")
Back to Journals » Journal of Pain Research » Volume 15
The Role of Mental Health and Behavioral Disorders in the Development of Temporomandibular Disorder: A SWEREG-TMD Nationwide Case-Control Study
Authors Salinas Fredricson A , Krüger Weiner C, Adami J, Rosén A , Lund B, Hedenberg-Magnusson B, Fredriksson L, Naimi-Akbar A
Received 6 July 2022
Accepted for publication 19 August 2022
Published 6 September 2022 Volume 2022:15 Pages 2641—2655
DOI https://doi.org/10.2147/JPR.S381333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Adrian Salinas Fredricson,1,2 Carina Krüger Weiner,1,2 Johanna Adami,3 Annika Rosén,4,5 Bodil Lund,2,6 Britt Hedenberg-Magnusson,2,7 Lars Fredriksson,2,7 Aron Naimi-Akbar1,2,8
1Public Dental Services, Folktandvården Stockholm, Eastmaninstitutet, Department of Oral and Maxillofacial Surgery, Stockholm, Sweden; 2Division of Oral Diagnostics and Rehabilitation, Department of Dental Medicine, Karolinska Institutet, Stockholm, Sweden; 3Sophiahemmet University, Stockholm, Sweden; 4Department of Clinical Dentistry, Division of Oral and Maxillofacial Surgery, University of Bergen, Bergen, Norway; 5Department of Oral and Maxillofacial Surgery, Haukeland University Hospital, Bergen, Norway; 6Medical Unit for Reconstructive Plastic and Craniofacial Surgery, Karolinska University Hospital, Stockholm, Sweden; 7Public Dental Services, Folktandvården Stockholm, Eastmaninstitutet, Department of Orofacial Pain and Jaw Function, Stockholm, Sweden; 8Health Technology Assessment-Odontology (HTA-O), Malmö University, Malmö, Sweden
Correspondence: Adrian Salinas Fredricson, Eastmaninstitutet Käkkirurgi, Dalagatan 11, Stockholm, 102 31, Sweden, Email [email protected]
Purpose: There is a well-known association between mental and behavioral disorders (MBD) and temporomandibular disorder (TMD), although the association has not been established in population-based samples. This study aimed to investigate this relationship using national population-based registry data.
Patients and Methods: This case–control study used prospectively collected data from Swedish national registries to investigate exposure to MBD and the probability of developing TMD in all Swedish citizens with hospital-diagnosed or surgically treated TMD between 1998 and 2016. Odds ratios were calculated using conditional logistic regression adjusted for educational level, living area, country of birth, musculoskeletal comorbidity, and history of orofacial/neck trauma.
Results: A statistically significant association between MBD and TMD was found for mood affective disorders (OR 1.4), neurotic, stress-related and somatoform disorders (OR 1.7), behavioral syndromes associated with psychological disturbances and physical factors (OR 1.4), disorders of adult personality and behavior (OR 1.4), disorders of psychological development (OR 1.3), behavioral and emotional disorders with onset usually occurring in childhood and adolescence (OR 1.4), and unspecified mental disorder (OR 1.3). The association was stronger for TMD requiring surgery, with the strongest association in patients with disorders of psychological development (OR 2.9). No significant association was found with schizophrenia, schizotypal and delusional disorders, or mental retardation.
Conclusion: The findings indicate an increased probability of TMD among patients with a history of certain MBD diagnoses, and a stronger association with TMD requiring surgery, specifically repeated surgery. This highlights the need for improved preoperative understanding of the impact of MBD on TMD, as TMD and chronic pain itself may have a negative impact on mental health.
Keywords: TMD, registry-based, case-control, epidemiology, TMJ surgery, oral and maxillofacial surgery
Introduction
Temporomandibular disorder (TMD) is a collective term for multiple disorders affecting the muscles of mastication, the temporomandibular joint (TMJ), and the surrounding tissues and is characterized by orofacial pain and impaired function. TMD is usually reported to have a prevalence of 5% to 15% in the adult population, it is more prevalent in women, and the gender difference in persistent orofacial pain increases over time.1–3
Studies have found that psychological factors such as somatization, anxiety, depression, psychological distress, and pain-catastrophizing are predictors of both first onset of orofacial pain and chronic orofacial pain.4–10 The intensity of pain has also been shown to affect recovery after treatment.11 Furthermore, individuals with anxiety, depression, and substance use disorder have higher prevalence of other types of chronic pain, and the association seems to be bidirectional. However, studies on more severe mental disorders such as schizophrenia show inconclusive results with sometimes lower prevalence of chronic pain such as back pain and headaches in these patients.12
In Sweden, the vast majority of TMD patients are identified and receive conservative treatment within the dental care system and diagnostics are carried out using the Diagnostic Criteria for TMD (DC/TMD), which includes assessment of psychosocial functioning associated with the pain condition.13 Some patients might seek health care for their TMD symptoms and will be diagnosed within the health care system but subsequently treated within the dental care system. Of the patients diagnosed with TMD, only 1% are referred for surgical treatment.14 The surgical treatment of TMD in Sweden is conducted within the subsidized health care system and is mainly carried out on patients with articular disorders that have failed conservative treatment or patients with more complicated articular disorders such as fibrous or bony ankylosis.15
The International Classification of Diseases 10th Revision (ICD-10) (chapter 5) for mental and behavioral disorders (MBD) contains a heterogeneous group of diagnoses including a span of quite common diagnoses such as depression and anxiety as well as more rare diagnoses such as schizophrenia. Patients diagnosed or treated within the Swedish health care system are automatically registered in the National Patient Registry (NPR), which was initiated in 1964 and contains individual data from patient care with almost complete national coverage since 1987.16
This study from the Swedish National Registry Studies for Surgically Treated TMD (SWEREG-TMD) uses the unique prerequisites of prospectively collected population-based data to investigate the role of MBDs in the development of TMD. In addition, it investigates differences in odds for patients who are diagnosed but not treated for TMD within the health care system and patients who receive surgical treatment for TMD.
Material and Methods
Study Design and Registries
This is a registry-based case–control study with information collected from three nationwide population-based Swedish registries.
- The NPR was used to identify the cases and retrieve information on exposure variables. The registry is administered by the National Board of Health and Welfare (NBHW).16
- The Total Population Registry (TPR) was used to identify the controls. The registry is administered by Statistics Sweden (SCB) and has a coverage of 100% of all Swedish citizens.17
- The Longitudinal Integrated Database for Health Insurance and Labor Market Studies (LISA) was used to collect sociodemographic variables and is administered by SCB.18
Study Population and Data Linking
All study subjects included were aged 18 or above. Cases were all Swedish citizens diagnosed with TMD in a hospital or surgically treated for TMD between 1998 and 2016. The TPR was used to collect the controls, who were matched 1:10 on age, sex, and living area.
The Personal Identification Number (PIN) was used to link the subjects between the various registries and to collect data on exposure, outcome, comorbidities, and sociodemographic covariates. The PIN is given to all Swedish residents and is unique for each individual.19
Outcome
The definition of the outcome (TMD) was ICD-10 diagnostic code K07.6 (temporomandibular joint disorders) and/or any of the following treatment codes, which were used as proxy variables for TMD:
- TMJ-disc surgical procedure (EGB10)
- TMJ arthroscopy (EGA00)
- TMJ condylectomy (EGB00)
- TMJ prosthesis surgical procedure (EGC30)
- Other surgical reconstruction of TMJ (EGC99)
- TMJ synovectomy (EGB20)
- TMJ biopsy (EGA20)
- Injection of diagnostic or therapeutic substance in the TMJ (TEG10)
- TMJ condylotomy (EDC00)
- Open reposition of TMJ luxation (EGC00)
- TMJ plastic surgery (EGC10)
- TMJ plastic surgery with bone graft or other type of transplant (EGC20)
The cases were classified into three subcategories: non-surgical (NS) (ie, diagnosed but with no subsequent surgical treatment registered), surgically treated once (ST1) (ie, one surgical event), and surgically treated twice or more (ST2) (ie, multiple surgical interventions). Patients who had received bilateral surgical treatment on both TMJs but in one event were considered as surgically treated once. Injection of diagnostic or therapeutic substance in the TMJ (TEG10) was also considered a surgical intervention.
Exposures
NPR was used to collect information on MBD diagnoses for both cases and controls. Exposure data were defined as all diagnoses from the chapter 5 of ICD-10 (F00–F99) or equivalent diagnoses from earlier versions of ICD, between 1964 and time of TMD diagnosis (cases) or inclusion in the study (controls). ICD-7 to ICD-10 codes included were:
ICD-7 (1958–1968)
- Psychoses (300–309)
- Psychoneurotic disorders (310–318)
- Disorders of character, behavior and intelligence (320–326)
ICD-8 (1969–1986)
- Psychoses (290–299)
- Neuroses, personality disorders and other nonpsychotic mental disorders (300–309)
- Mental retardation (310–315)
ICD-9 (1987–1996)
- Mental disorders (290–319)
ICD-10 (1997–2016)
- Mental and behavioral disorders (F00–F99)
The translation between ICD-7, −8, and −9 to ICD-10 was conducted using a codebook provided by the NBHW. To present coherent results, the diagnoses were divided into 11 diagnostic categories in accordance with the ICD-10 divisions:
- Organic, including symptomatic, mental disorders (F00–F09)
- Mental and behavioral disorders due to psychoactive substance use (F10–F19)
- Schizophrenia, schizotypal and delusional disorders (F20–F29)
- Mood affective disorders (F30–F39)
- Neurotic, stress-related and somatoform disorders (F40–F48)
- Behavioral syndromes associated with physiological disturbances and physical factors (F50–F59)
- Disorders of adult personality and behavior (F60–F69)
- Mental retardation (F70–F79)
- Disorders of psychological development (F80–F89)
- Behavioral and emotional disorders with onset usually occurring in childhood and adolescence (F90–F98)
- Unspecified mental disorder (F99).
Sociodemographic Covariates and Comorbidities
Sociodemographic data were collected through LISA and included information on highest acquired educational level, country of birth, and living area. Educational level was divided into three levels: 0–9 years, 9–12 years, and more than 12 years. Birth country included Sweden, other Nordic Countries, European Countries, and non-European Countries. Sweden’s 290 municipalities were classified according to Eurostat’s Degree of Urbanization (DEGURBA) (revised definition, 2016): cities, towns or suburbs, and rural areas.
Information on comorbidity was collected from the NPR and included musculoskeletal and connective tissue diseases (M00-M99) and history of orofacial/neck trauma (S02.4, S02.6 and S13). The translation of diagnoses from earlier versions of ICD was conducted in the same manner as the exposure data (see “Exposures”). Chronic muscular disorders have been shown to affect both the risk for TMD and the development of mental health disorders such as anxiety and depression and was therefore considered a confounding factor.20–22 As history of trauma in the orofacial area and/or neck also affect both the exposure and the outcome it was included as a confounding factor.23–26
Statistical Methods
Conditional logistic regression was used to calculate odds ratios.27 Both outcome and exposures were considered binary variables, and adjustment variables were considered categorical dummy variables. Adjustment variables were educational level, country of birth, DEGURBA, musculoskeletal comorbidity, and history of orofacial/neck trauma. Musculoskeletal comorbidity and history of trauma were used as two independent binary adjustment variables to control for their presence and their influence on both mental health and the development of TMD. Missing data on educational level, country of birth, and DEGURBA were imputed using Multiple Imputation by Chained Equations (MICE).28 Educational level was imputed with ordinal logistic regression, whereas country of birth and DEGURBA were imputed with multinominal logistic regression, with 20 imputations and assuming missing at random.
Data Availability
The data that support the findings of this study are available from the Swedish NBHW and Statistics Sweden. Restrictions are applied to the availability of these data, which were used under license for this study. The data are not publicly available because of privacy and/or ethical restrictions but can be retrieved through the Swedish NBHW; however, approval from the Swedish Ethical Review Authority is required.
Ethical Declaration
This study was conducted in accordance with the Declaration of Helsinki and was comprised of a study population from Swedish national registries. The Swedish Ethical Review Authority approved the study (reference number 2018/401-31). The NBHW anonymized personal data before sending it to the researchers.
Results
A flowchart describing the recruitment process is presented in Figure 1, which is a modified model of earlier published data.29 The total study population consisted of 366 437subjects –33 315 cases and 333 122controls. In total, 120 individuals were excluded due to lack of index date or because of no possible match between the delivered data sets (see Figure 1). The case subgroups consisted of NS (n = 30 238), ST1 (n = 2443), and ST2 (n = 634). A total of 6201 cases and 40 486 controls were registered with MBD exposures in the NPR before inclusion in the study.
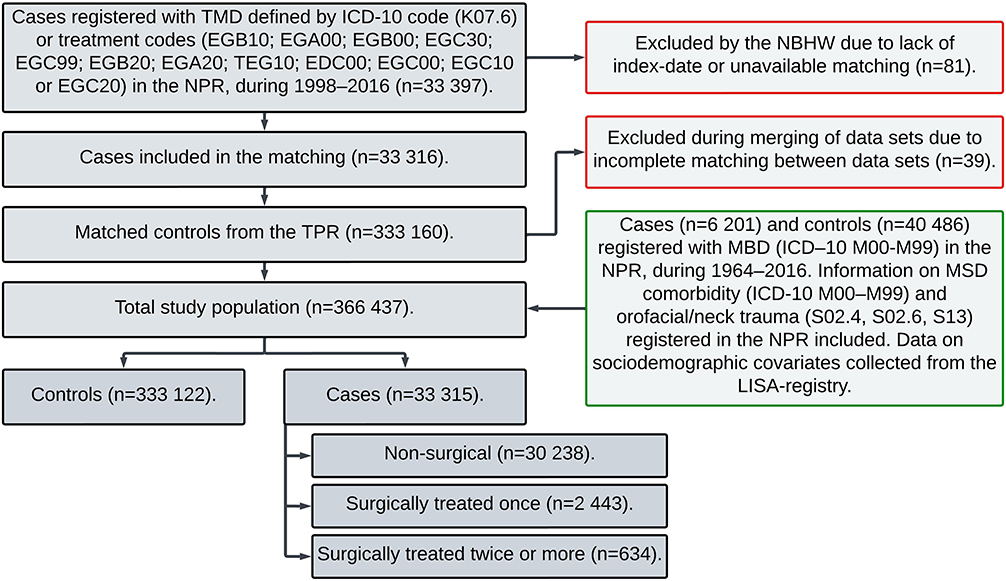 |
Figure 1 Recruitment process and registry inquiries of the study subjects as well as excluded subjects. The figure is a modified model of earlier published data. Abbreviations: ICD-10, International Classification of Diseases 10th Revision; LISA, Longitudinal Integrated Database for Health Insurance and Labor Market Studies; MBD, Mental and behavioral disorders; MSD, Musculoskeletal and connective tissue diseases; NBHW, National Board of Health and Welfare; NPR, National Patient Registry; TPR, Total Population Registry. |
Sociodemographic information and comorbidities of the study population are presented in Table 1. No large differences were seen in the baseline data, except for slightly lower ages in the surgically treated groups. The proportion of all musculoskeletal comorbidities was higher in the surgically treated subgroups. History of trauma was more common in the surgically treated groups.
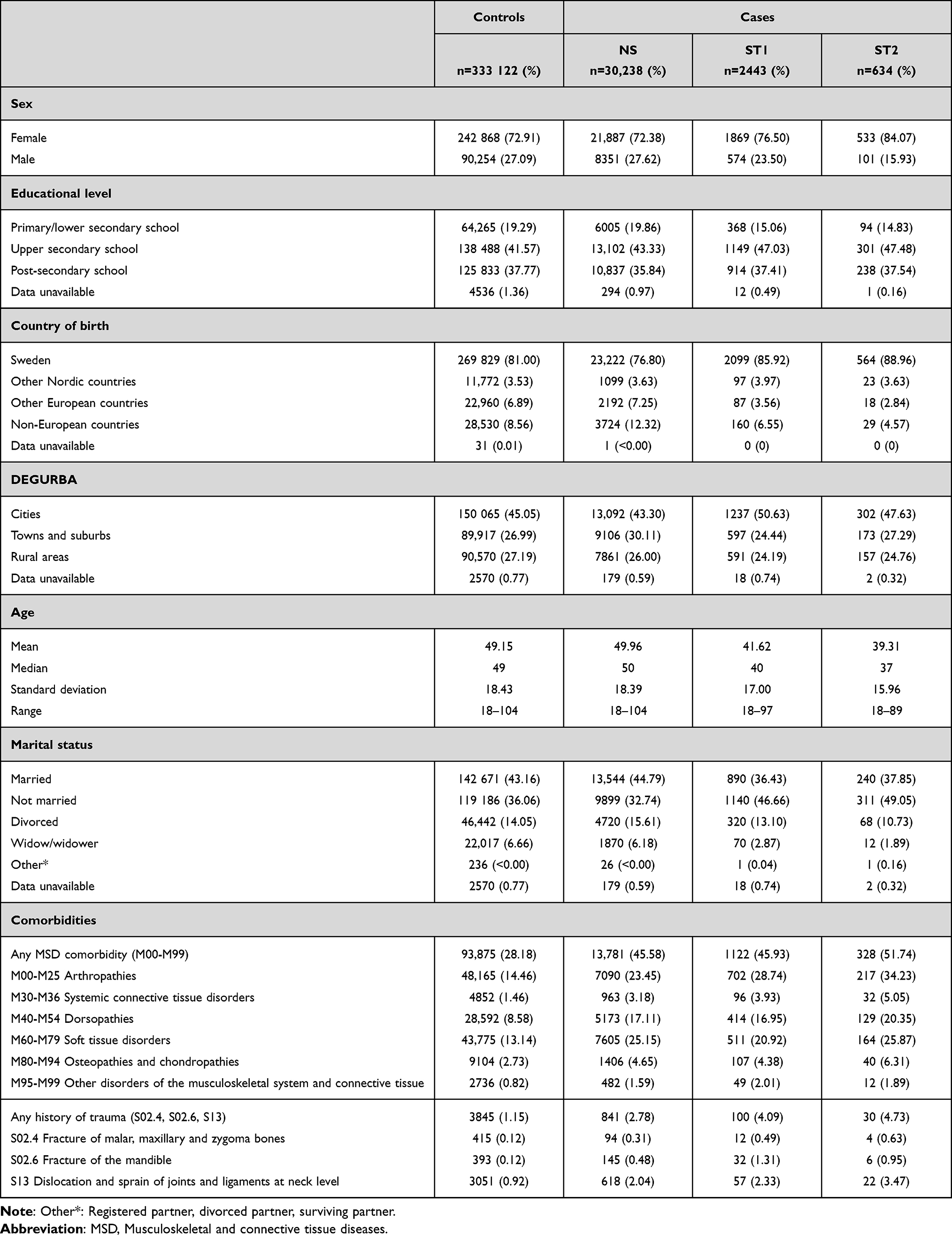 |
Table 1 The Sociodemographic Properties, MSD Comorbidity, and History of Orofacial/Neck Trauma of the Cases and Controls |
Table 2 displays the crude numbers and proportions of each category of ICD-10 MBD as well as each diagnosis contained in the 11 categories. Table 3 presents the results from the conditional logistic regression, which are shown with odds ratios for each diagnostic category regarding the entire case group (n = 33 315) and each subgroup of the cases. The model is adjusted for educational level, country of birth, DEGURBA, musculoskeletal comorbidity, and history of orofacial/neck trauma. Statistically significant association between MBD and TMD was found in individuals with mood affective disorders (OR 1.4, 95% CI 1.4–1.5), neurotic, stress-related and somatoform disorders (OR 1.7, 95% CI 1.7–1.8), behavioral syndromes associated with psychological disturbances and physical factors (OR1.4, 95% CI 1.3–1.5), disorders of adult personality and behavior (OR 1.4, 95% CI 1.3–1.5), disorders of psychological development (OR 1.3, 95% CI 1.2–1.4), behavioral and emotional disorders with onset usually occurring in childhood and adolescence (OR 1.4, 95% CI 1.4–1.5), and unspecified mental disorder (OR 1.3, 95% CI 1.2–1.4). The association between MBD and TMD was stronger in cases who had received surgical treatment, particularly cases with multiple surgical interventions. The odds increased up to two-fold for neurotic, stress-related and somatoform disorders, behavioral syndromes associated with physiological disturbances and physical factors, disorders of adult personality and behavior, behavioral and emotional disorders with onset usually occurring in childhood and adolescence, and unspecified mental disorders. The strongest association between MBD and TMD was found in cases who had received several surgical interventions and who had earlier been diagnosed with disorders of psychological development (OR 2.9).
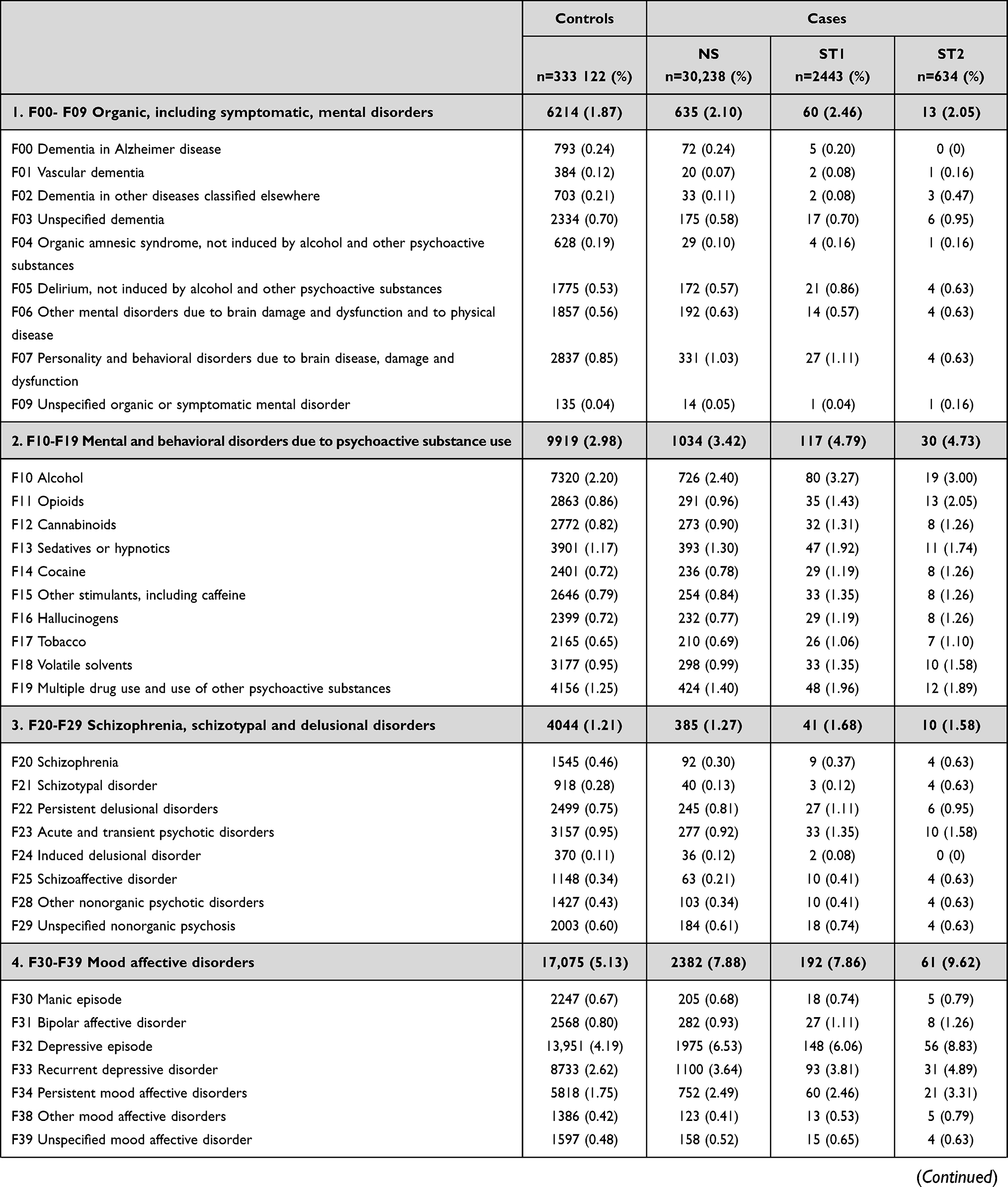 | 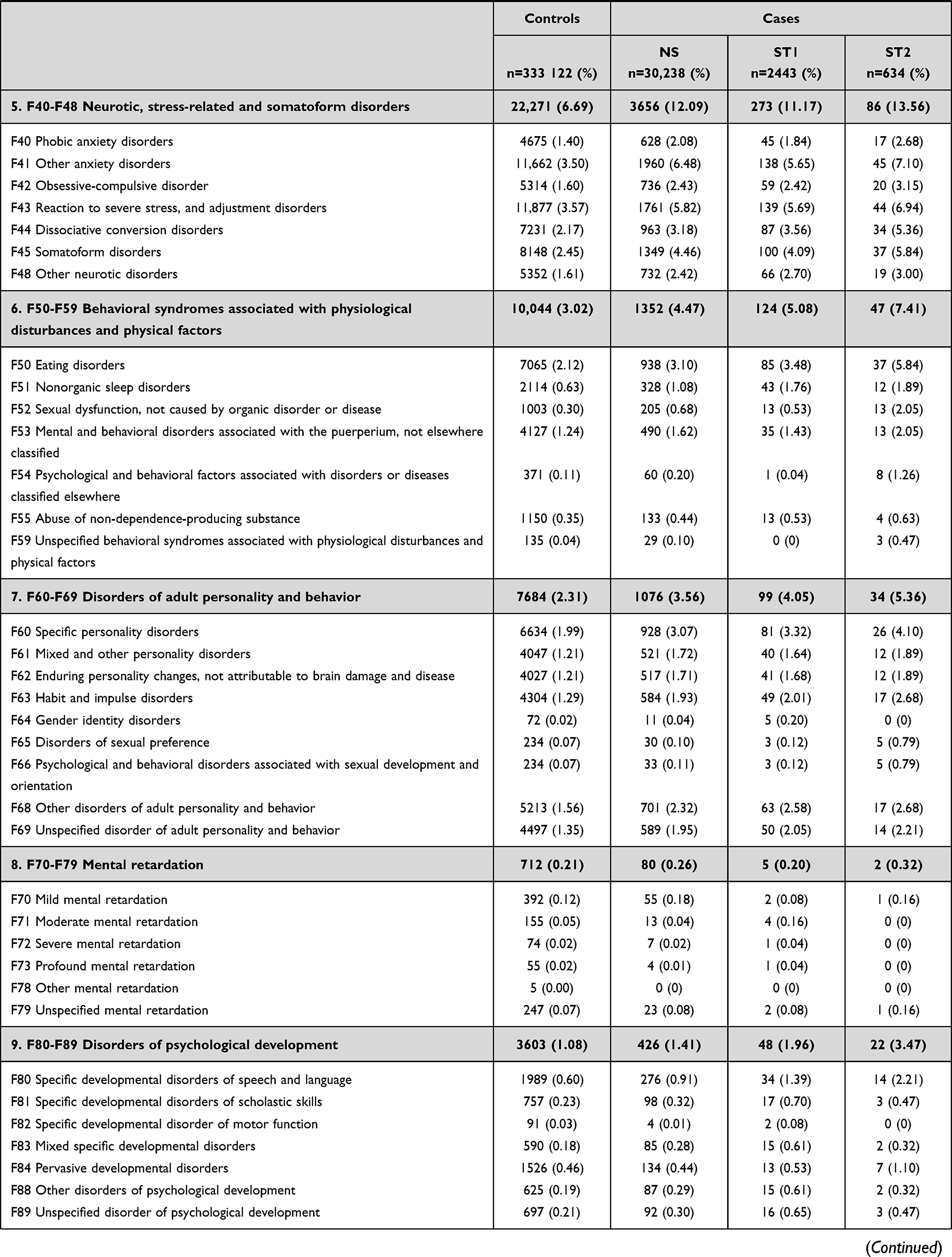 | 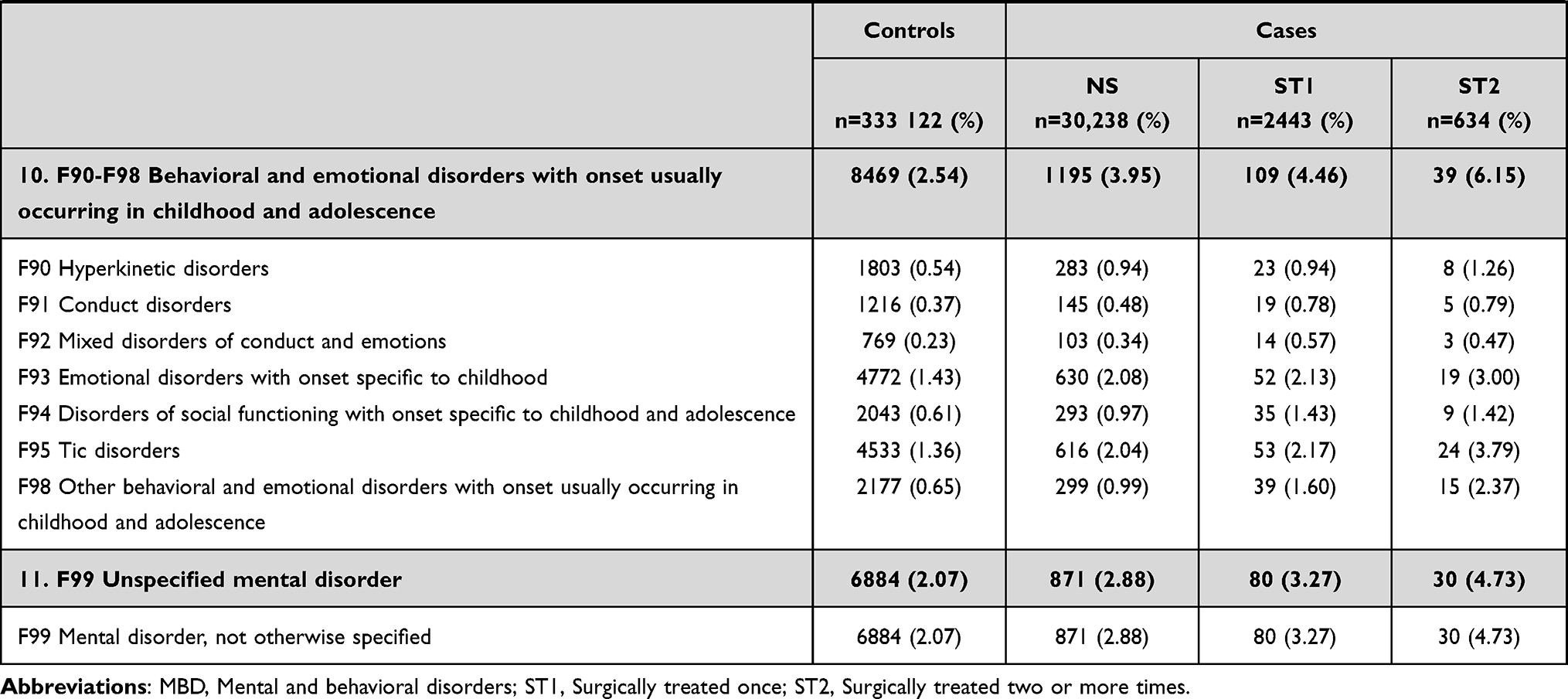 |
Table 2 Crude Data on Number of Subjects with MBD-Diagnoses from Chapter 5 of ICD-10 (F00–F99) and the Division into the 11 Categories of the Chapter |
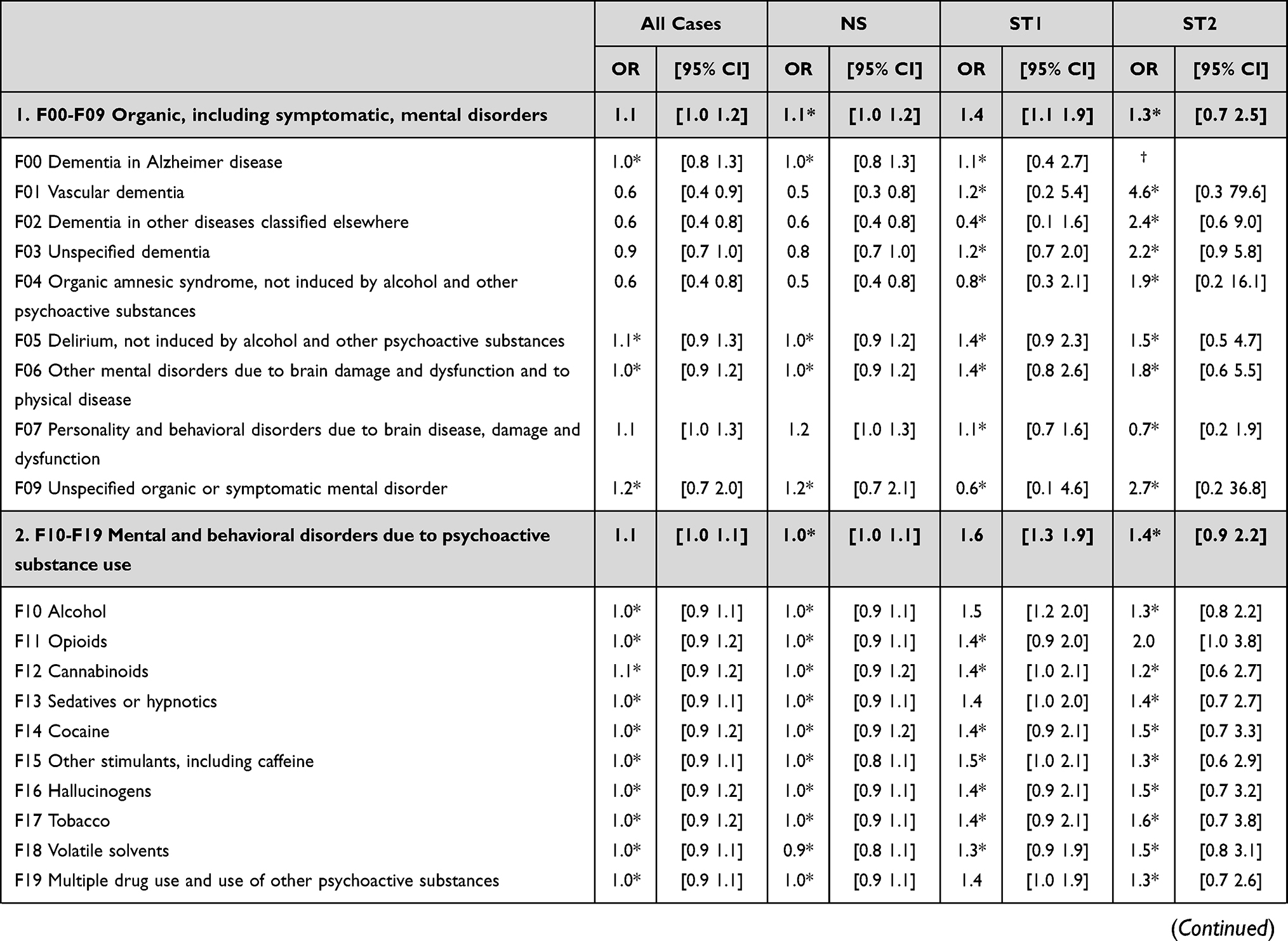 | 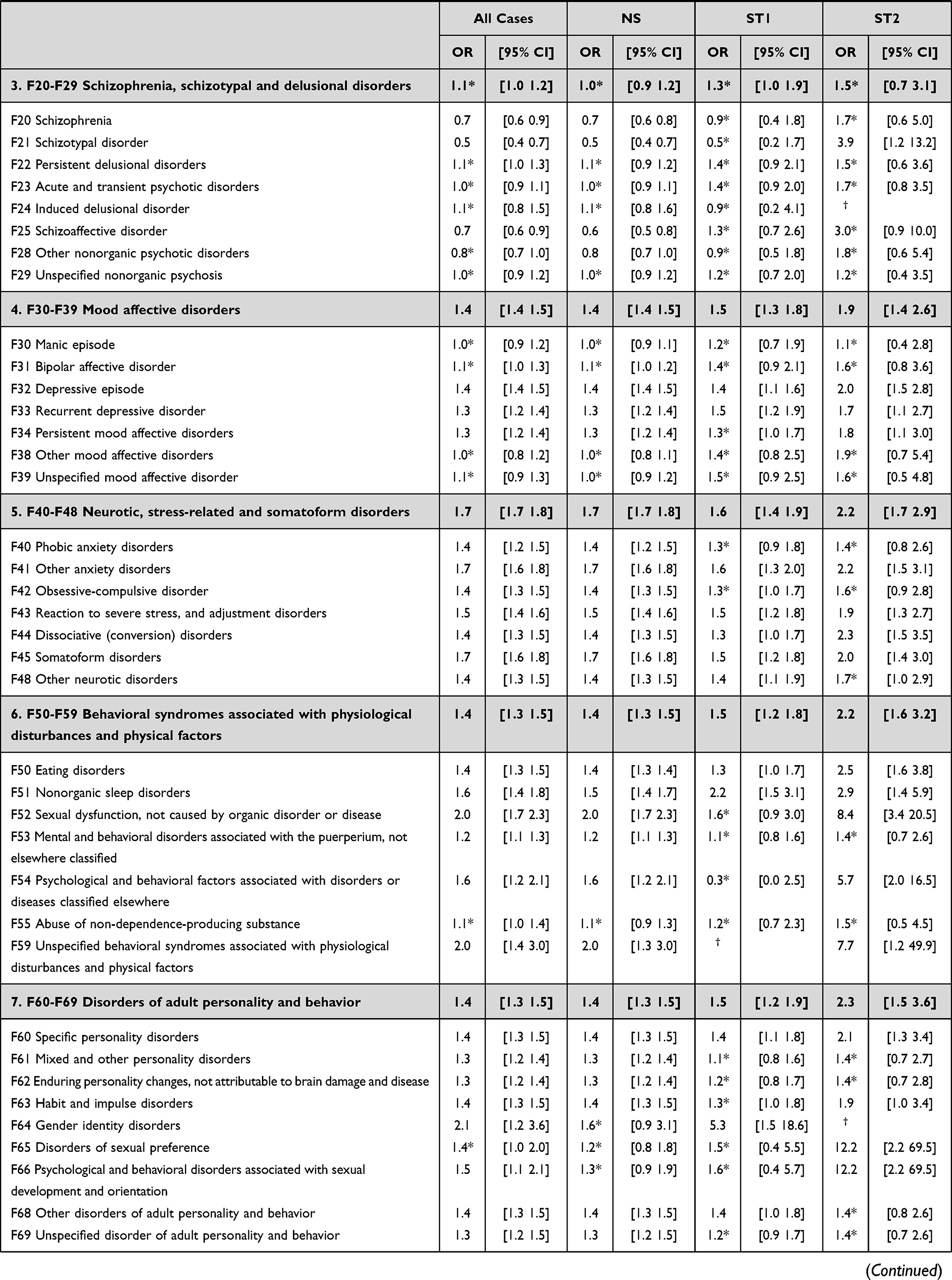 | 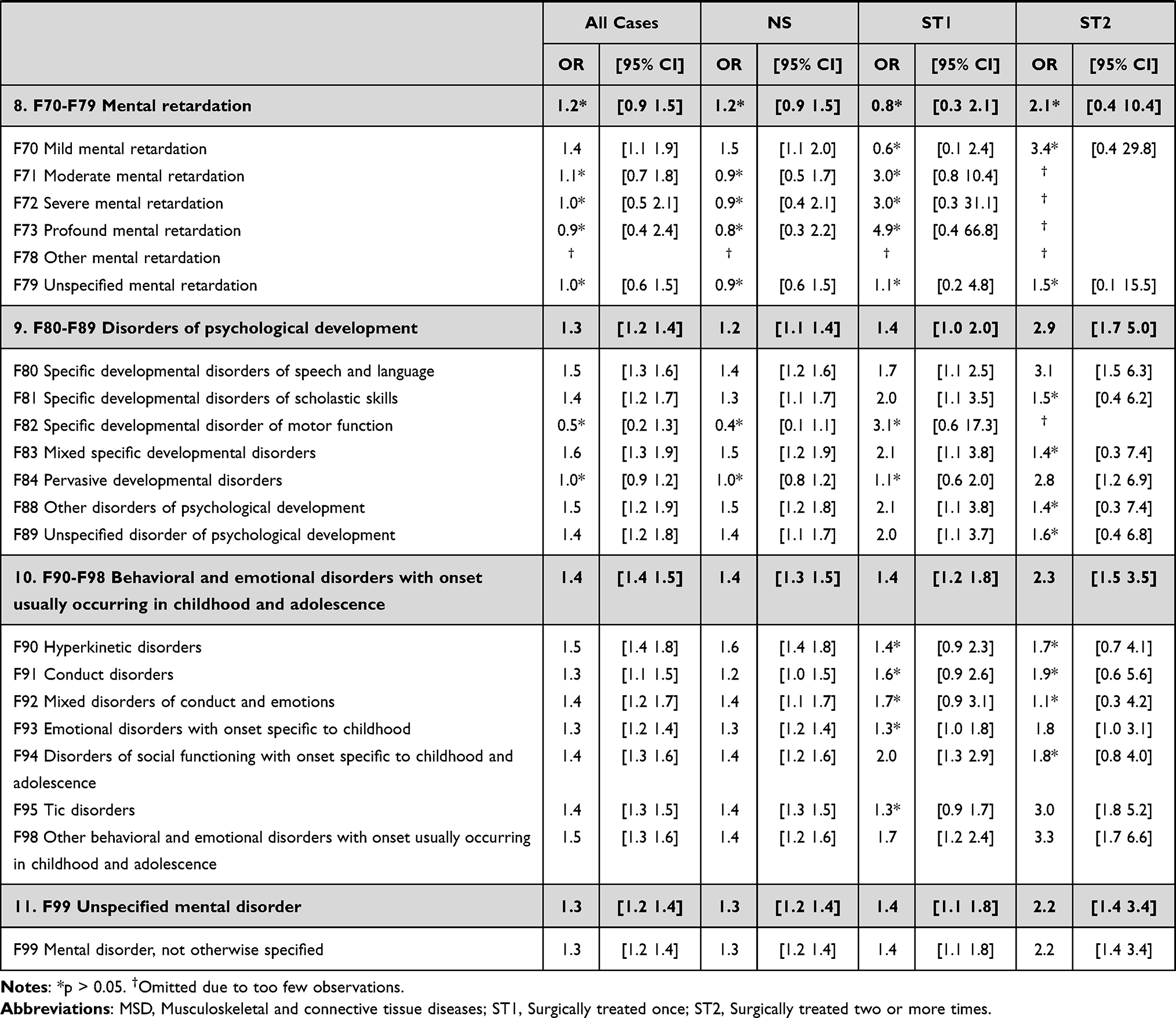 |
Table 3 Odds Ratios of the Outcome in Relation to the Exposures. Calculated Through Conditional Logistic Regression and Adjusted for Educational Level, Country of Birth, DEGURBA, MSD Comorbidity, and History of Orofacial/Neck Trauma |
Slightly, albeit statistically significant, elevated probability of TMD was seen in patients with organic disorders, including symptomatic disorders (OR 1.1, 95% CI 1.0–1.2) and mental and behavioral disorders due to psychoactive substance use (OR 1.1, 95% CI 1.0–1.1), these results are not expected to have any clinical relevance. No significant association between MBD and TMD was found in patients with schizophrenia, schizotypal, delusional disorders, or mental retardation.
Discussion
This study showed that there is a strong association between certain diagnoses of MBD and TMD diagnosed and treated in a hospital setting, with stronger associations in TMD requiring surgical treatment. The relation between mental health and TMD is complex, but understanding it is imperative when dealing with patients with TMD as well as with patients with impaired mental health who might be at risk of developing chronic pain conditions. Since this study relied on prospective registry data, the risk of temporal bias, which is often associated with case–control studies, has decreased. Indeed, as with earlier findings, the results here indicate that there is a strong association present, although it is important to acknowledge that the establishment of a true casual relation requires other study designs, and that TMD itself may cause impaired psychosocial abilities thereby creating a causal nexus.30,31 This is another important reason for physicians to be familiar with the quite common conditions within the TMD umbrella and to refer patients who present with onset orofacial pain or chronic orofacial pain at an early stage.
Pain, which is the most common symptom of TMD, is associated with depression, anxiety, and stress, three psychological conditions that have a modifying role in TMD.8,32–36 In addition, women have been found to experience chronic pain more often than men, a gender difference that could be related to both societal and biological factors.37 Comorbidity of chronic physical and mental disorders are also risk factors for chronic pain even after adjusting for well-known confounders, such as age, education, and gender.37 This is interesting considering the recognized fact that TMD patients are predominantly female as well as the obvious predisposition of comorbid diseases presented in this study. The intricate nexus of risks for chronic pain and TMD suggests that multimodal care and focused screening methods should be considered. The screening could be applied when selecting patients for TMJ surgery, with the goal of not initiating surgical intervention in patients where the rate of success is likely lower or the risk for reoperation is increased. Multimodal care and screening methods could also be applied at an earlier stage in close collaboration with oral pain clinics and in other instances of health care such as orthopedic or rheumatology clinics. These early screenings could focus on identifying early signs of TMD. National guidelines could help health care providers identify patients who should be referred for conservative treatment at an earlier stage, possibly preventing them from developing surgically demanding TMD.
Often, more severe psychiatric diagnoses are considered as absolute contraindicators of surgical treatment, but the results of this study, which might be indicative of a causal association between certain MBD and TMD, indicate that these premises perhaps need to be re-evaluated. If the cause-effect between impaired TMD and impaired mental health is bilateral, there is a possibility that the treatment of TMD, both surgical and conservative, might have the same bilateral effect. If treatment can relieve the patient from TMD symptoms, it may be possible that the psychosocial burden is reduced as well, emphasizing the need for early conservative treatment, perhaps in some form of subsidized treatment program from the health care system. The importance of optimizing treatment of MBD before TMD treatment should not be underestimated, and the impact of underlying diseases, such as MBD, and the effect on TMD treatment response should be investigated further both in relation to conservative and surgical treatment.
Preoperative psychological factors have been of interest for a long time, where methods examining the locus of control described by Rotter and later Wallston have been used to predict surgical outcome and pain management postoperatively, for example, in hand surgery.38–40 More recently, Howard L Fields, describing the influence of the expectations of pain, concluded that the expectation of perceived pain is particularly important in persistent or recurrent pain such as in arthritis or chronic headache. He further described early treatment failure as a predictor itself as it may become a self-fulfilling prophecy. As most patients who are surgically treated for TMD have foregone conservative treatment that most likely would have failed to alleviate their symptoms, correctly targeted early and adequate interventions are emphasized. Similarly, pain catastrophizing has been shown to be predictive of TMD pain and should also be evaluated when considering treatment modality.7,10
The results of this study repeatedly showed stronger associations between MBD and TMD in cases who had undergone surgical treatment, with many times a two-fold increase in probability. Whether this association is the result of more severe TMD symptoms in patients with these underlying diseases and whether there is an increased risk of failing conservative treatment as the result of MBD are interesting questions; however, these questions are outside the framework of this study. Other studies that have investigated the effect of preoperative anxiety and depression on post-surgical outcome have conflicting results. Patients with preoperative depression have been found to have significantly reduced postoperative gains in quality of life after endoscopic sinus surgery, and depression has been shown to increase hospital length following coronary bypass graft surgery.41,42 However, in a study on total hip or knee arthroplasty, patients with preoperative anxiety and/or depression had similar outcomes as patients without these premorbid conditions.43 Similarly, a 2017 review study concluded that there were inconclusive results in the abilities to predict postoperative pain due to preoperative depression and concluded that further studies are needed.44 It might also be of importance to consider the iatrogenic effects of surgical treatment, especially for aging patients with ongoing neurodegeneration, as the neuroinflammation caused by the surgical trauma itself may be the driver of further neurocognitive complications such as dementia or delirium.45 Furthermore, neuroinflammation has also been suggested to alter pain perception and sensitization in individuals with attention-deficit/hyperactivity disorder (ADHD). In this study, subjects with behavioral and emotional disorders with onset usually occurring in childhood and adolescence (F90-F98), which include neuropsychiatric disorders such as ADHD, autistic spectrum disorders and tic disorders, had a high probability of developing TMD. The odds of developing TMD that requires multiple surgical interventions were more than doubled in comparison to individuals without these comorbidities. ADHD not only increases the risk of mental health and social difficulties but is also strongly associated with extreme pain.46,47 In pediatric study populations neuropsychiatric symptoms have been shown to affect how pain interferes with daily activities, and children with ADHD have even been suggested to be at increased risk of developing TMD.48,49 Considering that the rates of ADHD are fairly consistent in Western countries, and that research is increasingly showing the substantial impact of ADHD on functioning, more studies on the association with TMD will advance the knowledge of how treatment of neuropsychiatric disorders might be incorporated in the management of orofacial pain.50
The strength of this study design is that it uses population-based data based on comprehensive and accurate national registries. The prospective nature of the registry data from NPR allows for assuming a temporal relationship between diagnoses of MBD and TMD, and the NPR has been validated with high reliability for many of the MBD diagnoses, but not all.51–55 The largest weakness is that patients with TMD who do not require surgery but still receive a TMD diagnosis within the health care system represent a small part of the entire population, as most TMD patients in Sweden are both diagnosed and treated within the dental care system and therefore are not available in the NPR. These patients (NS) might represent a subset of the TMD population that for some reason are diagnosed within the health care system. This also means that there might be a considerable proportion of TMD patients within the control group, that have not been diagnosed within the hospital care system and thereby cause misclassification bias. However, such misclassification could most likely be considered bias towards the null.
In conclusion, the findings of this study indicate a strong association between mood affective disorders, neurotic, stress-related and somatoform disorders, behavioral syndromes associated with physiological disturbances and physical factors, disorders of adult personality and behavior, disorders of the psychological development, unspecified mental disorder, and the development of TMD. These associations suggest a causal effect, and the association seems to be stronger for TMD requiring surgery, in particular repeated surgery. The results highlight the need of multimodal care of patients with combined MBD and pain disorders, suggesting the implementation of screening methods that can identify patients with early signs of TMD as the result of MBD conditions. These types of screenings could be used to identify patients who could benefit from conservative treatment at an earlier stage. Preoperative screening for psychosocial factors could also be used to identify patients who might be at risk of persistent postoperative pain after TMJ surgery, information that can be used to design postoperative treatment plans that anticipate this pain. These results emphasize the importance of early detection and initiation of relevant treatment. In addition, these results, in terms of articular problems, suggest preferentially involving a close interdisciplinary collaboration between dental and medical specialists, such as orofacial pain specialists, TMJ surgeons, pain specialists, psychologists, and psychiatrists to obtain precision treatment.
Abbreviations
DC/TMD, Diagnostic Criteria for Temporomandibular Disorders; DEGURBA, Eurostat’s Degree of Urbanization; ICD-10, International Classification of Diseases 10th Revision; LISA, The Longitudinal Integrated Database for Labor Market and Health Insurance Studies; MBD, Mental and behavioral disorders; MSD, Musculoskeletal and connective tissue diseases; NBHW, National Board of Health and Welfare; NPR, National Patient Registry; PIN, Personal Identification Number; SCB, Statistics Sweden; ST1, Surgically treated once; ST2, Surgically treated two or more times; SWEREG-TMD, Swedish National Registry Studies for Surgically Treated TMD; TMD, Temporomandibular Disorders; TMJ, Temporomandibular Joint; TPR, Total Population Registry.
Acknowledgments
This research was funded by the Swedish Public Dental Services, Folktandvården Stockholm AB, and Steering Group for Collaborative Odontological Research at Karolinska Institutet and Stockholm City County.
Disclosure
The authors report no conflicts of interest in this work. All authors approved the final version of this article.
References
1. LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8(3):291–305. doi:10.1177/10454411970080030401
2. Lövgren A, Häggman-Henrikson B, Visscher CM, Lobbezoo F, Marklund S, Wänman A. Temporomandibular pain and jaw dysfunction at different ages covering the lifespan–A population based study. Eur J Pain. 2016;20(4):532–540. doi:10.1002/ejp.755
3. Häggman-Henrikson B, Liv P, Ilgunas A, et al. Increasing gender differences in the prevalence and chronification of orofacial pain in the population. Pain. 2020;161(8):1768–1775. doi:10.1097/j.pain.0000000000001872
4. Macfarlane TV, Blinkhorn AS, Davies RM, Kincey J, Worthington HV. Predictors of outcome for orofacial pain in the general population: a four-year follow-up study. J Dent Res. 2004;83(9):712–717. doi:10.1177/154405910408300911
5. LeResche L, Mancl LA, Drangsholt MT, Huang G, Von Korff M. Predictors of onset of facial pain and temporomandibular disorders in early adolescence. Pain. 2007;129(3):269–278. doi:10.1016/j.pain.2006.10.012
6. Aggarwal VR, Macfarlane GJ, Farragher TM, McBeth J. Risk factors for onset of chronic oro-facial pain–results of the North Cheshire oro-facial pain prospective population study. Pain. 2010;149(2):354–359. doi:10.1016/j.pain.2010.02.040
7. Reiter S, Eli I, Mahameed M, et al. Pain catastrophizing and pain persistence in temporomandibular disorder patients. J Oral Facial Pain Headache. 2018;32(3):309–320. doi:10.11607/ofph.1968
8. Staniszewski K, Lygre H, Bifulco E, et al. Temporomandibular disorders related to stress and HPA-axis regulation. Pain Res Manag. 2018;2018:7020751. doi:10.1155/2018/7020751
9. Sójka A, Stelcer B, Roy M, Mojs E, Pryliński M. Is there a relationship between psychological factors and TMD? Brain Behav. 2019;9(9):e01360. doi:10.1002/brb3.1360
10. Willassen L, Johansson AA, Kvinnsland S, Staniszewski K, Berge T, Rosén A. Catastrophizing has a better prediction for TMD than other psychometric and experimental pain variables. Pain Res Manag. 2020;2020:7893023. doi:10.1155/2020/7893023
11. Staniszewski K, Willassen L, Berge T, Johansson A, Schjødt B, Rosen A. High pain intensity is a risk factor of non-resolving TMD: a three-year follow-up of a patient group in a Norwegian interdisciplinary evaluation program. J Pain Res. 2022;15:1283–1296. doi:10.2147/JPR.S341861
12. Velly AM, Mohit S. Epidemiology of pain and relation to psychiatric disorders. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(PtB):159–167. doi:10.1016/j.pnpbp.2017.05.012
13. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria For Temporomandibular Disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and orofacial pain special interest groupdagger. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
14. Widmark G. On surgical intervention in the temporomandibular joint. Swed Dent J Suppl. 1997;123:1–87.
15. Dimitroulis G. Management of temporomandibular joint disorders: a surgeon’s perspective. Aust Dent J. 2018;63(Suppl 1):S79–S90. doi:10.1111/adj.12593
16. Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11(1):450. doi:10.1186/1471-2458-11-450
17. Ludvigsson JF, Almqvist C, Bonamy AK, et al. Registers of the Swedish total population and their use in medical research. Eur J Epidemiol. 2016;31(2):125–136. doi:10.1007/s10654-016-0117-y
18. Ludvigsson JF, Svedberg P, Olén O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–437. doi:10.1007/s10654-019-00511-8
19. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur J Epidemiol. 2009;24(11):659–667. doi:10.1007/s10654-009-9350-y
20. Ayouni I, Chebbi R, Hela Z, Dhidah M. Comorbidity between fibromyalgia and temporomandibular disorders: a systematic review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019;128(1):33–42. doi:10.1016/j.oooo.2019.02.023
21. Pantoja LLQ, De toledo IP, Pupo YM, et al. Prevalence of degenerative joint disease of the temporomandibular joint: a systematic review. Clin Oral Investig. 2019;23(5):2475–2488. doi:10.1007/s00784-018-2664-y
22. Patten SB, Williams JV, Wang J. Mental disorders in a population sample with musculoskeletal disorders. BMC Musculoskelet Disord. 2006;7(1):37. doi:10.1186/1471-2474-7-37
23. Khan J, Zusman T, Wang Q, Eliav E. Acute and chronic pain in orofacial trauma patients. Dent Traumatol. 2019;35(6):348–357. doi:10.1111/edt.12493
24. Nazarevych M, Ohonovskyi R, Pohranychna K, Mokryk O, Melnychuk Y, Stasyshyn A. Frequency and nature of disorders in psycho-emotional and autonomic systems in patients with middle facial injury. Wiad Lek. 2022;75(1 pt 2):197–202. doi:10.36740/WLek202201209
25. Sterling M, Hendrikz J, Kenardy J. Compensation claim lodgement and health outcome developmental trajectories following whiplash injury: a prospective study. Pain. 2010;150(1):22–28. doi:10.1016/j.pain.2010.02.013
26. Sharma S, Ohrbach R, Fillingim RB, Greenspan JD, Slade G. Pain sensitivity modifies risk of injury-related temporomandibular disorder. J Dent Res. 2020;99(5):530–536. doi:10.1177/0022034520913247
27. Koletsi D, Pandis N. Conditional logistic regression. Am J Orthod Dentofacial Orthop. 2017;151(6):1191–1192. doi:10.1016/j.ajodo.2017.04.009
28. White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med. 2011;30(4):377–399. doi:10.1002/sim.4067
29. Salinas Fredricson A, Krüger Weiner C, Adami J, et al. Sick leave and disability pension in a cohort of TMD-patients - The Swedish National Registry Studies for Surgically Treated TMD (SWEREG-TMD). BMC Public Health. 2022;22(1):916. doi:10.1186/s12889-022-13329-z
30. Fillingim RB, Ohrbach R, Greenspan JD, et al. Psychological factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013;14(12 Suppl):T75–90. doi:10.1016/j.jpain.2013.06.009
31. Fillingim RB, Slade GD, Greenspan JD, et al. Long-term changes in biopsychosocial characteristics related to temporomandibular disorder: findings from the OPPERA study. Pain. 2018;159(11):2403–2413. doi:10.1097/j.pain.0000000000001348
32. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433–2445. doi:10.1001/archinte.163.20.2433
33. Andias R, Silva AG. Impact of sex, sleep, symptoms of central sensitization and psychosocial factors in adolescents with chronic musculoskeletal pain-an exploratory study. Pain Med. 2022. doi:10.1093/pm/pnac053
34. Al-Khotani A, Naimi-Akbar A, Gjelset M, et al. The associations between psychosocial aspects and TMD-pain related aspects in children and adolescents. J Headache Pain. 2016;17(1):30. doi:10.1186/s10194-016-0622-0
35. List T, Jensen RH. Temporomandibular disorders: old ideas and new concepts. Cephalalgia. 2017;37(7):692–704. doi:10.1177/0333102416686302
36. Nazeri M, Ghahrechahi HR, Pourzare A, et al. Role of anxiety and depression in association with migraine and myofascial pain temporomandibular disorder. Indian J Dent Res. 2018;29(5):583–587. doi:10.4103/0970-9290.244932
37. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e283. doi:10.1016/j.bja.2019.03.023
38. Rotter JB. Generalized expectancies for internal versus external control of reinforcement. Psychol Monogr. 1966;80(1):1–28. doi:10.1037/h0092976
39. Wallston KA, Wallston BS, DeVellis R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ Monogr. 1978;6(2):160–170. doi:10.1177/109019817800600107
40. Stewart JA, Aebischer V, Egloff N, et al. The role of health locus of control in pain intensity outcome of conservatively and operatively treated hand surgery patients. Int J Behav Med. 2018;25(3):374–379. doi:10.1007/s12529-018-9713-4
41. AbuRuz ME. Pre-operative depression predicted longer hospital length of stay among patients undergoing coronary artery bypass graft surgery. Risk Manag Healthc Policy. 2019;12:75–83. doi:10.2147/RMHP.S190511
42. Ospina J, Liu G, Crump T, Sutherland JM, Janjua A. The impact of comorbid depression in chronic rhinosinusitis on post-operative sino-nasal quality of life and pain following endoscopic sinus surgery. J Otolaryngol Head Neck Surg. 2019;48(1):18. doi:10.1186/s40463-019-0340-0
43. Seagrave KG, Lewin AM, Harris IA, Badge H, Naylor J. Association between pre-operative anxiety and/or depression and outcomes following total Hip or knee arthroplasty. J Orthop Surg. 2021;29(1):2309499021992605. doi:10.1177/2309499021992605
44. Dadgostar A, Bigder M, Punjani N, Lozo S, Chahal V, Kavanagh A. Does preoperative depression predict post-operative surgical pain: a systematic review. Int J Surg. 2017;41:162–173. doi:10.1016/j.ijsu.2017.03.061
45. Yang T, Velagapudi R, Terrando N. Neuroinflammation after surgery: from mechanisms to therapeutic targets. Nat Immunol. 2020;21(11):1319–1326. doi:10.1038/s41590-020-00812-1
46. Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet. 2016;387(10024):1240–1250. doi:10.1016/S0140-6736(15)00238-X
47. Stickley A, Koyanagi A, Takahashi H, Kamio Y. ADHD symptoms and pain among adults in England. Psychiatry Res. 2016;246:326–331. doi:10.1016/j.psychres.2016.10.004
48. Suligowska K, Mikietyńska M, Pakalska-Korcala A, Wolańczyk T, Prośba-Mackiewicz M, Zdrojewski T. Parafunctions, signs and symptoms of Temporomandibular Disorders (TMD), in children with Attention-Deficit Hyperactivity Disorder (ADHD): the results of the SOPKARD-Junior study. Psychiatr Pol. 2021;55(4):887–900. doi:10.12740/PP/OnlineFirst/113438
49. Balter LJT, Wiwe Lipsker C, Wicksell RK, Lekander M. Neuropsychiatric symptoms in pediatric chronic pain and outcome of acceptance and commitment therapy. Front Psychol. 2021;12:576943. doi:10.3389/fpsyg.2021.576943
50. Cortese S, Coghill D. Twenty years of research on attention-deficit/hyperactivity disorder (ADHD): looking back, looking forward. Evid Based Ment Health. 2018;21(4):173–176. doi:10.1136/ebmental-2018-300050
51. Dalman C, Broms J, Cullberg J, Allebeck P. Young cases of schizophrenia identified in a national inpatient register–are the diagnoses valid? Soc Psychiatry Psychiatr Epidemiol. 2002;37(11):527–531. doi:10.1007/s00127-002-0582-3
52. Ekholm B, Ekholm A, Adolfsson R, et al. Evaluation of diagnostic procedures in Swedish patients with schizophrenia and related psychoses. Nord J Psychiatry. 2005;59(6):457–464. doi:10.1080/08039480500360906
53. Sellgren C, Landén M, Lichtenstein P, Hultman CM, Långström N. Validity of bipolar disorder hospital discharge diagnoses: file review and multiple register linkage in Sweden. Acta Psychiatr Scand. 2011;124(6):447–453. doi:10.1111/j.1600-0447.2011.01747.x
54. Rück C, Larsson KJ, Lind K, et al. Validity and reliability of chronic tic disorder and obsessive-compulsive disorder diagnoses in the Swedish National Patient Register. BMJ Open. 2015;5(6):e007520. doi:10.1136/bmjopen-2014-007520
55. Kouppis E, Ekselius L. Validity of the personality disorder diagnosis in the Swedish National Patient Register. Acta Psychiatr Scand. 2020;141(5):432–438. doi:10.1111/acps.13166
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.