")
Back to Journals » Patient Preference and Adherence » Volume 10
The role of adjunctive dexamethasone in the treatment of bacterial meningitis: an updated systematic meta-analysis
Authors Shao M, Xu P, Liu J, Liu W, Wu X
Received 2 April 2016
Accepted for publication 24 April 2016
Published 14 July 2016 Volume 2016:10 Pages 1243—1249
DOI https://doi.org/10.2147/PPA.S109720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Mei Shao,1 Peng Xu,2 Jun Liu,3 Wenyun Liu,1 Xiujie Wu1
1Department of Neurosurgery, Linyi People’s Hospital, 2Department of Neurosurgery, Linyi Yishui Central Hospital, Linyi, 3Department of Neurosurgery, Binzhou Medical College, Yantai, Shandong, People’s Republic of China
Background: Bacterial meningitis is a serious infection in children and adults worldwide, with considerable morbidity, mortality, and severe neurological sequelae. Dexamethasone is often used before antibiotics in cases of this disease, and improves outcomes.
Objective: Although several studies have identified the role of adjunctive dexamethasone therapy in the treatment of bacterial meningitis, the results are still inconclusive. The aim of this study was to systematically evaluate the therapeutic and adverse effect of adjunctive dexamethasone in patients with bacterial meningitis.
Materials and methods: Relevant randomized, double-blind, placebo-controlled trials of dexamethasone in bacterial meningitis published between 2000 and 2016 were retrieved from the common electronic databases. The odds ratio (OR) and risk ratio (RR) with their 95% confidence interval (CI) were employed to calculate the effect.
Results: A total of ten articles including 2,459 bacterial meningitis patients (1,245 in the dexamethasone group and 1,214 in the placebo group) were included in this meta-analysis. Our result found that dexamethasone was not associated with a significant reduction in follow-up mortality (292 of 1,245 on dexamethasone versus 314 of 1,214 on placebo; OR =0.91, 95% CI =0.80–1.03, P=0.14) and severe neurological sequelae (22.4% versus 24.1%, OR =0.84, 95% CI =0.54–1.29, P=0.42). However, dexamethasone seemed to reduce hearing loss among survivors (21.2% versus 26.1%; OR =0.76, 95% CI =0.59–0.98, P=0.03). No significant difference was found between these two groups in adverse events.
Conclusion: Our results suggested that adjunctive dexamethasone might not be beneficial in the treatment of bacterial meningitis. Future studies with more data are needed to further prove the role of dexamethasone in bacterial meningitis.
Keywords: bacterial meningitis, dexamethasone, treatment, meta-analysis
Introduction
Bacterial meningitis is a serious life-threatening disease with severe neurological emergency such as hearing loss, developmental disorders, and neuropsychological impairment, occurring in up to 50% of survivors of the disease.1 The clinical signs of bacterial meningitis include fever, headache, meningismus, an altered level of consciousness, and so on.2 It is ranked fourth as a cause of disability, and the estimated incidence is 1–2 million cases per year worldwide.3 Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis are the leading causes, still resulting in unacceptably high levels of human mortality and morbidity.4 Although routine vaccination against the common pathogens has decreased the burden of disease, improved the outcomes, and had a notable effect on the prevalence of bacterial meningitis,5,6 due to global emergence of multidrug-resistant bacteria, an estimated 1.2 million cases occur worldwide every year and 180,000 deaths in children aged 1–59 months were reported in 2010.7,8 In addition, bacterial meningitis often causes hearing loss and is fatal in 5%–40% of children and 20%–50% of adults despite treatment with adequate antibiotics.9 Early diagnosis and rapid initiation of empiric antimicrobial and adjunctive therapy are vital. Therefore, therapy should be initiated as soon as blood cultures have been obtained, preceding any imaging studies.
Corticosteroids, which have metabolic and regulatory functions in humans, are a class of steroid hormones that are produced in the adrenal cortex of vertebrates and the synthetic analogs of these hormones. They are implicated in a wide range of physiological processes such as stress response, immune response, inflammation regulation, carbohydrate metabolism, and protein catabolism.10 Corticosteroids can also attenuate the intrathecal inflammatory response caused by infection and are used as an adjunct to antibiotics in the treatment of bacterial meningitis, reducing the mortality and morbidity.11 Dexamethasone is a type of corticosteroid medication.12,13 The use of dexamethasone was significantly associated with improved cancer-related fatigue and quality of life.14 Dexamethasone therapy has been implemented as adjunctive treatment for bacterial meningitis and is correlated with a lower mortality and fewer neurological and auditory sequelae in adults and children.15 Moreover, the adjunctive dexamethasone therapy can improve survival for years in the acute phase in adults with community-acquired bacterial meningitis.16
Although several studies have shown that dexamethasone was used as a complementary therapy to antibacterials, it is still not clear whether it is effective in the treatment of bacterial meningitis because of the disparate findings from clinical trials and clinical evidence,17 and empirical use of dexamethasone in bacterial meningitis appears controversial.18,19 Borchorst and Møller20 found that dexamethasone treatment might be correlated with lower mortality and fewer neurological and auditory sequelae in adults and children from high-income countries, especially in adults suffering from pneumococcal meningitis. However, Peterković et al21 did not substantiate the reported benefits of adjunctive dexamethasone in adult bacterial meningitis based on 20 years of experience in daily practice. Therefore, we conducted this meta-analysis to systematically evaluate the role of dexamethasone in bacterial meningitis.
Materials and methods
Literature search
The electronic databases of PubMed, Embase, Medline, and the Chinese biomedicine literature were used to retrieve relevant articles published between January 2000 and 2016. The MeSH terms were “bacterial meningitis”, “dexamethasone or corticosteroids”, “treatment or therapy”, and their combinations. We also manually searched the references of retrieved articles to obtain more resources. We considered only those studies that were written in English and Chinese.
Inclusion criteria
The eligible articles must meet the following criteria: 1) randomized, double-blind, placebo-controlled trials of dexamethasone in the treatment of bacterial meningitis; 2) the diagnosis of bacterial meningitis was accepted in the presence of positive cerebrospinal fluid (CSF) culture, positive blood culture, positive latex agglutination test, or suggestive CSF cytology and biochemical profile;22 3) the primary outcomes were death at the time of first follow-up, severe neurological sequelae at first follow-up, and severe bilateral hearing loss at first follow-up; and 4) the search was focused on studies that had been conducted in humans.
Data extraction
Two of our authors independently assessed the quality of the included studies based on the descriptions provided by the authors of the included trials. Any disagreement was subsequently resolved by discussion with a third author to reach a final consensus on each item. The following information was extracted from each included article: the name of first author, year of publication, country, study period, age range, sample size, diagnostic criteria, dexamethasone dose, and primary outcomes.
Statistical analyses
Statistical analyses were conducted in Review Manager (Version 5.2, The Cochrane Collaboration). The overall effect was measured by odds ratios (ORs) and risk ratios (RRs) with their 95% confidence interval (CI). The significance of the pooled ratios was determined by the Z-test with a P-value <0.05 considered statistically significant. The I2 test and the Q-statistic test were employed to calculate the between-study heterogeneity. The fixed-effect model was used when the P-value for the Q-test was >0.10 and I2 for the I2 test was <50%; otherwise, the random-effect model was used when the effect was heterogeneous. The evidence of publication bias was assessed by visual funnel plot inspection. The sensitivity analysis was used to assess whether our results were substantially influenced by the presence of any individual study.
Results
Characteristics of included studies
After applying the inclusion criteria, a total of ten articles were finally screened out, including 2,459 patients (1,245 in the dexamethasone group and 1,214 in the placebo group) with bacterial meningitis. Figure 1 presents the process of literature search. The ten articles (two were written in Chinese23,24 and eight in English25–32) were conducted in six countries (the Netherlands, India, Malawi, Vietnam, Brazil, and the People’s Republic of China). All the patients were confirmed by clinically suspected bacterial meningitis plus CSF or blood criteria. The characteristics of the studies included in this analysis are listed in Table 1.
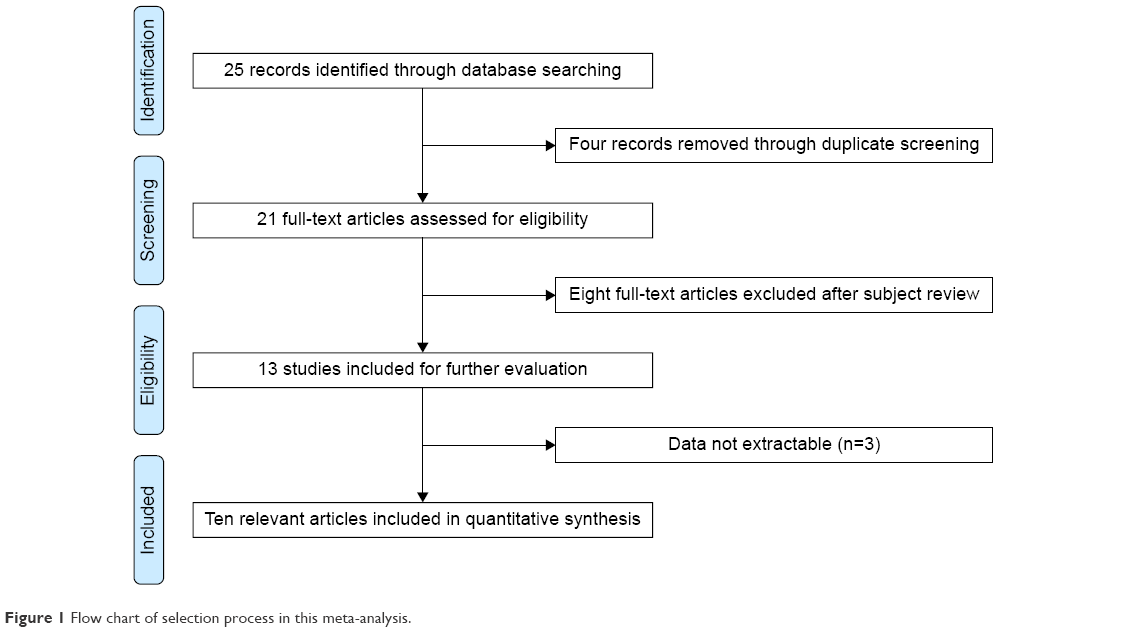 | Figure 1 Flow chart of selection process in this meta-analysis. |
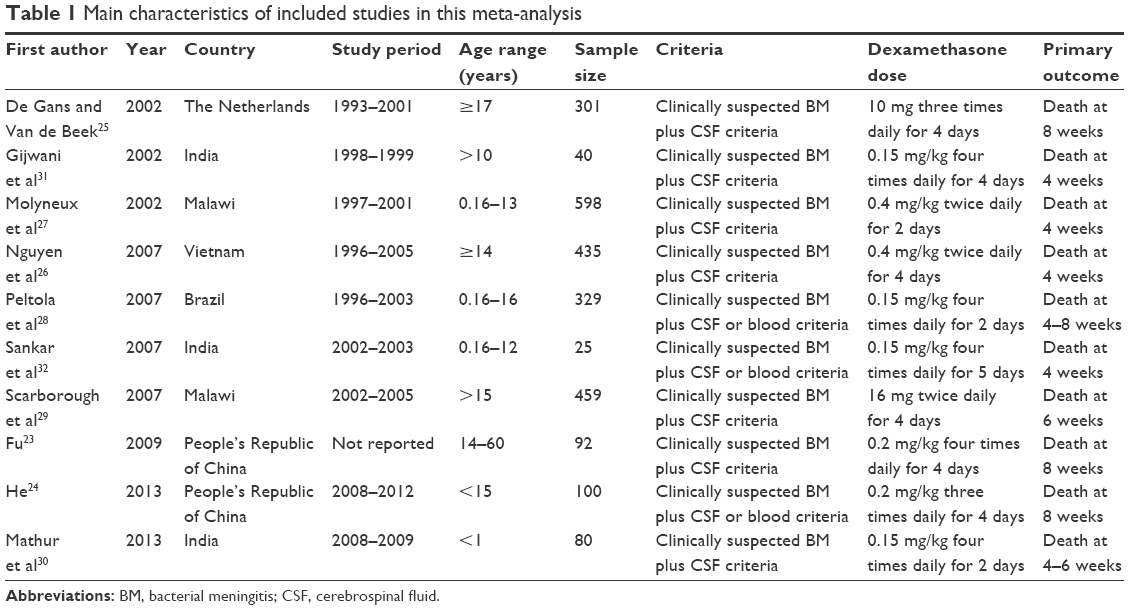 | Table 1 Main characteristics of included studies in this meta-analysis |
Curative effect analysis of dexamethasone in the treatment of bacterial meningitis
Follow-up mortality
All the ten articles reported the follow-up mortality of dexamethasone in the treatment of bacterial meningitis. No significant between-study heterogeneity was observed, and the fixed-effect model was used. Overall, we found that the frequency of follow-up mortality in the dexamethasone group was a little lower than that in the placebo group (23.5% versus 25.9%), but the statistical analysis proved that dexamethasone was not associated with a significant reduction in death (OR =0.91, 95% CI =0.80–1.03, P=0.14) as shown in Figure 2. Subgroup analysis by age group showed that dexamethasone was not correlated with follow-up mortality reduction either in adults (OR =0.93, 95% CI =0.79–1.09, P=0.39) or in children (OR =0.88, 95% CI =0.71–1.08, P=0.22).
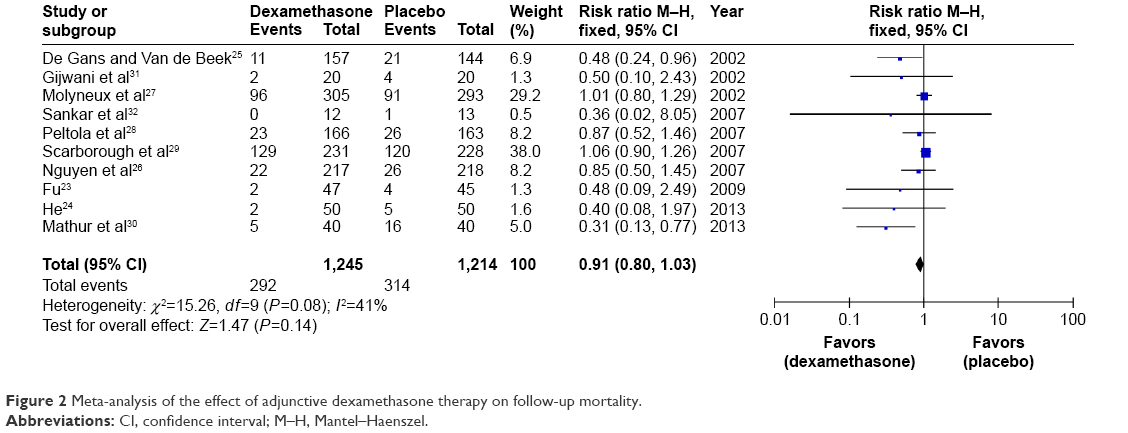 | Figure 2 Meta-analysis of the effect of adjunctive dexamethasone therapy on follow-up mortality. |
Hearing loss
Nine articles reported the incidence of hearing loss. Our result found that the frequency of hearing loss in the dexamethasone group was lower than that in the placebo group (21.2% versus 26.1%), and the statistical analysis found that dexamethasone was associated with a significant reduction in hearing loss (OR =0.76, 95% CI =0.59–0.98, P=0.03) as shown in Figure 3.
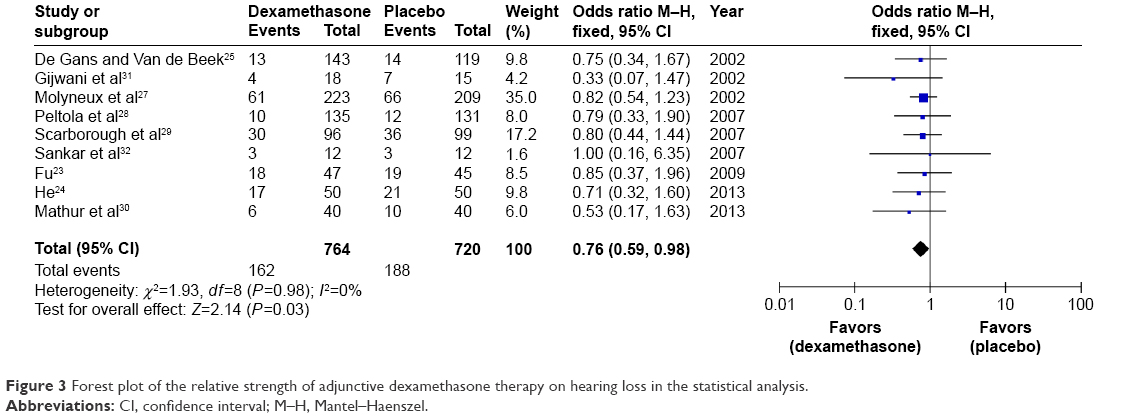 | Figure 3 Forest plot of the relative strength of adjunctive dexamethasone therapy on hearing loss in the statistical analysis. |
Neurological sequelae
Eight articles considered the role of dexamethasone in severe neurological sequelae of patients with bacterial meningitis. Our result demonstrated that dexamethasone was not associated with a significant reduction in severe neurological sequelae (22.4% versus 24.1%, OR =0.84, 95% CI =0.54–1.29, P=0.42) in the random-effect model as shown in Figure 4.
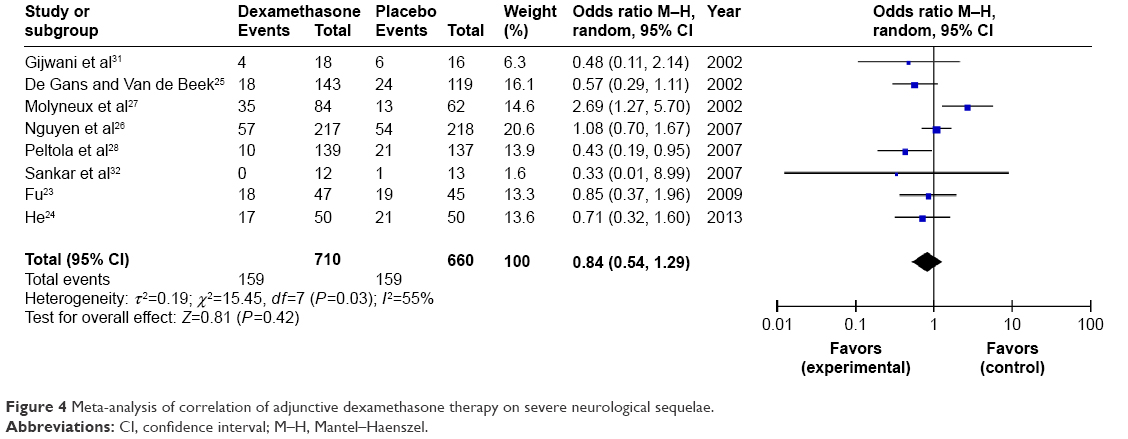 | Figure 4 Meta-analysis of correlation of adjunctive dexamethasone therapy on severe neurological sequelae. |
Adverse effect
Adverse events included gastrointestinal bleeding, hyperglycemia, hydrocephalus, blindness, second fever, and so on. These adverse events showed no significant difference between the dexamethasone group and the placebo group (P>0.05).
Sensitivity analysis and publication bias
We conducted a sensitivity analysis by systematically removing each study and recalculating the significance of the result to confirm whether each study influenced the overall results. Our result found that the pooled RRs and ORs were not significantly changed. The funnel plots were used to evaluate the publication bias. All the plots were found to be roughly symmetrical, indicating no publication bias as shown in Figure 5.
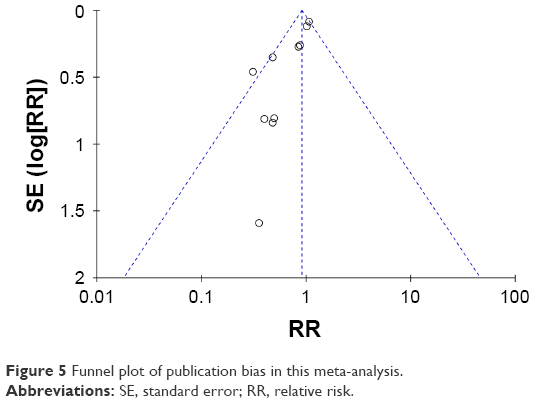 | Figure 5 Funnel plot of publication bias in this meta-analysis. |
Discussion
In this meta-analysis, we totally screened out ten articles, including 2,459 patients. Our result found that dexamethasone was not associated with a significant reduction in follow-up mortality (P=0.14) and severe neurological sequelae (P=0.42). However, dexamethasone seemed to reduce hearing loss among survivors (P=0.03). No significant difference was found between these two groups in adverse events. Our results were consistent with those of previous meta-analysis, which showed that adjunctive dexamethasone in the treatment of acute bacterial meningitis did not seem to significantly reduce death or neurological disability but reduced the hearing loss among survivors.33
Bacterial meningitis is a severe acute infectious disease. The intense inflammatory host’s response is potentially fatal and contributes to the neurological sequelae. The poor outcomes are mainly due to secondary systemic and intracranial complications resulting from a consequence of the inflammatory response to the invading pathogen and release of bacterial components by the pathogen itself.34 The inflammatory reaction involving the meninges, the subarachnoid space, and the brain parenchymal vessels was shown to contribute to neuronal injury.35 The harmful inflammatory response is initiated by the recognition of bacterial products through pattern recognition receptors.36 Despite effective antimicrobial therapy, the morbidity and mortality still remain high. Adequate and prompt treatment of bacterial meningitis is critical to outcome.
Dexamethasone is used to treat many inflammatory and autoimmune conditions. It can trigger a wide cellular response modulating the expression of genes involved in the innate immune system, growth, and stress and increases susceptibility to bacterial disease.37 High-dose dexamethasone was shown to modulate serum cytokine profile in patients with primary immune thrombocytopenia.38 Dexamethasone is often administered before antibiotics in cases of bacterial meningitis. It then acts to reduce the inflammatory response of the body to the bacteria killed by the antibiotics (bacterial death releases proinflammatory mediators that can cause a response that is harmful to the patient), thus improving prognosis and outcome.39
Many studies have identified the role of dexamethasone in the treatment of bacterial meningitis. However, the results still remain inconclusive. Bodilsen et al40 proved that patients treated with dexamethasone were more likely to have a favorable outcome. Baunbæk-Knudsen et al41 indicated that adjuvant corticosteroid treatment in acute bacterial meningitis improved the outcome and could safely be administered in an elderly population with high levels of immunosuppressive comorbidity. Heckenberg et al42 suggested that adjunctive dexamethasone was widely prescribed for patients with meningococcal meningitis, was not associated with harm, and the rate of arthritis had decreased after the implementation of dexamethasone. Weisfelt et al43 showed that treatment with adjunctive dexamethasone was not associated with an increased risk for long-term cognitive impairment. Brouwer et al44 demonstrated that the corticosteroid dexamethasone did not significantly reduce the death rate, but patients treated with corticosteroids had significantly lower rates of severe hearing loss, any hearing loss, and neurological sequelae.
The combination of dexamethasone plus other antibodies might be the new treatment strategy for patients with bacterial meningitis. Kasanmoentalib et al45 found that adjunctive treatment with dexamethasone plus anti-C5 antibodies improved the survival in severe experimental meningitis caused by S. pneumoniae serotype 3. Vivas et al46 showed that low-dose daptomycin was affected by concomitant use of dexamethasone, suggesting that the combination appeared to be a good choice for the treatment of pneumococcal meningitis. Du et al47 suggested that dexamethasone could downregulate the expression of AQP4 in the brain tissue of rats with meningitis and provided evidence for the mechanism of protective effect of dexamethasone on the central nervous system.
Dexamethasone may also have some adverse effect in the treatment of bacterial meningitis. Leib et al48 demonstrated that dexamethasone as adjuvant therapy increased hippocampal cell injury and reduced learning capacity in the model of pneumococcal meningitis in infant rats. Spreer et al49 found that dexamethasone increased the rate of apoptotic neurons in the granular layer of the hippocampal dentate gyrus in rabbits with Escherichia coli meningitis.
There were several limitations in our present meta-analysis. First, the event numbers of each included study were too small to show whether results were positive or negative. Second, dexamethasone in the treatment of bacterial meningitis was all short-course therapy, thus less side effects were reported. Third, the performance of adjunctive therapy with dexamethasone in bacterial meningitis was shown to be dependent on circumstances;50 therefore, other related factors should be considered. Finally, the dexamethasone dose and empiric antibiotic therapy were different in each study, which may have influenced our results.
Conclusion
Our results indicated that patients with bacterial meningitis neither benefit from nor are harmed by treatment with adjunctive dexamethasone. Future well-designed, large-sample studies are still needed to further evaluate the role of dexamethasone in the treatment of bacterial meningitis.
Disclosure
The authors report no conflicts of interest in this work.
References
Heckenberg SG, Brouwer MC, van de Beek D. Bacterial meningitis. Handb Clin Neurol. 2013;121:1361–1375. | ||
Van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med. 2004;351(18):1849–1859. | ||
Castelblanco RL, Lee M, Hasbun R. Epidemiology of bacterial meningitis in the USA from 1997 to 2010: a population-based observational study. Lancet Infect Dis. 2014;14(9):813–819. | ||
Namani S, Milenkovic Z, Kuchar E, Koci R, Mehmeti M. Mortality from bacterial meningitis in children in Kosovo. J Child Neurol. 2012;27(1):46–50. | ||
McIntyre PB, O’Brien KL, Greenwood B, van de Beek D. Effect of vaccines on bacterial meningitis worldwide. Lancet. 2012;380(9854):1703–1711. | ||
Glimåker M, Johansson B, Grindborg Ö, Bottai M, Lindquist L, Sjölin J. Adult bacterial meningitis: earlier treatment and improved outcome following guideline revision promoting prompt lumbar puncture. Clin Infect Dis. 2015;60(8):1162–1169. | ||
van de Beek D. Progress and challenges in bacterial meningitis. Lancet. 2012;380(9854):1623–1624. | ||
van de Beek D, Brouwer MC, Thwaites GE, Tunkel AR. Advances in treatment of bacterial meningitis. Lancet. 2012;380(9854):1693–1702. | ||
Rodenburg-Vlot MB, Ruytjens L, Oostenbrink R, Goedegebure A, van der Schroeff MP. Systematic review: incidence and course of hearing loss caused by bacterial meningitis: in search of an optimal timed audiological follow-up. Otol Neurotol. 2016;37(1):1–8. | ||
Grant P. Coumarin anticoagulants and endocrine interactions. Coumarin Anticoagulant Research Progress; 2008;1:11. | ||
Shin M. Dexamethasone in bacterial meningitis. Ethics. 2015;8(3):3090–3096. | ||
Cáceres-del-Carpio J, Donato Costa R, Haider A, Narayanan R, Kuppermann BD. Corticosteroids: Triamcinolone, Dexamethasone and Fluocinolone. Dev Ophthalmol. 2016;55:221–231. | ||
Pukkila-Worley R. Dexamethasone/prednisone. Reactions. 2015;1552:93. | ||
Franco M, William L, Poon P, Azad A. Dexamethasone for cancer-related fatigue. J Clin Oncol. 2014;32(6):608–609. | ||
Ogunlesi TA, Odigwe CC, Oladapo OT. Adjuvant corticosteroids for reducing death in neonatal bacterial meningitis. Cochrane Database Syst Rev. 2015;11:CD010435. | ||
Fritz D, Brouwer MC, van de Beek D. Dexamethasone and long-term survival in bacterial meningitis. Neurology. 2012;79(22):2177–2179. | ||
Esposito S, Semino M, Picciolli I, Principi N. Should corticosteroids be used in bacterial meningitis in children? Eur J Paediatr Neurol. 2013;17(1):24–28. | ||
Pfausler B, Schmutzhard E. Controversies in neurology, Vienna, 2012: steroids in bacterial meningitis: no. J Neural Transm (Vienna). 2013;120(2):343–346. | ||
Benninger F, Steiner I. Steroids in bacterial meningitis: yes. J Neural Transm (Vienna). 2013;120(2):339–342. | ||
Borchorst S, Møller K. The role of dexamethasone in the treatment of bacterial meningitis-a systematic review. Acta Anaesthesiol Scand. 2012;56(10):1210–1221. | ||
Peterković V, Trkulja V, Kutleša M, Krajinović V, Lepur D. Dexamethasone for adult community-acquired bacterial meningitis: 20 years of experience in daily practice. J Neurol. 2012;259(2):225–236. | ||
Leib SL, Boscacci R, Gratzl O, Zimmerli W. Predictive value of cerebrospinal fluid (CSF) lactate level versus CSF/blood glucose ratio for the diagnosis of bacterial meningitis following neurosurgery. Clin Infect Dis. 1999;29(1):69–74. | ||
Fu X. Dexamethasone in adolescents and adults with bacterial meningitis. China Pract Med. 2009;4(12):82–83. | ||
He Y. Clinical observation of adjuvant dexamethasone in treatment of childhood bacterial meningitis. China Foreign Med Treat. 2013;32(30):91–92. | ||
De Gans J, Van de Beek D; European Dexamethasone in Adulthood Bacterial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549–1556. | ||
Nguyen TH, Tran TH, Thwaites G, et al. Dexamethasone in Vietnamese adolescents and adults with bacterial meningitis. N Engl J Med. 2007;357(24):2431–2440. | ||
Molyneux EM, Walsh AL, Forsyth H, et al. Dexamethasone treatment in childhood bacterial meningitis in Malawi: a randomised controlled trial. Lancet. 2002;360(9328):211–218. | ||
Peltola H, Roine I, Fernández J, et al. Adjuvant glycerol and/or dexamethasone to improve the outcomes of childhood bacterial meningitis: a prospective, randomized, double-blind, placebo-controlled trial. Clin Infect Dis. 2007;45(10):1277–1286. | ||
Scarborough M, Gordon SB, Whitty CJ, et al. Corticosteroids for bacterial meningitis in adults in sub-Saharan Africa. N Engl J Med. 2007;357(24):2441–2450. | ||
Mathur NB, Garg A, Mishra TK. Role of dexamethasone in neonatal meningitis: a randomized controlled trial. Indian J Pediatr. 2013;80(2):102–107. | ||
Gijwani D, Kumhar MR, Singh VB, et al. Dexamethasone therapy for bacterial meningitis in adults: a double blind placebo control study. Neurol India. 2002;50(1):63–67. | ||
Sankar J, Singhi P, Bansal A, Ray P, Singhi S. Role of dexamethasone and oral glycerol in reducing hearing and neurological sequelae in children with bacterial meningitis. Indian Pediatr. 2007;44(9):649–656. | ||
van de Beek D, Farrar JJ, de Gans J, et al. Adjunctive dexamethasone in bacterial meningitis: a meta-analysis of individual patient data. Lancet Neurol. 2010;9(3):254–263. | ||
Woehrl B, Klein M, Grandgirard D, Koedel U, Leib S. Bacterial meningitis: current therapy and possible future treatment options. Expert Rev Anti Infect Ther. 2011;9(11):1053–1065. | ||
Barichello T, Fagundes GD, Generoso JS, Elias SG, Simões LR, Teixeira AL. Pathophysiology of neonatal acute bacterial meningitis. J Med Microbiol. 2013;62(pt 12):1781–1789. | ||
Koedel U, Klein M, Pfister H-W. In: Peterson PK, Toborek M, editors. Immunopathogenesis of bacterial meningitis. Neuroinflammation and Neurodegeneration. New York: Springer; 2014:387–404. | ||
Salas-Leiton E, Coste O, Asensio E, Infante C, Cañavate JP, Manchado M. Dexamethasone modulates expression of genes involved in the innate immune system, growth and stress and increases susceptibility to bacterial disease in Senegalese sole (Solea senegalensis Kaup, 1858). Fish Shellfish Immunol. 2012;32(5):769–778. | ||
Zhan Y, Zou S, Hua F, et al. High-dose dexamethasone modulates serum cytokine profile in patients with primary immune thrombocytopenia. Immunol Lett. 2014;160(1):33–38. | ||
van de Beek D, de Gans J, McIntyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cochrane Database Syst Rev. 2007;1:CD004405. | ||
Bodilsen J, Dalager-Pedersen M, Schønheyder HC, Nielsen H. Dexamethasone treatment and prognostic factors in community-acquired bacterial meningitis: a Danish retrospective population-based cohort study. Scand J Infect Dis. 2014;46(6):418–425. | ||
Baunbæk-Knudsen G, Sølling M, Farre A, Benfield T, Brandt CT. Improved outcome of bacterial meningitis associated with use of corticosteroid treatment. Infect Dis (Lond). Epub 2015 Nov 11. | ||
Heckenberg SG, Brouwer MC, van der Ende A, van de Beek D. Adjunctive dexamethasone in adults with meningococcal meningitis. Neurology. 2012;79(15):1563–1569. | ||
Weisfelt M, Hoogman M, van de Beek D, de Gans J, Dreschler WA, Schmand BA. Dexamethasone and long-term outcome in adults with bacterial meningitis. Ann Neurol. 2006;60(4):456–468. | ||
Brouwer MC, McIntyre P, Prasad K, van de Beek D. Corticosteroids for bacterial meningitis. Health. 2013;6:CD004405. | ||
Kasanmoentalib ES, Valls Seron M, Morgan BP, Brouwer MC, van de Beek D. Adjuvant treatment with dexamethasone plus anti-C5 antibodies improves outcome of experimental pneumococcal meningitis: a randomized controlled trial. J Neuroinflammation. 2015;12(1):149. | ||
Vivas M, Force E, Tubau F, El Haj C, Ariza J, Cabellos C. Effect of dexamethasone on the efficacy of daptomycin in the therapy of experimental pneumococcal meningitis. Int J Antimicrob Agents. 2015;46(1):28–32. | ||
Du KX, Dong Y, Zhang Y, et al. Effects of dexamethasone on aquaporin-4 expression in brain tissue of rat with bacterial meningitis. Int J Clin Exp Pathol. 2015;8(3):3090–3096. | ||
Leib SL, Heimgartner C, Bifrare YD, Loeffler JM, Täuber MG. Dexamethasone aggravates hippocampal apoptosis and learning deficiency in pneumococcal meningitis in infant rats. Pediatr Res. 2003;54(3):353–357. | ||
Spreer A, Gerber J, Hanssen M, et al. Dexamethasone increases hippocampal neuronal apoptosis in a rabbit model of Escherichia coli meningitis. Pediatr Res. 2006;60(2):210–215. | ||
Peltola H, Leib SL. Performance of adjunctive therapy in bacterial meningitis depends on circumstances. Pediatr Infect Dis J. 2013;32(12):1381–1382. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.