")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
The role of salivary sIgA as protection for dental caries activity in Indonesian children
Authors Soesilawati P, Notopuro H, Yuliati Y, Ariani MD, Alwino Bayu Firdauzy M
Received 16 November 2018
Accepted for publication 23 July 2019
Published 2 September 2019 Volume 2019:11 Pages 291—295
DOI https://doi.org/10.2147/CCIDE.S194865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Pratiwi Soesilawati,1 Harianto Notopuro,2 Yuliati Yuliati,1 Maretaningtias Dwi Ariani,3 Muhammad Alwino Bayu Firdauzy4
1Department of Oral Biology, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia; 2Department of Biochemistry, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 3Department of Prosthodontics, Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia; 4Faculty of Dental Medicine, Universitas Airlangga, Surabaya, Indonesia
Correspondence: Pratiwi Soesilawati
Department of Oral Biology, Faculty of Dental Medicine, Universitas Airlangga, Jl. Prof. Dr. Moestopo No. 47 Surabaya, East Java, Indonesia
Tel +62 31 503 0255
Email [email protected]
Purpose: The aim of this study is to asses the relationship between the level of sIgA and dental caries experience in healthy children who are 6- to 9-years-old from Indonesia. The case-control study is conducted to determine the protective role of salivary secretory immunoglobulin A (sIgA) levels in the stimulated whole saliva of dental caries-active and caries-free children.
Methods: This research was done by stimulating the whole saliva which had been collected from 6- to 9-years-old children with the index def-t≥3 of 30 children as the caries-active children group and 30 children with def-t<3 as the low caries-active children group. Saliva samples were collected in sterile vials between 10 am-12 pm due to the circadian rhythm, which is at least one hour after last meal. 1,5 ml of collected salivary sample was centrifuged, then the supernatants was transferred to other tube and stored immediately to the laboratory at a temperature of –20 °C. The estimation of sIgA concentration was done by using ELISA. The differences in the level of sIgA between the two groups with caries were analyzed using the t-test afterward.
Results: The total salivary concentration of sIgA was statistically significantly higher in the low caries-active children group than in the caries-active children group.
Conclusion: The total salivary concentration of sIgA was statistically and significantly higher in the low caries-active children group than caries-active children Group. There is a negative correlation between sIgA level and dental caries activity of 6 to 9-years-old children.
Keywords: sIgA level, ELISA, dental caries, Indonesia
Introduction
Dental caries is an infectious disease that causes health problems in some developed and developing countries. Based on Republic of Indonesia Basic Health Research in 2018, the def-t index in Indonesian children who are 6- to 9-years-old is 92,746.1
The risk of dental caries is controlled by saliva due to the presence of Secretory Immunoglobulin A (sIgA) as an antibacterial substance. Factors that play a role in the development of dental caries are the host response, bacteria in plaque as antigen, quality and quantity of diet, and time. Genetic and environmental factors are considerated to contribute to an increased risk of dental caries. A previous research has shown that there is a relationship between the genetic aspect and the immune response to dental caries.2 Genetic factors have an impact on the introduction of antigen, immune response and dietary patterns. A research on humans and animals proves that genetic differences causes immunomodulatory deviations from antigens in which they play a role in dental caries.4–11
SIgA in saliva has the same role as sIgA in the mucosal immune system. The roles of sIgA includes viral neutralization, neutralization of toxins, as well as growth and colonization of microorganisms in the epithelium or tooth surfaces.7,12,13,14 Rashkova34 classifies sIgA values of examined children with these criteria, up to 100 µg/ml as low sIgA group, medium sIgA in range 100–300 µg/ml and >300 µg/ml as high sIgA group.
Indonesia shows a high prevalence of dental caries with growth tending to increase. The Household Health Survey (SKRT) in 2004 showed that 39% of Indonesians suffered from dental and oral diseases. This study was conducted to predict the response of mucosal immunity to cariogenic bacteria through measurement of salivary titer in 6- to 9-years-old children from Java population in Surabaya Indonesia.
Methods
Study sample
Elementary students who were 6- to 9-years-old in Surabaya, East Java, Indonesia. The subjects were randomly selected from all areas of Surabaya, by dividing the municipality into Central, West, East, North and South region of Surabaya, it was based on the data from the Ministry of National Education in Surabaya. Judgment sample was taken in second grade elementary school in each region.
Clinical examination and evaluation of dental caries
The caries-active population were students with def-t≥3 and low caries-active population was students with def-t<3.3 The sample was 60 children, They were divided into 30 low caries-active children group samples and 30 caries-active children group samples. Samples of saliva were performed on all elementary school students aged 6–9 years who met the inclusion criteria for the def-t test. Then the results of measurements def-t were used as the basis for determining low caries-active children group and caries-active children group by matching the age and sex of two sample groups. If there were students who could not match the criteria, then the student would not be included in the sample group.
Ethical aspect
All students were taken from the same population and ethnicity, Javanese population in Surabaya city. This matching was expected to reduce the possibility of differences in final results. Written informed consent forms were distributed one day before the saliva collection and parents or legal guardians of all participating students were given the written informed consent. All samples have determined several sample criteria. Six- to 9-year-old children, children who had suffered from upper respiratory tract infections in the past week were excluded from the study due to development of IgA and lysozyme. This study was approved by the Health Reseach Ethical Clearance Commission (Universitas Airlangga Faculty of Dental Medicine Number 307/HERCC.FODM/XII/2017).
Method of saliva collection
Stimulated saliva was collected in the morning, between 10 am and 12 pm, one hour after the last meal, this was done in order to prevent circadian rhythm effects at the concentration of saliva samples. Before collecting saliva samples, oral hygiene instruction was given to all students who would be the respondents in this study. The instruction required them to brush their teeth regularly. Moreover, prospective respondents were instructed not to chew anything for an hour before saliva collecting.
ELISA method for determining sIgA level
The sIgA level was examined through indirect ELISA (Immun Diagnostik, K8870) to describe the antigen-antibody reaction in units of ng/ml. SIgA levels were grouped by def-t index. Based on the clinical examination and evaluation of dental caries, we obtain data that the def-t index in this population ranges from 0–5
Results
Total from 60 research subjects, the case group which consists of 30 subject (11 boys and 19 girls) with the mean age of 93.3 months (7.7 years). The control group contained 30 research subjects (11 boys and 19 girls) with the mean age of 9.33 months (7.9 years). The sex and age data distribution in the total subject research is shown in Table 1.
 |
Table 1 Distribution of sex and age in the low caries-active children group and the caries-active children group |
Def-t index in low caries-active children group and caries-active children group
The def-t index is the index that describes the severity of dental caries in the early teeth, it is measured using WHO standards. Based on results of intra-oral examination in 60 samples, we have grouped samples into caries-active children group with def- index t≥3 and low caries-active children group with def-t index <3. Data of def-t index from the two groups are shown in Table 2.
 |
Table 2 Def-t index in low caries-active children group and caries-active children group |
SIgA level on low caries-active children group and caries-active children group
The result of sIgA titer assessment through ELISA testing on saliva samples based on the variety of def-t index valued by intra-oral assessment is shown in Table 3.
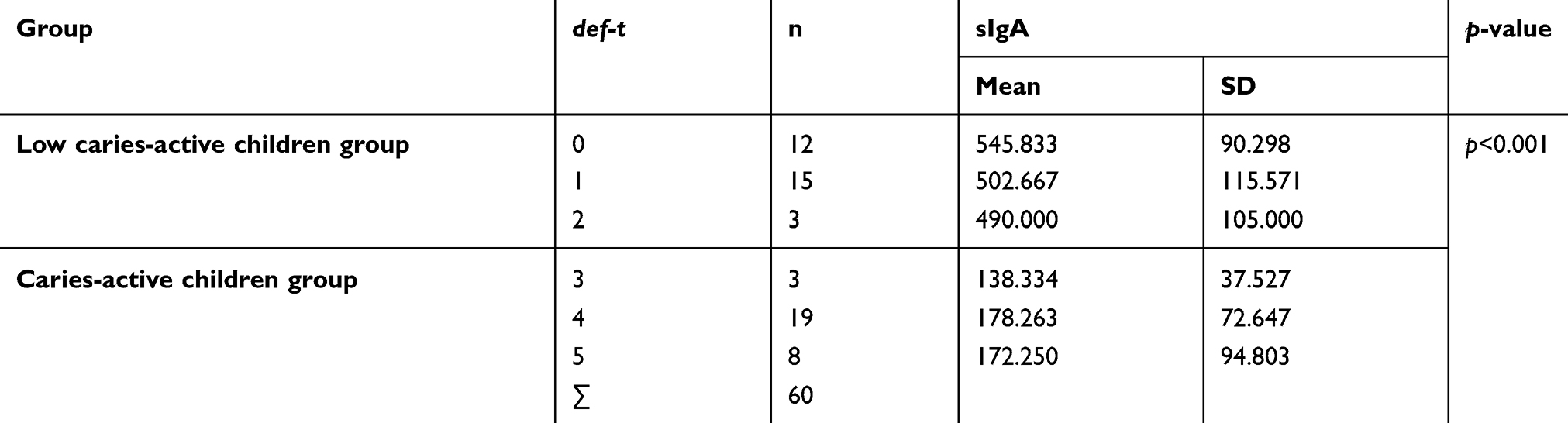 |
Table 3 SIgA titer assessment through ELISA testing on saliva samples based on the variety of def-t index value |
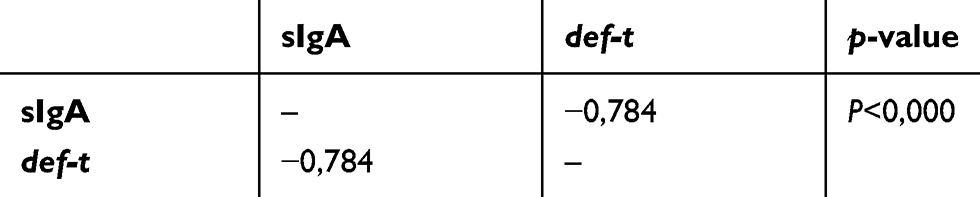 |
Table 4 Correlation between the sIgA level and def-t index |
Correlation between sIgA and def-t index
There is a significant correlation between sIgA level and def-t index by −0,784. This correlation value reveals an inverse relationship between sIgA level and def-t index, in which the higher the def-t index value the lower the sIgA level, and vice versa. Correlation between the two groups are shown in Table 4.
Discussion
The study has been conducted on 60 subjects who have met the Declaration of Helsinki standard with the saliva as an analysis unit. Dental caries is an infectious disease with multifactorial causes that occurs in many populations of both developing and industrialized countries. Caries is more common in low socioeconomic groups, this is influenced by educational background and opportunities for health care15 The etiology of caries is influenced by host, environmental, and time factors. In particular, environmental factors are influenced by the accumulation of oral and dietary bacteria. Host factors are influenced by genetic variations of control of antibody secretion in saliva, and genetic variations in locus which takes control of the formation of the hard tissue of teeth, including amelogenin, enamelin and tuftelin.16
The role of sIgA in the oral cavity is to prevent the adhesion of S. mutans to the surface of the tooth, thus glucan is not formed and inhibits the demineralization process of hard tooth tissue. Various studies have shown that low sIgA levels in the oral cavity has implications for high caries risk, whereas high sIgA levels lead to low caries risk.1,17,18
The use of cut off in this study was def-t <3 in the low caries-active children group and def-t≥3 in the caries-active children group. It is based on previous studies that the increased levels of s-IgA in caries-active children might be a defensive mechanism to the number of S. mutans in whole saliva of caries-active children.32
As previously explained, the correlations relate to the role of saliva in dental caries. The secretion of sIgA from gingival crevicular fluid and the presence of sIgA in saliva play a role in the caries pathogenesis. Salivary gland hypophysis has an effect on the rate of saliva flow and also affects the development of dental caries. In addition, Several studies have reported the fact that treatment with psychopharmaceutic drugs and unregulated diabetes treatment have an effect on the decrease of saliva flow rate.19–21
The relationship between carbohydrate diet and dental caries is difficult to predict. If a person consumes a large amount of sugar while at the same time also consuming fluoride treatments, the sugar consumption does not damage the tooth tissue.22–25
The history of dental caries for mothers might increase the risk of caries for their children and the caries history in the early tooth phase is a prediction of caries in the permanent dental phase.26–30 Age affects dental caries due to mucosal immunity to cariogenic bacteria played by sIgA which is in line with body immunity maturity. The measurement of child immunity is recommended over 6-years-old because the immune system is considered to be complete at this age.31
Dental caries remains a common dental health problem and often found in early childhood, between the ages of one and six years. Children of preschool age are one of the most vulnerable groups to dental and oral disease because generally they do not properly maintain their oral health. Parental care is an important factor as it serves as the basis of the formation of behaviors that support, or not, childhood oral hygiene. Prevention and management of dental caries in children need special concern. Mothers' beliefs about the importance of maintaining children’s dental health is the main principle in the development of early childhood caries.35,36
Conclusion
The total salivary concentration of sIgA is statistically and significantly higher in the low caries-active children group than caries-active children group. There is a negative correlation between sIgA level and dental caries activity in 6- to 9-year-old children. As can be seen, sIgA levels of stimulated saliva has some roles, one of them is as protection against dental caries. Further research is needed on the effect of sIgA as protection against the activity of dental caries, with various tests and increasing the number of samples. Long term studies should be conducted to investigate sIgA levels and dental caries with different def-t indexes.
Acknowledgments
We would like to thank the parents and children who participated in this study. Furthermore, We thank Taufan Bramantyo BDS., DDS., MSc, PhD and Gilang Rasuna Sabdho Wening BDS., DDS., MSc, for assistance with statistical analysis. we also want to thank my beloved brother Agus Prabowo who facilitated the implementation of this study, may he rest in peace.
The study was financially supported by Ministry of Research, Technology and Higher Education, Republic of Indonesia (Grant no. 004/ADD/SP2H/LT/DRPM/VIII/2017).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kesehatan K. Riset Kesehatan Dasar (Riskesdas). Indonesia: Kemenkes; 2018.
2. Senpuku H, Yumiko M 2004. Method for examining the caries risk, United States Patent 20040132071.
3. Badabaan GM, Arafa AA. The relationship between salivary IgA level and dental caries in healthy school-aged children in Makkah Al-Mukarramah. 2017. Available from: http://www.ijhsr.org/IJHSR_Vol.7_Issue.6_June2017/20.pdf. Accessed August 28, 2019.
4. Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;21(19):3–8.
5. Acton RT, Dasanayake AP, Harrison RA, et al. Associations of MHC genes with levels of caries-inducing organism and caries severity in African-American women. Hum Immunol. 1999;60:984–989.
6. Pinkham JR. Pediatric Dentistry: Infancy through Adolescence. St. Louis, Mo: Elsevier Saunders; 2005.
7. Munns C, Zacharin MR, Rodda CP, et al. Prevention and treatment of infant and childhood vitamin D deficiency in Australia and New Zealand: a consensus statement. Med J Aust. 2006;185(85):268–272.
8. Kindt TJ, Osborne BA, Goldsby RA. Kuby Immunology.
9. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369(9555):51–59. doi:10.1016/S0140-6736(07)60031-2
10. Barros SP, Offenbacher S. Epigenetics: connecting environment and genotype to phenotype and disease. J Dent Res. 2009;88(5):400–408. doi:10.1177/0022034509335868
11. Harris NO, García-Godoy F, Nathe CN. Primary Preventive Dentistry. Upper Saddle River, N.J.: Pearson; 2009.
12. Robinett CC, Giansanti MG, Gatti M, Fuller MT. TRAPPII is required for cleavage furrow ingression and localization of Rab11 in dividing male meiotic cells of drosophila. J Cell Sci. 2009;122(24):4526–4534. doi:10.1242/jcs.054536
13. Mestecky J, Lamm ME, Strober W, Bienenstock J, mcghee JR, Mayer L. Mucosal Immunology.
14. Abbas AK, Lichtman AH. Basic Immunology: Function and Disorders of the Immune System.
15. Senpuku H. Inhibitory effects of moabs against a surface protein antigen in real-time adherence in-vitro and recolonization in-vivo of Streptococcus mutans. Scand J Immunol. 2001;54:109–116.
16. Ettinger RL. Epidemiology of dental caries: a broad review. National Institutes of Health. Diagnosis and management of dental caries throughout life. Bethesda, Md.: National Institutes of Health. Dent Clin North Am. 2001;43(4):679–694.
17. Amerongen AN, Ligtenberg AJM, Veermen ECI. Implications for diagnostics in the biochemistry and physiology of Saliva. Ann N Y Acad Sci. 2007;1098(1):1–6. doi:10.1196/annals.1384.033
18. Lehner T. Imunologi Pada Penyakit Mulut. Translate by Farida and Suryadana.
19. Van Wallace MC
20. Fox PC, van der Ven PF, Sonies BC, Weiffenbach JM, Baum BJ. Xerostomia. Evaluation of a symptom with increasing significance. JADA. 1985;110(4):519–525. doi:10.14219/jada.archive.1985.0384
21. Navazesh M. Salivary gland hypofunction in elderly patients. J Calif Dent Assoc. 1994;22(3):62–68.
22. Leone CW, Oppenheim FG. Physical and chemical aspects of saliva as indicators of risk for dental caries in humans. J Dent Educ. 2001;65(10):1054–1062.
23. Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dent Educ. 2001;65(10):1017–1023.
24. Tinanoff N, Douglass J. Clinical decision-making for caries management in primary teeth. J Dent Educ. 2001;65(10):1133–1142.
25. Zero D. Sugars: the arch criminal? Caries Res. 2004;38(3):277–285. doi:10.1159/000077767
26. Tsuha Y, Hanada N, Asano T, et al. Role of peptida antigen for induction of inhibitory antibodies tostreptococcus mutans in the human oral cavity. Clin Exp Immunol. 2004;137:393–401. doi:10.1111/cei.2004.137.issue-2
27. Helm S, Helm T. Correlation between caries experience in primary and permanent dentition in birth-cohorts 1950-70. Scand J Dent Res. 1990;98(3):225–227.
28. Reich E, Lussi A, Newbrun E. Caries risk assessment. Int Dent J. 1999;49(1):15–26.
29. Russell JI, Macfarlane TW, Aitchison TC, Stephen KW, Burchell CK. Prediction of dental caries in Scottish adolescents. Community Dent Oral Epidemiol. 1999;19(2):74–77. doi:10.1111/j.1600-0528.1991.tb00114.x
30. Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J Dent Res. 2002;81(8):561–566. doi:10.1177/154405910208100812
31. Indrawati R. Aktivitas enzim dextranase dan sebaran genotype Streptococcus mutans penderita karies dan bebas karies [Disertasi]. Surabaya: Program Pasca Sarjana Universitas Airlangga; 2006:58–72
32. Ranadheer E, Nayak UA, Reddy NV, Rao VAP. The relationship between salivary IgA levels and dental caries in children. J Indian Soc Pedod Prev Dent. 2011;29(2):106. doi:10.4103/0970-4388.84681
33. Da Silveira Moreira R. Epidemiology of dental caries in the world. In: Oral Health Care-pediatric, Research, Epidemiology and Clinical Practices. Shanghai: IntechOpen; 2012.
34. Rashkova M, Baleva M, Peneva M, Toneva N, Jegova G. Secretory immunoglobulin A and dental caries of children with different disease and conditions influencing oral medium. J IMAB. 2009;2:6–9.
35. Bramantoro T, Tedjosasongk U, Ismail D. Mother’s belief regarding their children’s dental health as a potential predictor of Mother’s dental health attitude for early childhood. J Int Dent Med Res. 2018;11(3).
36. Setijanto RD, Bramantoro T, Palupi R, Hanani A. The role of attitude, subjective norm, and perceived behavioral control (PBC) of mothers on teaching toothbrushing to preschool children–based on the theory of planned behavior: a cross-sectional study. Family Med Prim Care Rev. 2019;21(1):53. doi:10.5114/fmpcr.2019.82974
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.