")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
The role of pain in pulmonary rehabilitation: a qualitative study
Authors Harrison SL , Lee AL, Elliott-Button HL, Shea R, Goldstein RS , Brooks D, Ryan CG, Martin DJ
Received 3 July 2017
Accepted for publication 8 September 2017
Published 8 November 2017 Volume 2017:12 Pages 3289—3299
DOI https://doi.org/10.2147/COPD.S145442
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Samantha L Harrison,1 Annemarie L Lee,2–4 Helene L Elliott-Button,1 Rebecca Shea,5 Roger S Goldstein,2,3,6 Dina Brooks,2,3 Cormac G Ryan,1 Denis J Martin1
1School of Health and Social Care, Teesside University, Middlesbrough, UK; 2The Department of Respiratory Medicine, West Park Healthcare Centre, Toronto, ON, Canada; 3Department of Physical Therapy, University of Toronto, Toronto, ON, Canada; 4School of Allied Health, College of Science, Health and Engineering, La Trobe University, Melbourne, VIC, Australia; 5The Rehabilitation Centre, South Tees Hospital NHS Foundation Trust, James Cook University Hospital, Middlesbrough, UK; 6Department of Medicine, University of Toronto, Toronto, ON, Canada
Introduction: One third of individuals with chronic obstructive pulmonary disease (COPD) report pain. To help inform a COPD-specific pain intervention, we explored the views of health care providers (HCPs) and individuals with COPD on pain during pulmonary rehabilitation (PR).
Methods: This is a qualitative study using inductive thematic analysis. Eighteen HCPs familiar with PR and 19 patients enrolled in PR participated in semi-structured interviews. Demographic data were recorded, and the patients completed the Brief Pain Inventory (Short Form).
Results: 1) Interaction between pain and COPD: pain is a common experience in COPD, heightened by breathlessness and anxiety. 2) Pain interfering with PR: a) Communicating pain: HCPs rarely ask about pain and patients are reluctant to report it for fear of being removed from PR. b) PR is a short-term aggravator but long-term reliever: although pain limits exercise, concentration, and program adherence, PR may reduce pain by increasing muscle strength and improving coping. c) Advice and strategies for pain: some attention is given to pain management but this is often counterproductive, encouraging patients to cease exercise. 3) An intervention to manage pain: HCPs were enthusiastic about delivering a pain intervention within their knowledge and time constraints. Early group education was preferred.
Conclusion: A pain intervention seems warranted in PR and may improve adherence and therefore clinical benefit. A pain intervention could be provided as part of PR education with HCP training.
Keywords: COPD, pain, qualitative, health care professions, education, pulmonary rehabilitation
Introduction
Although breathlessness is the most common symptom in chronic obstructive pulmonary disease (COPD), there is an increasing awareness of pain in this population with a prevalence of 66% in older people with COPD1 compared to 25% in those without COPD.2 The pathophysiology of pain is complex, and the details are rarely reported, but osteoporosis and osteoarthritis are identified risk factors.3
Pulmonary rehabilitation (PR) is recommended to address breathlessness, diminished exercise capacity, psychological symptoms, and health-related quality of life.4 Endurance-based exercise training is the cornerstone of PR, and the presence of pain has been reported to inhibit patients’ ability to successfully complete the training program.5 For some patients, dyspnoea on even light exercise elicits pain.6
Given the high prevalence of comorbidities in COPD,7 the association between pain and reduced physical function8 as well as the influence of breathlessness on pain,6 it is not surprising that patients describe pain as negatively affecting exercise training in PR.9
Considering the adverse influence of pain in COPD, a pain intervention has the potential to improve function. To develop such an intervention, it is important to understand the views of health care providers (HCPs) and individuals with COPD on pain within the context of PR. The aims of this study were twofold: 1) to explore the views of HCPs, responsible for delivering PR, on pain in individuals with COPD and 2) to understand the opinions of patients enrolled in PR on the impact and influence of pain and to explore whether they feel their pain needs are currently being met.
Methods
Study design
A collaborative, international, qualitative study design was conducted between the UK and Canada. Ethical approval was obtained from Teesside University research ethics committee, the NHS research ethics committee, South Tees Hospital NHS Foundation Trust Research and Development, and The Joint Bridgepoint Health – West Park Healthcare Centre – Toronto Central Community Care Access Centre – Toronto Grace Health Centre Research Ethics Board. All participants provided informed consent.
Participants
Recruitment took place at PR programs within the South Tees Hospitals NHS Foundation Trust, UK, and at West Park Healthcare Centre, Ontario, Canada. Convenience sampling was used to target HCPs responsible for delivering PR and individuals with COPD enrolled in PR programs. Individuals with COPD who reported experiencing pain were considered eligible. Individuals were excluded if they had a respiratory diagnosis other than COPD; did not report pain; or were unable to communicate because of language skills, hearing, or cognitive impairment.
Data collection
Eighteen HCPs completed an interview (seven UK and 11 Canada) and 19 patients (nine UK and 10 Canada) (Figure 1). Recruitment was considered to be complete once data saturation was reached. This occurred following 15 interviews with HCPs and 18 interviews with individuals with COPD and was confirmed in a further three interviews with HCPs and one interview with a patient.
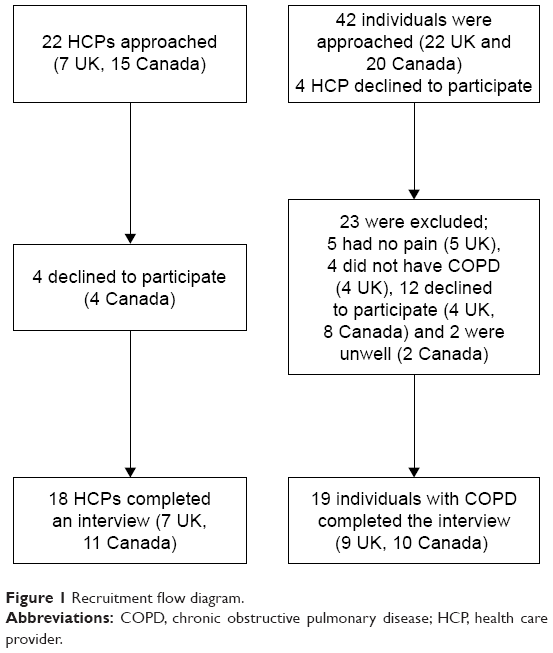 | Figure 1 Recruitment flow diagram. |
Demographic data were recorded and individuals with COPD also completed the Brief Pain Inventory (Short Form) (BPI).10 The BPI consists of nine items and evaluates the severity and impact of pain. Ratings are provided on a 10-point scale ranging from 0 (no pain) to 10 (worst pain). The BPI has high internal consistency and validity in people with COPD.11
Face-to-face semi-structured interviews with HCPs and patients with COPD were performed by two researchers, one at each site. The interviews were held in a quiet space at the hospitals and lasted ~30 minutes. The content of the interview schedules (Supplementary materials) was informed by a previous systematic review1 and a qualitative study.9
Data analysis
The interviews were audio recorded and transcribed verbatim by a professional transcriber. The data were stored and organized using a computer software program (QSR NVivo version 10; QSR International, Doncaster, Australia) and analyzed using inductive thematic analysis (ITA) following the procedure described by Hayes.12 SH completed the initial coding, which involved grouping units of text into categories and provisionally labeling them. Two researchers (SH and HE) completed this step independently for two transcripts, agreeing the categories before SH coded the remaining transcripts. SH and HE reviewed the original transcripts and ensured that the labels and descriptions assigned to each code were accurately supported by the data. Categories were then grouped into emerging themes agreed on by the two researchers. Each data set (HCPs and individuals with COPD) was analyzed separately and presented to other members of the research team (AL, CR, and DM). During this team meeting, relationships were discussed between the themes and the findings from the two data sets were combined.
Findings
Demographic data of HCPs and individuals with COPD are shown in Tables 1 and 2, respectively. Pain-related information of individuals with COPD, including results from the BPI, is given in Table 3.
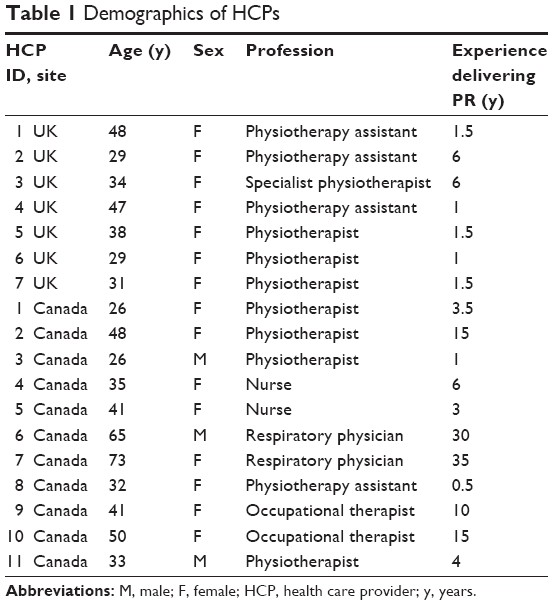 | Table 1 Demographics of HCPs |
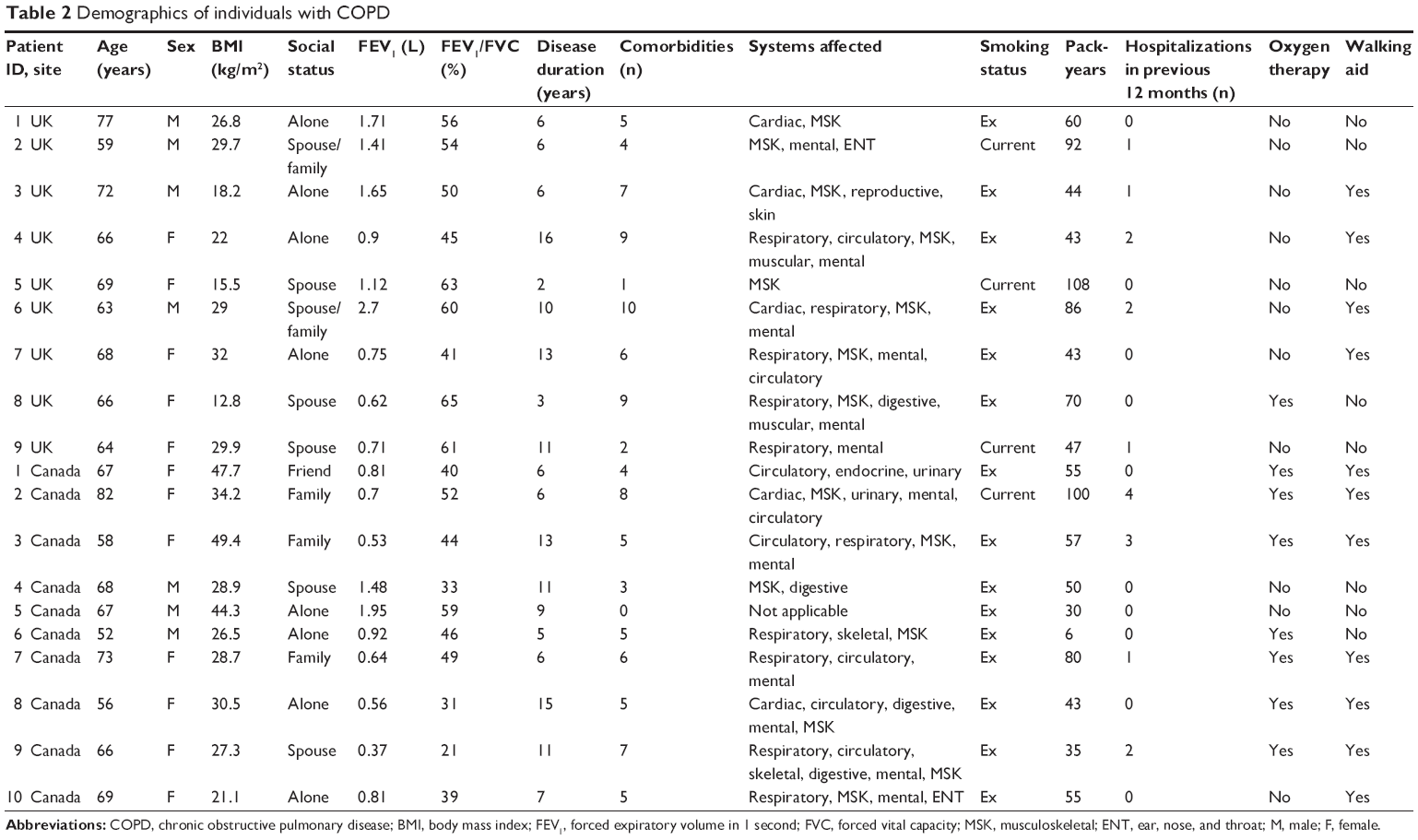 | Table 2 Demographics of individuals with COPD |
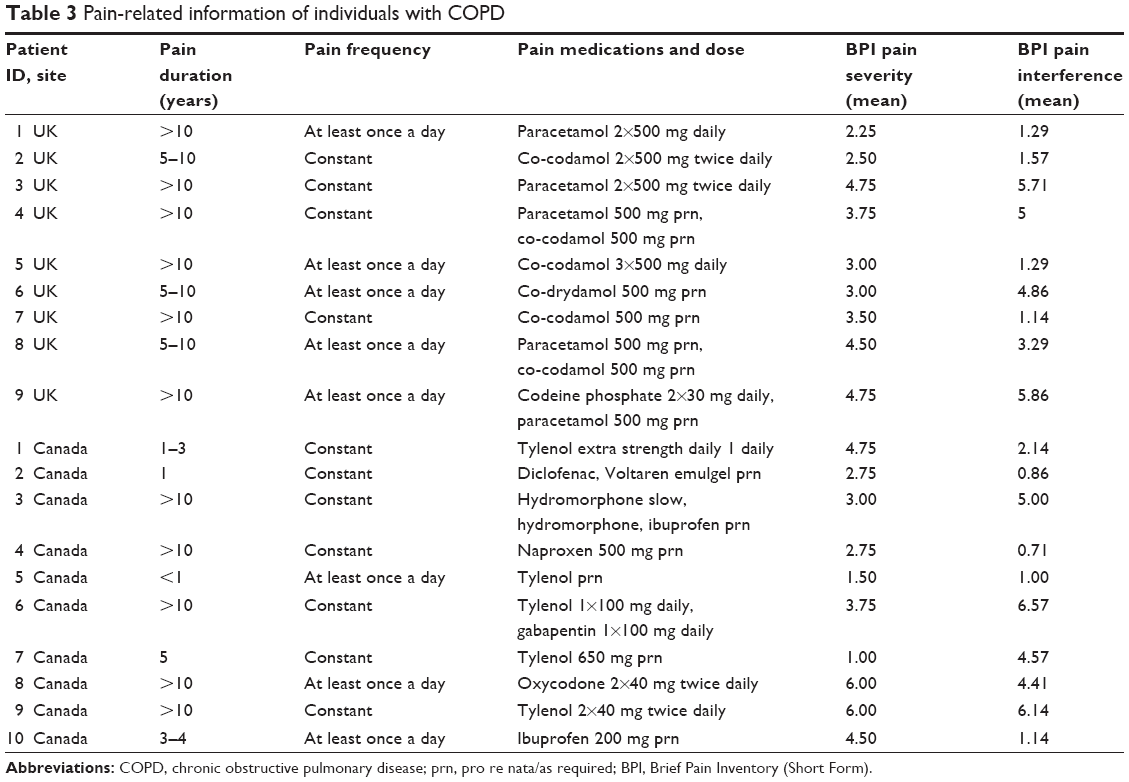 | Table 3 Pain-related information of individuals with COPD |
Three overarching themes were identified from the data: 1) interaction between pain and COPD, 2) pain interfering with PR, and 3) an intervention to manage pain. Nine individuals with COPD also highlighted other benefits of PR, not related to pain. These benefits of PR are well described in the qualitative literature13 and the prevalence and impact of pain has also been documented.1 Therefore, these findings were largely bracketed although they provide context for the individuals’ views.
Interaction between pain and COPD
Pain was identified in a variety of locations, some common in elderly individuals without COPD; back, shoulders, hips, and knees and others more specific to those suffering with COPD; headaches and thoracic pain. Three patients blamed coughing for their thoracic pain:
Most of the pain I have from when I’ve got the COPD is because I’m coughing and I’ve got the ache in the neck and the shoulders and across the back. [Patient 9 UK]
One patient assigned the pain in her neck due to the use of a continuous positive airway pressure (CPAP) mask. The HCPs also assigned rib pain to the effort of breathing and coughing while shoulder and neck pain was described as a consequence of anxiety and tension associated with the increased effort of breathing. Sixteen HCPs considered pain to be related to breathlessness and nine felt that anxiety was an important factor:
Neck and shoulder pain is a big one you know because they get themselves so worked up and then they can’t breath and then they’re using all their muscles in the neck and their shoulders to breath. [HCP 1 UK]
They will say ‘I can’t breathe because I got pain. [HCP 5 Canada]
All but four patients articulated that pain and breathlessness were inter-related, and these patients tended to have greater pain severity according to the BPI:
I’m feeling the pain erm I don’t know whether this is a natural erm reaction or what but I kind of hold my breath. [Patient 1 Canada]
I think if you can sort your breathing out and calm yourself down the pain isn’t as bad. [Patient 8 UK]
Some patients were unclear whether their pain was a consequence of COPD or an independent comorbidity. Not knowing made patients question the legitimacy of pain wondering if it is “all in my head” [Patient 3 Canada].
Those patients who described pain as separate from their COPD had suffered with pain prior to their COPD diagnosis:
That has nothing to do with my erm COPD. Because I’ve had that long before I had COPD. [Patient 2 Canada]
They also commented on the role of other conditions such as arthritis, sciatica, restless leg and angina:
My chest pain er is a mixture of angina and er COPD pain. [Patient 6 UK]
Only two patients articulated that pain was the result of “wear and tear” [Patient 9 UK] associated with aging, although this was overwhelmingly the opinion expressed by HCPs:
Pain tends to come with wear and tear a lot more with age. [HCP 3 Canada]
An acceptance of the reality of living with pain seemed to reduce the emotional impact of pain and improve patients’ ability to cope by removing the element of uncertainty:
I can’t say it makes my life any different […] just something I’ve got used to […] I’ve had it [pain] all my life. [Patient 7 UK]
Pain interfering with PR
Communicating pain
HCPs emphasized that they do not usually enquire about pain:
I don’t generally ask about pain. I ask more open ended questions like is there anything else I need to know about. [HCP 6 Canada]
As a general rule we don’t have a specific question on pain. [HCP 3 UK]
In addition, patients often viewed pain as separate from PR:
Well I well no [to disclosing pain to HCPs] because I’m only here for breathing exercises. [Patient 2 UK]
Both the groups acknowledged patients’ reluctance to communicate pain for fear of it being dismissed, maintaining stoical attitudes, or anticipation that they may be removed from the program:
They might be in chronic pain they just don’t say anything because they think that nobody will care. [HCP 11 Canada]
I’d probably say the older older men and women erm and there quite headstrong, males particularly as well who well they just probably feel embarrassed about erm talking about the pain. [HCP 7 UK]
I don’t want him [HCP] to say ‘okay because you’re injured or you’re hurt then you’re going to have to go home and we’ll have you come back at another time’ you know and I don’t need that. [Patient 5 Canada]
Both HCPs and individuals with COPD described patients’ increased willingness to report their pain to HCPs as the program progressed, emphasizing the necessity of building a rapport with patients:
You build up that little bit of a rapport with them and they do feel like they can come to you and let you know so yeah. [HCP 1 UK]
Patients also described being more likely to communicate their pain to HCPs once they understood the aims of PR:
I don’t really like to talk about it because to me you’re wimping out when I first came here, I don’t feel that way now. [Patient 6 Canada]
HCPs stressed the importance of continually monitoring patients throughout PR:
You know they’re face will say a thousand words and they’ll look, you can tell that they’re in pain. [HCP 6 UK]
PR is a short-term aggravator but long-term reliever of pain
All the HCPs and 18 individuals with COPD reported that pain hindered their ability to participate fully in PR:
They might reach their pain threshold before their shortness of breath. [HCP 11 Canada]
If I walk a lot it really hurts, it’s not just a dull ache, it’s actual hurting. [Patient 2 UK]
A couple of times on the arm circles I’ve thought ‘ooh’ it’s been my shoulders that have hurt not the breathing. [Patient 7 UK]
This was underlined by a strong sense of frustration from patients, emphasized by the use of emotionally charged descriptions:
Trying to do more just angers it more. [Patient 6 Canada]
HCPs considered pain to impact not only on the exercise component of PR but also on patients’ ability to concentrate during education sessions:
When we think of our educational component, erm they sat down for up to thirty minutes, so seating might not be very comfortable. [HCP 3 UK]
If you were to actually test their knowledge they really have not gained that education, based on the pain being a barrier. [HCP 10 Canada]
However, the impact of pain on concentration was only reported by two patients:
This ankle bugged me the last two days, that’s affected my concentration because it’s just been throbbing. [Patient 8 UK]
Patients’ ability and willingness to engage socially with others during the PR program was influenced by pain:
I don’t want people around me. [Patient 9 UK]
It [pain] would affect how they are getting on with other people in the group because they’re kind of talking about their own problems. [HCP 7 UK]
I think it does sort of ah also affect how much they socialise because it affects your mood when you’re in pain. [HCP 4 Canada]
HCPs identified pain as a key contributor to patients’ missing classes, dropping out of the program, or even refusing to attend in the first place:
We’ve had a few patients over the years who have stopped rehab because of the pain escalating. [HCP 10 Canada]
There’s been quite a few kind of drop outs because of pain. [HCP 6 UK]
One HCP indicated that PR was not appropriate for patients with COPD and severe pain:
Of course if the pain is not severe pain, otherwise they should not even come to the programme. [HCP 8 Canada]
Yet, more than half of the patients, experiencing both chronic and incidental pain, voiced the belief that
There’s no gain without pain. [Patient 6 UK]
For these patients, pain was a necessary part of PR, facilitating recovery and improvement.
Patients described PR as a welcome source of distraction from pain:
You usually do maybe 10 minutes on the treadmill but the day that you’re in pain maybe only do 5 minutes but er you’re still doing something and you’re not just sitting there thinking about the pain. [Patient 3 Canada]
HCPs noted that improved muscle strength and a heightened sense of control diminished the impact of pain:
If they persevere I think it can make a big difference, erm because the exercises that we do in pulmonary rehab not only helps to rebuild kind of the strength of respiratory muscles helps with all muscles within the joint [HCP 6 UK]
It gives them confidence that they can actually move with knee pain, or back pain and actually still do some activity, some exercise. [HCP 5 UK]
Advice and strategies for managing pain
Six HCPs acknowledged that their major focus during PR is shortness of breath:
We are so focussed on pulmonary when patients have pains sometimes I don’t believe we deal with it that well. [HCP 1 Canada]
Although fifteen HCPs described adapting exercises for patients suffering with pain:
I’ll modify activities so they’re still maybe using the joint but not in such a wide range. [HCP 1 Canada]
We will like make an easier version of the exercise. [HCP 2 UK]
Almost half of the HCPs will discontinue exercise if it provokes pain:
If they’re in any pain or they look like they’re in pain we ask them to stop. [HCP 4 UK]
Patients value this reassurance and it engenders a sense of safety and trust in HCPs:
‘Well take it easy, don’t overdo it’ and it’s reassuring to hear that because you think well am I just dropping out because I’m hurting or should I really drop out and they do impress on me don’t do anything if it’s hurting. [Patient 3 UK]
He said when it’s when you get the pain and you stop, stop, and you can go back at it tomorrow. [Patient 5 Canada]
In instances where severe pain prevents participation, HCPs report referring patients back to their general practitioner (GP)/family doctor, cementing patients’ concerns about communicating pain, especially if they have already spoken to their GP and found them to be unhelpful in addressing pain. Current advice in PR to manage pain is limited to heat therapy, transcutaneous electric nerve stimulation, prescription of an assistive walking device, and recommendations to take medications before exercise. Patients’ report their own strategies for managing/relieving pain including: bath/shower, rubbing volterol (anti-inflammatory gel) into the affected area, medication, distraction (knitting), relaxation, heat packs and repositioning. It is not clear how these techniques evolved, but it seems to be through the process of trial and error.
An intervention to manage pain
Content
While patients seem to find it difficult to articulate what they would want from a pain intervention, HCPs indicated that it should align with chronic pain management, emphasizing education regarding causes and specific exercises:
I think you know having that education of actually what is pain, why do we get pain, how can we manage pain, I think would be massively beneficial for patients. [HCP 6 UK]
Showing that spine and how it works and how the discs are and what the discs do and you can do certain things and stuff like that so er you focus on that rather than focussing on the pain, where it’s coming from. [Patient 3 Canada]
The usefulness of written information is also highlighted:
Give them resources they can use and help them to access to use resources. [HCP 3 Canada]
Some information that was placed in black and white and I could use it at home. Get something out of it. [Patient 7 UK]
HCPs also cited distraction therapy and mindfulness as potentially useful adjuncts to assist with reducing pain:
I would do more mindfulness like a mindful kind of erm approach and maybe some education about being mindful. [HCP 2 Canada]
Delivery
All interviewees identified PR as an appropriate setting for pain management. The majority of HCPs and patients reported that a pain intervention would be best offered early in the program:
I think yeah at the beginning would be probably be the best. [HCP 9 Canada].
Although others advocated at least starting the program:
People don’t realise how bad they are until they get in the gym and start having to do. [Patient 3 UK]
HCPs and patients preferred a group setting with the opportunity to discuss shared experiences for the delivery of a pain intervention:
I think a group discussion would be appropriate. [HCP 9 Canada]
If you put it into a group I mean more people would open up as well. [Patient 2 UK]
This was combined with one-on-one support as required for more complex pain control issues:
I think it should be in the group situation but be available to actually speak individually. [Patient 9 UK]
I think general principles should be in a group and specific location focussed pain management should be one to one. [HCP 6 Canada]
Interventionist
A multidisciplinary approach to a pain intervention was most frequently recommended by HCPs although most patients identified physiotherapists as the professional most qualified to deliver a pain intervention. Patients criticized other disciplines such as physicians or psychologists as being too rushed and intimidating. Both the groups felt that a pain intervention would be best delivered by respiratory professionals experienced in pain management:
Well somebody who’s obviously trained in pain management. [Patient 3 UK]
Somebody who has a lot of experience working with pain, somebody who has a lot of experience working with people with COPD. [HCP 1 Canada]
Willingness and barriers for a pain intervention
HCPs were enthusiastic but recognized the need for specific training in pain management as well as time constraints:
As much as we treat the whole patient our focus is so much on the cardio-respiratory part of that you kind of forget your MSK stuff. [HCP 1 Canada]
We’d probably need a kind of refresher, I think it would be almost good to have a bit of a training session on what’s the most common conditions your likely to see related to COPD. [HCP 3 UK]
Seventeen patients expressed their willingness to participate in a non-pharmacological pain intervention:
You can put my name right at the top of the list. [Patient 5 UK]
Discussion
This is the first qualitative study exploring the role of pain in PR from the perspectives of HCPs and individuals with COPD. The focus of PR on predominantly addressing symptoms of dyspnea deters a broader enquiry of pain. This plus patients’ fear that pain might render them ineligible for PR results in patients being reluctant to communicate pain at least until later in the program when they have developed a rapport with HCPs. When exercise aggravates musculoskeletal pain, HCPs will modify and limit exercise. In the upper body and thorax, pain may be aggravated by the increased efforts of breathing as well as local muscle tension, in which case attention to both functional and emotional activities contributing to increased ventilation may be valuable. A COPD-specific pain intervention could be delivered as part of the group education sessions during PR, although specific pain management training for HCPs, as well as additional time, would be required.
Notwithstanding the comorbidities of osteoporosis and osteoarthritis, both of which are increased in COPD,7 most patients reported thoracic pain, in keeping with previous reports of the prevalence of thoracic pain between 36% and 54% in patients with COPD enrolled in PR.2,14 Thoracic pain is much less common in the non-COPD population.15 In one study although thoracic pain was associated with worse quality of life, no difference in airflow limitation, lung hyperinflation, or diffusing capacity was observed among COPD patients with or without pain.14 A pain intervention that highlights the interactive relationship between experiences of pain, dyspnea, and anxiety will help patients rationalize how these symptoms interact in COPD.16,17 It will also likely reduce non-completion of PR,5 which is seen as aggravating pain in the short term.
Interestingly although HCPs identified the influence of anxious symptoms on both breathlessness and pain, patients did not make this observation. Similarly, in chronic pain, people often do not link pain and emotions.18 Including an emotional component in a COPD-specific pain intervention is likely important given the inherent role that thoughts and emotions play in pain processing. A recent systematic review of non-COPD studies suggested that an education program alone is more likely to be effective when it is in conjunction with other pain management approaches.17 The emotional contribution to pain is often overlooked by patients and HCPs and needs to be addressed.18
Given its prevalence, a systematic assessment of pain is warranted early in the exercise component and reassessed at the end of the intensive phase. This assessment will result in an intervention plan matched to the severity, duration, and triggers of pain. Approaches will vary depending on the location and underlying pathophysiology of the pain as well as whether it is incidental from injury, in which case reducing activity may be important, or chronic in which case strengthening muscles, reducing ventilation on exertion through increased fitness and addressing attendant psychological impairments would be the preferred approach. For those with chronic pain, instructions to cease exercise are unlikely to be effective and may promote fear-avoidance behavior.19
There are a number of study limitations to note. The HCPs and patients agreeing to the study were more likely to be interested in the symptoms of pain and more enthusiastic about a pain intervention. The two interviewers had different clinical backgrounds, although the inclusion of participants from two different countries strengthens the authenticity of the findings. This study has focused on the non-pharmacological issues, but clearly any non-pharmacological intervention should be balanced with the necessary analgesics and anti-inflammatories. The transcripts were not reviewed to verify accuracy, but the moderate sample size and the inclusion of five researchers (two with experience in PR [SH and AL], one with a psychological background [HE], and two with expertise in pain [CR and DM]) in the analysis enhances rigor.
The impact of pain among patients with COPD enrolled in PR is both unrecognized and unreported. The specific effect of PR on pain has not been formally studied although there is optimism that a combination of improved physical function and improved symptoms of dyspnea, anxiety, emotional function, and mastery will complement a pain intervention. A specific pain intervention would be welcomed by both HCPs and patients. The content of such an intervention should be informed by the views of HCPs and patients on the role of pain in PR.
A pain intervention could be provided early in the PR program by HCPs provided that they received additional training in this area. Such an intervention could be in conjunction with other pain management strategies that link pain and breathlessness. A group setting is preferred for delivery with the option for one-on-one support as necessary.
Acknowledgments
This research was funded by Teesside University Research Funds (grant number 15/10/04). DB holds a Canadian research chair from Canada Research Chairs Program.
Disclosure
The authors report no conflicts of interest in this work.
References
Lee AL, Harrison SL, Goldstein RS, Brooks D. Pain and its clinical associations in individuals with COPD: a systematic review. Chest. 2015;147:1246–1258. | ||
Bentsen SB, Rustoen T, Miaskowski C. Prevalence and characteristics of pain in patients with chronic obstructive pulmonary disease compared to the Norwegian general population. J Pain. 2011;12:539–545. | ||
Bentsen SB, Rustøen T, Miaskowski C. Differences in subjective and objective respiratory parameters in patients with chronic obstructive pulmonary disease with and without pain. Int J Chron Obstruct Pulmon Dis. 2012;7:137–143. | ||
Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188:13–64. | ||
Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8:89–99. | ||
Borge CR, Wahl AK, Moum T. Association of breathlessness with multiple symptoms in chronic obstructive pulmonary disease. J Adv Nurs. 2010;66:2688–2700. | ||
Franssen FME, Rochester CL. Comorbidities in patients with COPD and pulmonary rehabilitation: do they matter? Eur Respir Rev. 2014;23:131. | ||
HajGhanbari B, Holsti L, Road JD, Darlene Reid W. Pain in people with chronic obstructive pulmonary disease (COPD). Respir Med. 2012;106:998–1005. | ||
Lee AL, Harrison SL, Goldstein RS, Brooks D. An exploration of pain experiences and their meaning in people with chronic obstructive pulmonary disease (COPD). Physiother Theory Pract. In press 2017. | ||
Keller S, Bann CM, Dodd SL, Schein J, Mendoza TR, Cleeland CS. Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin J Pain. 2004;20:309–318. | ||
Reid WD, Chen Y-W, HajGhanbari B, Coxson H. Validation of the brief pain inventory in people with chronic obstructive pulmonary disease. Eur Respir J. 2016;48(Suppl 60):PA3735. | ||
Hayes N. Doing Psychological Research. Buckingham, PA: Open University Press; 2000. | ||
Williams V, Bruton A, Ellis-Hill C, McPherson K. The effect of pulmonary rehabilitation on perceptions of breathlessness and activity in COPD patients: a qualitative study. Primary Care Respir J. 2010;19:45–51. | ||
Janssen DJA, Wouters EFM, Parra YL, Stakenborg K, Franssen FME. Prevalence of thoracic pain in patients with chronic obstructive pulmonary disease and relationship with patient characteristics: a cross-sectional observational study. BMC Pulmon Med. 2016;16:47. | ||
Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskel Disord. 2009;10:77. | ||
Clarke A, Anthony G, Gray D, et al. “I feel so stupid because I can’t give a proper answer…” How older adults describe chronic pain: a qualitative study. BMC Geriatr. 2012;12:78. | ||
Geneen LJ, Martin DJ, Adams N, et al. Effects of education to facilitate knowledge about chronic pain for adults: a systematic review with meta-analysis. Syst Rev. 2015;4:132. | ||
Robinson V, King R, Ryan CG, Martin DJ. A qualitative exploration of people’s experiences of pain neurophysiological education for chronic pain: the importance of relevance for the individual. Man Ther. 2016;22:56–61. | ||
Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30:77–94. |
Supplementary materials
Interview schedule – health care providers
- Do you believe pain to be a common symptom in individuals with COPD? What do you know about pain in individuals with COPD? If yes, how do you think it affects them? Locations? Severity?
- A recent systematic review suggests that approximately 66% of individuals with COPD have pain. Does this surprise you? Why?
- Why do you think patients with COPD have pain? Do you think it is associated with their breathlessness?
- Do you think participating in PR makes patients pain better or worse? Why?
- Do you think pain affects patient’s ability to participate fully in PR? How? Please could you provide some examples?
- Do you ask patients about their pain during their initial assessment for PR or during the program? How important do you think it is that HCPs ask about pain? Why?
- Have any patients approached you to talk about their pain? How did you respond? Did you feel able to deal with their issues? What would have made you feel more able to offer advice/treatment?
- Other than the exercises, do you think pain affects any other aspects of PR? How? Education/concentration? Mood/less sociable?
- Can you describe any strategies or techniques which might help patients manage their pain whilst in PR? Education? Talking to a HCP? Specific exercises? Peer support?
- If we were to develop a pain intervention which may consist of some education and specific exercises is this something you would be interested in delivering to individuals with COPD? If not, why not? If yes, what additional training/support would you need, if any?
- Do you think a pain intervention could be delivered within PR or should it be delivered before or after PR? Why?
- Should a pain intervention be delivered in a group or in one-on-one sessions? Why?
I have asked the questions I have, is there anything you would like to add about pain that we haven’t discussed?
Interview schedule – individuals with COPD
- You said that you experience pain which is why you have been invited to take part in this interview, can you please begin by describing your pain? What makes it worse? What makes it better? Is it constant or does it fluctuate? Does it come on gradually or all of a sudden? Where is your pain? How does it affect you?
- Do you think pain is associated with your breathing problems or is it something separate? Why? Does it get worse when you get breathless? Or does your breathlessness get worse when you are in pain?
- Does pain affect your ability to be active and exercise? How? If not, why, how do you overcome this? Describe?
- Do you think participating in PR makes your pain better or worse? Why?
- Do you think your pain affects your ability to participate fully in PR? How? Please could you provide some examples?
- Does pain affect your ability to exercise at home?
- Has anyone in the PR program asked you about your pain? How important do you think it is for healthcare professionals to ask about your pain when you are entering this kind of program? Why?
- Have you talked to anyone in PR about your pain? If not, why not? Health care professional and peers? How did they respond? How did that make you feel?
- Other than the exercises, does pain affect any other aspect of PR? How? Education/concentration? Mood/less sociable?
- Can you describe any strategies or techniques you use to try to manage your pain whilst in PR? How effective are they?
- What do you think might help you manage your pain in PR? Education? Talking to a HCP? Specific exercises? Peer support?
- If we were to develop a pain intervention which may consist of some education and specific exercises is that something you would be interested in participating in? If not, why not? If yes, what would you expect from the intervention? How do you think it would help you?
- Should an intervention of this kind be delivered within PR, before or afterwards? Why?
- Should a pain intervention be delivered in a group or in one-on-one sessions? Why?
- Who do you think should deliver this kind of interventions? Should it be someone in the PR team or someone separate?
I have asked the questions I have, is there anything you would like to add about pain that we haven’t discussed?
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.