")
Back to Journals » Clinical Ophthalmology » Volume 15
The Role of Infection Control Measures in Ophthalmology: Do They Prevent COVID-19 Infection Among Ophthalmologists in Egypt? A Survey-Based Study
Authors Esmat SM , Aboulfotouh MR, Ezzelarab MH, Abdalgeleel SA, Tolba DA
Received 14 August 2021
Accepted for publication 15 October 2021
Published 29 October 2021 Volume 2021:15 Pages 4347—4355
DOI https://doi.org/10.2147/OPTH.S334252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sara M Esmat,1 Mohammad R Aboulfotouh,1 Moushira H Ezzelarab,2 Shaimaa A Abdalgeleel,3 Doaa A Tolba1
1Department of Ophthalmology, Faculty of Medicine, Cairo University, Cairo, Egypt; 2Department of Clinical and Chemical Pathology, Faculty of Medicine, Cairo University, Cairo, Egypt; 3Department of Biostatistics and Epidemiology, National Cancer Institute, Cairo University, Cairo, Egypt
Correspondence: Sara M Esmat
Department of Ophthalmology, Faculty of Medicine, Cairo University, Cairo, 11562, Egypt
Tel +201069186501
Email [email protected]
Introduction: Ophthalmologists are at a high risk of coronavirus disease 2019 (COVID-19) infection owing to their working environments and proximity to patients during examinations. Compliance with infection control measures in examination offices can lessen the risk of infection to this group. In Egypt, several deaths from COVID-19 have been reported among ophthalmologists; therefore, we studied the prevalence of COVID-19 infections in this group and assessed ophthalmologists’ commitments to recommended infection control measures.
Aim: To evaluate the rate of COVID-19 infections among ophthalmologists, identify risk factors for infections, and evaluate ophthalmologists’ commitments to infection control measures in their medical facilities.
Methods: An online questionnaire was designed and distributed to ophthalmologists in the Cairo Governorate from May 1, 2021 to mid-June 2021.
Results: Out of 161 responders, the percentage of COVID-19 infections was 52.8% (85 responders). This was significantly higher among younger ophthalmologists (P-value = 0.019) and those with fewer years of experience (P-value = 0.010). Adopting full precautions while examining patients with or without respiratory illness were significantly associated with a lower infection rate (P-value = 0.019 and 0.046, respectively). A significantly higher infection rate was reported for ophthalmologists who examined known COVID-19 patients at outpatient clinics, even when taking precautions (P-value = 0.032). A lower rate of COVID-19 infection was significantly associated with adopting full precautions while operating on suspected or nonsuspected COVID-19 patients (P-value = 0.007 and 0.003, respectively).
Conclusion: Both young age and limited experience were significant infection risk factors in our study. The most important infection control measures that significantly decreased infection risks were adherence to full protective measures while working in outpatient clinics and operating rooms.
Keywords: COVID-19, infection control, ophthalmologists
Introduction
The 2019 novel coronavirus (2019-nCoV) or severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has rapidly spread from its origins in Wuhan City, China, to the rest of the world.1 Infection is transmitted through airborne droplets from symptomatic or asymptomatic individuals.2 In addition, the eyes may serve as a source of infection and an entryway for transmission.3 The clinical features of coronavirus disease 2019 (COVID-19) are variable, ranging from an asymptomatic state to acute respiratory distress syndrome and multiorgan dysfunction.4
Since the pandemic was declared in March 2020, medical staff have expressed grave concerns regarding infection with the fast-spreading virus, and in particular, ophthalmologists due to the nature of their work and patient proximity during examinations.5 Importantly, these perceptions have been reflected in the literature.6,7 In addition, ocular manifestations of the virus, including follicular conjunctivitis, epiphora or chemosis, may indicate the first presentation of COVID-19.8,9 Similarly, ophthalmic consultations often require several examination techniques involving visual acuity, intraocular pressure measurements, and fundus examinations. Hence, patients usually require prolonged stays in the clinic to complete examinations.10
Several ophthalmic societies have formulated different ophthalmic care plans to ensure ophthalmologist personal safety.11 The most common measures advocated lowering patient attendance, suspending elective clinical services, donning personal protective equipment (PPE), using environmental controls, such as protective shields (plastic) on slit lamps, and suspending proximity techniques, such as direct ophthalmoscopy.12 In a Chinese study, only two new symptomatic COVID-19 cases were reported in two hospitals after PPE was used when compared with nine cases before its introduction.13
In a previous international study, ophthalmologists were identified as one of the most vulnerable medical subspecialties in terms of disease morbidity and mortality.14 Therefore, this prompted us to investigate the prevalence of COVID-19 infections in ophthalmologists in Egypt, to identify risk factors increasing susceptibility to infection, and assess ophthalmologists’ commitments to recommended infection control measures in outpatient clinics and operating wards.
Materials and Methods
Ethical Considerations and Study Information
This was a cross-sectional observational study. We used online questionnaires to collect data from ophthalmologists working in the Cairo Governorate. The study protocol was approved by the Ophthalmology Department Ethics Committee at Cairo University (1/5/2021-1). The questionnaire was made available in electronic form (Google™ forms) and sent to 200 ophthalmologists via e-mail and social media. We received responses from 161 responders who self-administered the questionnaires. Responses were received anonymously over 6 weeks, from May 1, 2021 to mid-June 2021.
The Questionnaire
The questionnaire covered various aspects of the infection control process and included six sections, which collected information/data on the following: 1) responder demographics, 2) COVID-19 perceptions and training levels related to infection control measures, 3) infection control measures followed by medical facilities, 4) and 5) measures followed personally by ophthalmologists in clinics and operating rooms, and 6) COVID-19 infections and vaccinations among ophthalmologists.
Pilot Study and Questionnaire Authentication
A pilot study was conducted in 10 responders to assess questionnaire clarity, applicability, and responsiveness. Also, a panel of three experts from the Faculty of Medicine, Cairo University, examined the questionnaire to validate its contents. Using Cronbach’s alpha test, questionnaire reliability was 0.761.
Statistical Methods
The Statistical Package of Social Science (SPSS) (version 6, IBM Corp, Armonk, NY, USA) was used to analyze data and generate results. Data normality was tested using the Kolmogorov Smirnov test. As the data were not normally distributed. Numerical data were summarized as medians and ranges. Numerical comparisons between two groups were performed using the Mann–Whitney U-test. Qualitative data were described as frequencies and percentages. Relationships between qualitative data were assessed using the Chi-square test or Fisher’s exact test as required. Stepwise logistic regression analyses were applied to significant variables in univariate analysis using the forward likelihood ratio method. The odds ratio and associated 95% confidence intervals (CI) were calculated to estimate the infection risk. Probability (P-value) ≤0.05 was considered significant.
Results
Responder Socio-Demographic Data and the Relationship with COVID-19 Infection
We received responses from 161 ophthalmologists. Ages ranged from 26 to 65 years, with a median age of 34 years. We observed that 92 responders were females (57.2%) and 97 (60.2%) worked in university hospitals. Cornea and refractive surgery (N = 55) was the most common subspecialty (34.2%), followed by retina subspeciality in 23 responders (14.4%). We noted that 108 responders (67.1%) had ≥10 years experience in ophthalmology.
Our questionnaire also assessed the rate of COVID-19 infection in responders and its relationship to different variables; 85 (52.8%) responders were infected with COVID-19 at the time of the survey. The relationship between COVID-19 infection and responder socio-demographic characteristics is summarized (Table 1). The mean age was significantly lower in infected (median = 34) than noninfected (median = 36) responders (P-value = 0.019). In addition, prior ophthalmology experience (measured in years) was less in those with the infection (P-value = 0.010). However, no statistically significant associations were observed between COVID-19 infection rates and gender (P-value = 0.649), marital status (P-value = 0.634), job title (P-value = 0.170), place of work (P-value=0.351), or subspecialty (P-value = 0.701).
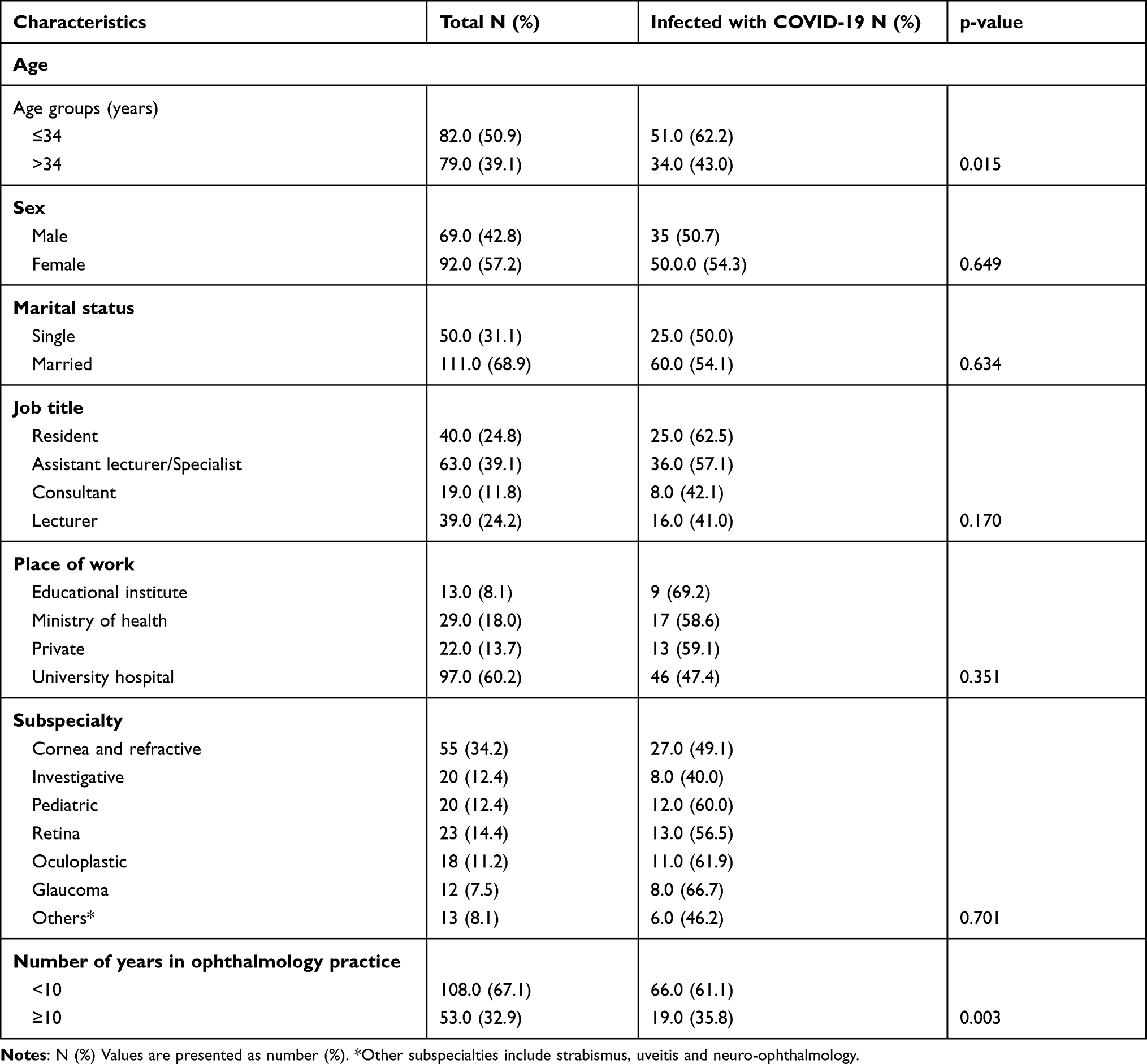 |
Table 1 Relation Between Socio-Demographic Characteristics and COVID-19 Infection |
Ophthalmologist Beliefs About COVID-19 and Vaccinations
Responder concerns about COVID-19 infections and opinions regarding the examination of a suspected COVID-19 patient are shown (Table 2). We observed that 96 (59.6%) responders identified COVID-19 infection as very dangerous and 104 (64.6%) responders preferred to avoid suspected COVID-19 patients. However, no significant associations were found between these beliefs and COVID-19 infection opinions in responders (P-value = 0.338 and 0.975, respectively).
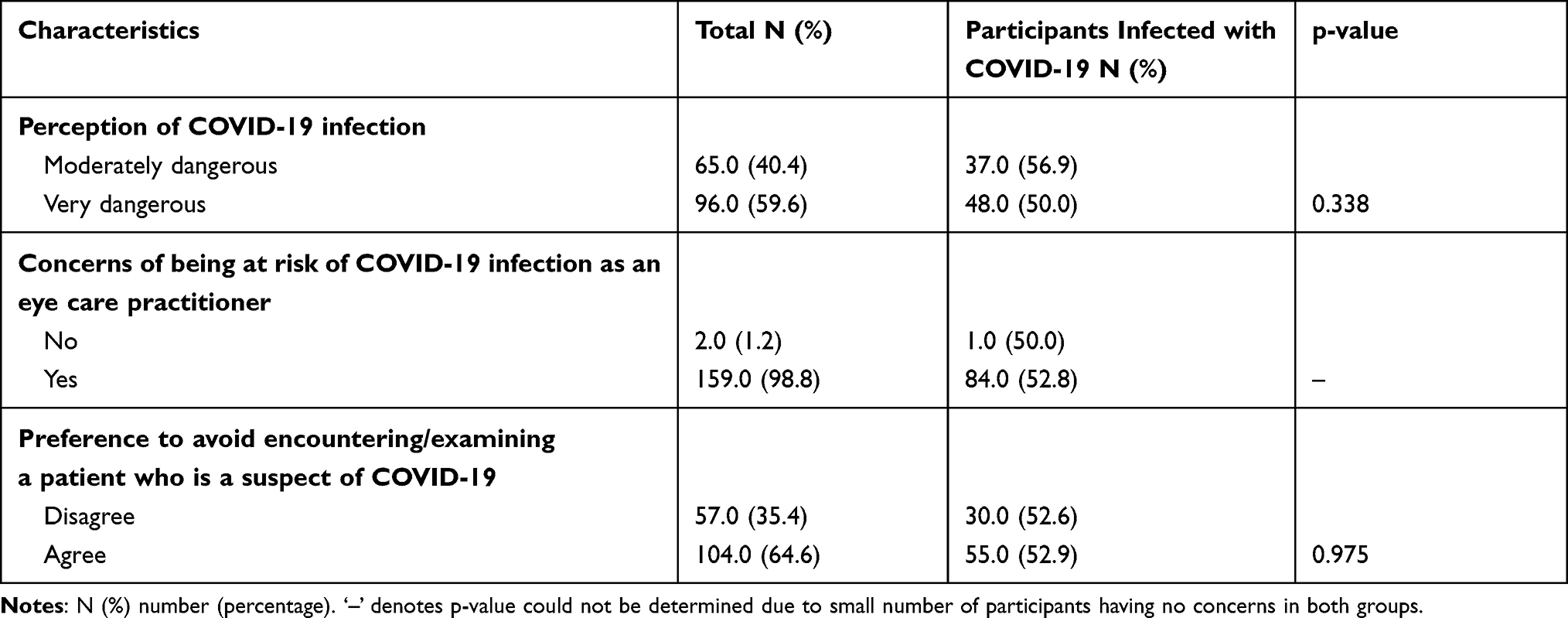 |
Table 2 Beliefs of Ophthalmologists About COVID-19 and COVID-19 Infection and Vaccination |
In terms of vaccination, 80 responders had received a COVID-19 vaccination. The vaccination rate was not affected by the perception of the danger by responders towards COVID-19, as 31 responders reported perceiving COVID-19 as moderately dangerous (38.8%) while 49 responders reported perceiving it as very dangerous (61.3%) (P-value = 0.677).
Ophthalmologist Training in Infection Control Measures and COVID-19 Infections
In terms of training on infection control measures, 60 responders (37.3%) received training on PPE to prevent COVID-19 transmission. Face-to-face training was provided by an infection control specialist for 24 responders (14.9%), online lectures for 17 responders (10.6%), and self-learning for 19 responders (11.8%). However, surprisingly, we observed no statistically significant differences in the prevalence of COVID-19 infections between 35 ophthalmologists who had received training (58.3%) and 50 who had not (49.5%) (P-value = 0.278).
The Application of Preventive Measures by Medical Facilities and COVID-19 Infection Rates
Different strategies were adopted by medical facilities to prevent COVID-19 transmission among health care providers. These included limiting the numbers of patients in elective clinics, as reported by 103 (64%) responders, and a requirement by patients to put on masks, as reported by 154 responders (95.7%). Fever assessments for either health care providers or patients were only reported by approximately 25% of responders. Environmental factors, such as good ventilation, in examination rooms were implemented by 83 responders (51.6%). The availability of disinfectants at all times was reported by 134 responders (83.2%); however, PPE was not always available as indicated by 97 (60.2%) responders. The relationship between the application of preventive measures and the incidence of COVID-19 infection is summarized (Table 3). Surprisingly, no association was observed between the percent of application of preventive measures and the COVID-19 infection rate.
 |
Table 3 Relation Between Application of Infection Control Measures by Medical Facilities and COVID-19 Infection |
The Application of Preventive Measures by Ophthalmologists in Clinics
Ophthalmologist adherence to preventive measures in the clinic as disinfecting hands between patients was reported by 131 responders (81.4%). However, disinfection of the slit lamp was not routinely performed between patients (only reported by 75 responders (46.6%)). We observed that full precautions while examining patients without respiratory illness, by wearing a surgical mask, washing hands before and after examinations, asking the patient to refrain from speaking, and ensuring the patient wore a mask, were significantly associated with a lower rate of COVID-19 infection (P-value = 0.046). Similarly, full precautions while examining patients with respiratory illness, by wearing an N95 mask, gowns, gloves, and eye protection, in addition to the aforementioned precautions, were significantly associated with a lower infection rate (P-value = 0.019) (Table 4). We noted that 73 (45.3%) responders reported they would treat a known COVID-19 patient at an outpatient clinic after taking precautions and 45 the rate of those ophthalmologists were infected with rate (61.6%) (P-value = 0.032).
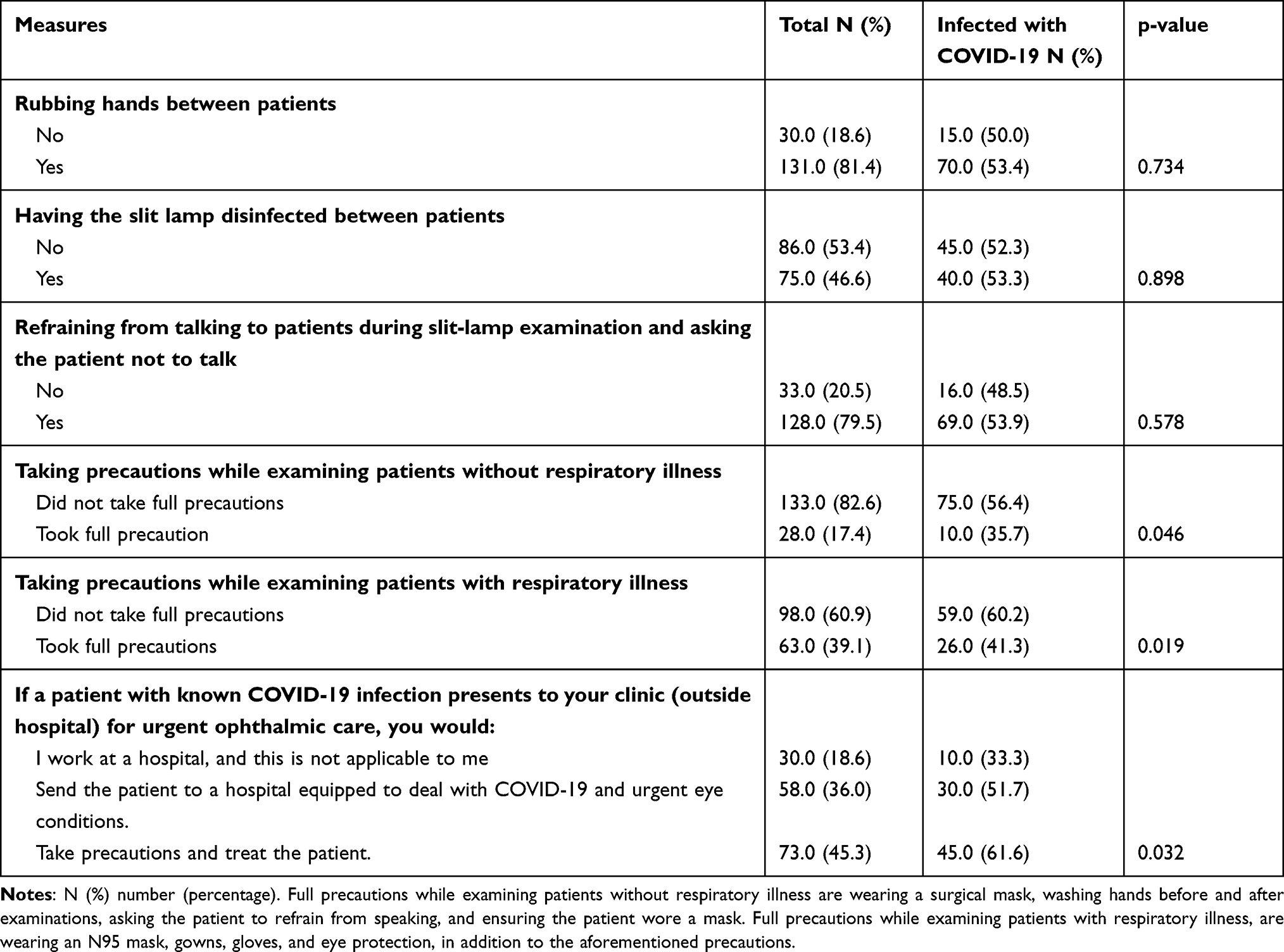 |
Table 4 Relation Between Application of Infection Control Measures by Ophthalmologist in Clinics and COVID-19 Infection |
The Application of Preventive Measures by Ophthalmologists in Operating Rooms
The number of urgent surgical interventions per month ranged from 0 to 35 surgeries, with a median of two per month. Before an urgent surgery, 71 responders (44.1%) reported asking the patients for C reactive protein and complete blood picture. However, the number of performed elective surgical interventions per month ranged from 0 to 250, with a median of four surgeries per month. Importantly, 77 responders (47.8%) reported asking patients for polymerase chain reaction information before these surgeries. Sixty-one responders (37.9%) reported operating on suspect or confirmed COVID-19 patients. A lower rate of infection was significantly associated with taking full safety precautions while operating on either suspected or nonsuspected COVID-19 patients (P-value = 0.007 and 0.003, respectively). These precautions included full PPE while operating on a nonsuspected COVID-19 case, while for suspected COVID-19 cases, precautions included postoperatively referring the patient to an isolation ward and closing the operating room for disinfection (Table 5).
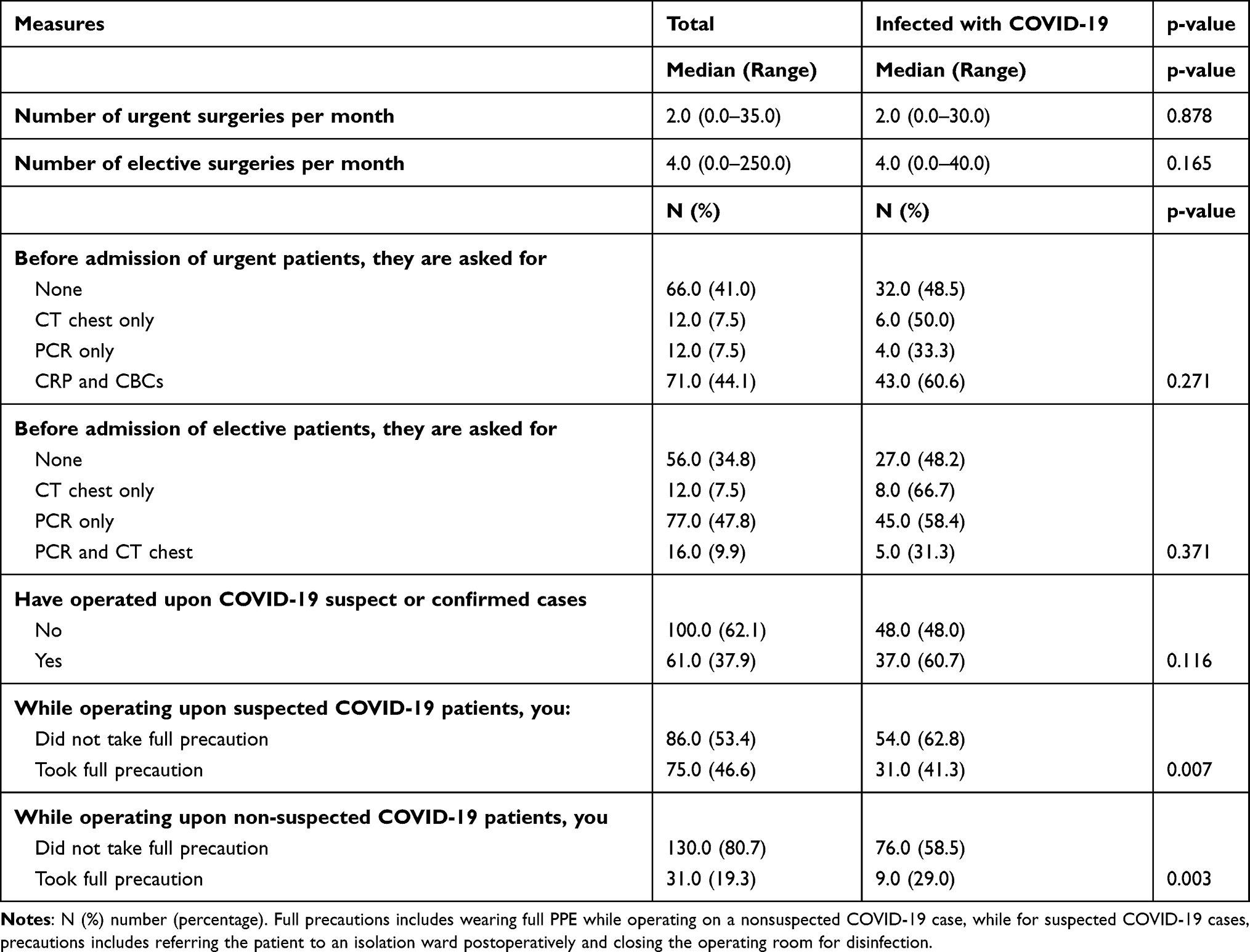 |
Table 5 Relation Between Application of Infection Control Measures by Ophthalmologist in Operating Room and COVID-19 Infection |
COVID-19 Infection Risk Factors Among Ophthalmologists
The factors independently affecting COVID-19 infections were the number of years in ophthalmology practice and adopting full precautions while operating on suspected or nonsuspected COVID-19 patients (Table 6). Ophthalmologists practicing ophthalmology for <10 years were 2.4-times more liable to contract COVID-19 infection (95% CI: 1.1–4.6). Responders not taking full precautions while operating on suspected COVID-19 patients were twice more likely to contract a COVID-19 infection when compared to those who adopted full precautions (95% CI: 1.0–3.9). Responders not taking full precautions while operating on nonsuspected COVID-19 patients were 2.6 times more likely to get a COVID-19 infection (95% CI: 1.1–5.6).
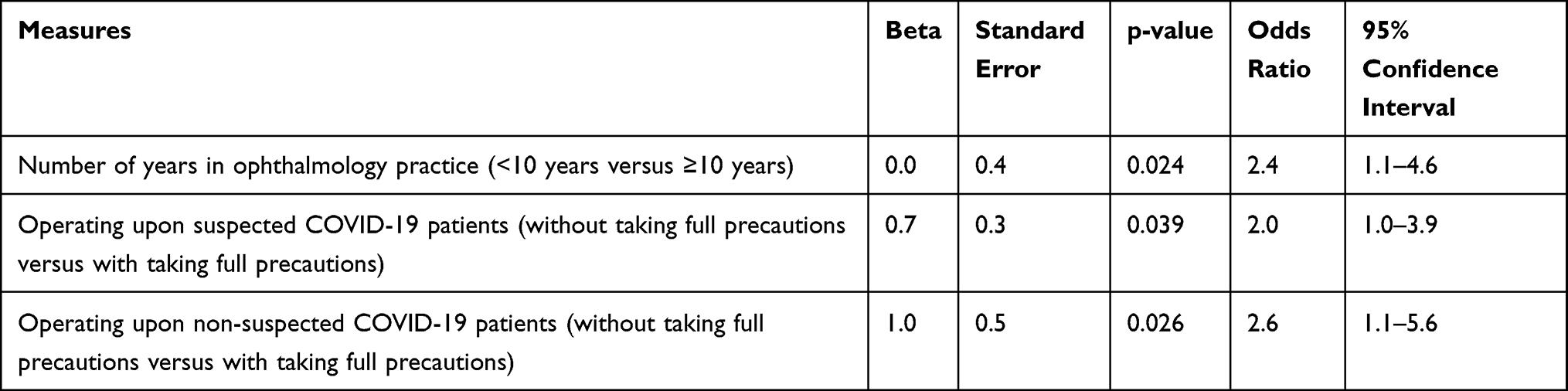 |
Table 6 Multivariate Analysis of Risk Factors Affecting Contracting COVID Infection |
Discussion
As the second year of the pandemic elapses, the world must learn to cohabit with COVID-19. While healthcare providers remain at the front-line, major concerns still persist across most countries about protecting these health care workers. In our survey of ophthalmologists in Egypt, we investigated relationships between infection rates, responder compliance with protective measures, awareness of such protective measures, and perceptions of the seriousness of the pandemic. Ophthalmologists in particular are at a higher risk of infection due to their working environments and proximity to patients during examinations.
From our survey, we observed a high infection rate (52.8%) in responders when compared with data from Wuhan, China, or Granada, Spain, respectively.13,15 This could be partly explained by the fact that these reports were published early in the first year of the pandemic, before global infection rates increased. Our observations also indicated that ophthalmologists have an ongoing risk of acquiring infections from asymptomatic carriers.
Our data indicated that younger ophthalmologists had a significantly higher risk of contracting infections, ie, we recorded a 62.2% infection rate among responders ≤34 years old. This may have been due to increased contact and interactions with more patients in public hospitals and associated long working hours. Also, this group represented a large proportion of study responders. In addition, responders who were infected had significantly fewer years of ophthalmology experience. These observations did not concur with a survey in Wuhan, China, where older age and years of practice were associated with a significantly higher risk of infection.13
While responders worked at different hospitals with different patient flow rates and resources, the working environment had no impact on infection rates. This was similar for gender, marital status, and subspecialty.
In general, almost all responders (98.8%) indicated they were likely to contract the infection during practice, in agreement with a study from Cairo (Egypt).6 In addition, 59.6% of the responders, regardless of age and sex, reported that COVID-19 infection was very dangerous, while 37.9% indicated it was moderately dangerous. This reflected the huge burden of COVID-19 and agreed with an Egyptian study where 66% of the responders graded their psychological concerns by being anxious about their health and economic status.6 However, these feelings had no significant impact on the rate of infection among ophthalmologists.
Almost half of responders (80/163) were vaccinated. Yet, there was no link between the compliance to the vaccination and perception of disease severity. The vaccine was received after the start of the second wave this spring after a high percent of the doctors had already contracted the COVID-19 infection.
In examination rooms, the transmission risk to ophthalmologists can be lessened by following protective measures, precautions, and compliance steps. However, not all ophthalmologists are aware of these precautions, and importantly, not all strictly follow these rules. Moreover, the application of such preventive measures involves different hierarchical tiers, starting with medical facility management down to physician adherence.
In our survey, proper PPE training and precautions provided by individual medical facilities had no significant impact on infection rates. Notably, only 14% of the responders received their PPE training at a hands-on tutorial. These results agreed with a study from China.13 It appeared that most measures adopted by facilities were not adequately applied or effective to prevent the spread of infection.
However, ophthalmologist adherence to full personal protective measures, as recommended by the American Academy of Ophthalmology (AAO) when examining patients with or without respiratory illness, was significantly associated with a lower risk of infection (P-value = 0.019 and 0.046, respectively).16 The AAO recommended managing known COVID-19 patients at appropriately equipped hospitals.16 However, 45% of our responders reported they would treat a known COVID-19 patient in the outpatient clinic, but with precautions. This could have reflected the higher infection rates seen in our study. Importantly, these were higher than a Jordanian study.7
Also, full precautions while operating on suspected or nonsuspected COVID-19 patients were significantly associated with decreased COVID-19 infection rates. This observation agreed with a Hong Kong study that highlighted the importance of precautionary measures to protect healthcare workers.17 In a survey by Sanjay et al, these measures were further reinforced by limiting the number of elective cases.18
Our study had some limitations. It was performed online; hence, the response rate was relatively low when compared with face-to-face surveys. The data were limited to the short survey period; therefore, more updates are warranted.
Conclusions
Ophthalmologists have a high risk of COVID-19 infection. We observed that a young age and less ophthalmology experience were important risk factors for injection. This could be explained by the fact that the main ophthalmic services are provided by front-line trainees and young ophthalmologists. Critically, most of the survey responders in this study were in this group. Adherence to full protective measures in outpatient clinics and operating rooms significantly decreased infection risks.
Ethics Statement
Informed consent was obtained from all responders at the beginning of the questionnaire.
Ethics Committee
The study protocol was revised and approved by the Ophthalmology Department Ethics Committee at Cairo University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
2. Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;382(10):970–971. doi:10.1056/NEJMc2001468
3. Thapa B. Role of eyes and eyes protection amidst SARS-CoV-2 infection. JNMA J Nepal Med Assoc. 2021;59(233):108–110.
4. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
5. EuroTimes. Ophthalmologists among most at risk specialities by Jose L. Guell, MD, PHD. Available from: https://www.eurotimes.org/spanish-ophthalmologists-among-most-at-risk-specialties/.
6. Abdullatif AM, Makled HS, Hamza MM, Macky TA, El-Saied HM. Change in ophthalmology practice during COVID-19 pandemic: Egyptian perspective. Ophthalmologica. 2021;244(1):76–82.
7. Jammal HM, Alqudah NM, Khader Y. Awareness, perceptions, and attitude regarding coronavirus disease 2019 (COVID-19) among ophthalmologists in Jordan: cross-sectional online survey. Clin Ophthalmol. 2020;14:2195–2202. doi:10.2147/OPTH.S260460
8. Zhou Y, Duan C, Zeng Y, et al. Ocular findings and proportion with conjunctival SARS-COV-2 in COVID-19 patients. Ophthalmology. 2020;127(7):982–983. doi:10.1016/j.ophtha.2020.04.028
9. Lu CW, Liu XF, Jia ZF. 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395(10224):e39. doi:10.1016/S0140-6736(20)30313-5
10. What happens at an eye exam? WebMD. Available from: https://www.webmd.com/eye-health/what-to-expect-checkup-eye-exam-adults#2.
11. Nguyen AX, Gervasio K, Wu A. Differences in SARS-CoV-2 recommendations from major ophthalmology societies worldwide. BMJ Open Ophthalmol. 2020;5(1):000525. doi:10.1136/bmjophth-2020-000525
12. Lai TH, Tang EW, Chau SK, Fung KS, Li KK. Stepping up infection control measures in ophthalmology during the novel coronavirus outbreak: an experience from Hong Kong. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1049–1055. doi:10.1007/s00417-020-04641-8
13. Qiao C, Zhang H, He M, et al. Symptomatic COVID-19 in eye professionals in Wuhan, China. Ophthalmology. 2020;127(9):1268–1270. doi:10.1016/j.ophtha.2020.04.026
14. Ing EB, Xu QA, Salimi A, Torun N. Physician deaths from Corona virus (COVID-19) disease. Occup Med. 2020;70(5):370–374. doi:10.1093/occmed/kqaa088
15. Lacorzana J, Ortiz-Perez S, Rubio Prats M. Incidence of COVID-19 among ophthalmology professionals. Med Clin. 2020;155(5):225.
16. Alert: important coronavirus updates for ophthalmologists. American Academy of Ophthalmology; March 23, 2020. Available from: https://www.aao.org/headline/alert-important-coronavirus-context.
17. Kelvin KW, Yuen KY. Responding to COVID-19 in Hong Kong. Hong Kong Med J. 2020;26(3):164–166.
18. Sanjay S, Leo SW, Au Eong KG, et al. Global ophthalmology practice patterns during COVID-19 pandemic and lockdown. Ophthal Epidemiol. 2021:1–12. doi:10.1080/09286586.2021.1934037.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.