extensive and randomly selected. The tools chosen involve self-assessment, which entails the risk of receiving biased data. This study did not have a control group. The approach of testing multiple associations with multiple bivariate correlation analyses is sensitive to the effects of third variable causation.
Practical Implications
Because MS is a chronic disease that significantly affects both the patient’s physical and psychological functioning, professional care should involve the performance of medical procedures and interventions related to the physical condition and assistance aimed at improving the patient’s psychological well-being. It is not uncommon for patients to experience high-stress levels, which correlate with perceived life satisfaction. Healthcare providers, especially nursing staff, should support the patient in developing the ability to cope with stress because effective coping strategies in challenging situations, conditioned by the health status, positively impact the QOL of MS patients. It also appears that psychological support should concern the patient and include guidance to the medical staff who directly care for the MS patient and who can contribute through their actions to reduce the level of stress experienced by the patient.
Conclusions
QOL in MS patients is negatively affected by a higher level of perceived stress. The use of coping strategies such as active coping, positive reframing, acceptance, and seeking emotional support is positively correlated with the quality of life of MS patients.
Abbreviations
Mini-COPE, Inventory for Measuring Coping with Stress; MS, multiple sclerosis; MusiQoL, Multiple Sclerosis International Quality of Life Questionnaire; PSS-10, Perceived Stress Scale; RRMS, relapsing-remitting MS.
Acknowledgments
There were no other contributors to the article apart from the authors, and no writing assistance was required. We would like to thank the patients for their contribution to this research. The certified English language services were provided.
Funding
This work was supported by the Ministry of Health subventions according to the number of SUB.E020.21.002 from the IT Simple system of the Wroclaw Medical University, Poland.
Disclosure
The authors have declared no conflicts of interest for this work.
References
1. Yamout B, Alroughani R. Multiple sclerosis. Semin Neurol. 2018;38(02):212–225. doi:10.1055/s-0038-1649502
2. Kobelt G, Thompson A, Berg J, et al. New insights into the burden and costs of multiple sclerosis in Europe. Mult Scler J. 2017;23(8):1123–1136. doi:10.1177/1352458517694432
3. Palace J. Making the diagnosis of multiple sclerosis. J Neurol Neurosurg Amp Psychiatry. 2001;71(suppl 2):ii3. doi:10.1136/jnnp.71.suppl_2.ii3
4. Pena JA, Lotze TE. Pediatric multiple sclerosis: current concepts and consensus definitions. Autoimmune Dis. 2013;2013:1–12. doi:10.1155/2013/673947
5. Magyari M. Gender differences in multiple sclerosis epidemiology and treatment response. Dan Med J. 2016;63(3):B5212.
6. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. The Lancet. 2018;391(10130):1622–1636. doi:10.1016/S0140-6736(18)30481-1
7. Doshi A, Chataway J. Multiple sclerosis, a treatable disease. Clin Med. 2016;16(Suppl 6):s53–s59. doi:10.7861/clinmedicine.16-6-s53
8. Dobson R, Giovannoni G. Multiple sclerosis – a review. Eur J Neurol. 2019;26(1):27–40. doi:10.1111/ene.13819
9. Cree BAC. Multiple sclerosis genetics. In: Handbook of Clinical Neurology. Vol. 122. Elsevier;2014:193–209. doi:10.1016/B978-0-444-52001-2.00009-1
10. Sawcer S, Franklin RJM, Ban M. Multiple sclerosis genetics. Lancet Neurol. 2014;13(7):700–709. doi:10.1016/S1474-4422(14)70041-9
11. Lassmann H. Multiple sclerosis pathology. Cold Spring Harb Perspect Med. 2018;8:3. doi:10.1101/cshperspect.a028936
12. Oh J, Vidal-Jordana A, Montalban X. Multiple sclerosis: clinical aspects. Curr Opin Neurol. 2018;31(6):752–759. doi:10.1097/WCO.0000000000000622
13. Ford H. Clinical presentation and diagnosis of multiple sclerosis. Clin Med. 2020;20(4):380–383. doi:10.7861/clinmed.2020-0292
14. Galea I, Ward-Abel N, Heesen C. Relapse in multiple sclerosis. BMJ. 2015;350(apr148):h1765–h1765. doi:10.1136/bmj.h1765
15. Lublin FD. New multiple sclerosis phenotypic classification. Eur Neurol. 2014;72(s1):1–5. doi:10.1159/000367614
16. Patti F, Cacopardo M, Palermo F, et al. Health-related quality of life and depression in an Italian sample of multiple sclerosis patients. J Neurol Sci. 2003;211(1–2):55–62. doi:10.1016/s0022-510x(03)00040-6
17. Łabuz - Roszak B, Kubicka - Bączyk K, Pierzchała K, et al. Jakość życia chorych na stwardnienie rozsiane – związek z cechami klinicznymi choroby, zespołem zmęczenia i objawami depresyjnymi. Psychiatr Pol. 2013;47(3):433–442.
18. Gil-González I, Martín-Rodríguez A, Conrad R, Pérez-San-Gregorio MÁ. Quality of life in adults with multiple sclerosis: a systematic review. BMJ Open. 2020;10(11):e041249. doi:10.1136/bmjopen-2020-041249
19. Selye H. Stress in Health and Disease. Butterworth-Heinemann; 1976.
20. Rom O, Reznick AZ. The stress reaction: a historical perspective. Adv Exp Med Biol. 2016;905:1–4. doi:10.1007/5584_2015_195
21. Cohen S, Kessler R, Gordon L. Strategies for measuring stress in studies of psychiatric and physical disorders. In: Cohen S, Kessler R, Gordon L, editors. Measuring Stress: A Guide for Health and Social Scientists. Oxford University Press; 1995:3-26.
22. Bryant RA, Friedman MJ, Spiegel D, Ursano R, Strain J. A review of acute stress disorder in DSM-5. Depress Anxiety. 2011;28(9):802–817. doi:10.1002/da.20737
23. Benito-León J. Stress and multiple sclerosis: what’s new? Neuroepidemiology. 2011;36(2):121–122. doi:10.1159/000324174
24. Buljevac D. Self reported stressful life events and exacerbations in multiple sclerosis: prospective study. BMJ. 2003;327(7416):646. doi:10.1136/bmj.327.7416.646
25. Mitsonis CI, Zervas IM, Mitropoulos PA, et al. The impact of stressful life events on risk of relapse in women with multiple sclerosis: a prospective study. Eur Psychiatry. 2008;23(7):497–504. doi:10.1016/j.eurpsy.2008.06.003
26. Mohr DC. Stress and multiple sclerosis. J Neurol. 2007;254(S2):II65–II68. doi:10.1007/s00415-007-2015-4
27. Pham T, Jetté N, Bulloch AGM, Burton JM, Wiebe S, Patten SB. The prevalence of anxiety and associated factors in persons with multiple sclerosis. Mult Scler Relat Disord. 2018;19:35–39. doi:10.1016/j.msard.2017.11.003
28. Beier M, Hartoonian N, D’Orio VL, et al. Relationship of perceived stress and employment status in individuals with multiple sclerosis. Work. 2019;62(2):243–249. doi:10.3233/WOR-192859
29. Chrysovitsanou C, Ghika A, Voumvourakis K, et al. Assessing the impact of stress on a series of Greek patients with Multiple Sclerosis (MS). Interscientific Health Care. 2016;8(3):99–107.
30. Senders A, Bourdette D, Hanes D, Yadav V, Shinto L. Perceived stress in multiple sclerosis: the potential role of mindfulness in health and well-being. J Evid-Based Complement Altern Med. 2014;19(2):104–111. doi:10.1177/2156587214523291
31. Łabuz-Roszak B, Niewiadomska E, Kubicka-Bączyk K, et al. Prevalence of pain in patients with multiple sclerosis and its association with anxiety, depressive symptoms and quality of life. Psychiatr Pol. 2019;53(2):475–486. doi:10.12740/PP/94469
32. Łabuz-Roszak B, Kubicka-Bączyk K, Pierzchała K, Machowska-Majchrzak A, Skrzypek M. Fatigue and its association with sleep disorders, depressive symptoms and anxiety in patients with multiple sclerosis. Neurol Neurochir Pol. 2012;46(4):309–317. doi:10.5114/ninp.2012.30261
33. Mohr DC, Hart SL, Julian L, Cox D, Pelletier D. Association between stressful life events and exacerbation in multiple sclerosis: a meta-analysis. BMJ. 2004;328(7442):731. doi:10.1136/bmj.38041.724421.55
34. Strenge H. Zur Beziehung von psychologischem Stress und klinischem Verlauf der multiplen Sklerose - Eine aktuelle Bestandsaufnahme -. PPmP - Psychother · Psychosom · Med Psychol. 2001;51(3/4):166–175. doi:10.1055/s-2001-12378
35. Artemiadis AK, Anagnostouli MC, Alexopoulos EC. Stress as a risk factor for multiple sclerosis onset or relapse: a systematic review. Neuroepidemiology. 2011;36(2):109–120. doi:10.1159/000323953
36. Golan D, Somer E, Dishon S, Cuzin-Disegni L, Miller A. Impact of exposure to war stress on exacerbations of multiple sclerosis. Ann Neurol. 2008;64(2):143–148. doi:10.1002/ana.21409
37. Brown RF, Tennant CC, Sharrock M, Hodgkinson S, Dunn SM, Pollard JD. Relationship between stress and relapse in multiple sclerosis: part I. Important features. Mult Scler J. 2006;12(4):453–464. doi:10.1191/1352458506ms1295oa
38. Ackerman KD, Heyman R, Rabin BS, et al. Stressful life events precede exacerbations of multiple sclerosis. Psychosom Med. 2002;64(6):916–920. doi:10.1097/01.psy.0000038941.33335.40
39. Mohr DC, Lovera J, Brown T, et al. A randomized trial of stress management for the prevention of new brain lesions in MS. Neurology. 2012;79(5):412–419. doi:10.1212/WNL.0b013e3182616ff9
40. Burns MN, Nawacki E, Kwasny MJ, Pelletier D, Mohr DC. Do positive or negative stressful events predict the development of new brain lesions in people with multiple sclerosis? Psychol Med. 2014;44(2):349–359. doi:10.1017/S0033291713000755
41. Heesen C, Mohr D, Huitinga I, et al. Stress regulation in multiple sclerosis – current issues and concepts. Mult Scler J. 2007;13(2):143–148. doi:10.1177/1352458506070772
42. Gold SM, Mohr DC, Huitinga I, Flachenecker P, Sternberg EM, Heesen C. The role of stress-response systems for the pathogenesis and progression of MS. Trends Immunol. 2005;26(12):644–652. doi:10.1016/j.it.2005.09.010
43. Schumann EM, Kümpfel T, Then Bergh F, Trenkwalder C, Holsboer F, Auer DP. Activity of the hypothalamic-pituitary-adrenal axis in multiple sclerosis: correlations with gadolinium-enhancing lesions and ventricular volume. Ann Neurol. 2002;51(6):763–767. doi:10.1002/ana.10187
44. Ysrraelit MC, Gaitán MI, Lopez AS, Correale J. Impaired hypothalamic-pituitary-adrenal axis activity in patients with multiple sclerosis. Neurology. 2008;71(24):1948–1954. doi:10.1212/01.wnl.0000336918.32695.6b
45. Meyer-Arndt L, Hetzer S, Asseyer S, et al. Blunted neural and psychological stress processing predicts future grey matter atrophy in multiple sclerosis. Neurobiol Stress. 2020;13:100244. doi:10.1016/j.ynstr.2020.100244
46. Brown RF, Tennant CC, Dunn SM, Pollard JD. A review of stress-relapse interactions in multiple sclerosis: important features and stress-mediating and -moderating variables. Mult Scler J. 2005;11(4):477–484. doi:10.1191/1352458505ms1170oa
47. Nisipeanu P, Korczyn AD. Psychological stress as risk factor for exacerbations in multiple sclerosis. Neurology. 1993;43(7):1311–1312. doi:10.1212/wnl.43.7.1311
48. Minich DM, Bland JS. Personalized lifestyle medicine: relevance for nutrition and lifestyle recommendations. Sci World J. 2013;2013:1–14. doi:10.1155/2013/129841
49. Can YS, Iles-Smith H, Chalabianloo N, et al. How to relax in stressful situations: a smart stress reduction system. Healthcare. 2020;8(2):100. doi:10.3390/healthcare8020100
50. Southwick SM, Bonanno GA, Masten AS, Panter-Brick C, Yehuda R. Resilience definitions, theory, and challenges: interdisciplinary perspectives. Eur J Psychotraumatology. 2014;5. doi:10.3402/ejpt.v5.25338.
51. Nakazawa K, Noda T, Ichikura K, et al. Resilience and depression/anxiety symptoms in multiple sclerosis and neuromyelitis optica spectrum disorder. Mult Scler Relat Disord. 2018;25:309–315. doi:10.1016/j.msard.2018.08.023
52. Grossman P, Kappos L, Gensicke H, et al. MS quality of life, depression, and fatigue improve after mindfulness training: a randomized trial. Neurology. 2010;75(13):1141–1149. doi:10.1212/WNL.0b013e3181f4d80d
53. Barlow J, Turner A, Edwards R, Gilchrist M. A randomised controlled trial of lay-led self-management for people with multiple sclerosis. Patient Educ Couns. 2009;77(1):81–89. doi:10.1016/j.pec.2009.02.009
54. Bombardier CH, Cunniffe M, Wadhwani R, Gibbons LE, Blake KD, Kraft GH. The efficacy of telephone counseling for health promotion in people with multiple sclerosis: a randomized controlled trial. Arch Phys Med Rehabil. 2008;89(10):1849–1856. doi:10.1016/j.apmr.2008.03.021
55. Hughes RB, Robinson-Whelen S, Taylor HB, Hall JW. Stress self-management: an intervention for women with physical disabilities. Womens Health Issues. 2006;16(6):389–399. doi:10.1016/j.whi.2006.08.003
56. Ghafari S, Ahmadi F, Nabavi M, Anoshirvan K, Memarian R, Rafatbakhsh M. Effectiveness of applying progressive muscle relaxation technique on quality of life of patients with multiple sclerosis. J Clin Nurs. 2009;18(15):2171–2179. doi:10.1111/j.1365-2702.2009.02787.x
57. Sutherland G, Andersen MB, Morris T. Relaxation and health-related quality of life in multiple sclerosis: the example of autogenic training. J Behav Med. 2005;28(3):249–256. doi:10.1007/s10865-005-4661-2
58. Mackereth PA, Booth K, Hillier VF, Caress A-L. What do people talk about during reflexology? Analysis of worries and concerns expressed during sessions for patients with multiple sclerosis. Complement Ther Clin Pract. 2009;15(2):85–90. doi:10.1016/j.ctcp.2008.12.001
59. Agland S, Lydon A, Shaw S, Lea R, Mortimer-Jones S, Lechner-Scott J. Can a stress management programme reduce stress and improve quality of life in people diagnosed with multiple sclerosis? Mult Scler J. 2018;4(4):205521731881317. doi:10.1177/2055217318813179
60. Wilski M, Gabryelski J, Brola W, Tomasz T. Health-related quality of life in multiple sclerosis: links to acceptance, coping strategies and disease severity. Disabil Health J. 2019;12(4):608–614. doi:10.1016/j.dhjo.2019.06.003
61. Strober LB. Quality of life and psychological well-being in the early stages of multiple sclerosis (MS): importance of adopting a biopsychosocial model. Disabil Health J. 2018;11(4):555–561. doi:10.1016/j.dhjo.2018.05.003
62. Juczyński Z, Ogińska-Bulik N. PSS 10. In: Juczyński Z, editor. Narzędzia Pomiaru Stresu I Radzenia Sobie Ze Stresem. Pracownia Testów Psychologicznych; 2009:11–22.
63. Juczyński Z, Ogińska-Bulik. Inwentarz do pomiaru radzenia sobie ze stresem - Mini - COPE. In: Juczyński Z, editor. Narzędzia Pomiaru Stresu I Radzenia Sobie Ze Stresem. Pracownia Testów Psychologicznych; 2009:45–58.
64. Jamroz-Wiśniewska A, Stelmasiak Z, Bartosik-Psujek H. Validation analysis of the polish version of the multiple sclerosis International Quality of Life Questionnaire (MusiQoL). Neurol Neurochir Pol. 2011;45(3):235–244. doi:10.1016/S0028-3843(14)60076-1
65. Dennison L, Moss-Morris R, Chalder T. A review of psychological correlates of adjustment in patients with multiple sclerosis. Clin Psychol Rev. 2009;29(2):141–153. doi:10.1016/j.cpr.2008.12.001
66. Wakonig K, Eitel F, Ritter K, et al. Altered coupling of psychological relaxation and regional volume of brain reward areas in multiple sclerosis. Front Neurol. 2020;11:568850. doi:10.3389/fneur.2020.568850
67. Kołtuniuk A, Pytel A, Kulik A, Rosińczuk J. The role of disease acceptance, life satisfaction, and stress perception on the quality of life among patients with multiple sclerosis: a descriptive and correlational study. Rehabil Nurs off J Assoc Rehabil Nurses. 2020. doi:10.1097/RNJ.0000000000000288
68. Pritchard M, Elison‐Bowers P, Birdsall B. Impact of integrative restoration (iRest) meditation on perceived stress levels in multiple sclerosis and cancer outpatients. Stress Health. 2010;26(3):233–237. doi:10.1002/smi.1290
69. Senders A, Bourdette D, Hanes D, Yadav V, Shinto L. Perceived stress in multiple sclerosis: the potential role of mindfulness in health and well-being. J Evid-Based Complement Altern Med. 2014;19(2):104–111. doi:10.1177/2156587214523291
70. Senders A, Hanes D, Bourdette D, Carson K, Marshall LM, Shinto L. Impact of mindfulness-based stress reduction for people with multiple sclerosis at 8 weeks and 12 months: a randomized clinical trial. Mult Scler Houndmills Basingstoke Engl. 2019;25(8):1178–1188. doi:10.1177/1352458518786650
71. Waliszewska-Prosół M, Nowakowska-Kotas M, Kotas R, Bańkowski T, Pokryszko-Dragan A, Podemski R. The relationship between event-related potentials, stress perception and personality type in patients with multiple sclerosis without cognitive impairment: a pilot study. Adv Clin Exp Med off Organ Wroclaw Med Univ. 2018;27(6):787–794. doi:10.17219/acem/68944
72. Ifantopoulou N, Artemiadis A, Triantafyllou N, Chrousos G, Papanastasiou I, Darviri C. Self-esteem is associated with perceived stress in multiple sclerosis patients. Neurol Res. 2015;37(7):588–592. doi:10.1179/1743132815Y.0000000016
73. Holland DP, Schlüter DK, Young CA, et al. use of coping strategies in multiple sclerosis: association with demographic and disease-related characteristics✰. Mult Scler Relat Disord. 2019;27:214–222. doi:10.1016/j.msard.2018.10.016
74. Carnero Contentti E, López PA, Alonso R, et al. Coping strategies used by patients with relapsing multiple sclerosis from Argentina: correlation with quality of life and clinical features. Neurol Res. 2021;43(2):126–132. doi:10.1080/01616412.2020.1831304
75. Farran N, Ammar D, Darwish H. Quality of life and coping strategies in Lebanese Multiple Sclerosis patients: a pilot study. Mult Scler Relat Disord. 2016;6:21–27. doi:10.1016/j.msard.2015.12.003
76. Farran N, Safieddine BR, Bayram M, et al. Factors affecting MS patients’ health-related quality of life and measurement challenges in Lebanon and the MENA region. Mult Scler J. 2020;6(1):2055217319848467. doi:10.1177/2055217319848467
77. Nickel S, von Dem Knesebeck O, Kofahl C. Self-assessments and determinants of HRQoL in a German MS population. Acta Neurol Scand. 2018;137(2):174–180. doi:10.1111/ane.12854
78. Beltrán E, Díaz D, Díaz C, Zarco L. Quality of life in patients with multiple sclerosis and their caregivers in Colombia: one-year follow-up. Biomédica. 2020;40(1):129–136. doi:10.7705/biomedica.4759
79. Kołtuniuk A, Przestrzelska M, Karnas A, Rosińczuk J. The association between sexual disorders and the quality of life of woman patients with multiple sclerosis: findings of a prospective, observational, and cross-sectional survey. Sex Med. 2020;8(2):297–306. doi:10.1016/j.esxm.2020.02.009
80. Bishop M, Rumrill PD, Roessler RT. Quality of life among people with multiple sclerosis: replication of a three-factor prediction model. Work Read Mass. 2015;52(4):757–765. doi:10.3233/WOR-152203
81. Wollin JA, Spencer N, McDonald E, Fulcher G, Bourne M, Simmons RD. Longitudinal changes in quality of life and related psychosocial variables in australians with multiple sclerosis. Int J MS Care. 2013;15(2):90–97. doi:10.7224/1537-2073.2012-032
82. Brands I, Bol Y, Stapert S, Köhler S, van Heugten C. Is the effect of coping styles disease specific? Relationships with emotional distress and quality of life in acquired brain injury and multiple sclerosis. Clin Rehabil. 2018;32(1):116–126. doi:10.1177/0269215517718367
83. Kristofferzon M-L, Engström M, Nilsson A. Coping mediates the relationship between sense of coherence and mental quality of life in patients with chronic illness: a cross-sectional study. Qual Life Res Int J Qual Life Asp Treat Care Rehabil. 2018;27(7):1855–1863. doi:10.1007/s11136-018-1845-0
84. Grech LB, Kiropoulos LA, Kirby KM, Butler E, Paine M, Hester R. Target coping strategies for interventions aimed at maximizing psychosocial adjustment in people with multiple sclerosis. Int J MS Care. 2018;20(3):109–119. doi:10.7224/1537-2073.2016-008
85. Hernández-Ledesma AL, Rodríguez-Méndez AJ, Gallardo-Vidal LS, Trejo-Cruz G, García-Solís P, de Dávila-esquivel FJ. Coping strategies and quality of life in Mexican multiple sclerosis patients: physical, psychological and social factors relationship. Mult Scler Relat Disord. 2018;25:122–127. doi:10.1016/j.msard.2018.06.001
86. Somer E, Golan D, Dishon S, Cuzin-Disegni L, Lavi I, Miller A. Patients with multiple sclerosis in a war zone: coping strategies associated with reduced risk for relapse. Mult Scler J. 2010;16(4):463–471. doi:10.1177/1352458509358714
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.