")
Back to Journals » Cancer Management and Research » Volume 13
The Role of Neoadjuvant Chemotherapy in Locally Advanced Colon Cancer
Authors Body A, Prenen H, Latham S , Lam M , Tipping-Smith S , Raghunath A , Segelov E
Received 19 November 2020
Accepted for publication 14 February 2021
Published 17 March 2021 Volume 2021:13 Pages 2567—2579
DOI https://doi.org/10.2147/CMAR.S262870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Eileen O'Reilly
Amy Body,1,2 Hans Prenen,1,3 Sarah Latham,1 Marissa Lam,1 Samuel Tipping-Smith,1 Ajay Raghunath,1 Eva Segelov1,2
1Medical Oncology, Monash Medical Centre, Clayton, Melbourne, VIC, Australia; 2School of Clinical Sciences, Monash University, Clayton, Melbourne, VIC, Australia; 3Oncology Department, University Hospital Antwerp, Antwerp, Belgium
Correspondence: Amy Body
Monash Health Translational Precinct, Monash Medical Centre, 246 Clayton Road, Clayton, Melbourne, VIC 3168, Australia
Email [email protected]
Abstract: Neoadjuvant systemic therapy has many potential advantages over up-front surgery, including tumor downstaging, early treatment of micrometastatic disease, and providing an in vivo test of tumor biology. Due to these advantages, neoadjuvant therapy is becoming the standard of care for an increasing number of tumor types. Currently, colon cancer patients are still routinely treated with up-front surgery, and neoadjuvant systemic therapy is not yet standard. Limitations to widespread use of neoadjuvant therapy have included inaccurate radiological staging, concerns about tumor progression while undergoing preoperative treatment rendering a patient incurable, and a lack of randomized data demonstrating benefit. However, there is great interest in neoadjuvant chemotherapy, and a number of trials are under way. Early follow up of the first phase III trial of neoadjuvant chemotherapy for colon cancer demonstrated tumor downstaging and suggested an improvement in disease-free survival with neoadjuvant chemotherapy, and it is hoped that this will translate into longer-term overall survival benefit. Clinicians should closely watch this developing field, consider the option of neoadjuvant chemotherapy for colon cancer patients, and actively seek out opportunities for their patients to participate in ongoing clinical trials to further inform this field in future.
Keywords: colorectal cancer, preoperative chemotherapy, perioperative chemotherapy, staging
Introduction
Chemotherapy for colon cancer was initially used in the metastatic setting and later proven to be of benefit in the postoperative adjuvant setting, reducing the risk of systemic recurrence. The main driver of prognosis for a patient with localized colon cancer is the risk of later distant metastases; therefore, the opportunity to treat up front any potential distant micrometastases at the time of diagnosis may represent the best opportunity to attain long-term cure.
For an increasing number of cancers where treatment is aimed at cure, including early-stage gastric, lung, and bladder cancers, the neoadjuvant approach of chemotherapy or chemoradiation administered prior to definitive treatment (usually surgery) shows superior outcomes to up-front surgery and is the standard of care.1–4 The theoretical benefits of neoadjuvant therapy are multiple, but need to be proven in each tumor type by randomized controlled trials against the current standard (usually up-front surgery and subsequent adjuvant chemotherapy).
Neoadjuvant chemotherapy is not currently a standard treatment for colon cancer, unlike rectal cancer (below the peritoneal reflection), where chemoradiation prior to resection has proven to be of benefit and is the standard of care for locally advanced disease. One reason for this is that adjuvant chemotherapy is not of benefit for all stages of colon cancer, and radiological differentiation between low- and high-risk tumors requires definition and validation in clinical trials, which has recently been achieved.
In the field of rectal cancer, the additional benefit of neoadjuvant systemic chemotherapy added to the current standard neoadjuvant chemoradiation has been shown to improve disease-free survival, and mature data to determine effects on overall survival are eagerly awaited.5,6 The success of this approach, known as total neoadjuvant therapy (TNT) implies that intensification of neoadjuvant chemotherapy for colon cancer is likely to also be of benefit, given the similar biology of these cancer types.
This review aimed to explore the current evidence for neoadjuvant chemotherapy in locally advanced colon cancer. We discuss the practical limitations of current staging modalities, which impact on appropriate patient selection for neoadjuvant treatment. We also discuss ongoing trials and emerging evidence for new agents, such as immunotherapy and targeted therapy, in this setting.
Search Strategy and Selection Criteria
The indexed databases PubMed and Embase were searched for the keywords “colon cancer”, “neoadjuvant chemotherapy”, “neoadjuvant therapy”, “locally advanced”, “staging”, “computerized tomography”, “magnetic resonance imaging”, and “positron-emission tomography”. Medical subject-heading terms used included “colonic neoplasms” and “neoadjuvant therapy.” The ClinicalTrials.gov registry was searched for “neoadjuvant” and “colon cancer” to identify ongoing clinical trials. Relevant papers were included if they had been published in English and specifically addressed the question at hand. This paper was constructed as a narrative review, rather than a systematic review, to allow full discussion of important background details, rather than focusing solely on completed clinical trials.
Definition of Locally Advanced Colon Cancer
For the purposes of clinical trials, locally advanced colon cancer has been defined by radiological T stage, focusing on high-risk T3 (>5 mm extramural invasion to pericolic fat) and T4 primary tumors.7,8 This is for the pragmatic reason that nodal staging is less accurate than T staging with current methods, as well as the clinical rationale that these patients have at least higher-risk stage II disease and thus may benefit from chemotherapy.
Despite the trial definition of “locally advanced” to describe any primary tumor sufficiently advanced to derive benefit from chemotherapy, in much of the literature this term has been used synonymously with T4 colon cancer (ie, tumors invading to the visceral peritoneum or into adjacent structures). This review includes high-risk T3 and T4 disease.
Rationale for Neoadjuvant Chemotherapy
The mainstay of treatment for stage I–III (nonmetastatic) colon cancer remains surgical resection. While local failure rates with surgery are low, systemic disease recurrence (usually equating to incurability) in those with locally advanced disease remains common. Five-year survival rates after surgery alone are 60%–80% for “high-risk” stage II and 30%–60% for stage III colon cancer.9–11 Adjuvant chemotherapy with 5-fluorouracil and folinic acid improves survival by 22% relative to observation for Dukes B and C disease (equivalent to stage II and III disease).12 There is a further incremental benefit from the addition of oxaliplatin for patients with stage III disease (20% relative survival benefit compared to 5-fluorouracil and folinic acid without oxaliplatin, or an absolute benefit of 8.1% at 10 years).13 These incremental benefits have resulted in 5-year survival for patients with stage III colon cancer of 80%–82% with adjuvant oxaliplatin-based chemotherapy.14,15 For stage II disease, the benefit of oxaliplatin is less clear, with no benefit observed for low-risk disease and a numeric but non–statistically significant benefit in high-risk stage II disease (defined as T4 tumor, perforation, or fewer than ten lymph nodes in pathological specimens).13
While adjuvant chemotherapy is currently the standard of care for many tumors, mounting evidence across broad tumor types, including gastric, esophageal, rectal, and breast cancers, suggests that neoadjuvant chemotherapy may be substantially more effective1,16–19 for both disease- and patient-related reasons.
Factors Favoring Neoadjuvant Chemotherapy
Factors Against Neoadjuvant Chemotherapy
There are a number of concerns relating to potential adverse impacts of a neoadjuvant approach.
Diagnosis
Endoscopy
Colonoscopy is typically the initial diagnostic test for localized colon cancer, providing assessment of the degree of luminal obstruction and biopsy for histopathological confirmation. At present, further staging of the tumor is not a routine component of colonoscopy, although there is emerging evidence of a role for endoscopic ultrasound (EUS) to evaluate the T stage of in situ colon cancer. This approach has been used widely for rectal cancers, and is now being examined for colonic tumors.
A systematic review and meta-analysis conducted in 2015 examined the diagnostic accuracy of EUS for prediction of T and N stages in colon cancers proximal to the rectum.42 It found that sensitivity to detect T3 or T4 tumors was 0.97, with a specificity of 0.83. Its sensitivity in detecting nodal involvement was 0.58, with specificity of 0.78. A subsequent prospective study showed sensitivity of 0.75 and specificity of 0.90 for higher-risk (T3 with ≥5 mm submucosal invasion or T4) tumors, with overall accuracy of 0.88.43 This study compared EUS to CT, reporting sensitivity in detecting high-risk tumors was similar, while the specificity of EUS was superior. This has important implications in avoiding overtreatment when considering a neoadjuvant approach. It is important to note that the majority of cases in these studies involved tumors in the sigmoid or descending colon and that EUS staging may not be practical throughout the colon.
No neoadjuvant trials have included colonic EUS staging to date. However, given its increased accuracy over CT staging, this could be incorporated into future clinical trials to optimize patient selection.
Imaging
Computed Tomography
CT is widely available and already a routine part of preoperative staging of colon cancer, but in the context of documenting extracolonic disease. As mentioned, there is a learning curve for applying T and N stages to primary colon tumors, but technological improvements and protocols to optimize settings to examine local parameters are emerging.
A 2007 study of preoperative CT staging for evaluation of T and N stages showed low diagnostic accuracy of 60% for T stage and 62% for N stage.44 The authors noted that despite the relatively poor accuracy, the prognostic outcome of high-risk radiologically staged tumors was similar to that of high-risk pathologically staged tumors. In 2012, as part of the training and quality control for the randomized phase III FOxTROT trial of neoadjuvant chemotherapy for colon cancer, a pilot study of radiological staging was undertaken.45 CT and pathological staging was compared for 94 patients, reporting 87% sensitivity and 49% specificity for high-risk tumors (T3 with ≥5 mm submucosal invasion or T4). Sensitivity to predict any tumor eligible for chemotherapy (T3 or T4) was 95%, with specificity of 50%. Sensitivity for node-positive disease was 68% and specificity 42%.
More recently, a large US National Cancer Database study of over 100,000 patients showed 80% correlation between radiological and pathological T stage. For N stage, this was 83%.46 This study used nationwide database-level data and did not evaluate specific staging modalities, although the authors noted that CT scanning was the most widespread staging modality in use. It was noted that sensitivity in detecting T3/4 tumors was 80%, with 98% specificity.
Magnetic Resonance Imaging
Standard for rectal and prostate cancers, magnetic resonance imaging (MRI) is an emerging tool for T and N staging of colon cancers. Small studies have shown somewhat improved diagnostic accuracy with MRI compared to CT imaging and a lower rate of false-positive T3/4 tumor classifications.47,48 A retrospective study in the Netherlands showed the sensitivity of MRI in detecting any T3/4 tumor was high (72%–91%); however, for “high-risk” T3 or T4 tumors it was only 40%–60%.49 One reason for this may be the difficulty in accurately differentiating reactive serosal changes compared with bona fide serosal involvement of the tumor, as both have similar imaging appearances.49
CT Colonography
CT colonography is an evolving technique using contrast-enhanced CT to obtain three-dimensional images of the bowel wall. Diagnostic accuracy for T stage is 73%–83%, depending on whether multiplanar reconstructions are used.50 Further refinement to the staging technique has been suggested, using bordering blood vessels to better define the bowel wall.51 This technique improved accuracy to 77% for T2 tumors, 81% for T3, and 97% for T4a tumors. A major limitation of CT colonography is the requirement for bowel preparation, an arduous and unpleasant process, in patients who have likely already undergone this for their diagnostic endoscopy. However, if further validation confirms the accuracy of colonography, this could potentially be concurrently timed with colonoscopy so that a single preparation is required.
Clinical Applications of Imaging Data
It is likely that a combination of staging modalities is more accurate than a single modality, but this would add time and expense, and further research is required. For those who may be understaged radiologically, it is important to design follow-up and manage patient expectations, including apprising them of the fact that higher pathological stage leads to postoperative adjuvant therapy as required. Conversely, clinical trials need to recognize the potential for overstaging and subjecting patients to chemotherapy who otherwise would not have received adjuvant treatment.
Current Evidence
Preclinical and Translational Data
Initial preclinical research studied cell kinetics following tumor removal. Fisher et al noted that removal of a primary mammary adenocarcinoma in mice prompted secretion of a serum growth-stimulating factor and associated increased cell proliferation in residual tumor cells.52 Subsequently, they reported that chemotherapy administered prior to surgery was more effective at preventing cell proliferation than when administered after surgery.53 Furthermore, when sera from mice with mammary tumors who had received neoadjuvant chemotherapy was injected into other mice with the same tumors, it failed to cause the same cell proliferation.53 On the basis of these results, it was proposed that administration of chemotherapy prior to surgery may prevent the increase in cell proliferation after tumor removal.
A similar phenomenon of metastasis proliferation postresection was investigated in humans. A paper examining pathological tumor vascularity pre- and postresection and also change in FDG-PET avidity found that human colorectal cancer demonstrated similar behavior to animal models.54 Metastasis samples collected after primary tumor resection were more vascular than those collected prior to resection, with lower rates of apoptosis.54
Apart from direct tumor-cell killing, cytotoxic chemotherapy has been shown to have extensive immunogenic effects that likely contribute to its effectiveness, discussed in an excellent 2018 review.55 Comparison of resected liver metastases after neoadjuvant chemotherapy compared to no neoadjuvant chemotherapy showed a transient increase in T-cell tumor infiltration postchemotherapy.56 This suggests that antitumor immunity could potentially be increased by the administration of neoadjuvant chemotherapy, allowing for ongoing immunosurveillance for dormant tumor cells postresection.
Neoadjuvant treatments other than chemotherapy are also supported by preclinical data. A study on colon cancer also displayed improved survival with preresection radiofrequency ablation in aggressive murine colon cancer by inducing antitumor systemic immunity.57
Patient-derived organoids (PDOs) and xenografts offer exciting translational approaches to refine neoadjuvant treatment, and correlate with in situ biology. Weeber et al demonstrated that colorectal cancer PDOs preserved 90% of somatic mutations found in the tumors from which they were derived.58 In rectal cancer, response to neoadjuvant chemoradiation in both models has been shown to correlate with treatment response in the patients from which they were derived.59,60 PDOs are a promising avenue for high-throughput drug screening for neoadjuvant therapy, due to their low cost, quick propagation time, and close correlation with human cancers. This has already been utilized in intraperitoneal chemotherapy for peritoneal metastases of colorectal cancer.61 One disadvantage, however, is the lack of the tumor microenvironment in these samples.
Single-Arm Clinical and Cohort Studies
Growing evidence supports the use of neoadjuvant chemotherapy in locally advanced colon cancer. A number of single-arm trials have suggested that the fluoropyrimidine–oxaliplatin combination is both safe and feasible.20,32,37,40,41
A minimum of two cycles of neoadjuvant capecitabine and oxaliplatin (CAPOX; alone or with panitumumab in RAS/RAF wild-type patients) has been shown to result in both radiological response and pathological regression in two studies,37,41 with a small number of patients (2%–4%) demonstrating complete pathological response at surgery. A longer regimen of four to six cycles of 5-fluorouracil, folinic acid, and oxaliplatin (FOLFOX) or CAPOX neoadjuvant therapy has also demonstrated efficacy in terms of radiological response and pathological response without evidence of distant progression during the preoperative period, though with a similarly low rate of complete pathological response (4.6%).20
Triplet neoadjuvant chemotherapy with (FOLFOX plus irinotecan (FOLFOXIRI) has also been assessed in a phase II study.40 This demonstrated a trend to greater tumor volume reduction with each subsequent chemotherapy cycle administered when comparing patients who received all or nearly all of the four planned preoperative cycles, with patients who completed only one or two cycles. It should be noted that triplet therapy was also associated with high rates of toxicity, with more than half (56.5%) the patients experiencing grade 3 or 4 toxicities, most commonly cytopenias and gastrointestinal side effects.40 Two of the 23 patients in the FOLFOXIRI study had progressive disease during the preoperative period; however, this study recruited high-risk patients with clinical stage IIIb disease (a higher-risk cohort than used for other comparable trials).
Importantly, neoadjuvant chemotherapy did not appear to delay surgery in any of the studies, and rates of perioperative complications were similar to published rates in patients undergoing surgery alone.37,40,41 Length of postoperative stay in these trials ranged 6–9 days, which is comparable to that seen in the general surgical population. Hospital stay is impacted by surgical technique and local hospital practices, and reported duration posthemicolectomy is 4–14 days, depending on technique and country.62–64 Similarly, rates of anastomotic leak postoperatively were 0–7% in these phase 2 studies,37,40,41 comparable to the 6.4% rate seen in a nationwide Danish population-wide study.65
The effect on overall survival also appeared to be encouraging in these single-arm studies, but will be further elucidated in randomized trials.20,32 At a population level, a large cohort study utilizing data from the US National Cancer database found that survival was improved in patients with very locally advanced (T4b) colon cancer who received neoadjuvant chemotherapy, but not in patients with T3 or T4a disease.66 Of note, only 3% of the cohort (921 of 27,575) were treated with neoadjuvant chemotherapy and tended to have higher-stage and -grade tumors. These data suggest that the downstaging effect of neoadjuvant chemotherapy may be most useful in T4b tumors; however randomized prospective data are needed to better elucidate treatment effects. Five-year survival in smaller cohorts with T4 colon cancer post–neoadjuvant therapy ranges from the expected 67%32 to the very promising 95%,20 highlighting the need for prospective randomized studies to truly estimate the treatment effect.
Randomized Data
The key clinical trials reported to date are summarized in the following sections.
PRODIGE 22–ECKINOXE
This randomized phase II trial included patients with high-risk T3 and T4 tumors or N2 nodal status (regardless of T stage) staged by CT.7 The primary end point was degree of pathological response. The experimental arm received four cycles of neoadjuvant FOLFOX4, followed by eight cycles of the same chemotherapy adjuvantly, while the control arm received immediate surgery and adjuvant chemotherapy (12 cycles of FOLFOX4). RAS wild-type tumors were additionally randomized to receive chemotherapy versus chemotherapy plus cetuximab; however, this arm was stopped early after interim analysis showed lack of efficacy.
Response was evaluated according to tumor-response grading (TRG), as defined by Ryan et al.67 In sum, 7% of patients in the preoperative chemotherapy arm had a TRG 1 (major) response and 36% TRG 2 (significant tumor regression). Pathological stage was numerically lower in the preoperative-treatment group, but this was not statistically significant. Other high-risk features, including extramural vascular invasion and perineural invasion, were significantly reduced in the preoperative-treatment arm. Importantly, 33% of patients in the control arm were found to have low-risk stage II disease at surgery and had been overstaged based on preoperative CT. These patients would not routinely be administered adjuvant chemotherapy. Preoperative chemotherapy was safe, with no difference in perioperative morbidity. Three-year survival was reported in 2020, and was equivalent in both arms at 90.3%, while disease-free survival was numerically better in the neoadjuvant-treatment arm (76.8% vs 69.2% in controls, p=0.6).68 Of note, the study was not designed or powered to demonstrate differences in these end points.
FOxTROT
This phase III trial conducted from the UK recruited patients with at least T3 disease on preoperative staging and randomized them to neoadjuvant chemotherapy ± panitumumab or to immediate surgery followed by adjuvant chemotherapy.21 The pilot phase included only higher-risk patients with radiological (r) T3 tumors with ≥5 mm extramural extension or rT4 tumors. The pilot study found that the approach was well tolerated and appeared to downstage the primary tumor.21
Further results were reported at the 2019 American Society of Clinical Oncology Annual Meeting: the 2-year failure rate (defined as either relapse or persistent disease) was reduced numerically (HR 0.77, 95% CI 0.56–1.06), but did not reach statistical significance (p=0.11).69 There was a significantly reduced rate of incomplete tumor (R1 or R2) resection and reduced pathological staging. Nonprespecified subgroup analysis suggested less benefit in patients with deficient mismatch repair (dMMR) tumors.39 The pilot phase included only higher-risk patients with radiological rT3 tumors with ≥5 mm extramural extension or rT4 tumors. Later protocol revision allowed any rT3 tumor to be enrolled in a “younger age/good general health” patient, as determined by the treating physician. There was no specific nodal status prescribed.8 Of note, a significant proportion of the control arm were node-negative at surgery (48%), suggesting that it is likely a large number of stage II patients were also included in the neoadjuvant-treatment arm.39 The final results of this trial are yet to be published.
Use of Biological Agents
Both the clinically available anti-EGFR monoclonal antibodies, cetuximab and panitumumab, have been studied in combination with neoadjuvant chemotherapy. In the PRODIGE 22 study, the cetuximab arm was stopped early for lack of efficacy. A panitumumab arm was included in the FOxTROT trial, but results have not yet been published. Interest is high, given the somewhat analogous situation studied in the New EPOC trial, where there was a deleterious effect of cetuximab in patients with resectable liver metastases.70,71 Anti-VEGF agents have not been included in trials; however, in the adjuvant setting bevacizumab has proven ineffective.72 There are also potential safety concerns, with the use of preoperative bevacizumab possibly impairing wound healing.
Future Directions
Triplet Regimens
The triplet FOLFOXIRI regimen plus bevacizumab improves overall response rates, progression-free survival, and overall survival (OS) compared to FOLFIRI plus bevacizumab/FOLFOX plus bevacizumab in the first-line metastatic setting,73,74 recently confirmed in a meta-analysis.75 Neoadjuvant benefit is being assessed in a phase II trial with neoadjuvant FOLFOXIRI, using PET-CT imaging assessment and ctDNA monitoring during and after therapy (see Table 1).76
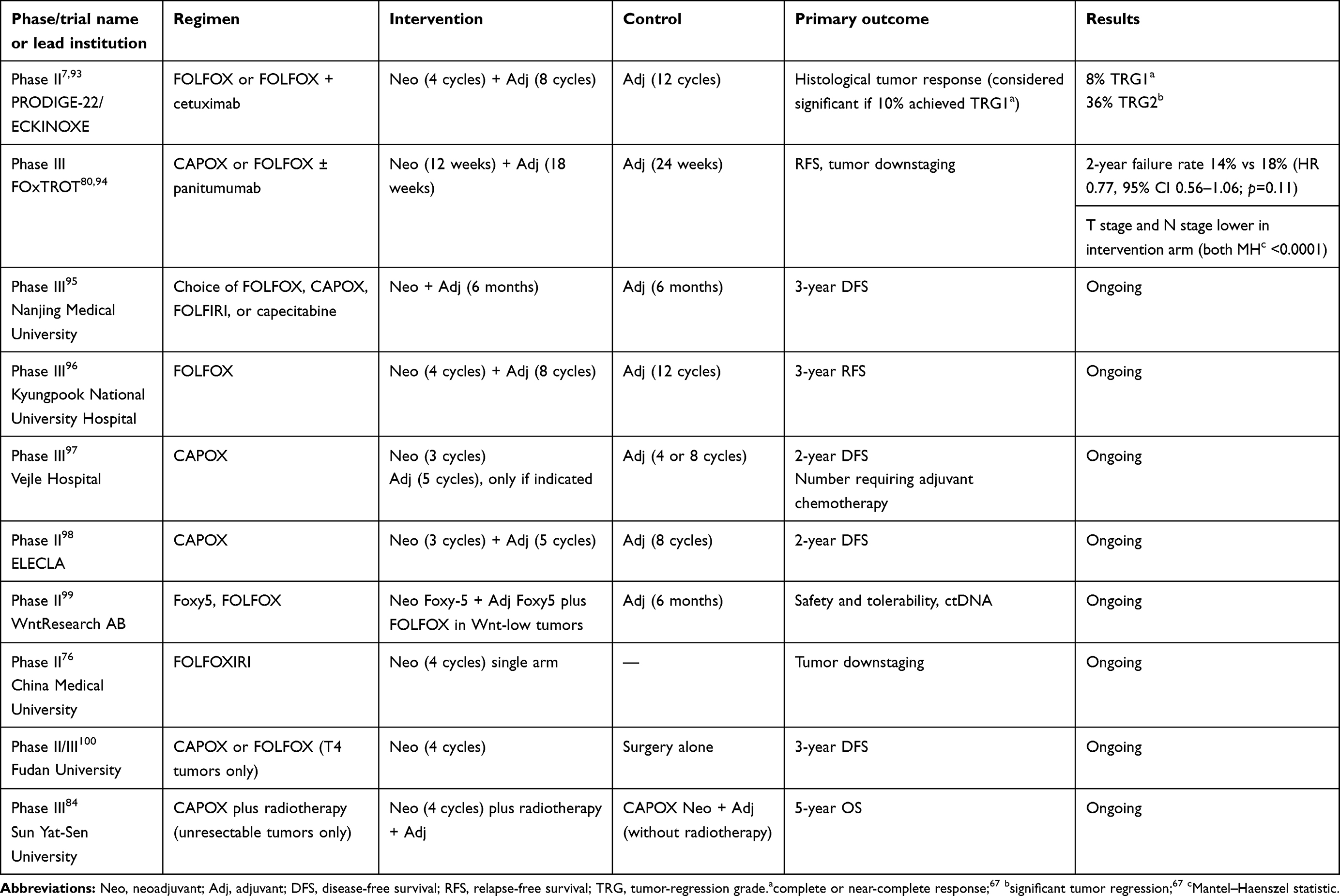 |
Table 1 Completed and ongoing clinical trials using neoadjuvant chemotherapy for locally advanced colon cancer |
Immunotherapy
The body of evidence for the efficacy of immunotherapy in advanced dMMR colorectal cancer is growing, with objective response rates of 31%–40% for single-agent PD1 inhibitors and 55% for dual-checkpoint inhibition, whereas the response rate in proficient MMR (pMMR) metastatic disease is almost nil.77–79 Immunotherapy may provide a more efficacious alternative to neoadjuvant chemotherapy in the dMMR group, which comprises 10%–15% of early-stage colorectal cancer (as opposed to only 4% of metastatic cases). The dMMR subgroup in the phase 3 FOxTROT trial had reduced rates of tumor regression after neoadjuvant FOLFOX chemotherapy compared to pMMR tumors, with no pathological response seen in 74% vs 27% of patients.80 Several studies are now examining the role of immunotherapy earlier in the disease trajectory. A small retrospective study (eight patients with four T4N1–T4N2 colon cancers) reported one pathological complete response and one partial response after single-agent neoadjuvant PD1-inhibitor treatment.81
Recent data from the NICHE study support the use of dual-checkpoint inhibition with ipilimumab and nivolumab in the neoadjuvant setting for dMMR colorectal cancer. The huge surprise was the benefit shown in pMMR cancers:35 19 of 20 patients with dMMR colorectal cancer achieved a major pathological response, while 25% (n=4) of pMMR patients responded.35 Translational studies will be pivotal in understanding these results. Ongoing trials in this setting are presented in Table 1.
Immunomodulation using antitumor vaccines and chimeric antigen–receptor T cells are also being explored as neoadjuvant treatments in early-phase trials.82
Neoadjuvant Chemoradiotherapy
Although the standard of care in locally advanced rectal cancer, neoadjuvant chemoradiotherapy has not been well studied in colon cancer, with only a few small studies and case reports to date. Barriers include feasibility of irradiating mobile areas of the bowel and increased toxicity with concurrent therapy. A prospective observational study of 60 Chinese patients with unresectable colon cancer (located over 15 cm from the anal verge) found that 95% of patients became suitable for resection after neoadjuvant chemoradiotherapy with CAPOX (or capecitabine in patients aged over 70 years).83 Some were able to avoid radical cystectomy or enterectomy. These findings promoted a phase III trial of neoadjuvant CAPOX/radiotherapy versus neoadjuvant CAPOX with a primary end point of overall survival, which is under way (Table 1).84
Chemoradiation may also be a more attractive option for dMMR tumors. In the rectal cancer setting, a retrospective cohort study of 50 dMMR patients found 29% of dMMR versus 0 pMMR rectal cancer patients progressed while on neoadjuvant FOLFOX, but that dMMR and pMMR patients responded at comparable rates to chemoradiation.85 These data suggest that neoadjuvant chemoradiotherapy could be explored in further research for patients with more proximal locally advanced dMMR colorectal cancers.
Novel Biomarkers
It is hoped that biomarkers will be able to better personalise and refine neoadjuvant therapy, avoiding futile therapy in those where it is likely to be ineffective and providing stronger evidence for treatment in those with markers associated with response. Upregulation of PDK4 has been shown to be associated with improved liver function following neoadjuvant chemotherapy in oligometastatic colorectal cancer.86 NDRG1 is associated with response to oxaliplatin.87 Furthermore, several markers are associated with chemotherapy-refractory cells in colorectal cancer, including nucleus NAC1, HMGB1, andABCB5.88–90 ctDNA is an emerging tool that in the neoadjuvant setting could be used to assess treatment response, potentially directing nonresponding patients to intensification of therapy or immediate surgery.23
Elderly and Other “Special” Populations
Trial patients have been in general younger than the average patient with colon cancer, the median age at diagnosis of colorectal cancer in the SEER database being 67 years, with 24.6% of patients aged 65–74 years and 30% of patients diagnosed aged ≥75 years.91 In general, as in most trials, the elderly have been underrepresented in neoadjuvant studies, so extrapolation into real-world practice needs caution. The intervention arm in the FOxTROT pilot cohort had a median age of 64 years, with only 24% of patients aged >70 years. In PRODIGE 22, the median age in the treatment arm was 65 years, with the oldest patient in this trial aged 79 years.7,21
Patients with colonic obstruction have generally been excluded from neoadjuvant trials, though some trials have included a small number of patients with uncomplicated defunctioning stomata. One phase II study specifically evaluated neoadjuvant chemotherapy in those with defunctioning stomata for obstructing colon cancer, and found that this was feasible and safe.92 Major comorbidities and poor performance status were also excluded.
Conclusion
Neoadjuvant chemotherapy for locally advanced colon cancer remains an evolving treatment paradigm. There have been encouraging findings in surrogate end points, such as tumor downstaging and reduction in high-risk features of resected tumors. Limitations at present include the inaccuracy of traditional radiological staging and a lack of prospective data showing definite survival benefit. Novel approaches incorporating biomarkers and new therapies, such as neoadjuvant immunotherapy, are of great interest. The results of ongoing clinical trials are awaited to provide stronger evidence regarding the benefits (or lack thereof) of this treatment approach.
Disclosure
Dr Ajay Raghunath reports a conference-travel grant from Amgen outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11–20. doi:10.1056/NEJMoa055531
2. Vale C. Neoadjuvant chemotherapy in invasive bladder cancer: a systematic review and meta-analysis. Lancet. 2003;361(9373):1927–1934. doi:10.1016/S0140-6736(03)13580-5
3. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351(17):1731–1740. doi:10.1056/NEJMoa040694
4. van Hagen P, Hulshof MCCM, van Lanschot JJB, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–2084. doi:10.1056/NEJMoa1112088
5. Conroy T, Lamfichekh N, Etienne P-L, et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: final results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J Clin Oncol. 2020;38(15_suppl):4007. doi:10.1200/JCO.2020.38.15_suppl.4007
6. Hospers G, Bahadoer RR, Dijkstra EA, et al. Short-course radiotherapy followed by chemotherapy before TME in locally advanced rectal cancer: the randomized RAPIDO trial. J Clin Oncol. 2020;38(15_suppl):4006. doi:10.1200/JCO.2020.38.15_suppl.4006
7. Karoui M, Rullier A, Luciani A, et al. Neoadjuvant FOLFOX 4 versus FOLFOX 4 with Cetuximab versus immediate surgery for high-risk stage II and III colon cancers: a multicentre randomised controlled phase II trial–the PRODIGE 22–ECKINOXE trial. BMC Cancer. 2015;15:511. doi:10.1186/s12885-015-1507-3
8. FoxTROT Collaborative Group. FOxTROT protocol: a randomised trial assessing whether preoperative chemotherapy and/or an anti-EGFR monoclonal antibody improve outcome in high-risk operable colon cancer; 2012. Available from: https://www.birmingham.ac.uk/Documents/college-mds/trials/bctu/foxtrot/FOxTROTProtocolv60090712.pdf.
9. Labianca R, Nordlinger B, Beretta GD, et al. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi64–72. doi:10.1093/annonc/mdt354
10. Benson AB, Schrag D, Somerfield MR, et al. American Society of Clinical Oncology recommendations on adjuvant chemotherapy for stage II colon cancer. J Clin Oncol. 2004;22(16):3408–3419. doi:10.1200/JCO.2004.05.063
11. Edge SB, Compton CC. The American Joint Committee on cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
12. Labianca R, Marsoni S, Pancera G, et al. Efficacy of adjuvant fluorouracil and folinic acid in colon cancer. Lancet. 1995;345(8955):939–944.
13. André T, de Gramont A, Vernerey D, et al. Adjuvant fluorouracil, leucovorin, and oxaliplatin in stage II to III colon cancer: updated 10-year survival and outcomes according to BRAF mutation and mismatch repair status of the MOSAIC study. J Clin Oncol. 2015;33(35):4176–4187. doi:10.1200/JCO.2015.63.4238
14. André T, Meyerhardt J, Iveson T, et al. Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): final results from a prospective, pooled analysis of six randomised, phase 3 trials. Lancet Oncol. 2020;21(12):1620–1629. doi:10.1016/S1470-2045(20)30527-1
15. Yothers G, O’Connell MJ, Allegra CJ, et al. Oxaliplatin as adjuvant therapy for colon cancer: updated results of NSABP C-07 trial, including survival and subset analyses. J Clin Oncol. 2011;29(28):3768–3774. doi:10.1200/JCO.2011.36.4539
16. Medical Research Council Oesophageal Cancer Working Party. Surgical resection with or without preoperative chemotherapy in oesophageal cancer: a randomised controlled trial. Lancet. 2002;359(9319):1727–1733. doi:10.1016/S0140-6736(02)08651-8
17. Sebag-Montefiore D, Stephens RJ, Steele SR, et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016) - a multicentre, randomised trial. Lancet. 2009;373:811–820. doi:10.1016/S0140-6736(09)60484-0
18. Newton AD, Datta J, Loaiza-Bonilla A, Karakousis GC, Roses RE. Neoadjuvant therapy for gastric cancer: current evidence and future directions. J Gastrointest Oncol. 2015;6(5):534–543. doi:10.3978/j.issn.2078-6891.2015.047
19. Graham PJ, Brar MS, Foster T, et al. Neoadjuvant chemotherapy for breast cancer, is practice changing? A population-based review of current surgical trends. Ann Surg Oncol. 2015;22(10):3376–3382. doi:10.1245/s10434-015-4714-x
20. Arredondo J, Baixauli J, Pastor C, et al. Mid-term oncologic outcome of a novel approach for locally advanced colon cancer with neoadjuvant chemotherapy and surgery. Clin Transl Oncol. 2017;19(3):379–385. doi:10.1007/s12094-016-1539-4
21. Collaborative Group F; FOxTROT Collaborative Group. Feasibility of preoperative chemotherapy for locally advanced, operable colon cancer: the pilot phase of a randomised controlled trial. Lancet Oncol. 2012;13(11):1152–1160. doi:10.1016/S1470-2045(12)70348-0
22. Rodel C, Martus P, Papadoupolos T, et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol. 2005;23(34):8688–8696. doi:10.1200/JCO.2005.02.1329
23. Riva F, Bidard F-C, Houy A, et al. Patient-specific circulating tumor DNA detection during neoadjuvant chemotherapy in triple-negative breast cancer. Clin Chem. 2017;63(3):691–699. doi:10.1373/clinchem.2016.262337
24. Yang L, Wang Y, Shen L, et al. Predicting treatment outcome of rectal cancer patients underwent neoadjuvant chemoradiotherapy by ctDNA: the potential use of ctDNA monitoring as organ-sparing approach. J Clin Oncol. 2018;36(15_suppl):3608. doi:10.1200/JCO.2018.36.15_suppl.3608
25. Tanaka K, Shimada H, Miura M, et al. Metastatic tumor doubling time: most important prehepatectomy predictor of survival and nonrecurrence of hepatic colorectal cancer metastasis. World J Surg. 2004;28(3):263–270. doi:10.1007/s00268-003-7088-3
26. Finlay IG, Meek D, Brunton F, McArdle CS. Growth rate of hepatic metastases in colorectal carcinoma. Br J Surg. 1988;75(7):641–644. doi:10.1002/bjs.1800750707
27. Scheer MG, Stollman TH, Vogel WV, Boerman OC, Oyen WJ, Ruers TJ. Increased metabolic activity of indolent liver metastases after resection of a primary colorectal tumor. J Nucl Med. 2008;49(6):887–891. doi:10.2967/jnumed.107.048371
28. Zeamari S, Roos E, Stewart FA. Tumour seeding in peritoneal wound sites in relation to growth-factor expression in early granulation tissue. Eur J Cancer. 2004;40(9):1431–1440. doi:10.1016/j.ejca.2004.01.035
29. Nelson H, Petrelli N, Carlin A, et al. Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst. 2001;93(8):583–596. doi:10.1093/jnci/93.8.583
30. Hendren S, Birkmeyer JD, Yin H, Banerjee M, Sonnenday C, Morris AM. Surgical complications are associated with omission of chemotherapy for stage III colorectal cancer. Dis Colon Rectum. 2010;53(12):1587–1593. doi:10.1007/DCR.0b013e3181f2f202
31. Yamamoto S, Inomata M, Katayama H, et al. Short-term surgical outcomes from a randomized controlled trial to evaluate laparoscopic and open D3 dissection for stage II/III colon cancer: Japan Clinical Oncology Group Study JCOG 0404. Ann Surg. 2014;260(1):23–30. doi:10.1097/SLA.0000000000000499
32. de Gooyer JM, Verstegen MG, t Lam-Boer J, et al. Neoadjuvant chemotherapy for locally advanced T4 colon cancer: a nationwide propensity-score matched cohort analysis. Dig Surg. 2020;37(4):292–301. doi:10.1159/000503446
33. Weinrich M, Bochow J, Kutsch AL, et al. High compliance with guideline recommendations but low completion rates of adjuvant chemotherapy in resected pancreatic cancer: a cohort study. Ann Med Surg (Lond). 2018;32:32–37. doi:10.1016/j.amsu.2018.06.004
34. Hershman DL, Shao T, Kushi LH, et al. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res Treat. 2011;126(2):529–537. doi:10.1007/s10549-010-1132-4
35. Chalabi M, Fanchi LF, Dijkstra KK, et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat Med. 2020;26(4):566–576. doi:10.1038/s41591-020-0805-8
36. Petrelli F, Coinu A, Lonati V, Barni S. A systematic review and meta-analysis of adjuvant chemotherapy after neoadjuvant treatment and surgery for rectal cancer. Int J Colorectal Dis. 2015;30(4):447–457. doi:10.1007/s00384-014-2082-9
37. Jakobsen A, Andersen F, Fischer A, et al. Neoadjuvant chemotherapy in locally advanced colon cancer. A phase II trial. Acta Oncol. 2015;54(10):1747–1753. doi:10.3109/0284186X.2015.1037007
38. Ingraham AM, Cohen ME, Bilimoria KY, et al. Comparison of hospital performance in nonemergency versus emergency colorectal operations at 142 hospitals. J Am Coll Surg. 2010;210(2):155–165. doi:10.1016/j.jamcollsurg.2009.10.016
39. Seymour MT, Morton D; on behalf of the International FOxTROT Trial Investigators. FOxTROT: an international randomised controlled trial in 1052 patients (pts) evaluating neoadjuvant chemotherapy (NAC) for colon cancer. J Clin Oncol. 2019;37(15_suppl):3504. doi:10.1200/JCO.2019.37.15_suppl.3504
40. Zhou H, Song Y, Jiang J, et al. A pilot phase II study of neoadjuvant triplet chemotherapy regimen in patients with locally advanced resectable colon cancer. Chin J Cancer Res. 2016;28(6):598–605. doi:10.21147/j.issn.1000-9604.2016.06.06
41. Liu F, Yang L, Wu Y, et al. CapOX as neoadjuvant chemotherapy for locally advanced operable colon cancer patients: a prospective single-arm phase II trial. Chin J Cancer Res. 2016;28(6):589–597. doi:10.21147/j.issn.1000-9604.2016.06.05
42. Malmstrøm ML, Săftoiu A, Vilmann P, Klausen TW, Gögenur I. Endoscopic ultrasound for staging of colonic cancer proximal to the rectum: a systematic review and meta-analysis. Endosc Ultrasound. 2016;5(5):307–314. doi:10.4103/2303-9027.191610
43. Malmstrøm ML, Gögenur I, Riis LB, et al. Endoscopic ultrasonography and computed tomography scanning for preoperative staging of colonic cancer. Int J Colorectal Dis. 2017;32(6):813–820. doi:10.1007/s00384-017-2820-x
44. Smith NJ, Bees N, Barbachano Y, Norman AR, Swift RI, Brown G. Preoperative computed tomography staging of nonmetastatic colon cancer predicts outcome: implications for clinical trials. Br J Cancer. 2007;96(7):1030–1036. doi:10.1038/sj.bjc.6603646
45. Dighe S, Swift I, Magill L, et al. Accuracy of radiological staging in identifying high-risk colon cancer patients suitable for neoadjuvant chemotherapy: a multicentre experience. Colorectal Dis. 2012;14(4):438–444. doi:10.1111/j.1463-1318.2011.02638.x
46. Dehal AN, Graff-Baker AN, Vuong B, et al. Correlation between clinical and pathologic staging in colon cancer: implications for neoadjuvant treatment. J Gastrointest Surg. 2018;22(10):1764–1771. doi:10.1007/s11605-018-3777-y
47. Park SY, Cho SH, Lee MA, et al. Diagnostic performance of MRI- versus MDCT-categorized T3cd/T4 for identifying high-risk stage II or stage III colon cancers: a pilot study. Abdom Radiol. 2019;44(5):1675–1685. doi:10.1007/s00261-018-1822-7
48. Rollvén E, Holm T, Glimelius B, Lörinc E, Blomqvist L. Potentials of high resolution magnetic resonance imaging versus computed tomography for preoperative local staging of colon cancer. Acta Radiologica. 2013;54(7):722–730. doi:10.1177/0284185113484018
49. Nerad E, Lambregts DMJ, Kersten ELJ, et al. MRI for local staging of colon cancer: can MRI become the optimal staging modality for patients with colon cancer? Dis Colon Rectum. 2017;60(4):385–392. doi:10.1097/DCR.0000000000000794
50. Filippone A, Ambrosini R, Fuschi M, Marinelli T, Genovesi D, Bonomo L. Preoperative T and N staging of colorectal cancer: accuracy of contrast-enhanced multi-detector row CT colonography–initial experience. Radiology. 2004;231(1):83–90. doi:10.1148/radiol.2311021152
51. Komono A, Shida D, Iinuma G, et al. Preoperative T staging of colon cancer using CT colonography with multiplanar reconstruction: new diagnostic criteria based on “bordering vessels”. Int J Colorectal Dis. 2019;34(4):641–648. doi:10.1007/s00384-019-03236-y
52. Fisher B, Gunduz N, Saffer EA. Influence of the interval between primary tumor removal and chemotherapy on kinetics and growth of metastases. Cancer Res. 1983;43(4):1488–1492.
53. Fisher B, Saffer E, Rudock C, Coyle J, Gunduz N. Effect of local or systemic treatment prior to primary tumor removal on the production and response to a serum growth-stimulating factor in mice. Cancer Res. 1989;49(8):2002–2004.
54. Peeters CFJM, de Waal RMW, Wobbes T, Ruers TJM. Metastatic dormancy imposed by the primary tumor: does it exist in humans? Ann Surg Oncol. 2008;15(11):3308–3315. doi:10.1245/s10434-008-0029-5
55. Wang Y-J, Fletcher R, Yu J, Zhang L. Immunogenic effects of chemotherapy-induced tumor cell death. Genes Dis. 2018;5(3):194–203. doi:10.1016/j.gendis.2018.05.003
56. Dagenborg VJ, Marshall SE, Yaqub S, et al. Neoadjuvant chemotherapy is associated with a transient increase of intratumoral T-cell density in microsatellite stable colorectal liver metastases. Cancer Biol Ther. 2020;21(5):432–440. doi:10.1080/15384047.2020.1721252
57. Ito F, Ku AW, Bucsek MJ, et al. Immune adjuvant activity of pre-resectional radiofrequency ablation protects against local and systemic recurrence in aggressive murine colorectal cancer. PLoS One. 2015;10(11):e0143370. doi:10.1371/journal.pone.0143370
58. Weeber F, van de Wetering M, Hoogstraat M, et al. Preserved genetic diversity in organoids cultured from biopsies of human colorectal cancer metastases. Proc Natl Acad Sci U S A. 2015;112(43):13308–13311. doi:10.1073/pnas.1516689112
59. Yao Y, Xu X, Yang L, et al. Patient-derived organoids predict chemoradiation responses of locally advanced rectal cancer. Cell Stem Cell. 2020;26(1):17–26. doi:10.1016/j.stem.2019.10.010
60. Janakiraman H, Zhu Y, Becker SA, et al. Modeling rectal cancer to advance neoadjuvant precision therapy. Int J Cancer. 2020;147:1405–1418. doi:10.1002/ijc.32876
61. Roy P, Canet-Jourdan C, Annereau M, et al. Organoids as preclinical models to improve intraperitoneal chemotherapy effectiveness for colorectal cancer patients with peritoneal metastases: preclinical models to improve HIPEC. Int J Pharm. 2017;531(1):143–152. doi:10.1016/j.ijpharm.2017.07.084
62. Salimath J, Jones MW, Hunt DL, Lane MK. Comparison of return of bowel function and length of stay in patients undergoing laparoscopic versus open colectomy. JSLS. 2007;11(1):72–75.
63. Kelly M, Sharp L, Dwane F, Kelleher T, Comber H. Factors predicting hospital length-of-stay and readmission after colorectal resection: a population-based study of elective and emergency admissions. BMC Health Serv Res. 2012;12(1):77. doi:10.1186/1472-6963-12-77
64. Miller T, Thacker J, White W, et al. Reduced length of hospital stay in colorectal surgery after implementation of an enhanced recovery protocol. Anesth Analg. 2014;118:1052–1061. doi:10.1213/ANE.0000000000000206
65. Krarup P-M, Jorgensen LN, Andreasen AH, Harling H; Group obotDCC. A nationwide study on anastomotic leakage after colonic cancer surgery. Colorectal Dis. 2012;14(10):e661–e667. doi:10.1111/j.1463-1318.2012.03079.x
66. Dehal A, Graff-Baker AN, Vuong B, et al. Neoadjuvant chemotherapy improves survival in patients with clinical T4b colon cancer. J Gastrointest Surg. 2018;22(2):242–249. doi:10.1007/s11605-017-3566-z
67. Ryan R, Gibbons D, Hyland JM, et al. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology. 2005;47(2):141–146. doi:10.1111/j.1365-2559.2005.02176.x
68. Karoui M, Gallois C, Piessen G, et al. Does neoadjuvant FOLFOX chemotherapy improve the oncological prognosis of high-risk stage II and III colon cancers? Three years’ follow-up results of the Prodige 22 phase II randomized multicenter trial. J Clin Oncol. 2020;38(15_suppl):4110. doi:10.1200/JCO.2020.38.15_suppl.4110
69. Morton D. FOxTROT: an international randomised controlled trial in 1053 patients evaluating neoadjuvant chemotherapy (NAC) for colon cancer. Ann Oncol. 2019;30:v198–v252. doi:10.1093/annonc/mdz246.001
70. Primrose J, Falk S, Finch-Jones M, et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis: the New EPOC randomised controlled trial. Lancet Oncol. 2014;15(6):601–611. doi:10.1016/S1470-2045(14)70105-6
71. Bridgewater JA, Pugh SA, Maishman T, et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020;21(3):398–411. doi:10.1016/S1470-2045(19)30798-3
72. Kerr RS, Love S, Segelov E, et al. Adjuvant capecitabine plus bevacizumab versus capecitabine alone in patients with colorectal cancer (QUASAR 2): an open-label, randomised phase 3 trial. Lancet Oncol. 2016;17(11):1543–1557. doi:10.1016/S1470-2045(16)30172-3
73. Cremolini C, Antoniotti C, Rossini D, et al. Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2020;21(4):497–507. doi:10.1016/S1470-2045(19)30862-9
74. Cremolini C, Antoniotti C, Lonardi S, et al. Primary tumor sidedness and benefit from FOLFOXIRI plus bevacizumab as initial therapy for metastatic colorectal cancer. Retrospective analysis of the TRIBE trial by GONO. Ann Oncol. 2018;29(7):1528–1534. doi:10.1093/annonc/mdy140
75. Cremolini C, Antoniotti C, Stein A, et al. Individual patient data meta-analysis of FOLFOXIRI plus bevacizumab versus doublets plus bevacizumab as initial therapy of unresectable metastatic colorectal cancer. J Clin Oncol. 2020;38(28):3314–3324. doi:10.1200/JCO.20.01225
76. China Medical University. Neoadjuvant FOLFOXIRI chemotherapy in patients with locally advanced colon cancer. Available from: https://ClinicalTrials.gov/show/NCT03484195.
77. Le DT, Uram JN, Wang H, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015;372(26):2509–2520. doi:10.1056/NEJMoa1500596
78. Overman MJ, McDermott R, Leach JL, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. 2017;18(9):1182–1191. doi:10.1016/S1470-2045(17)30422-9
79. Overman MJ, Lonardi S, Wong KYM, et al. Durable Clinical Benefit With Nivolumab Plus Ipilimumab in DNA Mismatch Repair–Deficient/Microsatellite Instability–High Metastatic Colorectal Cancer. J Clin Oncol. 2018;36(8):773–779. doi:10.1200/JCO.2017.76.9901
80. Seligmann JF. FOxTROT: neoadjuvant FOLFOX chemotherapy with or without panitumumab (Pan) for patients (pts) with locally advanced colon cancer (CC). J Clin Oncol. 2020;38(15_suppl):4013. doi:10.1200/JCO.2020.38.15_suppl.4013
81. Liu D-X, Li -D-D, He W, et al. PD-1 blockade in neoadjuvant setting of DNA mismatch repair-deficient/microsatellite instability-high colorectal cancer. Oncoimmunology. 2020;9(1):1711650. doi:10.1080/2162402X.2020.1711650
82. George E. People;s trial of PalloV-CC in colon cancer. Available from: https://ClinicalTrials.gov/show/NCT03827967.
83. Chang H, Yu X, Xiao -W-W, et al. Neoadjuvant chemoradiotherapy followed by surgery in patients with unresectable locally advanced colon cancer: a prospective observational study. Onco Targets Ther. 2018;11:409–418. doi:10.2147/OTT.S150367
84. Sun Yat-sen University. Neoadjuvant chemoradiotherapy versus neoadjuvant chemotherapy for unresectable locally advanced colon cancer. Available from: https://ClinicalTrials.gov/show/NCT03970694.
85. Cercek A, Dos Santos Fernandes G, Roxburgh CS, et al. Mismatch repair deficient rectal cancer and resistance to neoadjuvant chemotherapy. Clin Cancer Res. 2020;26(13):3271–3279. doi:10.1158/1078-0432.CCR-19-3728
86. Strowitzki MJ, Radhakrishnan P, Pavicevic S, et al. High hepatic expression of PDK4 improves survival upon multimodal treatment of colorectal liver metastases. Br J Cancer. 2019;120(7):675–688. doi:10.1038/s41416-019-0406-9
87. Yang X, Zhu F, Yu C, et al. N-myc downstream-regulated gene 1 promotes oxaliplatin-triggered apoptosis in colorectal cancer cells via enhancing the ubiquitination of Bcl-2. Oncotarget. 2017;8(29):47709–47724. doi:10.18632/oncotarget.17711
88. Wilson BJ, Schatton T, Zhan Q, et al. ABCB5 identifies a therapy-refractory tumor cell population in colorectal cancer patients. Cancer Res. 2011;71(15):5307–5316. doi:10.1158/0008-5472.CAN-11-0221
89. Huang C-Y, Chiang S-F, Chen WT-L, et al. HMGB1 promotes ERK-mediated mitochondrial Drp1 phosphorylation for chemoresistance through RAGE in colorectal cancer. Cell Death Dis. 2018;9(10):1004. doi:10.1038/s41419-018-1019-6
90. Ju T, Jin H, Ying R, Xie Q, Zhou C, Gao D. Overexpression of NAC1 confers drug resistance via HOXA9 in colorectal carcinoma cells. Mol Med Rep. 2017;16(3):3194–3200. doi:10.3892/mmr.2017.6986
91. National Cancer Institute. SEER cancer stat facts: colorectal cancer; 2020. Available from: https://seer.cancer.gov/statfacts/html/colorect.html.
92. Ishibe A, Watanabe J, Suwa Y, et al. A prospective, single-arm, multicenter trial of diverting stoma followed by neoadjuvant chemotherapy using mFOLFOX6 for obstructive colon cancer: YCOG 1305 (PROBE study). Ann Surg. 2020. doi:10.1097/SLA.0000000000004494
93. Hôpitaux de Paris. Trial of neoadjuvant chemotherapy in locally advanced colon cancer (ECKINOXE). Available from: https://ClinicalTrials.gov/show/NCT01675999.
94. University of Birmingham. Fluorouracil and oxaliplatin with or without panitumumab in treating patients with high-risk colon cancer that can be removed by surgery (FOxTROT). Available from: https://ClinicalTrials.gov/show/NCT00647530.
95. First Affiliated Hospital with Nanjing Medical University. Neoadjuvant chemotherapy for the treatment of resectable locally advanced colon cancer. Available from: https://ClinicalTrials.gov/show/NCT02882269.
96. Kyungpook National University Hospital. Neoadjuvant FOLFOX chemotherapy for patients with locally advanced colon cancer NCT03426904. Available from: https://ClinicalTrials.gov/show/NCT03426904.
97. Vejle Hospital. Neoadjuvant chemotherapy versus standard treatment in patients with locally advanced colon cancer NCT03970694. Available from: https://ClinicalTrials.gov/show/NCT01918527.
98. Universidad de Leon. Analysis of the effectiveness of neoadjuvant chemotherapy in the treatment of colon cancer locally advanced (ELECLA) NCT04188158. Available from: https://ClinicalTrials.gov/show/NCT04188158.
99. WntResearch AB. Foxy-5 as neo-adjuvant therapy in subjects with wnt-5a low colon cancer. Available from: https://ClinicalTrials.gov/show/NCT03883802.
100. Fudan University. Laparoscopic surgery vs laparoscopic surgery + neoadjuvant chemotherapy for T4 tumor of the colon cancer. Available from: https://ClinicalTrials.gov/show/NCT02777437.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.