")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
The Risk of Cerebrovascular Accidents in Inflammatory Bowel Disease in the United States: A Population-Based National Study
Authors Ghoneim S , Shah A, Dhorepatil A , Butt MU , Waghray N
Received 12 March 2020
Accepted for publication 9 April 2020
Published 4 May 2020 Volume 2020:13 Pages 123—129
DOI https://doi.org/10.2147/CEG.S250182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Everson L.A. Artifon
Sara Ghoneim,1 Aun Shah,1 Aneesh Dhorepatil,1 Muhammad Umer Butt,2 Nisheet Waghray3
1Department of Internal Medicine, Case Western Reserve University at MetroHealth Medical Center, Cleveland, OH 44109, USA; 2Division of Cardiology, Case Western Reserve University at MetroHealth Medical Center, Cleveland, OH 44109, USA; 3Division of Gastroenterology, Case Western Reserve University at MetroHealth Medical Center, Cleveland, OH 44109, USA
Correspondence: Sara Ghoneim
Department of Internal Medicine, Case Western Reserve University at MetroHealth Medical Center, 2500 MetroHealth Drive, Cleveland, OH 44109, USA
Tel +1-216-777-0498
Email [email protected]
Background: Inflammatory bowel disease (IBD) has been associated with an increased risk of cardiovascular events, but the risk of cerebrovascular accidents (CVA) remains unknown. Hypercoagulability and systemic inflammation are two proposed mechanisms by which the presence of IBD might lead to the development of CVA.
Objective: To assess the risk of CVA in patients with IBD compared to those without IBD with known traditional risk factors for CVA.
Methods: We reviewed data from a large commercial database (Explorys, IBM) that aggregated records from 26 health-care systems nationwide. Using systemized nomenclature of medicine – clinical terms, we identified adult patients diagnosed with IBD (ulcerative colitis or Crohn’s disease) between September 1994 and September 2019. We then examined the risk of CVA in these patients. Known risk factors such as age ≥ 65-years old, diabetes mellitus (DM), hypertension (HTN), female gender, atrial fibrillation (Afib) were collected. A univariate binary logistic model was constructed using CVA as the dependent variable and other variables as independent variables. To adjust for possible confounding, a multivariable model adjusting for all covariates was created to test for CVA.
Results: A total of 52,176,550 patients were included in this analysis, and 261,890 had IBD. The prevalence of CVA was higher in IBD patients compared to non-IBD patients (6.24% versus 0.48%, p < 0.0001). The univariate binary logistic regression showed 13.7 times higher odds of having CVA in IBD patients than without IBD (odds ratio (OR) 13.74, p < 0.0001). In multivariate binary logistic regression, after adjusting for traditional risk factors for CVA (Afib, HTN, female gender, DM, age ≥ 65 years), odds ratio of CVA in IBD patients remained significantly higher (OR 8.07, 95% CI: 7.9– 8.2, p< 0.0001).
Conclusion: In our large cohort of patients, IBD appears to be an independent risk factor for CVA. Further prospective studies are needed to understand the underlying mechanisms by which IBD increases the risk of CVA. This may lead to early identification and intervention to reduce the risk of CVA in this highly heterogeneous group of patients.
Keywords: inflammatory bowel disease, cerebrovascular accident, IBD, CVA
Introduction
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), is a chronic debilitating disorder characterized by recurrent intestinal and systemic inflammation.1 It is estimated that 1.3% of the US adult population are diagnosed with IBD. There is a significant healthcare burden associated with IBD, with costs estimated to be between 14.1 and 31.6 billion dollars per year.2
The role of inflammation in the progression of atherosclerosis has fueled research to determine whether chronic inflammatory states such as IBD carry an increased risk of cardiovascular or cerebrovascular disease.2,3 Patients with IBD have long been known to have an increased risk of venous thromboembolic events (VTE), yet the risk of arterial thromboembolic events is not well characterized. Only recently have studies shown an increased risk of myocardial infarctions (MI) and cerebrovascular accidents (CVA) in patients with rheumatoid arthritis, psoriasis and systemic lupus erythematosus.4,5 However, this association with IBD remains debatable. With some studies showing a clear association between the risk of CVA and IBD and others failing to confirm this association.1,6
Stroke is a heterogeneous multifactorial disease that involves a complex interplay of genetic, environmental and vascular factors.7,8 It is the second leading cause of death, after ischemic heart disease, accounting for 9% of deaths worldwide. The prevalence of stroke in the United States is estimated to be 3%.9,10 Traditional risk factors such as hypertension, diabetes, atrial fibrillation, smoking, and advanced age have been known to increase the risk of stroke in the general population.9,10
Establishing a link between IBD and arterial thromboembolic diseases, including CVA, may have serious implications. Therefore, whether IBD increases the risk of CVA in the US population remains elusive and subject to debate. Given the lack of consensus on this important issue, and the ambiguity of data around this question, the aim of this study is to investigate the association between IBD and CVA in the US population.
Materials and Methods
Study Design
This is a retrospective analysis of a large electronic health record (EHR)-based commercial database called Explorys (IBM, Watson) that contains patient information from 26 different health-care systems spread over 50 states in the United States with over 50 million unique patient records.11 Each participating institution provides de-identified data from electronic health records.11 This data is then standardized, normalized and stored in a cloud database.11,12 Explorys uses Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) coding for medical diagnoses and procedures. For diagnoses, International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM) codes are mapped into the SNOMED-CT hierarchy. Cohorts can further be refined demographically and also allow for the identification of comorbidities.11,12 The use of Explorys platform has been validated in multiple fields including cardiology and gastroenterology.12 Explorys is Health Insurance Portability and Accountability Act (HIPAA) and Health Information Technology for Economic and Clinical Health Act (HITECH) compliant.11,12 To protect patient confidentiality, Explorys rounds population counts to the nearest 10 and treats all counts between zero and 10 as equivalent. For the purposes of this study, counts between 0 and 10 were approximated to be five.
Patient Selection
For this study, we used Explorys search tool to identify all non-deceased adult patients with active records since 1999. Patients with IBD were identified by searching the database for cases with listed SNOMED-CT diagnosis “inflammatory bowel disease”. Patients with CVA were identified as those with the following SNOMED-CT diagnosis “cerebrovascular accidents”. Controls were identified as those patients without the diagnosis of IBD. For our analysis, we identified cohorts of patients with IBD with and without CVA. We were unable to perform propensity-score matching because the Explorys platform only provides population-level data and not individual cases.
Covariates
We collected information on patient demographics and comorbidities known to be associated with an increased risk of IBD and CVA (eg, hypertension, diabetes mellitus, atrial fibrillation, age and gender) by searching the database for their respective SNOMED-CT terms.
Statistical Analysis
To assess the association between IBD with risk factors we divided the whole cohort of patients into IBD and Non-IBD patients. The prevalence of CVA in each risk group was calculated by dividing the number of patients with IBD in each risk group. Categorical variables are presented as numbers and percentages and were compared using the Pearson χ2 test. Odds ratios (OR) are presented with 95% confidence intervals (CI). Univariate binary logistic model was constructed using CVA as the dependent variable and other variables as independent variables. To adjust for possible confounding, a multivariable model adjusting for all covariates mentioned in univariate variables were added to test the main effect. Independence among covariate risk factors was assessed using the variance inflating factor (VIF) with cut-off of significant collinearity set at VIF > 1.5. “Goodness-of-fit” was assessed for all regression models using the Hosmer–Lemeshow test, with P > 0.05 indicating a good fit. All statistical analysis was done using SAS version 9.4 (SAS Inst., Cary, NC). Significance was defined as the 2-tailed value of p<0.05.
Regulatory Approvals
The Case Western Reserve University/Metrohealth Medical Center Institutional Review Board deemed studies using Explorys as the data set of record as exempt from approval because all data are de-identified.
Results
Out of 52,176,550 patients, 261,890 patients were diagnosed with IBD (0.50%) and 179,400 (0.34%) had a CVA. Baseline characteristics of subjects included in this study are displayed in Table 1. Of the IBD group, 103,850 subjects were diagnosed with hypertension, 52,820 had diabetes and 17,700 with atrial fibrillation. Cerebrovascular accidents were seen in 11,200 IBD subjects and 168,230 subjects without IBD (Table 1).
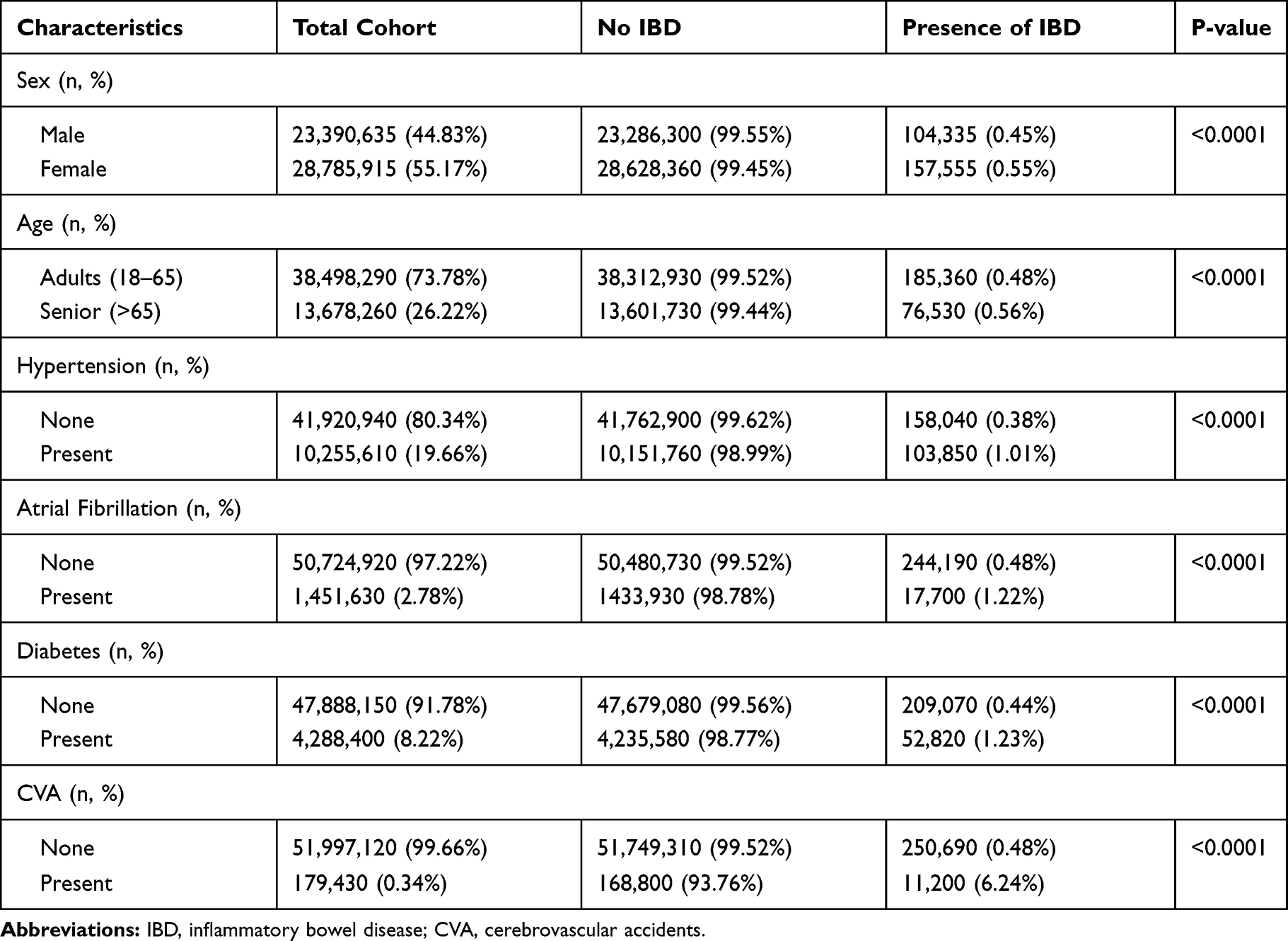 |
Table 1 Baseline Characteristics of the Study Population |
In overall unadjusted analysis, IBD was associated with an increased risk of CVA (odds ratio (OR) 13.74 [95% CI: 13.478–14.02, p<0.0001]). With regard to traditional risk factors, diabetes and atrial fibrillation were associated with an increased risk of CVA (OR 13.77 [13.59–13.82]; OR 13.30 [13.17–13.42], respectively. Hypertension was also associated with an increased risk of CVA OR 11.86 [11.75–11.98] while age ≥65 remained significantly associated with the risk of CVA OR 5.16 [5.12–5.21]. The female gender had a modest association with CVA with an OR 1.07 [1.06–1.08].
In our multivariate model, after adjusting for age, gender, hypertension, diabetes and atrial fibrillation, the presence of IBD had the strongest association with CVA (OR 8.08 95% CI: 7.91–8.24) (Table 2). Regarding traditional risk factors, diabetes remained second and was strongly associated with the risk of CVA (OR 4.86 (95% CI: 4.81–4.92). Atrial fibrillation and hypertension were associated with an increased risk of CVA (OR 3.35, 95% CI: 3.31–3.39; OR 3.141, 95% CI: 3.10–3.18), respectively. Similar to our unadjusted model, the female gender was found to have a modest association with the occurrence of CVA (OR 1.18 [1.17–1.120] (Figure 1).
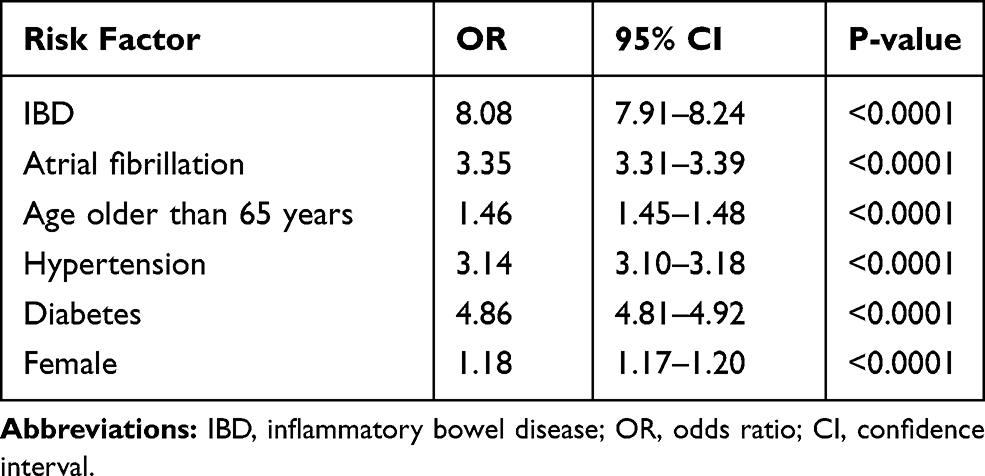 |
Table 2 Multivariate Regression Analysis |
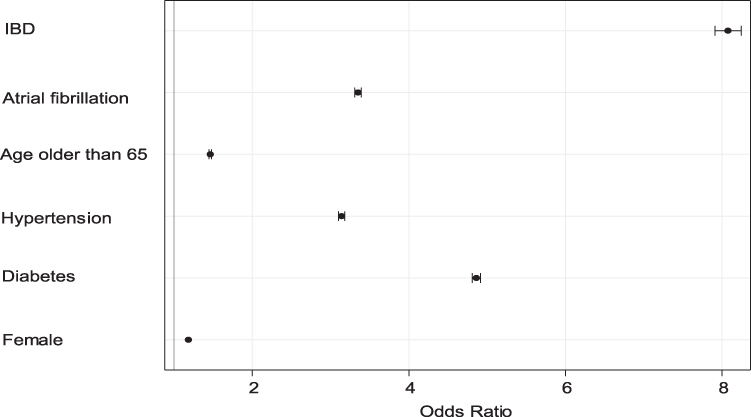 |
Figure 1 Forest plot showing adjusted odds ratio of having a cerebrovascular event. The odds ratio is represented by the circle. The whiskers represent 95% confidence intervals. Abbreviations: IBD, inflammatory bowel disease; CVA, cerebrovascular accidents. |
Discussion
In this large electronic medical record-based study of more than 52 million patients, we found that patients with IBD had a higher risk of CVA. This association persisted despite adjustments for multiple confounding traditional risk factors including hypertension, diabetes, female gender, advanced age and atrial fibrillation suggesting that IBD may be an independent risk factor for CVA.
The association between IBD and VTE is well established.9,13,14 However, the association between IBD and arterial thromboembolic disease has been more elusive and subject to debate. Five studies reported a total of 2,425 CVA events in 98,340 patients with IBD. On pooling the unadjusted odds ratio from each study, IBD was associated with a 21% percent risk of CVA (OR 1.21; 95% CI, 1.12–1.31). After adjusting for confounders, IBD conferred an 18% risk of CVA (OR 1.18; 95% CI, 1.09–1.27).6–8,15–18 Furthermore, Huang et al showed the risk of ischemic stroke to be 1.12 fold (95% CI, 1.02–1.223) higher in patients with IBD than without.9 In contrast, a large meta-analysis that included 17,487 IBD patients and 69,948 controls found that IBD patients did not have an increased risk of myocardial infarction or transient ischemic attacks when compared with controls.19 The findings from our study, the largest to date, help shed light on this controversy and support the adverse association of IBD and the higher risk of CVA.
Cardiovascular disease (CVD) which includes coronary heart disease (CHD), stroke and peripheral artery disease, is the leading cause of death in men and women.20,21 Several studies attempted to evaluate whether traditional CVD risk factors were more prevalent in IBD patients than the general population. Hypertension is a well-established risk factor for CVD including stroke. In our study, hypertension was more prevalent in patients with IBD than without IBD (40% vs 20%). This observation is contrary to findings from a study conducted by Yarur et al, who showed IBD patients to have significantly lower rates of hypertension.13 The contradicting results may be partially explained by the differences in the study population and in analysis methods.
The relationship between diabetes and IBD is well established. Jess et al demonstrated that IBD patients had an increased risk of diabetes (incidence ratio 1.54; 95% CI 1.49–1.60).19 In our study, the diagnosis of diabetes was also more prevalent in patients with IBD compared to those without IBD (20% vs 8%). One theory that may partially explain the mechanism behind this observation involves the development of insulin resistance from long-term steroid use. Stroke is a well-known macrovascular complication of diabetes. After adjusting for this factor in our multivariable model, CVA remained strongly associated with IBD. This finding further supports the existence of an independent pathogenic mechanism inherent to IBD.
There has been increasing emphasis on gender-differences in CVD. In both our adjusted and unadjusted models, the female gender was associated with a modest risk of CVA.22 This may be attributed to menopausal shifts in hormonal levels and the use of hormonal contraception. The incidence of stroke in a 65-year-old woman is reported to be 1 in 5 whereas a 65-year-old male’s risk of stroke is one in six.23 Likewise, women with IBD have a higher risk of CVD compared to their male counterparts.24–26 The use of oral contraception in females with IBD has been reported as high as 88%.24 Females with IBD were also more likely to have a higher baseline proinflammatory burden than males.25 This being said, Katsanos et al showed IBD to be associated with an increased risk of CVA independent of gender.26 Our study lends support to their work and suggests an independent association between IBD and the risk of CVA.
Age is a nonmodifiable risk factor for cerebrovascular disease. The risk doubles with each decade after the age of 45 years with 70% of all strokes occurring after the age of 65.27 Age-related microcirculatory changes are thought to contribute to cerebrovascular aging. A complex interaction between endothelial dysfunction, impaired cerebral autoregulation and neurovascular coupling leads to neuro-inflammation and microvascular injury and may explain why cerebrovascular accidents are more prevalent in the older population.28 In both our adjusted and unadjusted models, advanced age was shown to have a strong association with CVA.
Atrial fibrillation has long been recognized as a major risk factor for CVA. The association between atrial fibrillation and stroke is thought to be due to stasis of blood in the fibrillating left atrium leading to thrombus formation and embolization to the brain.29 The prevalence of atrial fibrillation in patients with IBD has been documented as high as 11.3% as compared to 0.9% in the general population.30–32 Our study also confirms a higher prevalence of atrial fibrillation in patients with IBD versus non-IBD patients (7% vs 3%). In both unadjusted and adjusted models, we observed a significant association between atrial fibrillation and the risk of stroke. The pathophysiology of atrial fibrillation in patients with IBD is not well understood but is thought to be related to the inflammatory effects of IBD. Higher rates of atrial fibrillation were observed in patients with active IBD flares (incidence rate ratio (IRR) 2.63 [2.23–3.06]) and persistent activity (IRR 2.06 [1.67–2.55]) compared to those in remission (IRR 0.97 [0.88–1.08]).30
An important strength of our study is that we used a large national database and reported data on over 52 million active adult subjects. We also provided comprehensive epidemiological information on the risk of stroke in patients with IBD based on established risk factors for both disease entities. Our results are therefore consistent with the growing body of evidence showing inflammation to be independently associated with a higher risk of strokes.
The prevalence of IBD in the United States is estimated to be between 1.3%.1,2 The reported prevalence of IBD in our study was 0.50%. As this is a retrospective study reliant on diagnosed SNOMED-CT codes, it is impossible to verify the accuracy of diagnoses and it is prone to coding errors. However, even with the lower numbers of IBD patients in the database, we were still able to observe a strong association between this inflammatory process and the higher risk of CVA.
Another significant limitation of our study is the validity of diagnosis of CVA. We were unable to differentiate between ischemic and non-ischemic CVA. Validation was also not possible as patient information in Explorys is de-identified. Another limitation in using this database is the inability to establish temporal relationships between IBD and CVA. Also, it is possible that some patients received care at institutions not part of the Explorys platform and thus we were not able to account for these patients.
IBD is a chronic inflammatory state with systemic manifestations. The pathophysiological contributions of IBD on CVD are currently not well understood. In our large US-based cohort study, we found IBD to be significantly associated with an increased risk of stroke independent of traditional risk factors. Experimental and clinical studies are warranted to improve our understanding of the pathogenesis of cerebrovascular accidents in patients with inflammatory bowel disease.
Informed Consent Statement
Informed consent was obtained from all participants.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
All authors have no conflict of interest and nothing to disclose.
References
1. Kristensen SL, Ahlehoff O, Lindhardsen J, et al. Disease activity in inflammatory bowel disease is associated with increased risk of myocardial infarction, stroke and cardiovascular death – A Danish nationwide cohort study. PLoS One. 2013;8(2):1–9. doi:10.1371/annotation/b4a49855-87b9-436a-a4bd-bc64b50a6c93
2. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–1695. doi:10.1056/NEJMra043430
3. Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147–157. doi:10.1111/j.1365-2796.2010.02310.x
4. Meune C, Touze E, Trinquart L, Allanore Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford). 2009;48(10):1309–1313. doi:10.1093/rheumatology/kep252
5. Svenungsson E, Jensen-Urstad K, Heimburger M, et al. Risk factors for cardiovascular disease in systemic lupus erythematosus. Circulation. 2001;104:1887–1893. doi:10.1161/hc4101.097518
6. Ha C, Magowan S, Accortt NA, Chen J, Stone CD. Risk of arterial thrombotic events in inflammatory bowel disease. Am J Gastroenterol. 2009;104(6):1445–1451. doi:10.1038/ajg.2009.81
7. Andersohn F, Waring M, Garbe E. Risk of ischemic stroke in patients with Crohn’s disease: a population based nested case-control study. Inflamm Bowel Dis. 2010;16(8):1387–1392. doi:10.1002/ibd.21187
8. Bernsetin CN, Wajda A, Blanchard JF. The incidence of arterial thromboembolic diseases in inflammatory bowel disease: a population-based study. Clin Gastroenterol Hepatol. 2008;6:41–45. doi:10.1016/j.cgh.2007.09.016
9. Huang W, Tseng C, Chen P, et al. Inflammatory bowel diseases increase future ischemic stroke risk: a Taiwanese population-based retrospective cohort study. Eur J Intern Med. 2014;25(6):561–565. doi:10.1016/j.ejim.2014.05.009
10. Keller JJ, Wang J, Hwang Y, et al. Increased risk of stroke among patients with Crohn’s disease: a population-based matched cohort study. Int J Colorectal Dis. 2015;30(5):645–653. doi:10.1007/s00384-015-2132-y
11. IBM explorys-accelerating insights from real-world evidence; 2019. Available from: http://www-01.ibm.com/common/ssi/cgi-bin/ssialias?htmlfid=HL912350U-SENhttp://www-01.ibm.com/common/ssi/cgi-bin/ssialias?htmlfid=HL912350U-SEN&.
12. Kaelber DC, Foster W, Gilder J, Glider J, Love TE, Jain AK. Patient characteristics associated with venous thromboembolic events: a cohort study using pooled electronic health record data. J Am Med Inform Assoc. 2012;19:965–972. doi:10.1136/amiajnl-2011-000782]
13. Yarur A, Deshpande A, Pechman D, Tamariz L, Abreu M, Sussman D. Inflammatory bowel disease is associated with an increased incidence of cardiovascular events. Am J Gastroenterol. 2011;106(4):741–747. doi:10.1038/ajg.2011.63
14. Zhang M, Sun K, Wu Y, Yang Y, Tso P, Wu Z. Interactions between intestinal microbiota and host immune response in inflammatory bowel disease. Front Immunol. 2017;8:942. doi:10.3389/fimmu.2017.00942
15. Zoller B, Li X, Sundquist J, Sundquist K. Risk of subsequent ischemic and hemorrhagic stroke in patients hospitalized for immune-mediated diseases: a nationwide follow-up study from Sweden. BMC Neurol. 2012;12:41. doi:10.1186/1471-2377-12-41
16. Singh S, Harkirat S, Loftus E, Pardi D. Risk of cerebrovascular accidents and ischemic heart disease in patients with inflammatory bowel disease: a systemic review and meta-analysis. Clin Gastroenterol Hepatol. 2014;12(3):382–393. doi:10.1016/j.cgh.2013.08.023
17. Meschia JF, Worral BB, Rich SS. Genetic susceptibility to ischemic stroke. Nat Rev Neurol. 2011;7:369–378. doi:10.1038/nrneurol.2011.80
18. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systemic analysis of population health data. Lancet. 2006;367(9524):1747. doi:10.1016/S0140-6736(06)68770-9
19. Jess T, Jensen BW, Andersson M, Villumsen M, Allin KH. Inflammatory bowel disease increases risk of type 2 diabetes in a nationwide cohort study. Clin Gastroenterol Hepatol. 2020;18(4):881–888.e1. doi:10.1016/j.cgh.2019.07.052
20. Seshardi S, Beiser AS, Kelly-Hayes M, et al. The lifetime risk of stroke. Estimates from the Framingham study. Stroke. 2006;37:345–350. doi:10.1161/01.STR.0000199613.38911.b2
21. Halling ML, Kjeldsen J, Knudsen T, Nielsen J, Hansen LK. Patients with inflammatory bowel disease have increased risk of autoimmune and inflammatory diseases. World J Gastroenterol. 2017;23:6137–6146. doi:10.3748/wjg.v23.i33.6137
22. Aniwan S, Pardi DS, Tremaine WJ, Loftus EV. Increased risk of acute myocardial infarction and heart failure in patients with inflammatory bowel disease. Clin Gstroenterol Hepatol. 2018;16:1607–1615. doi:10.1016/j.cgh.2018.04.031
23. Kang EA, Han K, Chun J, et al. Increased risk of diabetes in inflammatory bowel disease patients: a nationwide population-based study in Korea. J Clin Med. 2019;8(3):E343. doi:10.3390/jcm8030343
24. Gawron LM, Goldberger A, Gawron AJ, Hammond C, Keefer L. The impact of hormonal contraception on disease-related cyclical symptoms in women with inflammatory bowel diseases. Inflamm Bowel Dis. 2014;20:1729–1733. doi:10.1097/MIB.0000000000000134
25. Kappelman MD, Galanko JA, Porter CQ, Sandler RS. Association of paediatric inflammatory bowel disease with other immune-mediated diseases. Arch Dis Child. 2011;96:1042–1046. doi:10.1136/archdischild-2011-300633
26. Katsanos AH, Kosmidou M, Giannopoulos S, et al. Cerebral arterial infarction in inflammatory bowel diseases. Eur J Internal Med. 2014;25(1):37–44. doi:10.1016/j.ejim.2013.08.702
27. Kelly-Hayes M. Influence of age and health behaviors on stroke risk: lessons from longitudinal studies. J Am Geriatr Soc. 2010;58 Suppl2(Suppl 2):S325–S328. doi:10.1111/j.1532-5415.2010.02915.x
28. Yousufuffin M, Young N. Aging and ischemic stroke. Aging (Albany NY). 2019;11(9):2542–2544. doi:10.18632/aging.101931
29. Boehme A, Esenwa C, Elkind M. Stroke risk factors, genetics, and prevention. Circ Res. 2017;120(3):472–495. doi:10.1161/CIRCRESAHA.116.308398
30. Kristensen SL, Lindhardsen J, Ahlehoff O, et al. Increased risk of atrial fibrillation and stroke during active stages of inflammatory bowel disease: a nationwide study. Europace. 2014;16:477–484. doi:10.1093/europace/eut312
31. Dogan Y, Soylu A, Eren GA, et al. Evaluation of QT and P wave dispersion and mean platelet volume among inflammatory bowel disease patients. Int J Med Sci. 2011;8:540–546. doi:10.7150/ijms.8.540
32. Pattanshetty DJ, Anna K, Gajulapalli RD, Sappati-Biyyani RR. Inflammatory bowel “Cardiac” disease: point prevalence of atrial fibrillation in inflammatory bowel disease population. Saudi J Gastroenterol. 2015;21:325–329. doi:10.4103/1319-3767.166208
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.