")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
The relationship between single nucleotide polymorphisms and dental implant loss: a scoping review
Authors Zhang F , Finkelstein J
Received 3 March 2019
Accepted for publication 21 May 2019
Published 31 May 2019 Volume 2019:11 Pages 131—141
DOI https://doi.org/10.2147/CCIDE.S207445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Frederick Zhang,1 Joseph Finkelstein2
1College of Dental Medicine, Columbia University, New York, NY, USA; 2Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Objectives: The purpose of this review was to evaluate the relationship between genetic polymorphisms and dental implant loss.
Materials and methods: All case-control studies examining single nucleotide polymorphisms (SNPs) and dental implant failure were considered. A Boolean search was conducted on PubMed and Scopus to find eligible studies.
Results: The initial search produced 78 results. Twenty-one studies were considered for inclusion after review and 16 were included in the final review. Twenty-two different polymorphisms were analyzed and statistically significant correlation was found for IL-4, IL-1A, IL-1B, MMP-8, and MMP-1 polymorphisms for dental implant failure.
Discussion: A limited number of comprehensive studies have been done in this field. Additional studies with larger sample sizes and different ethnic backgrounds need to be done to see if the results can be reproduced. Of the polymorphisms studied, the IL-4 (+33), MMP-8 (−799), MMP-1 (−519), and MMP-1 (−1607) polymorphisms show the greatest association with dental implant loss.
Keywords: dental implants, single nucleotide polymorphisms, genetic risk factors, scoping review
Introduction
Dental implants have become a widespread and effective method for treatment of fully and partially edentulous patients. Nonetheless, implant failure still occurs. Global implant failure rate has been reported to be between 1.9% and 3.6%.1–3 Implant failures can be divided into two types based on timing: early and late.4 Early failure occurs before abutment connection and is caused by failed osseointegration.4 This can be the result of failure in the bone-healing process, where formation of scar tissue or inflammatory cell proliferation prevents the implant from adhering tightly to the bone.5 Late failure occurs after osseointegration has occurred and the implant is subjected to occlusal loading.5 Alveolar bone loss has been shown to be a primary cause of late implant failure.4
Peri-implantitis,40 occlusal overloading,41 systemic comorbid conditions,42 medication regimen,43 patient unhealthy behaviors,44 and implant location45 and characteristics46 are among risk factors associated with implant failure.47 Dental implants have been suggested to exhibit cluster behavior, where a small proportion of patients are responsible for the majority of implant failures.6,52 In one study, 58.6% of the overall implant failures occurred in just 32.1% of the patients.6 This suggests that these patients may have endogenous characteristics which predispose them to implant failure. Because of the high financial burden of dental implant treatment, it is important to understand the cause of these cluster failure patients in order to develop screening techniques for implant viability. A variety of primary predictors for implant failure have already been identified, such as advanced age, diabetes, smoking, and implant location.7 However, the relationship between genetic factors and implant failure susceptibility is poorly understood.
Previously, certain candidate genes have been identified and investigated for their relationship to periodontal disease.38 Polymorphisms involved in host inflammatory response such as inflammatory cytokines have been extensively investigated for their potential role in susceptibility to aggressive forms of periodontitis.39 Other gene polymorphisms, such as Vitamin D receptor genes involved in regulating bone mineral density or matrix metalloproteinase genes involved in connective tissue destruction, have also been implicated as risk factors for periodontal disease.8 The etiology of dental implant failure shows many parallels with that of periodontal disease due to the involvement of soft tissue damage, infection, and bone loss.9 For this reason, many studies examining the relationship between genetic polymorphisms and implant failure have examined the same candidate genes as for periodontal disease. The purpose of this scoping review was to 1) conduct a scoping review of articles examining the relationship between specific gene polymorphisms and dental implant failure and 2) discuss possible biological mechanisms which could explain these relationships.
Methods
The purpose of a scoping review has been defined as a method to quickly map out the available literature regarding an area of research. From here, gaps in the available literature can be identified so that further studies can be pursued.10 The scoping review methodology as defined by Arksey and O’Malley10 has five major steps:
- Identify a research question
- Identify relevant studies
- Evaluate and select studies to be included
- Chart the data
- Collect, summarize, and report the results
Research question
The primary goal of this scoping review was to identify single nucleotide polymorphisms (SNPs) which could potentially be associated with dental implant failure so that they could be studied further. Based on this goal, the research question developed was “Which gene polymorphisms show an association with dental implant failure?”
Search strategy
We conducted an electronic literature search on the PubMed and Scopus database in order to identify potential papers to be included in the study. The studies included were available in English and published from the year 2000 to the present day. We used the following Boolean search term: (dental implant failure) AND (“polymorphism” OR “genotype” OR “haplotype”). This search yielded 78 potential papers to be included in the study.
Study selection
The following inclusion criteria were established during the process of reviewing the articles:
- The study had to explicitly study dental implant failure resulting in implant loss, including both early and late failures. Studies which included other conditions such as peri-implantitis were excluded.
- Studies had to be done on human subjects.
- The study had to specifically target one or more SNPs.
- Any follow-up period was acceptable.
- Only case-control studies were considered in order to maintain homogeneity of studies analyzed.
After defining these criteria, the title and abstract of each paper were reviewed to determine eligibility. This review resulted in 21 papers which were relevant to the research question and satisfied the exclusion criteria based on a preliminary review. Each of these papers were then read in detail and reviewed more thoroughly, resulting in 16 papers to be included in the final study. The overall screening process is detailed in Figure 1.
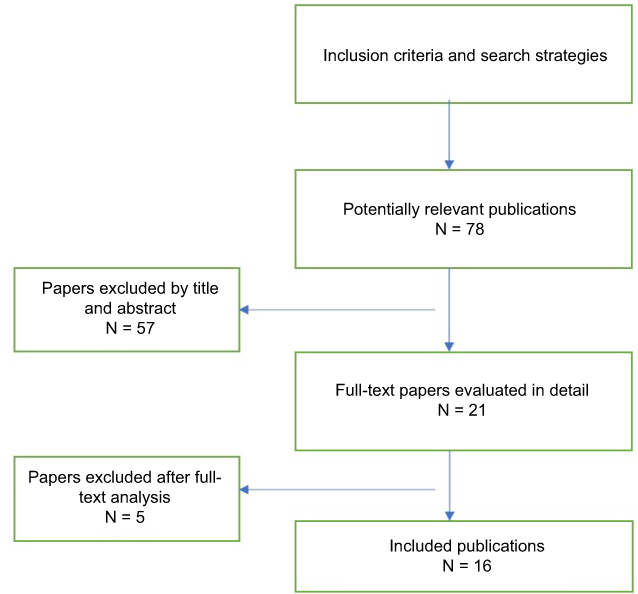 | Figure 1 Study search and exclusion process. |
Data extraction
The first author and date of publication were recorded for each of the included studies. Then, we determined whether the study looked at early implant failures only or all implant failures. Finally, we examined the exact polymorphism which was the subject of study, the characteristics of the patient samples used, the minimum duration that healthy controls needed to have their implants to be included in the study, and the results regarding the association of the polymorphism with implant failures. The specific characteristics for each study can be found in Table 1. We also identified the specific methodology used in the studies, the sample size of both patients and total number of implants, as well as any other factors which could contribute to implant failure identified in the study. These characteristics can be found for each of these studies in Table 2. For the “Statistical Findings for Study SNP” column of Table 2, all included odds ratios or other findings were specified as statistically significant within their respective articles.
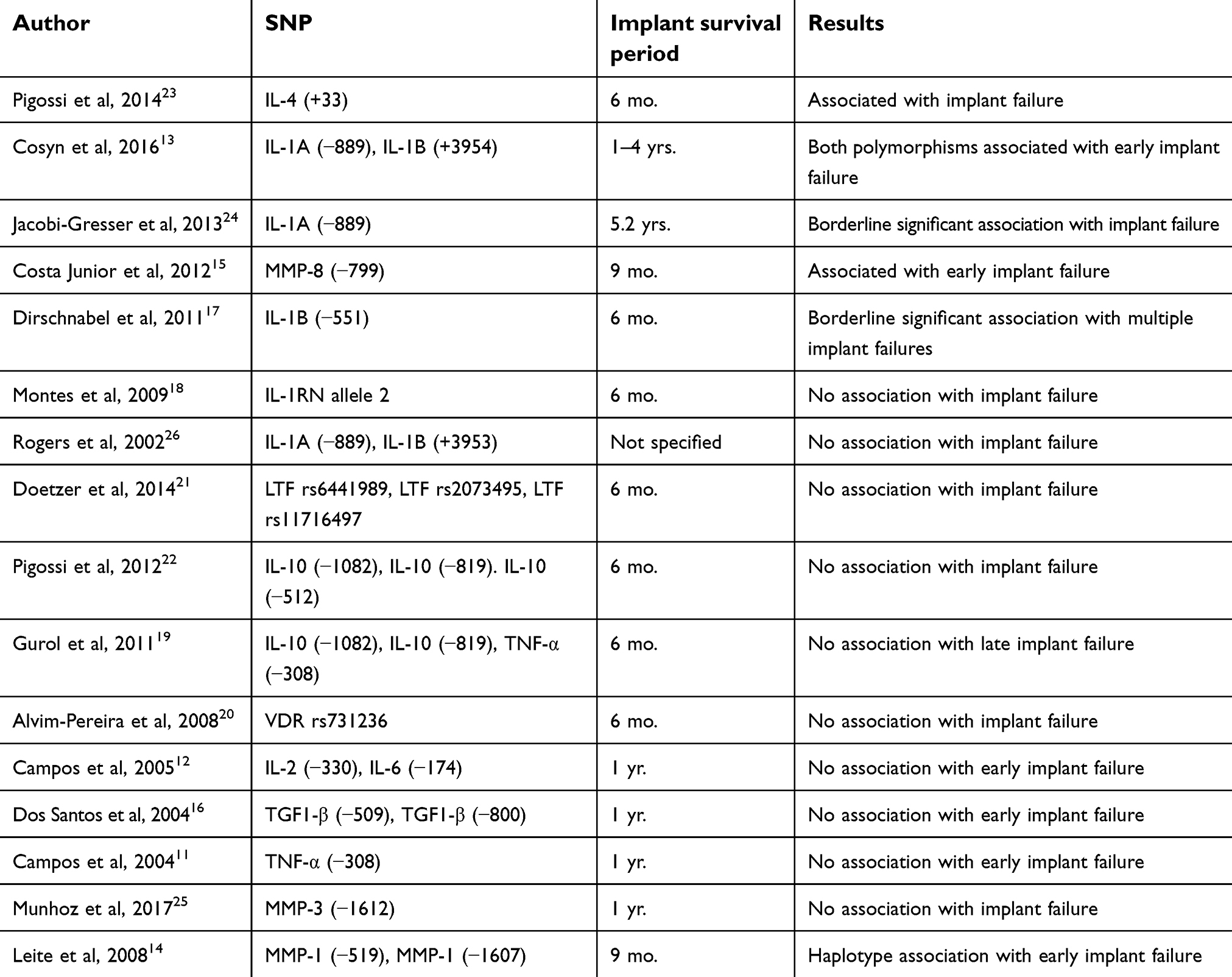 | Table 1 Summary of SNPs, follow-up period, and association results of the studies included |
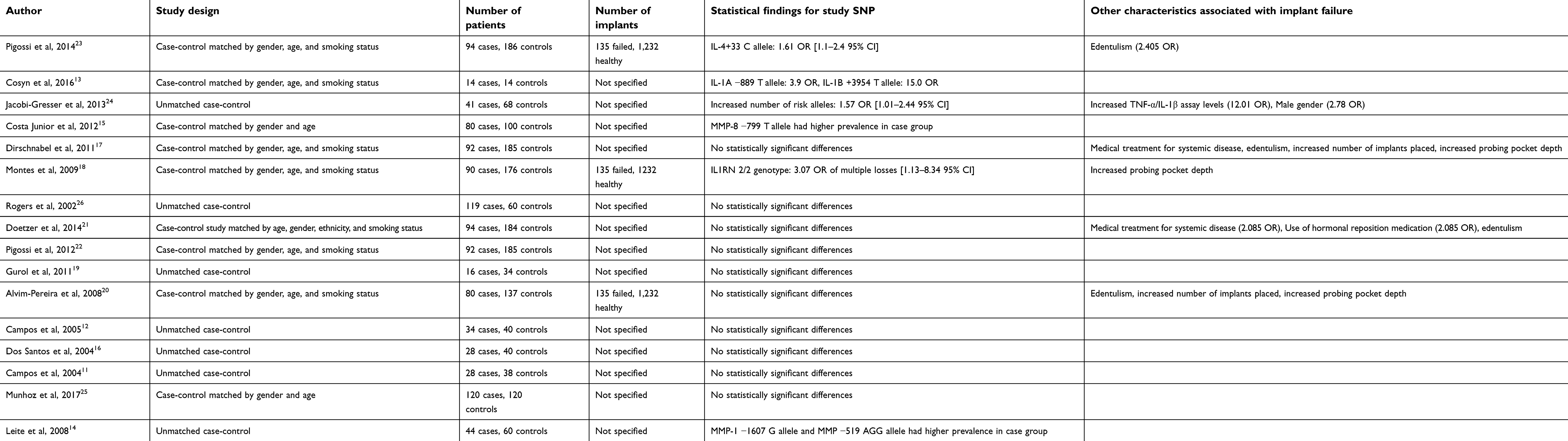 | Table 2 Summary of study characteristics and significant confounders in the studies included |
Results
Characteristics of the included studies
The included studies examined different categories of implant failures. Six of the papers studied early implant failure only.11–16 Two papers studied patients with both early and late implant failures but only had statistically significant findings with patients who experienced multiple implant failures.17,18 Only one paper excluded early implant failures.18 All of the remaining papers studied all types of implant failure.
All of the selected papers were case-control studies; however, they varied in their criteria for selection of the controls. Two of the papers selected patients whose implants had survived at least 9 months.15,16 Seven of the papers selected patients whose implants had survived at least 6 months.16–22 Rogers et al did not specify the minimum implant survival duration. All of the remaining papers chose patients whose implants survived 1 year or longer.11–13,24,25 These studies also varied in how they designed their case-control study. Six studies were unmatched case-control studies. The rest were matched.
Many of the papers used the same or similar patient pools. In particular, six studies drew their study sample from the exact same pool of 3,758 patient records from the Latin-American Dental Research Institute (ILAPEO) of Curitiba.17,18,20–23 Six of the studies used patient pools which included patients treated at University of Campinas, Piracicaba, Sao Paulo, Brazil.11,12,14–16,25 The remaining studies used patient pools from Belgium, Germany, Australia, and Turkey.13,19,24,26
Nine of the papers studied interleukin polymorphisms.12,13,17–19,22–24,26 Specifically, polymorphisms of IL-1A, IL-1B, IL-1RN, IL-2, IL-4, IL-6, and IL-10 were studied. Three of the papers studied matrix metalloproteinases, specifically MMP-1, MMP-3, and MMP-8.12,13,23 The remaining polymorphisms studied were TNF-α, TGF1-β, lactoferrin, and vitamin D receptors.11,16,19–21
Only four of the polymorphisms were the subject of more than one of the examined studies. The IL-1A (−889) polymorphism was the subject of three studies.13,24,26 The IL-10 (−1082), IL-10 (−819), and the TNF-α (−308) polymorphisms were the subject of two studies each.11,19,22
Effects of SNPs on implant failure
The general characteristics and results of the studies included are displayed in Table 1. Information regarding the sample size, methodology, and statistical findings of each study can be found in Table 2. The most highly studied polymorphism was the IL-1A (−889) C to T polymorphism. Cosyn et al found a statistically significant association between the T allele and early implant failure in a Belgian poulation, with a 3.9 OR.13 However, this study had a limited sample size, with only 14 cases and 14 controls. The other two studies examined both early and late failures and failed to find a statistically significant result, although Jacobi-Gresser et al found a borderline significant association (p=0.077).24 The IL-1A interleukin has been previously linked to peri-implantitis, which is one of the most common causes of late implant failure.28 The only study which showed a statistically significant association between the IL-1A polymorphism and implant failure, however, was the study which examined only early implant failures. This discrepancy in the findings could either be an indication of lack of statistical power in the first study, or an indication that the IL-1A interleukin plays a role in osseointegration which is not yet understood.
The IL-1B interleukin was the subject of four different studies. IL-1B has been demonstrated to stimulate a wide variety of cells which are involved in inflammatory responses, such as neutrophils and fibroblasts.27 Cosyn et al examined the IL-1B (+3954) polymorphism and found an OR of 15.0 for patients who had the T allele and early implant failure.13 As stated above, however, this study suffers from a limited sample size. Of the 14 controls used in the study, only one T allele was present within the entire sample, so it is unclear whether these results can be extrapolated to a larger population sample. Montes et al also looked at the IL-1b (+3954) polymorphism, however they used a Brazilian population and did not distinguish between early and late implant failures.18 Their study found no statistically significant association between the T allele and implant failure while using a much larger sample size of 176 controls and 90 cases.18 Rogers et al did not distinguish between early and late implant failures and examined the IL-1B (+3953) polymorphism in an Australian population.26 They found no significant difference in prevalence of allele 2 between individuals with failed implants and individuals with successful implants. Dirschnabel et al examined the IL-1B (−551) polymorphism within a Brazilian population and found a borderline significant difference (p=0.083) in the prevalence of the TT genotype between patients with zero to one implant failures and patients with multiple implant failures.17 These findings could either indicate that IL-1B polymorphisms have some specific effect on initial osseointegration but not affect later stages of implant survival, or that the first study lacked enough statistical power to generate a reproducible result. In addition, Cosyn et al and Montes et al matched their cases and controls by smoking status, whereas Rogers et al only matched by age and gender. Tobacco use is a major confounding factor of implant failure, and further studies could benefit from ensuring that cases and controls are always matched by smoking status.7
Two papers studied IL-10 polymorphisms. IL-10 is an anti-inflammatory cytokine which inhibits the production of proinflammatory cytokines, making it an important mediator of the immunosuppressive response.29 Polymorphisms which affect levels of IL-10 transcription could therefore lead to increased inflammation, resulting in implant failure. Pigossi et al examined the IL-10 (−1082), (−819), and (−592) polymorphisms within a Brazilian population and found no statistically significant associations between any of the polymorphisms and dental implant failure.22 Gurol et al also examined the IL-10 (−1082) and (−819) polymorphisms but within a Turkish population and also found no statistically significant associations between the polymorphisms and implant failure.19
Two papers studied the TNF-α (−308) polymorphisms. TNF-α is a proinflammatory cytokine produced by macrophages and could influence implant failure through similar mechanisms as the interleukins discussed above.30 Gurol et al examined the TNF-α (−308) polymorphism in a Turkish population and found no statistically significant association.19 Campos et al looked at the same polymorphism within a Brazilian population and also found no statistically significant association.11 This study excluded smokers from their study sample and noted that this exclusion created a fairly small sample size of 38 controls and 28 cases. The first study contained a fairly small sample size of 23 controls and 16 cases as well.
All of the remaining polymorphisms were only studied once each within the selected papers. Four other interleukin polymorphisms were studied. Of these, two produced statistically significant results. Pigossi et al examined the IL-4 (+33) polymorphism within a Brazilian population and found that individuals carrying the C allele had a 1.61 OR of dental implant loss.23 IL-4 is a T-cell secreted interleukin that inhibits macrophage secretion of proinflammatory cytokines and PGE2, and insufficient IL-4 has been implicated to be a potential trigger of periodontitis.27 Montes et al examined the presence of intron 2 in the IL-1RN gene compared to the presence of any of the other introns.18 Although no statistically significant association was found between the presence of intron 2 and overall dental implant failure, patients with the 2/2 genotype had a 3.07 OR of multiple implant failures when compared to patients with just one implant failure.18 This could indicate a role for IL-1RN in cluster implant failures. IL-1RN is involved in production of the IL-1ra cytokine, which has anti-inflammatory function.31 Both of these studies used patients from the same patient pool, so it could prove beneficial to test these polymorphisms on different patient pools to further examine the strength of association. Campos et al examined the IL-2 (−330) and IL-6 (−174) polymorphisms in a Brazilian population and found no significant association of either polymorphism with implant failure.12 IL-2 is secreted by activated T cells and induces proliferation in a variety of different lymphocytes.31 IL-6 has been shown to have pleiotropic functions which include stimulation of osteoclast formation, as well as induction of acute inflammatory factors.31
The other major family of genes studied were the matrix metalloproteinases. Three of the articles examined MMP polymorphisms, with two of these articles finding statistically significant results. After tissue injury, matrix metalloproteinases have been found to have a variety of functions in the wound healing process.32 MMP-1 cleaves type 1 collagen at wound sites in order to promote integrin binding to keratinocytes.32 MMP-8 plays a major role in neutrophil recruitment.32 Costa Jr et al examined the MMP-8 (−799) polymorphism on a Brazilian population and found that 76.25% patients with early implant failure carried the T allele compared to only 60% of the control group.15 Leite et al examined the MMP-1 (−519) and (−1607) polymorphisms and found that 38.63% of patients with early implant failures carried the GG allele at the (−1607) position compared to 25% in the control group.14 They also found that 28.9% of the patients with early implant failure carried the (−519)/(−1607) G/GG haplotype compared to only 12.5% in the control group. Finally, Munhoz et al examined the MMP-3 (−1612) polymorphism in a Brazilian population and found no significant association with early implant failure.25 However, the authors note that the MMP-3 and MMP-1 are located in close proximity on chromosome 11, and further studies which examine the polymorphism in haplotype combination could prove beneficial. All three of these studies examined only non-smoking patients and included systemic diseases such as osteoporosis and HIV, which eliminates several major confounding factors. It must be noted that all three of these studies examined patients selected from the University of Campinas and only examined early implant failures. Additional studies which consider both early and late implant failures could help clarify the roles these polymorphisms play in affecting not only initial osseointegration, but also overall implant survival.
The three remaining articles examined miscellaneous polymorphisms not related to genes in other studies. Alvim-Pereira et al examined the Vitamin D receptor rs731236 in a Brazilian population and found no statistically significant associations.20 Doetzer et al examined three different Lactotransferrin polymorphisms (rs6441989, rs2073495, rs11716497) and found no clinically significant associations.21 However, this study did not have exclusion criteria of systemic diseases for its patient sample, which could present as confounding factors for the results. Finally, dos Santos et al examined two TGF-1β polymorphisms [(−509), −800)] and found no statistically significant associations while looking at early implant failures only.16
Other factors associated with implant failure
Several studies included in this review also examined other factors associated with dental implant failure. With regards to dental risk factors, four studies found a significant association between edentulism and implant failure.17,20,21,23 Associations were also found between number of implants placed and implant failure, as well as increased pocket probing depth and implant failure.17,18,20 Certain systemic factors were found to be associated with implant failure as well. In the study conducted by Jacobi-Gresser et al, although they failed to find a statistically significant association with individual IL-1B or TNF-α polymorphisms, they did find a significant association between increased TNF-α/IL-1B serum assay levels and dental implant failure (OR=12.01).24 Two studies which included medically compromised patients found a significant association between medical treatment for systemic disease and implant failure.17,21 One of these studies also found a significant association with hormonal replacement therapy (OR=2.085).21 Finally, one study found that males were more susceptible to implant failure than females (OR=2.78).24
Discussion
Our review identified 16 studies in total which analyzed the association between SNPs and dental implant failure. Overall, 22 different polymorphisms were analyzed, and statistically significant associations with implant failures were found for six of them, specifically the IL-4, IL-1A, IL-1B, MMP-8, and MMP-1 polymorphisms. The study which found significant results for the IL-1A and IL-1B polymorphisms suffered from a low sample size, so it is unclear if those results could be reproduced. In addition, two earlier studies examined the same IL-1A (−889) polymorphism and found no significant results. Based on these findings, the IL-4 (+33), MMP-8 (−799), MMP-1 (−519), and MMP-1 (−1617) show the highest association with dental implant failure. With the exception of the IL-4 (+33) polymorphism, all of these polymorphisms were the subject of studies which examined early failures only. This is most likely due to the role these genes play in the inflammatory and wound-healing process, which is one of the main factors affecting early implant failure.20,32
There are some limitations to the studies that we have included in this review. First, not every study included differentiated between late and early implant failure. The mechanism of failure in early implant failure versus late implant failure differs, as early implant failure represents a failure in the osseointegration process, whereas in late implant failure osseointegration has already occurred.4,5 Thus, it may be necessary to treat these two types of implant failure as two distinct events when attempting to characterize risk factors. Second, the survival period to be considered an implant “success” varied widely between the selected studies. For some studies which examined all implant failures, the survival period was as short as 6 months. Future studies could benefit from expanding the required survival period to be considered an implant “success” in order to capture a greater range of late implant failure cases. The survival period also varied even between studies which only examined early implant failure.
According to the inclusion criteria for our scoping review, only original research articles with case-control design were included. Case-control studies were chosen as one of the criteria to ensure sufficient homogeneity of the resulting sample and because case-control design has been the most widely used approach in genetic association studies particularly concerning rare events such as implant failure.49 Case-control studies have been successfully used in identifying risk factors for periodontal disease,50 peri-implantitis,51 implant failure,52 and association of health care utilization with genetic polymorphisms.53 In case-control studies, subjects are grouped based on the outcome such as implant failure or success allowing comparison of exposure prevalence such as particular SNP between the groups. Unlike case-control studies, cohort studies group subjects based on the absence or presence of a particular exposure such as SNP to compare outcome frequencies in the study groups.54 Though case-control design is usually preferred for studies of rare conditions, cohort studies may also be used for this purpose. Though cohort studies were not included in this review based on the scoping review inclusion criteria, there is a number of valuable reports related to the genetic factors of dental implant failure. For example, Vaz et al demonstrated that particular alleles of IL1A and IL1B genes were significantly associated with dental implant failure.55 Another limitation of our study was that it was focused only on single dental implant survival. Articles focused on implants retaining overdentures such as the study by Fernandez et al.56 were not included to ensure sample homogeneity and due to a different role that the implant overload factors may play in these cases.
Other studies have also performed reviews on the available literature to find genetic associations with implant failure. In 2011, Dereka et al published a review that examined seven different studies.33 Their review found that no association has been demonstrated between TNF-α, IL-1, IL-2, IL-6, or TGF-β1 polymorphisms and dental implant complications. Our review differs from theirs in several ways. First, their review examined all biologic complications defined as “the biological processes that affect the soft and hard tissues supporting the implant.” This broad definition resulted in inclusion of genetic polymorphisms studies which examined peri-implantitis or peri-implant bone loss in addition to implant failure. Our review only examined those studies which looked at the association between SNPs and actual implant loss because peri-implantitis has been found to occur in anywhere from 28% to 56% of dental implants placed, so it represents an outcome which is both more common and less disastrous than implant failure.33 Second, their exclusion and inclusion criteria differed from ours. They only included studies were the implant did not develop any complications for a minimum of 1 year after loading, whereas our review included multiple studies with a shorter minimum implant survival period. In addition, they excluded studies which examined medically compromised patients, whereas we included a few studies which included these patients in their study sample. Finally, they only included studies which examined both early and late implant loss, whereas we examined several studies which only included early implant failure. We included these studies in order to find a broader range of candidate genes which could play a role in implant failure. A 2018 review also examined the association between certain SNPs and dental implant failure in the literature.35 Like the above review, this study also excluded articles which included patients with systemic disease from their review. We felt that these studies were important to include because implant failure and other conditions of the periodontium have a multifactorial etiology with possible ties to systemic disease.36 The effect of gene polymorphisms could have interactions with these systemic conditions in implant failure, so we wanted to investigate papers which included these populations. Another review published in 2018 by del Valle et al also included a broad spectrum of articles investigating association between genetic polymorphisms and risk for biological complications in implantology,48 similar to the report by Dereka et al.33 A review by Alvim-Pereira et al provided a broad examination of the literature available regarding gene polymorphisms and implant failure but did not specify inclusion and exclusion criteria or search terms.37 The resulting conclusion of these reviews that new investigations are necessary to overcome limitations of previous studies was in concordance with the conclusion of our scoping review. Our article represents the first review in this field which followed the methodology of scoping review.10 Following the scoping review requirements, strict inclusion and exclusion criteria were chosen to ensure quality control of the studies included in our review.
Dental implant placement is a complex surgical procedure and thus the etiology of its failure is often multifactorial. Although our review chooses to focus on possible genetic contributions, many of the articles included in this review identified other factors which could contribute to implant failure susceptibility, such as edentulism and smoking habits. Other factors which have been investigated for their relationship to dental implant outcomes include the implant position (anterior compared to posterior) and material.34 Continued investigation into all factors which could affect dental implant outcomes is needed in order to further improve the reliability and predictability of this treatment. Our findings indicate that very few studies have been made which examine the association between SNPs and dental implant loss. Of the few polymorphisms which have been examined, even fewer have been the subject of more than one study. In addition, of the few studies available there is a great deal of homogeneity with regards to the study samples used. Many of the studies included also have very short minimum implant survival periods ( <1 year), which could be affecting the late implant failure rate. Further studies should be done on these polymorphisms with different sample populations in order to see if the results can be reproduced.
Conclusion
Very few comprehensive studies have been done to identify SNP associated with dental implant failure. Existing studies are limited by a small sample size, choice of confounders, and population background. Additional studies with larger sample sizes and different ethnic backgrounds need to be done to see if the results can be reproduced. Of the polymorphisms studied, the IL-4 (+33), MMP-8 (−799), MMP-1 (−519), and MMP-1 (−1607) polymorphisms show the greatest association with dental implant loss.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alsaadi G, Quirynen M, Michiles K, Teughels W, Komárek A, Steenberghe DV. Impact of local and systemic factors on the incidence of failures up to abutment connection with modified surface oral implants. J Clinl Periodontol. 2008;35(1):51–57.
2. Alsaadi G, Quirynen M, Komárek A, Steenberghe DV. Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J Clin Periodontol. 2007;34(7):610–617. doi:10.1111/j.1600-051X.2007.01077.x
3. Alsaadi G, Quirynen M, Komárek A, Steenberghe DV. Impact of local and systemic factors on the incidence of late oral implant loss. Clin Oral Implants Res. 2008;19(7):670–676. doi:10.1111/j.1600-0501.2008.01534.x
4. Manor Y, Oubaid S, Mardinger O, Chaushu G, Nissan J. Characteristics of early versus late implant failure: a retrospective study. J Oral Maxillofac Surg. 2009;67(12):2649–2652. doi:10.1016/j.joms.2009.07.050
5. Esposito M, Thomsen P, Ericson LE, Sennerby L, Lekholm U. Histopathologic observations on late oral implant failures. Clin Implant Dent Relat Res. 2000;2(1):18–32.
6. Schwartz-Arad D, Laviv A, Levin L. Failure causes, timing, and cluster behavior: an 8-year study of dental implants. Implant Dent. 2008;17(2):200–207. doi:10.1097/ID.0b013e3181777906
7. Moy PK, Medina D, Shetty V, Aghaloo TL. Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants. 2005;20:569–577.
8. Tarannum F, Faizuddin M. Effect of gene polymorphisms on periodontal diseases. Indian J of Hum Genet. 2012;18(1):9–19. doi:10.4103/0971-6866.96638
9. Sakka S, Coulthard P. Implant failure: etiology and complications. Med Oral Patol Oral Cir Bucal. 2011;16(1):42–44. doi:10.4317/medoral.16.e42
10. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
11. Campos MIG, Dos Santos MCLG, Trevilatto PC, Scarel-Caminaga RM, Bezerra FJB, Line SRP. Early failure of dental implants and TNF-α (G-308A) gene polymorphism. Implant Dent. 2004;13(1):95–101.
12. Campos MIG, Dos Santos MCLG, Trevilatto PC, Scarel-Caminaga RM, Bezerra FJ, Line SRP. Interleukin-2 and interleukin-6 gene promoter polymorphisms, and early failure of dental implants. Implant Dent. 2005;14(4):391–396.
13. Cosyn J, Christiaens V, Koningsveld V, et al. An exploratory case-control study on the impact of IL-1 gene polymorphisms on early implant failure. Clin Implant Dent Relat Res. 2014;18(2):234–240. doi:10.1111/cid.12237
14. Leite MFF, Santos MCLG, De Souza AP, Line SRP. Osseointegrated implant failure associated with MMP-1 promotor polymorphisms (−1607 and −519). Int J Oral Maxillofac Implants. 2008;23(4):653–658.
15. Costa-Junior FR, Alvim-Pereira CC, Alvim-Pereira F, Trevilatto PC, Souza APD, Santos MCLG. Influence of MMP-8 promoter polymorphism in early osseointegrated implant failure. Clin Oral Investig. 2012;17(1):311–316. doi:10.1007/s00784-012-0699-z
16. Dos Santos MCLG, Campos MIG, Souza AP, Scarel-Caminaga RM, Mazzonetto R, Line SRP. Analysis of the transforming growth factor- β1 gene promoter polymorphisms in early osseointegrated implant failure. Implant Dent. 2004;13(3):262–269.
17. Dirschnabel AJ, Alvim-Pereira F, Alvim-Pereira CC, Bernardino JF, Rosa EAR, Trevilatto PC. Analysis of the association of IL1B (C-511T) polymorphism with dental implant loss and the clusterization phenomenon. Clin Oral Implants Res. 2011;22(11):1235–1241. doi:10.1111/j.1600-0501.2010.02080.x
18. Montes CC, Alvim-Pereira F, Castilhos BBD, Sakurai MLL, Olandoski M, Trevilatto PC. Analysis of the association of IL1B(C 3954T) and IL1RN(intron 2) polymorphisms with dental implant loss in a Brazilian population. Clin Oral Implants Res. 2009;20(2):208–217. doi:10.1111/j.1600-0501.2008.01629.x
19. Gurol C, Kazazoglu E, Dabakoglu B, Korachi M. A comparative study of the role of cytokine polymorphisms interleukin-10 and tumor necrosis factor alpha in susceptibility to implant failure and chronic periodontitis. Int J Oral Maxillofac Implants. 2011;26(5):955–960.
20. Alvim-Pereira F, Montes CC, Thomé G, Olandoski M, Trevilatto PC. Analysis of association of clinical aspects and vitamin D receptor gene polymorphism with dental implant loss. Clin Oral Implants Res. 2008;19(8):786–795. doi:10.1111/j.1600-0501.2008.01532.x
21. Doetzer AD, Schlipf N, Alvim-Pereira F, et al. Lactotransferrin gene (LTF) polymorphisms and dental implant loss: a case-control association study. Clin Implant Dent Related Res. 2014;17(Suppl. 2):550–561. doi:10.1111/cid.12284
22. Pigossi SC, Alvim-Pereira F, Montes CC, et al. Genetic association study between interleukin 10 gene and dental implant loss. Arch Oral Biol. 2012;57(9):1256–1263. doi:10.1016/j.archoralbio.2012.02.020
23. Pigossi SC, Alvim-Pereira F, Alvim-Pereira CCK, Trevilatto PC, Scarel-Caminaga RM. Association of interleukin 4 gene polymorphisms with dental implant loss. Implant Dent. 2014;23(6):723–731. doi:10.1097/ID.0000000000000157
24. Jacobi-Gresser E, Huesker K, Schütt S. Genetic and immunological markers predict titanium implant failure: a retrospective study. Int J Oral Maxillofac Surg. 2013;42(4):537–543. doi:10.1016/j.ijom.2012.07.018
25. Munhoz FBDA, Nogara PRB, Junior FRDC, Branco FP, Dos Santos MCLG. Analysis of MMP-3 polymorphism in osseointegrated implant failure. Braz J Oral Sci. 2017;15(4):304. doi:10.20396/bjos.v15i4.8650045
26. Rogers MA, Figliomeni L, Baluchova K, et al. Do interleukin-1 polymorphisms predict the development of periodontitis or the success of dental implants? J Periodontal Res. 2002;37(1):37–41.
27. Kamma JJ, Giannopoulou C, Vasdekis VGS, Mombelli A. Cytokine profile in gingival crevicular fluid of aggressive periodontitis: influence of smoking and stress. J Clin Periodontol. 2004;31(10):894–902. doi:10.1111/j.1600-051X.2004.00585.x
28. Hamdy AAE-M-M, Ebrahem -MAE-M. The effect of interleukin-1 allele 2 genotype (IL-1a (−889) and IL-1b (+3954)) on the individuals susceptibility to peri-implantitis: case-control study. J Oral Implantol. 2011;37(3):325–334. doi:10.1563/AAID-JOI-D-09-00117.1
29. Iyer SS, Cheng G. Role of interleukin 10 transcriptional regulation in inflammation and autoimmune disease. Crit Rev Immunol. 2012;32(1):23–63.
30. Parameswaran N, Patial S. Tumor necrosis factor-α signaling in macrophages. Crit Rev Eukaryot Gene Expr. 2010;20(2):87–103.
31. Akdis M, Burgler S, Crameri R, et al. Interleukins, from 1 to 37, and interferon-γ: receptors, functions, and roles in diseases. J Allergy Clin Immunol. 2011;127(3):701–721. doi:10.1016/j.jaci.2010.11.050
32. Manicone AM, McGuire JK. Matrix metalloproteinases as modulators of inflammation. Semin Cell Dev Biol. 2008;19(1):34–41. doi:10.1016/j.semcdb.2007.07.003
33. Dereka X, Mardas N, Chin S, Petrie A, Donos N. A systematic review on the association between genetic predisposition and dental implant biological complications. Clin Oral Implants Res. 2011;23(7):775–788. doi:10.1111/j.1600-0501.2011.02329.x
34. Elhoussiney AG, Zhang H, Song J, Ji P, Wang L, Yang S. Influence of implant location on the clinical outcomes of implant abutments: a systematic review and meta-analysis. Clin Cosmet Investig Dent. 2018;10:19–35. doi:10.2147/CCIDE.S143910
35. Junior JFS, Biguetti CC, Matsumoto MA, et al. Can genetic factors compromise the success of dental implants? A systematic review and meta-analysis. Genes (Basel). 2018;9(9):ii.
36. Arigbede A, Babatope B, Bamidele M. Periodontitis and systemic diseases: a literature review. J Ind Soc Periodontol. 2012;16(4):487. doi:10.4103/0972-124X.106878
37. Alvim-Pereira F, Montes CC, Mira MT, Travilatto PC. Genetic susceptibility to dental implant failure: a critical review. Int J Oral Maxillofac Implants. 2008;23(3):409–416.
38. Schaefer AS. Genetics of periodontitis: discovery, biology, and clinical impact. Periodontol 2000. 2018;78(1):162–173. doi:10.1111/prd.12232
39. Shaddox LM, Walker CB. Treating chronic periodontitis: current status, challenges, and future directions. Clin Cosmet Investig Dent. 2010;11(2):79–91. doi:10.2147/CCIDE.S7712
40. Kordbacheh Changi K, Finkelstein J, Papapanou PN. Peri-implantitis prevalence, incidence rate, and risk factors: a study of electronic health records at a U.S. dental school. Clin Oral Implants Res. 2019;30(4):306–314. doi:10.1111/clr.13416
41. Al-Juboori MJ. Progressive immediate loading of a perforated maxillary sinus dental implant: a case report. Clin Cosmet Investig Dent. 2015;29(7):25–31. doi:10.2147/CCIDE.S76637
42. Schimmel M, Srinivasan M, McKenna G, Müller F. Effect of advanced age and/or systemic medical conditions on dental implant survival: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):311–330. doi:10.1111/clr.13288
43. Chappuis V, Avila-Ortiz G, Araújo MG, Monje A. Medication-related dental implant failure: systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):55–68. doi:10.1111/clr.13137
44. Moy PK, Medina D, Shetty V, Aghaloo TL. Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants. 2005;20(4):569–577.
45. ElHoussiney AG, Zhang H, Song J, Ji P, Wang L, Yang S. Influence of implant location on the clinical outcomes of implant abutments: a systematic review and meta-analysis. Clin Cosmet Investig Dent. 2018;26(10):19–35. doi:10.2147/CCIDE.S143910
46. Hickin MP, Shariff JA, Jennette PJ, Finkelstein J, Papapanou PN. Incidence and determinants of dental implant failure: a review of electronic health records in a U.S. dental school. J Dent Educ. 2017;81(10):1233–1242. doi:10.21815/JDE.017.080
47. Jeong I, Papapanou PN, Finkelstein J. Implant failure prediction using discriminant analysis. Conf Proc IEEE Eng Med Biol Soc. 2019;2019:1–5.
48. Eguia Del Valle A, López-Vicente J, Martínez-Conde R, Aguirre-Zorzano LA. Current understanding of genetic polymorphisms as biomarkers for risk of biological complications in implantology. J Clin Exp Dent. 2018;10(10):e1029–e1039. doi:10.4317/jced.55141
49. Daly AK, Day CP. Candidate gene case-control association studies: advantages and potential pitfalls. Br J Clin Pharmacol. 2001;52(5):489–499. doi:10.1046/j.0306-5251.2001.01510.x
50. Tanaka K, Miyake Y, Hanioka T, Arakawa M. Relationship between IL1 gene polymorphisms and periodontal disease in Japanese women. DNA Cell Biol. 2014;33(4):227–233. doi:10.1089/dna.2013.2202
51. García-Delaney C, Sánchez-Garcés MÁ, Figueiredo R, Sánchez-Torres A, Gay-Escoda C. Clinical significance of interleukin-1 genotype in smoking patients as a predictor of peri-implantitis: a case-control study. Med Oral Patol Oral Cir Bucal. 2015;20(6):e737–43.
52. de Araujo Munhoz FB, Branco FP, Souza RLR, Dos Santos MCLG. Matrix metalloproteinases gene polymorphism haplotype is a risk factor to implant loss: a case-control study. Clin Implant Dent Relat Res. 2018;20(6):1003–1008. doi:10.1111/cid.12671
53. Finkelstein J, Friedman C, Hripcsak G, Cabrera M. Pharmacogenetic polymorphism as an independent risk factor for frequent hospitalizations in older adults with polypharmacy: a pilot study. Pharmgenomics Pers Med. 2016;14(9):107–116.
54. Song JW, Chung KC. Observational studies: cohort and case-control studies. Plast Reconstr Surg. 2010;126(6):2234–2242. doi:10.1097/PRS.0b013e3181f44abc
55. Vaz P, Gallas MM, Braga AC, Sampaio-Fernandes JC, Felino A, Tavares P. IL1 gene polymorphisms and unsuccessful dental implants. Clin Oral Implants Res. 2012;23(12):1404–1413. doi:10.1111/j.1600-0501.2011.02322.x
56. Sampaio Fernandes M, Vaz P, Braga AC, Sampaio Fernandes JC, Figueiral MH. The role of IL-1 gene polymorphisms (IL1A, IL1B, and IL1RN) as a risk factor in unsuccessful implants retaining overdentures. J Prosthodont Res. 2017;61(4):439–449. doi:10.1016/j.jpor.2017.01.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.