")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Role of Mental Adjustment in Mediating Post-Traumatic Stress Disorder Symptoms and Social Support in Chinese Ovarian Cancer Patients: A Cross-Sectional Study
Authors Pang X, Li F , Zhang Y
Received 28 April 2022
Accepted for publication 26 July 2022
Published 12 August 2022 Volume 2022:15 Pages 2183—2191
DOI https://doi.org/10.2147/PRBM.S372660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xiaoyan Pang, Fangmei Li, Yi Zhang
Department of Gynecology, the First Hospital of China Medical University, Shenyang, Liaoning, 110001, People’s Republic of China
Correspondence: Yi Zhang, Department of Gynecology, the First Hospital of China Medical University, Shenyang, Liaoning, 110001, People’s Republic of China, Email [email protected]
Background: Post-traumatic stress disorder (PTSD) can manifest in individuals following a traumatic event. There is a paucity of studies focusing on PTSD symptoms in ovarian cancer (OC) patients. This study aimed to investigate the association of social support, mental adjustment and PTSD symptoms in Chinese OC patients with a view to exploring whether mental adjustment could mediate the relationship.
Methods: A cross-sectional study was conducted from January 2015 to December 2016. A total of 171 OC subjects were recruited and the effective response rate was 81.3%. The PTSD Checklist-Civilian Version (PCL-C), Mini-Mental Adjustment to Cancer scale (Mini-MAC) and Duke-UNC Functional Social Support Questionnaire were disseminated to the patients. The Chinese Mini-MAC was used in this study focusing on three components, namely negative emotion, positive attitude, and cognitive avoidance. Hierarchical linear regression analyses were employed to investigate the association of social support and PTSD symptoms, and the role of mental adjustment in their mediation.
Results: The prevalence of PTSD symptoms was 17.3% in OC patients. PTSD symptoms were negatively related with both social support and positive attitude, and positively associated with negative emotion and cognitive avoidance. Social support was negatively associated with negative emotion and cognitive avoidance, and positively related with positive attitude. In addition, negative emotion and positive attitude mediated the association between social support and PTSD symptoms.
Conclusion: PTSD symptoms in OC patients should be paid attention to. Social support and mental adjustment were positive resources associated with PTSD symptoms. Moreover, mental adjustment could mediate the relation between social support and PTSD symptoms in OC patients. Therefore, intervention management that focusing on improving perceived social support as well as strengthening mental adjustment, especially negative emotion and positive attitude, may be useful for reducing PTSD symptoms in this context.
Keywords: social support, mental adjustment, post-traumatic stress disorder, ovarian cancer
Introduction
Ovarian cancer (OC) is the most common cause of mortality in women with gynecologic malignancies.1 Due to the lack of specific symptoms, OC is typically in the advanced stage at diagnosis with extensive metastases. Consequently, even following surgical cytoreduction and adjuvant chemotherapy, the overall 5-year survival rate is only 49%.1 Most OC patients suffer from severe physical, psychological, and even social consequences.
Post-traumatic stress disorder (PTSD) is characterized by severe psychological responses to a traumatic event, such as an earthquake, a war, or sexual assault.2–4 Specific clusters of symptoms exist in PTSD, including trauma-related intrusive thoughts and memories, avoidance tactics, and hyperarousal. Individuals with PTSD reported a decline in physical, mental, and social function, in addition to reduced quality of life.5 PTSD was applied to cancer patients when the Fourth Edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) diagnostic criteria were expanded to a broader variety of traumatic events, including life-threatening disease.6 Changes in DSM-5 diagnostic criteria for PTSD raise specific concerns on the evaluation of cancer-related PTSD, since they state that a life-threatening disease or debilitating medical condition is not necessarily considered a traumatic event.7 Therefore, for cancer patients to meet criterion A, the individual must be exposed to acute, severe complications or other extreme adverse events. The majority of patients with OC will be treated with surgery and chemotherapy, and a few of them will lose reproductive function, posing the patients in a traumatic condition. In addition, the unpredictability and uncontrollability of surgery and prognosis might induce and exacerbate depress and fear. The reported prevalence of OC-related PTSD among various studies is inconsistent, ranging from 0 to 45%.8–13 Our previous study focused on prevalence of PTSD symptoms in Chinese OC patients, and found that hope and resilience partly mediated the correlation between social support and PTSD symptoms.10 Therefore, the present study aimed to further explore the role of mental adjustment.
Social support consists of both physical and psychological assistance given by family, friends, colleagues, and other organizations. Social support has been shown to help protect against PTSD and depression.14–16 It is reported that the perception of greater social support correlated with milder PTSD symptoms,17 and individuals with lower levels of social support are more susceptible PTSD.18 Moreover, another study confirmed that social support was significantly associated with recovery from PTSD.19 In contrast, a study explored the bidirectional temporal relationship of perceived social support and PTSD symptoms. They revealed the impact of PTSD symptoms on subsequent perceived social support, while perceived social support was not related to subsequent changes in PTSD symptom, indicating a unidirectional relationship between them.20 Thus, it would be meaningful to evaluate the association between social support and symptoms of PTSD in OC patients.
Mental adjustment to cancer (MAC) is a coping strategy in terms of individual patient’s behavioral, cognitive, and emotional responses to diagnosis and therapy.21 Previous study found that adaptive coping was related to better health and quality of life, while maladaptive coping had opposite effects.22 It was reported that social support was positively associated with fighting spirit, while negatively associated with helplessness/hopelessness and fatalism.23 Among patients with gynecologic cancer, their responses were considerably affected by the perceived level of social support. Li et al24 demonstrated that mental adjustment could substantially intervene the association between perceived stress and depression symptoms. On the other hand, Wang et al25 concluded that mental adjustment played a mediating role between depressive symptoms and perceived social support. Only a limited number of studies have analyzed how mental adjustment mediates the relationship between social support and PTSD symptoms, leading to a significant research gap in the field.
In addition, demographic and clinical variables may also have effects on the occurrence of PTSD. A meta-analysis demonstrated that patients with younger age and advanced disease might at a greater risk of PTSD.26 Other studies highlighted that factors such as education and income were associated with PTSD.10,27 While, Mirabeau-Beale et al compared PTSD in early and advanced stage OC patients, and found no significant differences in marital status, educational status, occupational status or annual income.12 Therefore, it is important and meaningful to explore the relationship between these variables and PTSD, especially when the variables were controlled for in the hierarchical regression.
The objectives of the present study were to examine the association of social support with symptoms of PTSD in Chinese OC patients, and to analyze whether mental adjustment mediated these variables. We hypothesized that PTSD symptoms were significantly associated with social support, and mental adjustment would play a mediating role between them.
Methods
Study Population
From January 2015 to December 2016, a cross-sectional study was carried out using convenience sampling in OC patients at the First Hospital of China Medical University, one of the largest service centers for cancer patients in northeast China. The following inclusion criteria were used to enroll patients in the study: (1) aged 18 years or older; (2) histological evidence of epithelial ovarian cancer or fallopian tube cancer; (3) aware of their diagnosis; (4) able to speak, read and understand Chinese. The exclusion criteria were patients with psychiatric or intellectual problems, and those with other types of cancer. Written informed consent was received from each patient. The Ethics Committee for Human Trials of the hospital approved all study protocols. Clinical data were obtained from original medical records and structured questionnaires. A total of 171 OC subjects were recruited in the present study, and effective responses were received from 139 patients (81.3%).
Evaluation of PTSD
The PTSD Checklist Civilian Version (PCL-C)28 was employed for the measurement of PTSD symptoms, which consists of a 5-point Likert scale (1 = “not at all” to 5 = “extremely”) quantifying how bothersome the symptom has been to the patient over the past 4 weeks. The scale consists of 17 items, with scores from 17 to 85. A higher score suggests a higher level of PTSD symptoms, with the cutoff at 44 based on previous studies.10,29 The Chinese version has been proven to have great reliability.30 The total scale had a Cronbach’s alpha of 0.910.
Measurement of Social Support
We applied the Duke-UNC Functional Social Support Questionnaire for the assessment of social support,31 which consists of a 5-point Likert scale (1 = “much less than I would like” to 5 = “as much as I would like”) quantifying how is the patient’s satisfaction with their perceived level of social support. The total scale includes 8 items, with scores ranging from 8 to 40. A higher score represents a higher level of perceived social support. The Chinese version has been verified and widely applied to studies.32 The total scale had a Cronbach’s alpha of 0.865.
Measurement of Mental Adjustment
The Mini-Mental Adjustment to Cancer (Mini-MAC) scale, established for the evaluation of cognitive and behavioral responses to a cancer diagnosis, was used to assess mental adjustment. The Mini-MAC scale includes 29 items with five types of adjustment: helplessness/hopelessness, fatalism, fighting spirit, anxious preoccupation, and avoidance.33 The Chinese version focuses on three components, namely negative emotion, positive attitude, and cognitive avoidance on a 4-point Likert scale (1 = “definitely does not apply to me” to 4 = “definitely applies to me”). It is widely used and has been showing strong effectiveness and reliability.34 A higher score indicates a more efficient adjustment. Negative emotion, positive attitude, and cognitive avoidance had Cronbach’s alpha values of 0.867, 0.704, and 0.769, respectively.
Statistical Analysis
Statistical analysis was conducted using the SPSS 22.0 software, with a P-value < 0.05 being statistically significant (two-tailed). Variations of PTSD symptoms with respect to independent variables were examined by one-way ANOVA and an independent sample t-test. Associations between PTSD symptoms, level of social support, and mental adjustment were analyzed using Pearson’s correlation. Hierarchical multiple regression analysis was employed to investigate the impact of the three blocks of independent variables of the symptoms of PTSD. All clinical and demographic variables were placed in block 1. Dummy variables were employed since educational, income levels, cancer stage, and treatment type were categorical variables without a linear trend. Social support and mental adjustment were placed in block 2 and 3, respectively.
The SPSS PROCESS macro 3.5 with 5000 bootstrap samplings was adopted to examine the role of mental adjustment in mediating social support and PTSD symptoms.35–37 The specific indirect effect is calculated by a * b product. If zero is not included in the bias-corrected and accelerated 95% CI (BCa 95% CI), the role in mediation is statistically significant. To estimate the indirect effects, we analyzed their proportion in total effects.
Results
Descriptive Statistics
Patient clinical and demographic characteristics were displayed in Table 1. The average age at diagnosis was 57.78 ± 10.14 years old. More than half of the patients had completed secondary school education, and reported a household income above 2000 Chinese yuan. All patients were diagnosed with epithelial ovarian cancer. 66.2% of patients were diagnosed at stage III or IV, and 57.6% obtained combined treatment. Combined treatment included both surgery and chemotherapy. The prevalence of PTSD symptoms among these patients was 17.3% (PCL-C score ≥ 44).
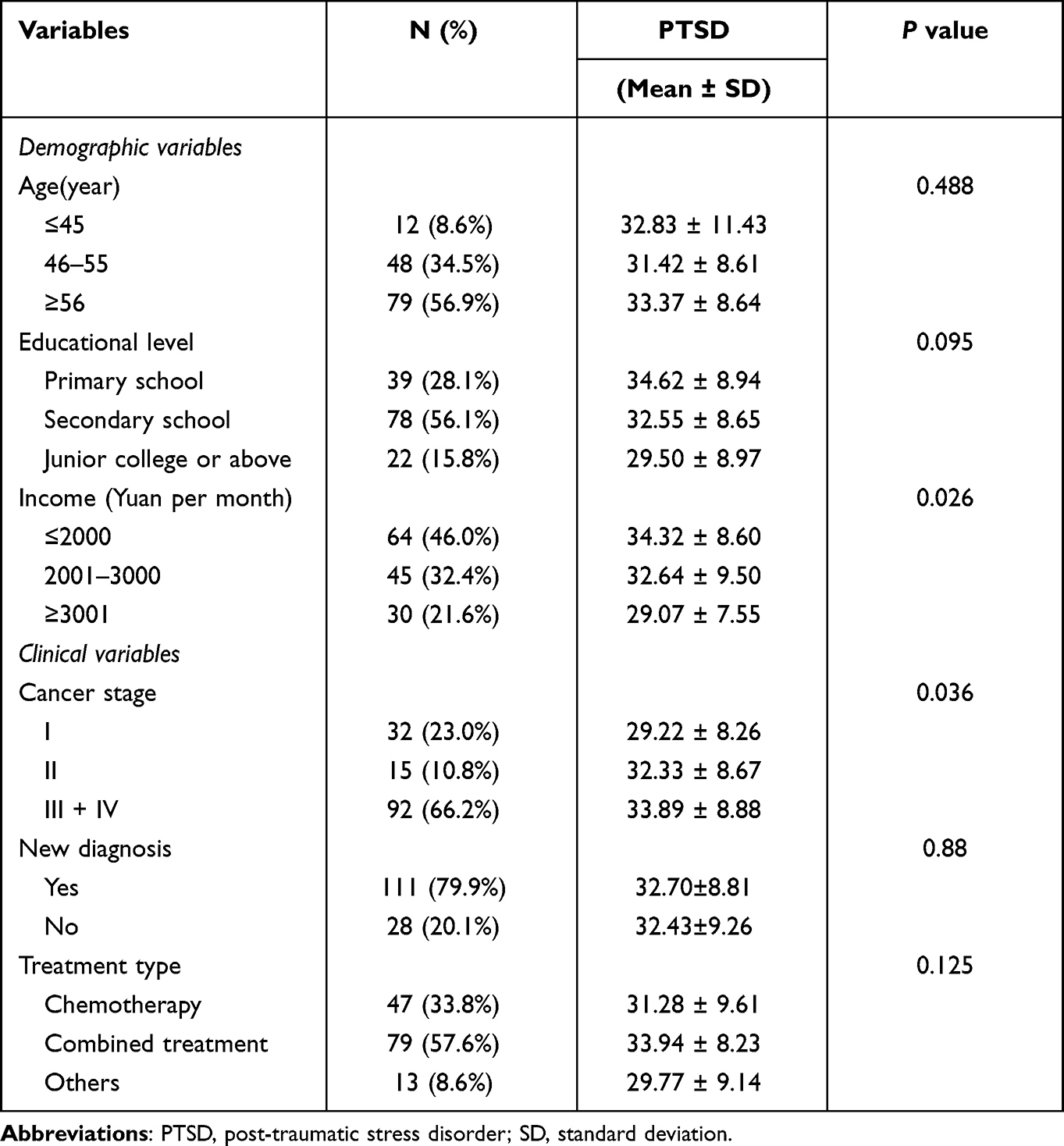 |
Table 1 Mean Scores of PTSD Symptoms According to Demographic and Clinical Variables (n = 139) |
Impact of Demographic and Clinical Variables on Symptoms of PTSD
Patients with an income less than 2000 yuan had more symptoms of PTSD (34.32 ± 8.60) as compared with those stating an income of 2001–3000 (32.64 ± 9.50) or higher than 3001 (29.07 ± 7.55) (Table 1). Patients with stage III or IV had more symptoms of PTSD (33.89 ± 8.88) compared to those with stages I (29.22 ± 8.26) and II (32.33 ± 8.67).
Correlations Between Social Support, Mental Adjustment, and PTSD Symptoms
In Table 2, PTSD symptoms were negatively related with both social support (r = −0.348, P < 0.01) and positive attitude (r = −0.363, P < 0.01), and positively associated with negative emotion (r = 0.494, P < 0.01) and cognitive avoidance (r = 0.410, P < 0.01). Social support was negatively associated with negative emotion (r = −0.377, P < 0.01) and cognitive avoidance (r = −0.169, P < 0.05), and positively related with positive attitude (r = 0.201, P < 0.01).
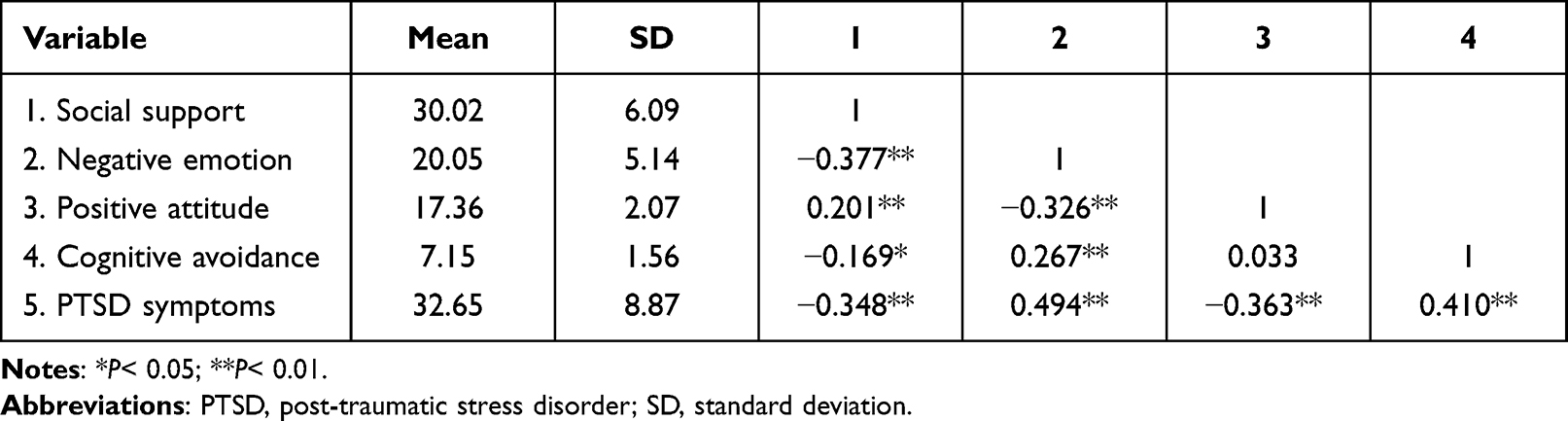 |
Table 2 Correlations Between Social Support, Mental Adjustment, and PTSD Symptoms |
Relationship of Social Support and PTSD Symptoms Based on Hierarchical Linear Regression
As shown in Table 3, following adjustments for age, income, cancer stage and social support, the result in block 3 had statistically significance (R2= 0.439, Adjusted R2= 0.400, F= 11.208, P< 0.001). Social support and the three factors of mental adjustment could explain 10.3% and 25.6% of the variance in PTSD symptoms, respectively. Moreover, after adding mental adjustment, the regression coefficient of social support decreased and was no longer statistically significant (β decreased from −0.324 to −0.130, P > 0.05), suggesting that mental adjustment might play a complete mediating role between social support and PTSD symptoms.
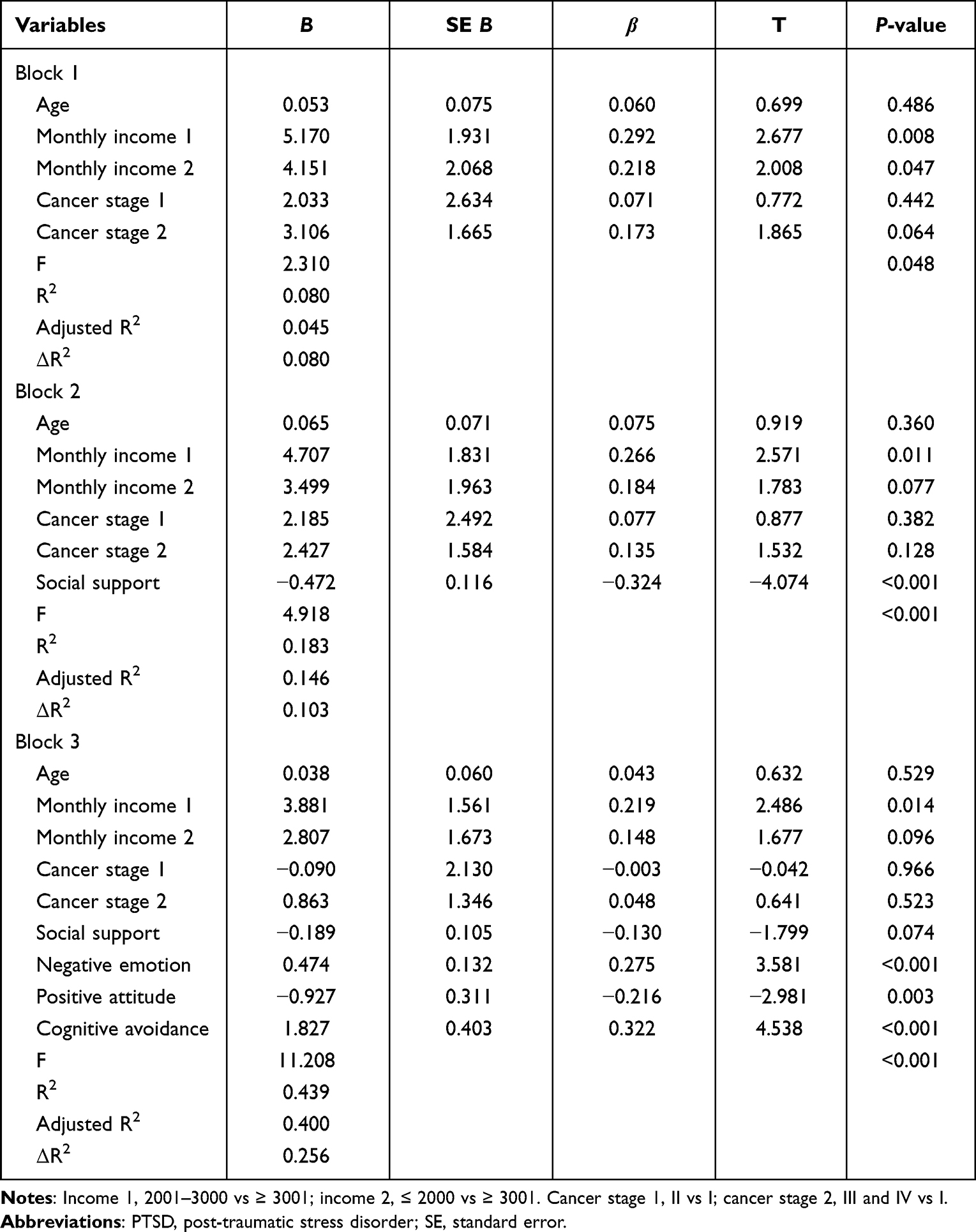 |
Table 3 Exploration of Variables Associated with PTSD Symptoms Using Hierarchical Linear Regression |
The Role of Mental Adjustment in Mediating the Association Between Social Support and PTSD
Results for the path coefficient of indirect effects (a * b product) were presented in Table 4 and Figure 1. In the model, social support was correlated with negative emotion, cognitive avoidance, and positive attitude. These three factors were significantly correlated with PTSD symptoms following adjustment for income, cancer stage, age, and social support. These results were in accordance with those of hierarchical multiple regression analysis. The indirect roles of negative emotion and positive attitude in mediating the association between social support and PTSD symptoms were −0.102 (BCa 95% CI: −0.174, −0.042) and −0.038 (BCa 95% CI: −0.086, −0.002). The mediating role of cognitive avoidance was insignificant (BCa 95% CI: −0.118, 0.004). The proportions of mediating roles of negative emotion and positive attitude were 31.5% and 11.7%, respectively (a * b /c).
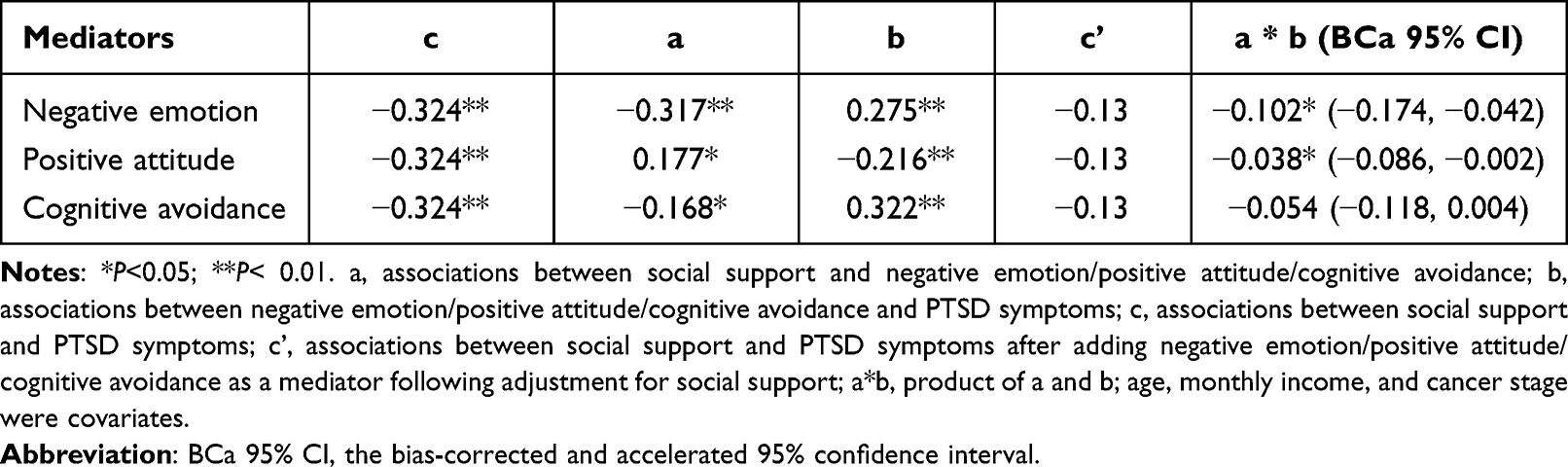 |
Table 4 The Role of Mental Adjustment in Mediating the Association Between Social Support and PTSD Symptoms |
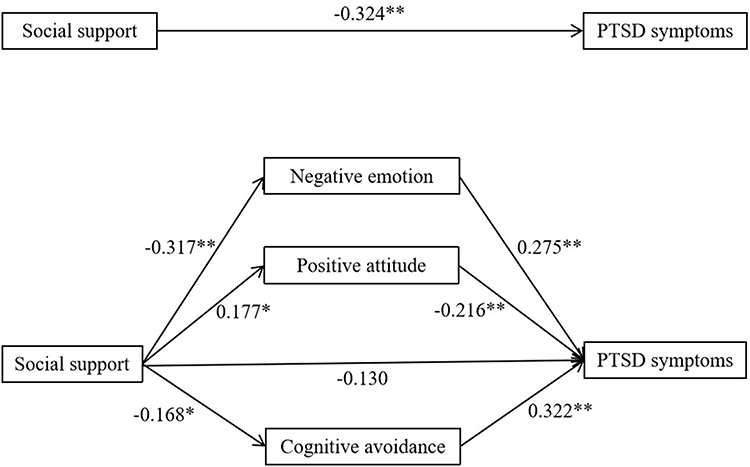 |
Figure 1 Indirect pathways of social support with PTSD symptoms through mental adjustment’s components (negative emotion, positive attitude and cognitive avoidance). Abbreviation: PTSD, post-traumatic stress disorder. Notes: *P< 0.05; **P< 0.01. Age, monthly income, and cancer stage were covariates. |
Discussion
The present study explored the relationship between social support and PTSD symptoms, and further examined the role of mental adjustment in mediation. In the present study, the prevalence of PTSD symptoms was 17.3%, which is higher than that among Australian women (9.25%)13 and lower than that in participants of a British study (36–45%).8 It was reported that no advanced stage OC patients were diagnosed with PTSD, while 6.9% of patients with early stage OC had PSTD symptoms.12 This variability might be attributed to the differences in the composition of study samples, or different dimensional tools being employed. Nevertheless, previous results indicated that patients with OC may be affected by PTSD symptoms to differing degrees. Therefore, it is important to monitor PTSD symptoms in OC patients to improve their mental health status.
In our study, we found OC patients with less income and advanced stage had more symptoms of PTSD, consistent with prior studies.10,26 After controlling for other factors, income was still a significant factor. To some extent, the month income reflects the socioeconomic status. The less the income, the less resources that can be used to cope with cancer, the more susceptible to suffer psychological trauma caused by major events. Some studies reported that PTSD was more common in early stage disease than advanced stage.9,11,12 It may be attributed to differences such as regions and populations. In the clinical practice, we should pay attention to these variables to cope with PTSD.
The results of this study demonstrated that social support had a negative correlation with symptoms of PTSD in OC patients, which is consistent with prior reports.38,39 It is reported that a lack of positive support is a predictor of psychological co-morbidity.40 Thus, additional attention should be paid to the importance of social support, calling for active interventions to reduce PTSD symptoms in cancer patients. On the contrary, Shnaider et al41 demonstrated that total support, as well as social support from family and friends, was not correlated with the initial severity of PTSD symptoms, while a significant correlation was found between social support from significant others and initial severity of PSTD. However, another study found that social support had a significant correlation with PTSD only when involving family support.42 Thus, different support types should be considered when developing effective strategies for PTSD.
The present study indicated that negative emotion was positively associated with PTSD symptoms, while positive attitude had a negative association. Coping strategies are significant resources for mental adjustment in cancer patients to prevent PTSD symptoms. Patients with highly positive attitude always expect the best outcome and view life events in a positive light. In accordance, another study reported that coping strategies related to positive emotion were negatively correlated with symptoms of PTSD.43 Screening for mental coping strategies at the beginning of treatment might help to predict PTSD symptoms in cancer patients.
As a major part of the present study, we found mental adjustment could fully mediate the correlation between social support and PTSD symptoms. In other words, social support worked through mental adjustment in this setting. This finding indicates that interventions focusing on mental adjustment may be more useful than targeting social support for psychological help assessment or assistance to OC patients. It is noteworthy that the proportion of mediation by negative emotion (31.5%) was higher than that by positive attitude (11.7%). Cancer patients with a high level of negative emotion may appear unconfident and pessimistic on issues, rendering these patients more susceptible to PTSD symptoms. In targeted intervention to improve their psychological adjustment, extra emphasis should be put on regulating the negative emotion factor of OC patients.
There are certain limitations in this study. Firstly, because of the cross-sectional design, a causal relationship cannot be determined. It is well known that the levels of both PTSD and social support may change over time. Hence, more longitudinal studies are demanded to increase the power of our findings. Secondly, our study was based on self-reporting measures. Therefore, the possibility of recall and report bias exists. Thirdly, this study focused on the PTSD symptoms using a self-report scale, while PTSD in clinical diagnosis needs to be further studied. Lastly, other moderating or mediating factors should be further evaluated, if a full mediation also exists in these factors.
Conclusions
PTSD symptoms in OC patients should be paid attention to. Social support and mental adjustment were positive resources associated with PTSD symptoms. Moreover, mental adjustment could mediate the relation between social support and PTSD symptoms in OC patients. Therefore, intervention management that focuses on improving perceived social support and strengthening mental adjustment, especially negative emotion and positive attitude, might be useful to reduce PTSD symptoms in this context.
Ethics Approval and Consent to Participate
This study was performed according to the Declaration of Helsinki for Medical Research involving Human Subjects, and was approved by the Ethical Committee for Human Trials of the China Medical University, China. All participants provided written informed consent before participating in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Special project for central guidance of local science and technology development of Liaoning province (Project No: 2019JH6/10400006).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7–33.
2. Karatas RD, Altinoz AE, Essizoglu A. Post-traumatic stress disorder and related factors among female victims of sexual assault required to attend a University Hospital in Turkey: a cross-sectional cohort study. Crim Behav Ment Health. 2020;30(2–3):79–94.
3. Li J, Reinhardt JD, Feng X. Physical function, post-traumatic stress disorder, and quality of life in persons with spinal cord injury caused by the Wenchuan earthquake versus nondisaster trauma: a cross-sectional modeling study. Spinal Cord. 2020;58(5):616–625.
4. Duagani MY, Leys C, Matonda-Ma-Nzuzi T, Blanchette I, Mampunza MMS, Kornreich C. Peritraumatic dissociation and post-traumatic stress disorder in individuals exposed to armed conflict in the Democratic Republic of Congo. J Trauma Dissociation. 2019;20(5):582–593.
5. van der Vlegel M, Polinder S, Mikolic A, et al. The Center-Tbi Participants And Investigators. The Association of Post-Concussion and Post-Traumatic Stress Disorder Symptoms with Health-Related Quality of Life, Health Care Use and Return-to-Work after Mild Traumatic Brain Injury. J Clin Med. 2021;10(11):2473.
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington, DC: American Psychiatric Association Press; 2000.
7. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5. Washington, DC: American Psychiatric Association Press; 2003.
8. Goncalves V, Jayson G, Tarrier N. A longitudinal investigation of posttraumatic stress disorder in patients with ovarian cancer. J Psychosom Res. 2011;70(5):422–431.
9. Kornblith AB, Mirabeau-Beale K, Lee H, et al. Long-term adjustment of survivors of ovarian cancer treated for advanced-stage disease. J Psychosoc Oncol. 2010;28(5):451–469.
10. Liu C, Zhang Y, Jiang H, Wu H. Association between social support and post-traumatic stress disorder symptoms among Chinese patients with ovarian cancer: a multiple mediation model. PLoS One. 2017;12(5):e177055.
11. Matulonis UA, Kornblith A, Lee H, et al. Long-term adjustment of early-stage ovarian cancer survivors. Int J Gynecol Cancer. 2008;18(6):1183–1193.
12. Mirabeau-Beale KL, Kornblith AB, Penson RT, et al. Comparison of the quality of life of early and advanced stage ovarian cancer survivors. Gynecol Oncol. 2009;114(2):353–359.
13. Shand LK, Brooker JE, Burney S, Fletcher J, Ricciardelli LA. Symptoms of posttraumatic stress in Australian women with ovarian cancer. Psychooncology. 2015;24(2):190–196.
14. Aydin B, Akbas S, Turla A, Dundar C. Depression and post-traumatic stress disorder in child victims of sexual abuse: perceived social support as a protection factor. Nord J Psychiatry. 2016;70(6):418–423.
15. Dinenberg RE, McCaslin SE, Bates MN, Cohen BE. Social support may protect against development of posttraumatic stress disorder: findings from the Heart and Soul Study. Am J Health Promot. 2014;28(5):294–297.
16. McGuire AP, Gauthier JM, Anderson LM, et al. Social Support Moderates Effects of Natural Disaster Exposure on Depression and Posttraumatic Stress Disorder Symptoms: effects for Displaced and Nondisplaced Residents. J Trauma Stress. 2018;31(2):223–233.
17. Southivong B, Ichikawa M, Nakahara S, Southivong C. A cross-sectional community study of post-traumatic stress disorder and social support in Lao People’s Democratic Republic. Bull World Health Organ. 2013;91(10):765–772.
18. Johansen VA, Milde AM, Nilsen RM, et al. The Relationship Between Perceived Social Support and PTSD Symptoms After Exposure to Physical Assault: an 8 Years Longitudinal Study. J Interpers Violence. 2020;1:886260520970314.
19. Dai W, Chen L, Tan H, et al. Association between social support and recovery from post-traumatic stress disorder after flood: a 13-14 year follow-up study in Hunan, China. BMC Public Health. 2016;16:194.
20. Nickerson A, Creamer M, Forbes D, et al. The longitudinal relationship between post-traumatic stress disorder and perceived social support in survivors of traumatic injury. Psychol Med. 2017;47(1):115–126.
21. Nordin K, Glimelius B. Reactions to gastrointestinal cancer–variation in mental adjustment and emotional well-being over time in patients with different prognoses. Psychooncology. 1998;7(5):413–423.
22. Kugbey N, Meyer-Weitz A, Oppong AK. Mental adjustment to cancer and quality of life among women living with breast cancer in Ghana. Int J Psychiatry Med. 2019;54(3):217–230.
23. Yagmur Y, Duman M. The relationship between the social support level perceived by patients with gynecologic cancer and mental adjustment to cancer. Int J Gynaecol Obstet. 2016;134(2):208–211.
24. Li Y, Yang Y, Zhang R, Yao K, Liu Z. The Mediating Role of Mental Adjustment in the Relationship between Perceived Stress and Depressive Symptoms in Hematological Cancer Patients: a Cross-Sectional Study. PLoS One. 2015;10(11):e142913.
25. Wang Z, Sun X, Qin B. Correlations of depressive symptom with perceived social support and mental adjustment among lung cancer patients (in Chinese). China J Public Health. 2017;33(3):499–502.
26. Abbey G, Thompson SB, Hickish T, Heathcote D. A meta-analysis of prevalence rates and moderating factors for cancer-related post-traumatic stress disorder. Psychooncology. 2015;24(4):371–381.
27. Cordova MJ, Andrykowski MA, Kenady DE, McGrath PC, Sloan DA, Redd WH. Frequency and correlates of posttraumatic-stress-disorder-like symptoms after treatment for breast cancer. J Consult Clin Psychol. 1995;63(6):981–986.
28. Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. In: Paper Presented at the Annual Meeting of the International Society for Traumatic Stress Studies. San Antonio, Texas; 1993.
29. Welch AE, Jasek JP, Caramanica K, Chiles MC, Johns M. Cigarette smoking and 9/11-related posttraumatic stress disorder among World Trade Center Health Registry enrollees, 2003-12. Prev Med. 2015;73:94–99.
30. Liang L, Gao T, Ren H, et al. Post-traumatic stress disorder and psychological distress in Chinese youths following the COVID-19 emergency. J Health Psychol. 2020;25(9):1164–1175.
31. Broadhead WE, Gehlbach SH, de Gruy FV, Kaplan BH. The Duke-UNC Functional Social Support Questionnaire. Measurement of social support in family medicine patients. Med Care. 1988;26(7):709–723.
32. Liu L, Pang R, Sun W, et al. Functional social support, psychological capital, and depressive and anxiety symptoms among people living with HIV/AIDS employed full-time. BMC Psychiatry. 2013;13:324.
33. Jimenez-Fonseca P, Lorenzo-Seva U, Ferrando PJ, et al. The mediating role of spirituality (meaning, peace, faith) between psychological distress and mental adjustment in cancer patients. Support Care Cancer. 2018;26(5):1411–1418.
34. Ho SM, Fung WK, Chan CL, Watson M, Tsui YK. Psychometric properties of the Chinese version of the Mini-Mental Adjustment to Cancer (MINI-MAC) scale. Psychooncology. 2003;12(6):547–556.
35. Hao W, Li J, Fu P, et al. Physical frailty and health-related quality of life among Chinese rural older adults: a moderated mediation analysis of physical disability and physical activity. BMJ Open. 2021;11(1):e42496.
36. Liu W, Li J, Huang Y, Yu B, Qin R, Cao X. The relationship between left-behind experience and obsessive-compulsive symptoms in college students in China: the mediation effect of self-esteem. Psychol Health Med. 2021;26(5):644–655.
37. Hayes AF. Introduction to Mediation, Moderation and Conditional Process Analysis: A Regression-Based Approach.
38. Kornblith AB, Herndon JN, Weiss RB, et al. Long-term adjustment of survivors of early-stage breast carcinoma, 20 years after adjuvant chemotherapy. Cancer Am Cancer Soc. 2003;98(4):679–689.
39. Zalta AK, Tirone V, Orlowska D, et al. Examining moderators of the relationship between social support and self-reported PTSD symptoms: a meta-analysis. Psychol Bull. 2021;147(1):33–54.
40. Mehnert A, Lehmann C, Graefen M, Huland H, Koch U. Depression, anxiety, post-traumatic stress disorder and health-related quality of life and its association with social support in ambulatory prostate cancer patients. Eur J Cancer Care (Engl). 2010;19(6):736–745.
41. Shnaider P, Sijercic I, Wanklyn SG, Suvak MK, Monson CM. The Role of Social Support in Cognitive-Behavioral Conjoint Therapy for Posttraumatic Stress Disorder. Behav Ther. 2017;48(3):285–294.
42. Yang YL, Liu L, Li MY, Shi M, Wang L. Psychological Disorders and Psychosocial Resources of Patients with Newly Diagnosed Bladder and Kidney Cancer: a Cross-Sectional Study. PLoS One. 2016;11(5):e155607.
43. Britt TW, Adler AB, Sawhney G, Bliese PD. Coping Strategies as Moderators of the Association Between Combat Exposure and Posttraumatic Stress Disorder Symptoms. J Trauma Stress. 2017;30(5):491–501.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.