")
Back to Journals » Open Access Surgery » Volume 15
The Role of Anatomic Dimensions in the Development of Primary Small Bowel Volvulus, NorthWestern Ethiopia: A Case-control Study
Received 25 December 2021
Accepted for publication 16 February 2022
Published 24 February 2022 Volume 2022:15 Pages 17—23
DOI https://doi.org/10.2147/OAS.S355822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Agegnehu Bayeh,1 Belta Abegaz2
1Department of Surgery, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 2Department of Biomedical Sciences, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Agegnehu Bayeh, Department of Surgery, College of Medicine and Health Sciences, Bahir Dar University, PO Box 79, Bahir Dar, Ethiopia, Tel +251 923486085, Email [email protected]
Background: Anatomic dimensions of jejunum and ileum have been known to vary among individuals; however, their role in the development of primary small bowel volvulus was barely studied. The main objective of this study was to assess the role of small bowel anatomic dimensions in the development of primary small bowel volvulus.
Methods and Materials: A prospective case-control study to compare small bowel anatomic dimensions between patients with intraoperatively confirmed primary small bowel volvulus (cases) and control groups was conducted from December 2019 to December 2020 at Tibebe Ghion Specialized Hospital (TGSH) and Felege Hiwot Comprehensive Specialized Hospital (FHCSH), two referral hospitals in Bahir Dar city, NorthWestern Ethiopia. Jejunoileal length, mesenteric length, mesenteric root, and the ratio of small bowel mesenteric length to small bowel mesenteric root were compared between cases and controls using unpaired Student’s t-test, Welch’s t-test, or Mann–Whitney U-test at p-value ≤ 0.05 (two-sided).
Results: A total of 78 participants (39 cases and 39 controls) were included and analyzed in the study. Twenty-nine (74.4%) cases and 18 (46.2%) controls were males. The mean ages in years for cases and controls were 40.2 (SD=14.1) and 46.6 (SD=15.0), respectively. The study showed that patients with primary small bowel volvulus had statistically significantly longer small bowel length and small bowel mesenteric length than controls, but small bowel mesenteric root was found not to be statistically significantly different between cases and controls. The Mann–Whitney U-test for the comparison of the ratio of small bowel mesenteric length to small bowel mesenteric root showed that the mean rank was statistically significantly higher in cases than in the controls.
Conclusion: A longer small bowel with longer mesentery and higher small bowel mesenteric length to small bowel mesenteric root ratio is highly likely to predispose individuals to primary small bowel volvulus.
Keywords: bowel obstruction, intestine, jejunum, ileum, human anatomy, mesentery
Background
Primary small bowel volvulus is twisting of part or whole of the jejunoileal segment on its mesentery in a normal peritoneal cavity in the absence of anatomic abnormalities or with no clearly known predisposing factors.1–3 Small bowel volvulus is a rare finding in western countries like the United States with an incidence of 1%;4 however, it is a common surgical emergency in parts of Africa, Asia, and the Middle East.1,5–10 Though a population-based data is lacking, primary small bowel volvulus is common in Ethiopia, a country found in the volvulus belt.8–11 A study in North-Central Ethiopia found that primary small bowel volvulus was a cause for more than half of small bowel obstructions and one third of bowel obstructions.8 Even though there are no generally accepted explanations offered, research outputs postulated that several different predisposing factors might act combined to result in primary small bowel volvulus.5,6,9,11–14 Wide variations in small bowel length among individuals were observed in different studies;15–20 however, their role in primary small bowel volvulus was barely studied. Longer mesenteric length and short mesenteric root were hypothesized and reported to allow abnormal mobility of the entire or a segment of small bowel.1,2,6,19,20
To the best knowledge of the authors, these conclusions came from case reports and few patients with primary small bowel volvulus creating an easily seen and felt paucity of information on the role of small bowel anatomic dimensions in the development of primary small bowel volvulus.
The main objective of this case-control study on live cases was to assess the role of jejunoileal length, small bowel mesenteric length, mesenteric root, and small bowel mesenteric length to small bowel mesenteric root ratio in the development of primary small bowel volvulus.
It provides evidence that refine a scarcely addressed prior hypothesis regarding the anatomic basis of primary small bowel volvulus and contributes to the body of knowledge about primary small bowel volvulus in clinical anatomy, surgery, and gastroenterology. It also serves as a good founding and ingredient for future multicenter and multi-ethnic research.
Methods and Materials
Study Design, Area, and Period
A prospective case-control study was conducted from December 2019 to December 2020 at TGSH and FHCSH, two specialized referral hospitals with high volume of patient flow, located in Bahir Dar city, North-Western Ethiopia, with the former under Bahir Dar University (BDU), College of medicine and health sciences (CMHS) administration.
Sample Size Calculation
A total sample size of 78 (39 cases and 39 controls) was calculated with a priori power analysis using G*power software version 3.1.9.2 for a t-test to compare two means between two independent groups with a = 0.05, 1- β = 0.80, and Cohen’s d =0 0.65 (a relatively moderate effect).
Inclusion and Exclusion Criteria
Cases included consenting adults (≥18 years-of-age) for whom laparotomy was done and found to have a viable primary small bowel volvulus. Controls included consenting adults (≥18 years-of-age) for whom laparotomy was done for various reasons. Those with previous abdominal surgery, intraoperative hemodynamic instability, intraperitoneal sepsis, adhesions, gangrenous bowel, jejunal, ileal, cecal, and ascending colon pathologies, and those in whom reaching the small bowel was not possible for technical reasons were excluded from the study.
Data Quality Assurance and Data Collectors
Three senior residents in general surgery participated as data collectors. A one-day training was given to data collectors on the purpose of the study and the procedures to be followed during data collection by the principal investigators who also supervised the whole process; and a pre-developed data recording format was used.
Data Collection Procedures and Measurements
Three small bowel (jejunum and ileum) anatomic dimensions were taken (Figure 1): jejunoileal length (JIL) from duodenojejunal junction to the ileocecal junction along the antimesenteric border; small bowel mesenteric length (SBML)—the longest dimension of small bowel mesentery from the mesenteric border perpendicular to the root of the small bowel mesentery; and small bowel mesenteric root (SBMR) from the ligament of Treitz to the ileocecal junction. These were measured in centimeters using non-stretchable sterile measuring tape for consecutive cases and controls who fulfilled the inclusion criteria. SBML to SBMR ratio was calculated. These measurements and the age (in years), sex, height in centimeters (CMS), weight in kilograms (kg), body mass index (BMI, in kg/m2), medical registration numbers and other demographic data of patients were recorded to a pre-developed data collection format.
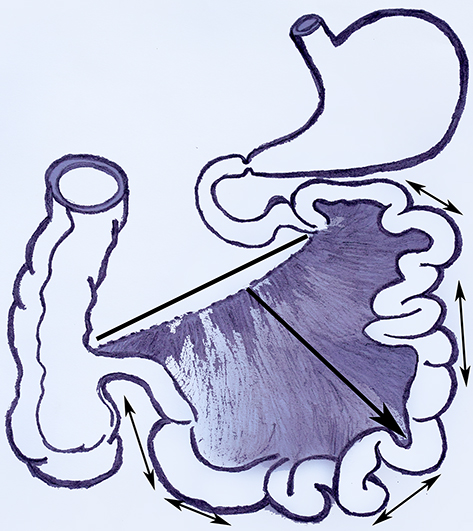 |
Figure 1 Small bowel anatomic dimensions. Jejunoileal length (double arrows); small bowel mesenteric length (single arrow); small bowel mesenteric root (thick line). It is a photograph of hand-sketched image processed using Microsoft paint and Adobe Photoshop CS3. |
Statistical Analysis
The collected data were checked for completeness and entered in to SPSS version 21 for analysis. Checking outliers, normality of distributions, and homogeneity of variances of continuous variables was analyzed using boxplots, Shapiro–Wilk test, and Levene’s test, respectively. The measurements of the small bowel anatomic dimensions were compared between cases and controls using unpaired Student’s t-test, Welch’s t-test, or Mann–Whitney U-test at p-value <0.05 (two-sided).
Results
Sociodemographic Data of Participants
A total of 78 participants, 39 of them with intraoperatively confirmed viable primary small bowel volvulus (cases) and the remaining 39 ones for whom abdominal surgery under general anesthesia was done for various reasons (controls) were included and analyzed in the study. Twenty-nine (74.4%) cases and 18 (46.2%) controls were males. Twenty-seven (69.2%) cases and 16 (41.0%) controls were from rural areas. The mean ages in years for the cases and controls were 40.2 (SD=14.1) and 46.6 (SD=15.0), respectively. The average BMI in kg/m2 for the cases and controls was 22.14 (SD=1.93) and 21.27 (SD = 2.48), respectively. No statistically significant difference was found in BMI and age between cases and controls (t (76)=1.736, p=0.087), and (Mann–Whitney U=568.5, p=0.055), respectively (Table 1).
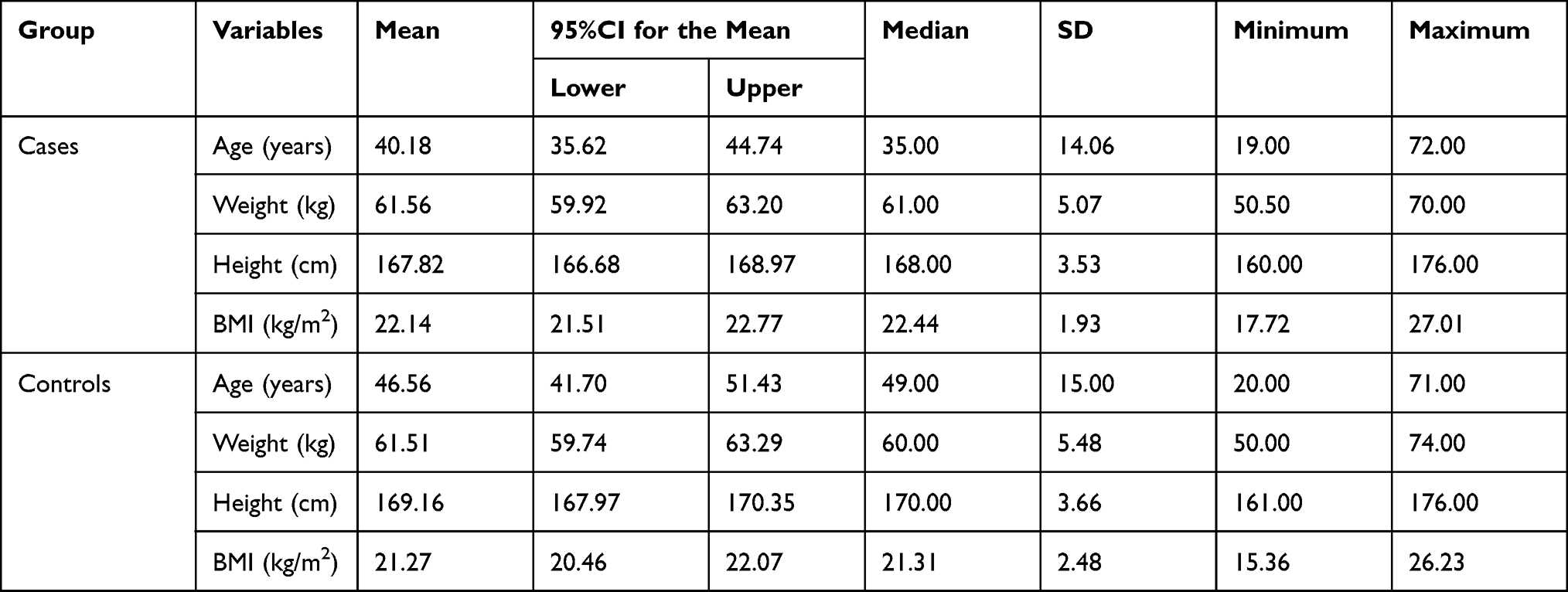 |
Table 1 Age, Weight, Height and BMI of Participants, North-Western Ethiopia |
Assumptions Test Results
As assessed by boxplots, there were no outliers in JIL, SBML, SBMR, and SBML to SBMR ratio for both cases and controls. Normality assessment using Shapiro–Wilk test showed that distributions of all small bowel anatomic dimensions were normal except SBML to SBMR ratio in controls which was found to be right skewed and for which the Mann–Whitney U-test was used to compare mean ranks. Levene’s test for homogeneity of variances showed that the assumption was met for SBML and SBML to SBMR ratio, but unmet for JIL and SBMR for which an unequal variance t-test was used for comparison of means (Table 2).
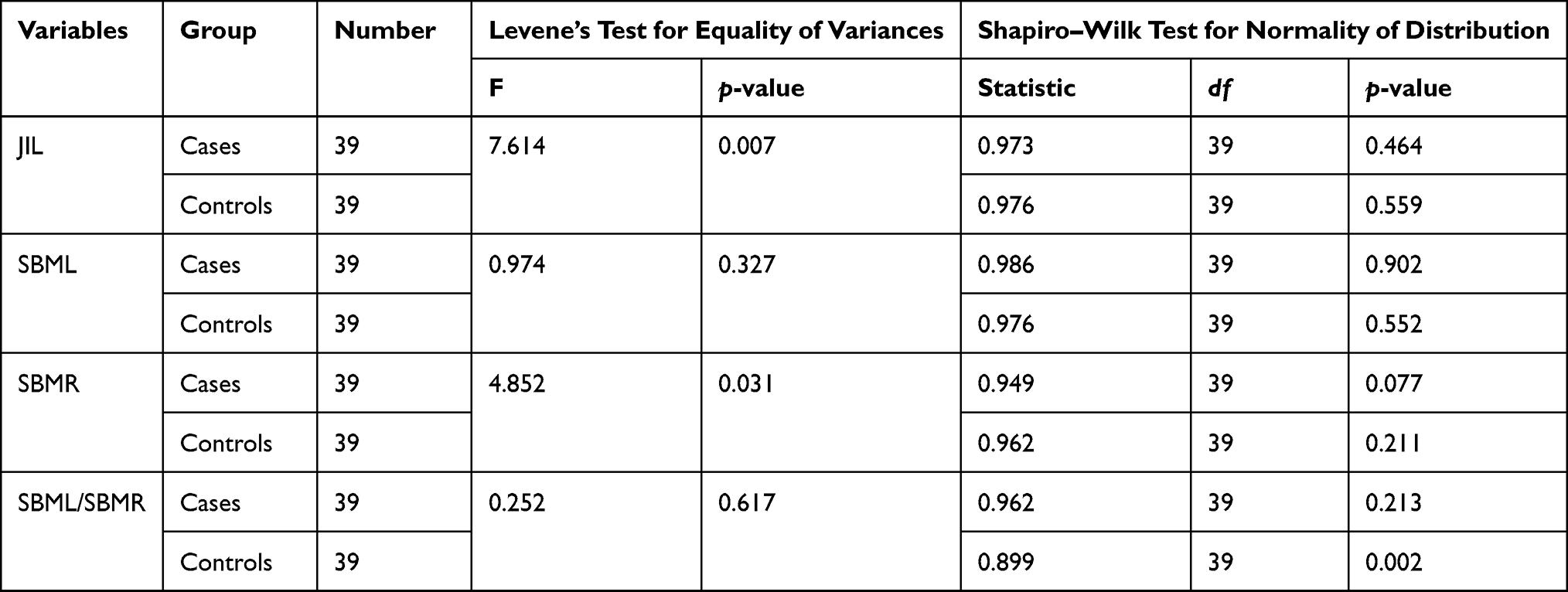 |
Table 2 Results of Levene’s Test for Equality of Variances and Shapiro–Wilk Test for Normality of Distributions, North-Western Ethiopia |
Measurements of Anatomic Dimensions
The study showed that cases have statistically significantly longer JIL (442.77±36.36) and SBML (23.05±3.37) than controls (418.69±22.35 and 19.47±2.78), t (63.133)=3.523, p=0.001, and t (76)=5.116, p<0.001, respectively. SBMR was found not to be statistically significantly different between cases (16.17±1.78) and controls (15.27±2.29), t (71.636)=1.934, p=0.057. The Mann–Whitney U-test for the comparison of SBML to SBMR ratio showed that the mean rank was statistically significantly higher in the cases than the controls (U=493.50, p=0.008) (Table 3).
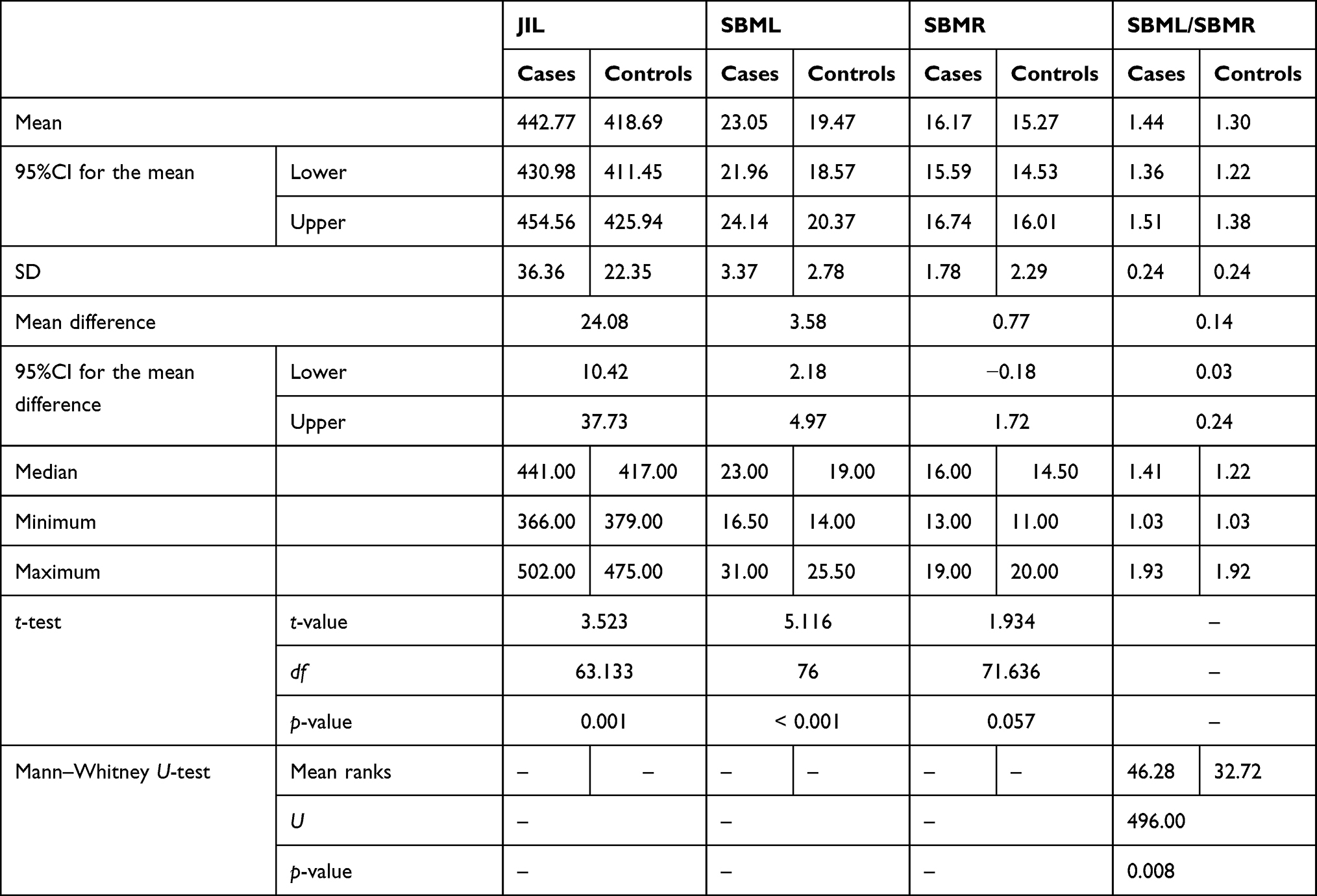 |
Table 3 Measurements of Small Bowel Anatomic Dimensions (in Centimeters), North-Western Ethiopia |
Discussion
Several factors contributing to the development of primary small bowel volvulus have been studied and reported. In areas where volvulus is common, primary small bowel volvulus affects predominantly relatively younger adult males and farmers.1,6,8,11,21 An interplay of hypermobility, hypermotility and high fiber bulky food following a period of fasting is thought to lead to small bowel twist. A bulky meal of high residue initiates small bowel volvulus. When this meal is taken on an empty bowel after a considerable period of no intake, the initial filled and consequently distended segments of jejunum descend down to the pelvis pushing the more distal empty ones up and to the left. Further distal movement of the meal, makes the loops heavier and get them down to the lower peritoneal cavity with the contribution of other factors like hypermotility causing rotation.1 Duke and Yar noticed that its occurrence was higher among Afghans during Ramadan.6 Consumption of large amount of local “Kongo beer” rich in serotonin which is a potent stimulant to bowel motility was also found to predispose to small bowel volvulus.14 A study in North-Western Ethiopia showed that primary small bowel volvulus admissions were higher in the seasons of winter and spring associated with the different seasonal activities of farmers.11 Other important risk factors are anatomic factors; however, their role in the development of primary small bowel volvulus has been scarcely addressed. To the best knowledge of the authors, there were few studies that tried to explore the role of anatomic dimensions in the development of primary small bowel volvulus each based on only six live cases and autopsies and/or estimates from standard anatomy text book as controls.1,21 Vaez-Zadeh et al theorized that long mesentery with narrow root could be a contributing factor to the mechanisms leading to the abnormal bowel twist.1
The current study on live cases and controls showed that participants with primary small bowel volvulus had statistically significantly longer jejunoileal length than controls. Contrary to this, in previous studies, jejunoileal length was found to be shorter in the cases with primary small bowel volvulus.1,21 However, these studies unlike the current one did not control the effect of postmortem changes on small bowel length18 which might be an important contributing factor to get longer small bowel length in the controls (autopsies). In consistent with this study, Koenig noticed that primary small bowel volvulus commonly occurs in nations known for longer small bowel length than those known for a relatively shorter one.22
In this study, small bowel mesenteric length was found to be statistically significantly longer in cases with primary small bowel volvulus than controls which is consistent with the findings and reports in previous studies.1,2,6,19,20
Although Vaez-Zadeh et al reported that small bowel mesenteric base was shorter in primary small bowel volvulus cases than in autopsies (controls), the current study showed that there was no statistically significant difference in small bowel mesenteric root between live cases and controls. This might be due to the fact that the sample size for the cases was too small (only six) and the controls were autopsies.1
Saidi reported that though a longer small bowel mesenteric breadth and a narrower mesenteric root were found in cases, the differences were not much to worry about.21
The other important small bowel anatomic dimension that was not reported in previous studies but addressed in this study was the ratio of small bowel mesenteric length to small bowel mesenteric root. It was found that the ratio was statistically significantly higher in patients with primary small bowel volvulus than in controls.
The authors of this study believe that it has some limitations. One is that the effect of acute small bowel volvulus (obstruction) on small bowel morphologic dimensions of cases was not controlled. Bowel when distended became elongated and the antimesenteric border of the bowel increased its length by 30%, whereas the mesenteric border increased by 10%.23 The study also lacked multicenter and multi-ethnic nature because it was confined to two hospitals in a single city. Interobserver differences among data collectors may also be an important source of bias. At last, there were no well-designed previous studies for better discussion, comparison, and contrast.
Conclusion
Cases with primary small bowel volvulus were found to have statistically significantly longer jejunoileal length, small bowel mesenteric length, and higher ratio of small bowel mesenteric length to small bowel mesenteric root. No statistically significant difference in small bowel mesenteric root was found between cases and controls. A longer small bowel with longer mesentery and higher SBML to SBMR ratio is highly likely to predispose individuals to primary small bowel volvulus.
Abbreviations
BMI, body mass index; cm, centimeter; FHCSH, Felege Hiwot Comprehensive Specialized Hospital; JIL, jejuno-ileal length; kg, kilogram; TGSH, Tibebe Ghion Specialized Hospital; SBML, small bowel mesenteric length; SBMR, small bowel mesenteric root; SD, standard deviation.
Data Sharing Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Before the start of the actual data collection, a letter of approval was obtained from the Institutional Review Board of BDU, CMHS (protocol number: 020160/18-09). A copy of this letter of approval was presented to the offices for directors of TGSH and FHCSH to obtain official permission to undergo the study.
Written informed consent was obtained from each participant before the data collection. The consent form was prepared in Amharic, the official language of the region and the country where the study was carried out and interpreted and/or explained for each participant by data collectors.
The study protocol was carried out in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vaez-Zadeh K, Dutz W, Nowrooz-Zadeh M. Volvulus of the small intestine in adults: a study of predisposing factors. Ann Surg. 1969;169(2):265–271. doi:10.1097/00000658-196902000-00014
2. Kim S-H, Cho Y-H, Kim H-Y. Primary segmental volvulus of small intestine: surgical perspectives according to age at diagnosis. Front Pediatr. 2019;7:146. doi:10.3389/fped.2019.00146
3. Tamura J, Kuniyoshi N, Maruwaka S, et al. “Whirl sign” of primary small bowel volvulus. West J Emerg Med. 2014;15(4):359–360. doi:10.5811/westjem.2014.4.20679
4. Coe TM, Chang DC, Sicklick JK. Small bowel volvulus in the adult populace of the United States: results from a population-based study. Am J Surg. 2015;210(2):201–210.e2. doi:10.1016/j.amjsurg.2014.12.048
5. Demissie M. Small intestinal volvulus in Southern Ethiopia. East Afr Med J. 2001;78(4):208–211. doi:10.4314/eamj.v78i4.9065
6. Duke JH, Yar MS. Primary small bowel volvulus: cause and management. Arch Surg. 1977;112(6):685–688. doi:10.1001/archsurg.1977.01370060017002
7. Roggo A, Ottinger LW. Acute small bowel volvulus in adults. A sporadic form of strangulating intestinal obstruction. Ann Surg. 1992;216(2):135–141. doi:10.1097/00000658-199208000-00003
8. Awedew AF, Belay WB, Amsalu BT, Yalewu DZ. Small bowel volvulus (SBV) in Northcentral Ethiopia. BMC Surg. 2020;20:221. doi:10.1186/s12893-020-00886-6
9. Tegegnie A. Small intestinal volvulus in adults of Gondar region, North West Ethiopia. Ethiop Med J. 1992;30(2):111–117.
10. Ghebrat K. The trend of small intestinal volvulus in North Western Ethiopia. East Afr Med J. 1998;75(9):549–552.
11. Ghebrat K. Seasonal variation of primary small intestinal volvulus in North Western Ethiopia. East Cent Afr J Surg. 2001;6(2).
12. Purcell LN, Reiss R, Mabedi C, Gallaher J, Maine R, Charles A. Characteristics of intestinal volvulus and risk of mortality in Malawi. World J Surg. 2020;44(7):2087–2093. doi:10.1007/s00268-020-05440-2
13. Agrawal S, Yadav AR, Nepal B, Upadhyay PK. Primary ileal volvulus: a rare twist in an elderly patient. BMC Surg. 2020;20:237. doi:10.1186/s12893-020-00901-w
14. De Souza LJ. Volvulus of the small bowel. Br Med J. 1976;1(6017):1055–1056. doi:10.1136/bmj.1.6017.1055
15. Khake SA, Mutalik MM. Variability of small bowel length: correlation with height, waist circumference, and gender. Ital J Anat Embryol. 2018;123(3):312–319. doi:10.13128/IJAE-25425
16. Raines D, Arbour A, Thompson HW, Figueroa-Bodine J, Joseph S. Variation in small bowel length: factor in achieving total enteroscopy? Dig Endosc. 2015;27(1):67–72. doi:10.1111/den.12309
17. Teitelbaum EN, Vaziri K, Zettervall S, Amdur RL, Orkin BA. Intraoperative small bowel length measurements and analysis of demographic predictors of increased length. Clin Anat. 2013;26:827–832. doi:10.1002/ca.22238
18. Weaver LT, Austin S, Cole TJ. Small intestinal length: a factor essential for gut adaptation. Gut. 1991;32:1321–1323. doi:10.1136/gut.32.11.1321
19. Paras KP, Ashish K, Ashwani K, Pankaj G, Nikhil M, Arun G. Primary small bowel volvulus. J Surg Acad. 2013;3(2):80–82.
20. Islam S, Hosein D, Dan D, Naraynsingh V. Volvulus of ileum: a rare cause of small bowel obstruction. BMJ Case Rep. 2016;2016:bcr2016216159. doi:10.1136/bcr-2016-216159
21. Saidi F. The high incidence of intestinal volvulus in Iran. Gut. 1969;10(10):838–841. doi:10.1136/gut.10.10.838
22. Koenig F. Liehrbuch der speciellen chirurgie fur aerzte und studierende [Textbook of special surgery for doctors and students]. Berlin: A. Hirschwald; 1904. German.
23. Perry EG. Intestinal volvulus: a new concept. Aust N Z J Surg. 1983;53(5):483–486. doi:10.1111/j.1445-2197.1983.tb02490.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.