")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Relationship Between Parent-Adolescent Communication and Depressive Symptoms: The Roles of School Life Experience, Learning Difficulties and Confidence in the Future
Authors Wang R, Li D, Zhang J, Song G, Liu Q, Tang X
Received 25 October 2021
Accepted for publication 3 May 2022
Published 23 May 2022 Volume 2022:15 Pages 1295—1310
DOI https://doi.org/10.2147/PRBM.S345009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Runnan Wang,1 Dong Li,2 Jiwei Zhang,1 Guirong Song,1 Qigui Liu,1 Xiao Tang1
1School of Public Health, Dalian Medical University, Dalian City, Liaoning Province, People’s Republic of China; 2School of Marxism, Dalian Ocean University, Dalian City, Liaoning Province, People’s Republic of China
Correspondence: Xiao Tang, School of Public Health, Dalian Medical University, Dalian City, Liaoning Province, People’s Republic of China, Tel +86-411-86110328, Email [email protected]
Purpose: Adolescent depression has become a public health issue in China. Family environment and school life play important roles in shaping adolescent mental health. Our study aimed to examine the effect of parent-adolescent communication, school-life experiences, learning difficulties, and confidence in the future on depressive symptoms. We also examined the mediating effects of school-life experiences, learning difficulties, and confidence in the future on the relationship between parent-adolescent communication and depressive symptoms.
Methods: Data on depressive symptoms, parent-adolescent communication, and mediating variables were obtained from the China Education Panel Survey (CEPS), including baseline data (2013– 2014) and follow-up data (2014– 2015). Mixed-effect models were used to evaluate the effects of parent-adolescent communication, school-life experiences, learning difficulties, and confidence in the future on depressive symptoms, and path analyses were performed to determine the mediating roles of school-life experiences, learning difficulties, and confidence in the future on the relationship between parent-adolescent communication and adolescent depressive symptoms.
Results: More father-adolescent communication, better school-life experiences, and higher confidence in the future were protective factors for depressive symptoms among all boys and girls, and learning difficulties were a risk factor for depressive symptoms among all boys and girls. School-life experiences, learning difficulties, and confidence in the future had statistically significant mediating effects on the relationship between parent-adolescent communication and depressive symptoms.
Conclusion: More father-adolescent communication, higher confidence in the future, better school-life experiences, and fewer academic difficulties were associated with lower levels of depressive symptoms. Both mother-adolescent communication and father-adolescent communication affected depressive symptoms through their effects on school-life experience, learning difficulties, and confidence in the future. This finding highlighted the importance of parent-adolescent communication and its impact on depression.
Keywords: depression, communication, adolescent, CEPS
Introduction
The World Health Organization’s (WHO) proposition “no health without mental health” illustrates the indispensability of mental health in overall health.1 Depression is the second leading cause of disability globally.2 Adolescent depression has serious consequences for present and future mental health. It can impair academic performance and increase social difficulties.3 More serious symptoms lead to substance abuse, strong feelings of guilt, schizophrenia, and even suicide.4 Furthermore, adolescent depression can follow individuals for life, resulting in severe loss of self-esteem, impaired relationships, and impaired vocational achievement.5,6 Recent studies have shown that the prevalence of adolescent depression in different areas of China ranges from 18% to 20%.7,8 Adolescent depression has become a public health concern in China.
Since adolescent mental health is mainly shaped in the family environment, many studies focus on the relationship between family members and mental health.9–11 Within the family, communication is defined as attending to the exchange of needs, feelings, and desires among family members and providing assistance to family members.12,13 Parent-adolescent communication is particularly important during adolescence. Good parent-adolescent communication has been reported to be a protective factor for adolescent depression,14,15 while hostile parent-adolescent relationships can increase the risk of depression in adolescents.16 Furthermore, adolescents who have less emotional interactions with their parents are more likely to develop serious consequences, such as delinquency, in addition to depression.16,17 Previous studies have shown that mothers and fathers have different characteristics in terms of communication with children. Mothers tend to communicate more frequently, emotionally, and actively with their children, receiving more information from them and providing more care and timely support. Fathers are less involved, but they can often provide more problem-solving strategies and autonomy support.18 However, whether both mother-child communication and father-child communication have significant effects on adolescent depressive symptoms is inconsistent in previous studies. Some studies have suggested that attachment security to the mother, rather than the father, was negatively associated with depressive symptoms in adolescents. Some suggested that open communication with fathers was negatively associated with depressive symptoms, whereas such communication with mothers was not.19
In addition to the impact of parent-adolescent communication on depressive symptoms, previous studies also indicated that parent-adolescent communication played important roles in other aspects of adolescents’ lives, such as academic performance, school experience, and optimism.20–24 Open and positive parent-adolescent communication can increase closeness among family members and help resolve children’s problems and difficulties in their lives, resulting in improved academic performance, school experience, and confidence in the future. These aspects have also been associated with adolescent depression.25–27 Therefore, parent-adolescent communication may also play a role in adolescent depression through these aspects, which has not been completely confirmed.
School-life experience mainly reflects relationships with teachers and classmates and satisfaction with school. It is wel-known that adolescents spend an important part of their lives at school. Therefore, school-life experience plays an important role in meeting the basic development needs of adolescents.28,29 Adolescents’ basic developmental needs include autonomy, intimacy, and identity formation; however, modern middle schools are characterized by increased discipline and academic and social competition. The mismatch between these two aspects leads to an increased risk of psychosocial problems such as anxiety and depression in adolescents.28,30,31 Conversely, positive school-life experiences such as good peer relationships and feeling supported by teachers help adolescents cope with difficulties and challenges appropriately, which contributes to reducing the risk of adolescent depression.26
Learning difficulties in courses can have a negative influence on adolescents. Some studies have shown that learning difficulties are positively related to depression in children and adolescents.32,33 Learning difficulties may make adolescents feel frustrated and intensify school failure and have a negative impact on self-esteem and mental health.34 Based on China’s huge population and its imbalance of social, economic, and cultural development, Chinese adolescents face fierce academic competition and high pressure.35,36 Therefore, it is necessary to explore the effect of academic difficulties on adolescent depression in China.
Confidence in the future is the individual’s expectations and hopes for a better life situation, and it is a dimension of optimism.37 Previous studies have found that optimism is a protective factor for mental and somatic health.38,39 However, very few studies have explored the association of confidence in the future with mental health problems.37 A cross-sectional study in Finland clarified that high confidence in the future appeared to be associated with low psychological distress in adults.37 High confidence helps children cope with negative outcomes and worry less about failure;40 conversely, low self-esteem has been identified as a key reason behind development of depressive symptoms in adolescents.
Since parent-adolescent communication benefits children’s developmental outcomes, including academic performance, school-life experience, and confidence in the future, and these aspects may be closely associated with depression,10,14,20,41–43 we assume that parent-adolescent communication can affect depression through school-life experience, learning difficulties, and confidence in the future. This study was based on the China Education Panel Survey (CEPS) database, which is a nationwide survey of adolescents in China, and had two main purposes: 1) to explore the effects of parent-adolescent communication, school-life experience, learning difficulties, and confidence in the future on depressive symptoms and 2) to determine the mediating roles of school-life experience, learning difficulties, and confidence in the future on the associations between parent-adolescent communication and depressive symptoms.
Methods
Study Design and Participants
This study used data from CEPS, conducted by the National Survey Research Center (NSRC), Renmin University of China. The CEPS aimed to record and explain the educational process of junior high school students from a lower education stage to a higher education stage.
The NSRC used a multistage probability-proportional-to-size sampling method to collect subjects. In the first stage, 28 county-level units (county/district/city) were randomly selected in mainland China. In the second stage, four middle schools were randomly selected in each unit. In the third stage, two seventh grade classes and two ninth grade classes were selected in each sample school, and all students in the selected classes were asked to complete the questionnaire.44
The first wave was collected during the 2013–2014 academic year, and the second was collected the next academic year (2014–2015), but the second wave of the survey only followed-up with the seventh graders. In the first wave, the sample size of seventh graders was 10,279 (5,310 boys, 4,773 girls, 196 gender unreported). In the second wave, the sample size of eighth graders was 9,449 (4,842 boys; 4,436 girls; 171 gender unreported, 830 were lost to follow-up), and there was no follow-up for ninth graders. Finally, 9,449 subjects who had both seventh- and eighth-grade data were included in our study.
Variables and Measurements
Dependent Variable: Depressive Symptoms
Depressive symptoms were assessed by a 4-item scale. Students were asked the frequency of the following feelings during the past seven days: “blue”, “unhappy”, “life is meaningless”, and “sad”. The responses used a 5-point Likert scale where “never” =1, “seldom” =2, “sometimes” =3, “most of the time” =4 and “always” =5. The total score of items was defined as the score for depressive symptoms. A higher score indicated worse mental status (scores ranged from 4 to 20, Cronbach’s α = 0.959). “Probable depression” was defined as baseline scoring ≥ top 10% of baseline depressive symptoms score.9
Independent Variables
Mother-adolescent communication and father-adolescent communication were measured by 4 items created by the CEPS researchers. Students were asked the frequency of communicating with their fathers and mothers about “what happened at school”, “your relationship with friends”, “your relationship with the teachers”, and “your thoughts or worries”. A 3-point Likert scale was used: “never” =1, “sometimes” =2 and “often” =3. Scores for each item were summed, and higher scores indicated more mother-adolescent communication or father-adolescent communication (scores ranged from 4 to 12, Cronbach’s α values were 0.769 and 0.788, respectively). Parent-adolescent communication score was defined as the sum of scores for mother-adolescent communication and father-adolescent communication (ranging from 8 to 24). In addition, mother-adolescent communication scores, father-adolescent communication scores, and parent-adolescent communication scores were divided into quartiles and defined as categorical variables.
School-life experience in this study referred to the students’ experiences and feelings about their school life. It was measured by 9 items in the questionnaire, including “my parents often receive criticism from my teachers”, “the teacher in charge of the class often praises me”, “the teacher in charge of the class often criticizes me”, “most of my classmates are very friendly to me”, “the atmosphere in my class is good”, “I often participate in activities in school or class”, “I feel close to the people at this school”, “I’m bored in this school”, and “I wish I could go to another school”. Students were asked to choose responses scored on a 4-point Likert scale to express their degree of consent: “strongly disagree” = 1, “slightly disagree” = 2, “somewhat agree” = 3, “strongly agree” = 4. The school-life experience score was calculated by summing the responses of all items (four items were reverse scored). A higher score indicated better school life experiences (scores ranged from 9 to 36, Cronbach’s α = 0.921). In addition, the school-life experience scores were divided into quartiles and defined as a categorical variable.
Learning difficulties referred to the level of experiencing difficulties in learning mathematics, Chinese, and English. Three questions reflecting the difficulties in each course and response options were as follows: “not strenuous at all” =1, “not very strenuous” =2, “a little strenuous” =3, and “particularly strenuous” =4. Learning difficulties were assessed by the total score for the three items, and a higher score indicated greater learning difficulties (scores ranged from 3 to 12, Cronbach’s α = 0.921). In addition, learning difficulties scores were also divided into quartiles and defined as a categorical variable.
Confidence in the future was reflected by one item. Students were asked “Do you have confidence in your future?” A 4-point Likert scale was used: “no confidence at all” =1, “less confident” =2, “comparative confidence” =3, and “very confident” = 4. The higher the score was, the more confident the student. In addition, confidence in the future was also used as a categorical variable, in which “no confidence at all” and “less confident” were combined as a group due to a small sample in level 1.
Covariates
Covariates included age, gender, ethnicity (Han, non-Han), whether mother and father get along well with each other (yes, no), household economic status (“very difficult” =1, “a little difficult” =2, “average” =3, “a little affluent” =4, “very affluent” =5), mother’s and father’s education level (junior middle school or less =1, senior middle school or vocational schools =2, college =3).
Statistical Analysis
First, the baseline characteristics of students were described. Means and standard deviations were used to present continuous variables, and frequencies and percentages were used to describe categorical variables. Chi-squared test, Wilcoxon’s rank-sum test, and two independent samples t-test were adopted to test differences between boys and girls at baseline.
Second, the score for depressive symptoms at baseline was divided into four quartiles, and analysis of variance (ANOVA) was used to determine the differences in the levels of independent variables between quartiles.
Third, baseline scores for parent-adolescent communication, mother-adolescent communication, father-adolescent communication, learning difficulties, school-life experiences, and confidence in the future were divided and used as categorical variables. Mixed-effects models were fit to examine the relationships between these independent variables and the outcome “probable depression”. The group with the lowest score was set as reference group in each independent variable, and the risk of “probable depression” with each other group versus reference group was tested.
Fourth, scores for parent-adolescent communication, mother-adolescent communication, father-adolescent communication, learning difficulties, school-life experiences, and confidence in the future were used as continuous variables, and path analyses were performed to study the potential mediating effects of learning difficulties, school-life experiences, and confidence in the future on the relationship between parent-adolescent communication and depressive symptoms (score). Three models were applied as setting parent-adolescent communication, father-adolescent communication, and mother-adolescent communication as the starting point of the path, respectively (Figure 1, Supplementary Figures 1 and 2). And a bootstrap test (n=2000 replications) was performed to test the indirect effect. The eighth-grade data were used in the path model building. An indirect effect was considered statistically significant if 95% CIs did not include zero.45
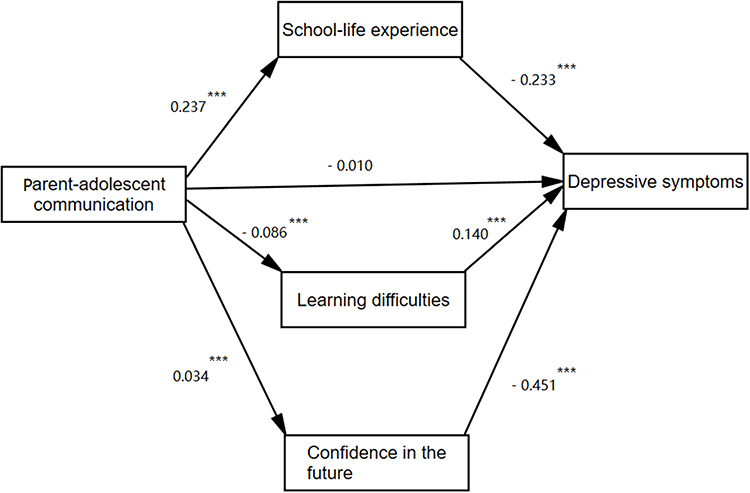 |
Figure 1 Mediation model between parent-adolescent communication and depressive symptoms (***p < 0.001). |
All analyses in this study were conducted by gender, and all models were adjusted for age, ethnicity, whether mother and father get along well with each other, household economic status and mother’s and father’s education level. SPSS 22.0 was used for general statistical analysis, and Mplus 7.4 (Los Angeles, CA) was used for mixed-effects modelling and path analyses.
Ethical approval for this study was granted by the Institutional Review Board (IRB) of Renmin University of China and the IRB of Dalian Medical University (Ethics Approval No. [2021] 002). Participation in the study was voluntary, and informed consent from guardians and verbal assent from children were received. This study complied with the Declaration of Helsinki.
Results
The General Characteristics of Adolescents
The general characteristics of adolescents at baseline are displayed in Table 1. The average age of the students was 13.3 years. Parent-adolescent communication, mother-adolescent communication, school-life experiences, and learning difficulties were significantly different between boys and girls. Boys were more likely to have more learning difficulties than girls, and girls were more likely to have more depressive symptoms than boys. Girls had better communication with their mothers and better school-life experiences than boys.
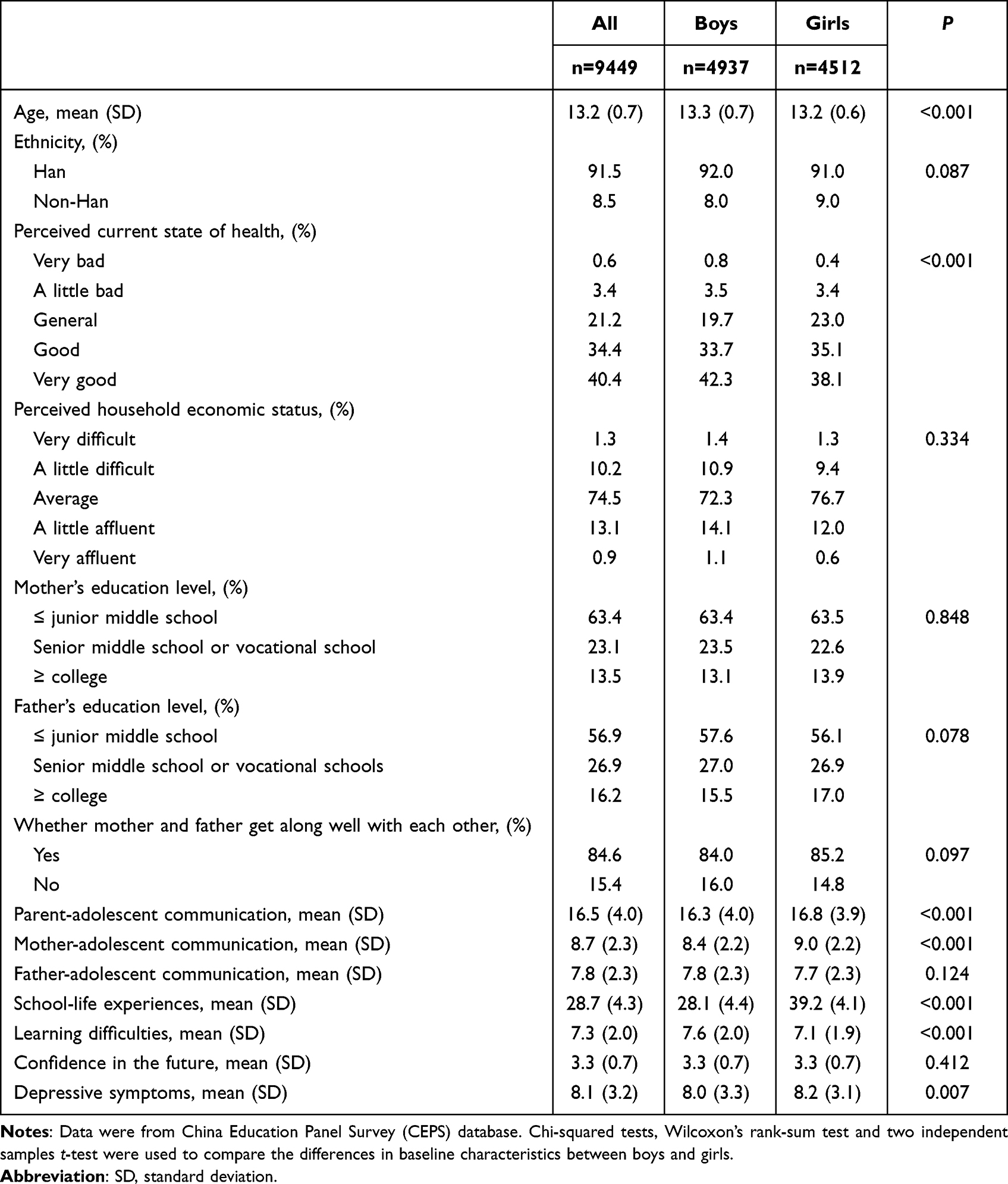 |
Table 1 The General Characteristics of Chinese Adolescents at Baseline |
Differences in the levels of factors among quartiles of depressive symptoms are presented in Table 2. The levels of parent-adolescent communication, father-adolescent communication, mother-adolescent communication, confidence in the future, and school-life experiences decreased with increasing depressive symptoms, whereas learning difficulties increased with increasing depressive symptoms.
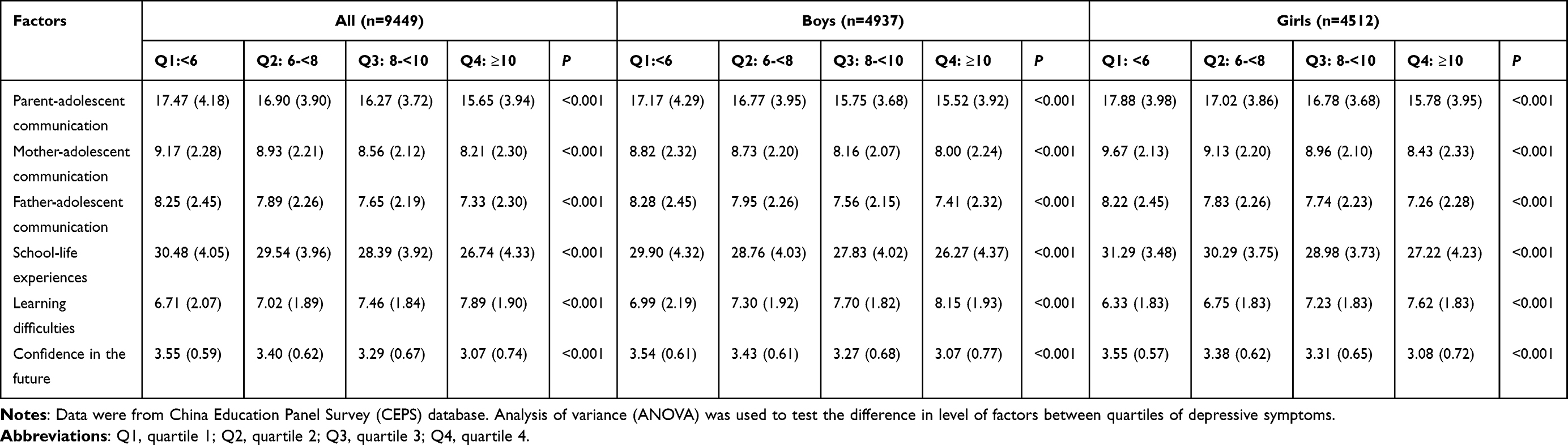 |
Table 2 The Differences in Levels of Factors Across Quartiles of Depressive Symptoms at Baseline |
The Results of Mixed-Effects Models
The results of mixed-effects models are presented in Table 3. Among all adolescents, the risk of “probable depression” decreased 41% (OR=0.59) and 22% (OR=0.78) with the 3rd and 4th quartiles of father-adolescent communication versus the 1st quartile, respectively. Among boys and girls, it was still statistically significant when the 3rd quartile of father-adolescent communication was compared with the 1st quartile, but significant result was not obtained when the 4th quartile was compared with the reference group. Learning difficulties had a positive association with “probable depression”, and the risk of “probable depression” increased 43% (OR=1.43) with the 4th quartile versus the 1st quartile among all adolescents. Similar results were also shown among boys. Good school-life experience was a protective factor for “probable depression” among all adolescents. Compared with the 1st quartile of school-life experience, the probabilities of having “probable depression” in the 2nd quartile, the 3rd and the 4th quartile decreased 51% (OR=0.49), 66% (OR=0.34), and 73% (OR=0.27), respectively. School-life experience was also a strong factor for “probable depression” in both boys and girls. Confidence in the future was negatively associated with “probable depression” among all adolescents. Compared with the 1st level of confidence in the future, the risks of “probable depression” in the 2nd and the 3rd levels decreased 61% (OR=0.39) and 70% (OR=0.30), respectively. These results on the relationship between confidence in the future and “probable depression” were consistent with those in boys and girls.
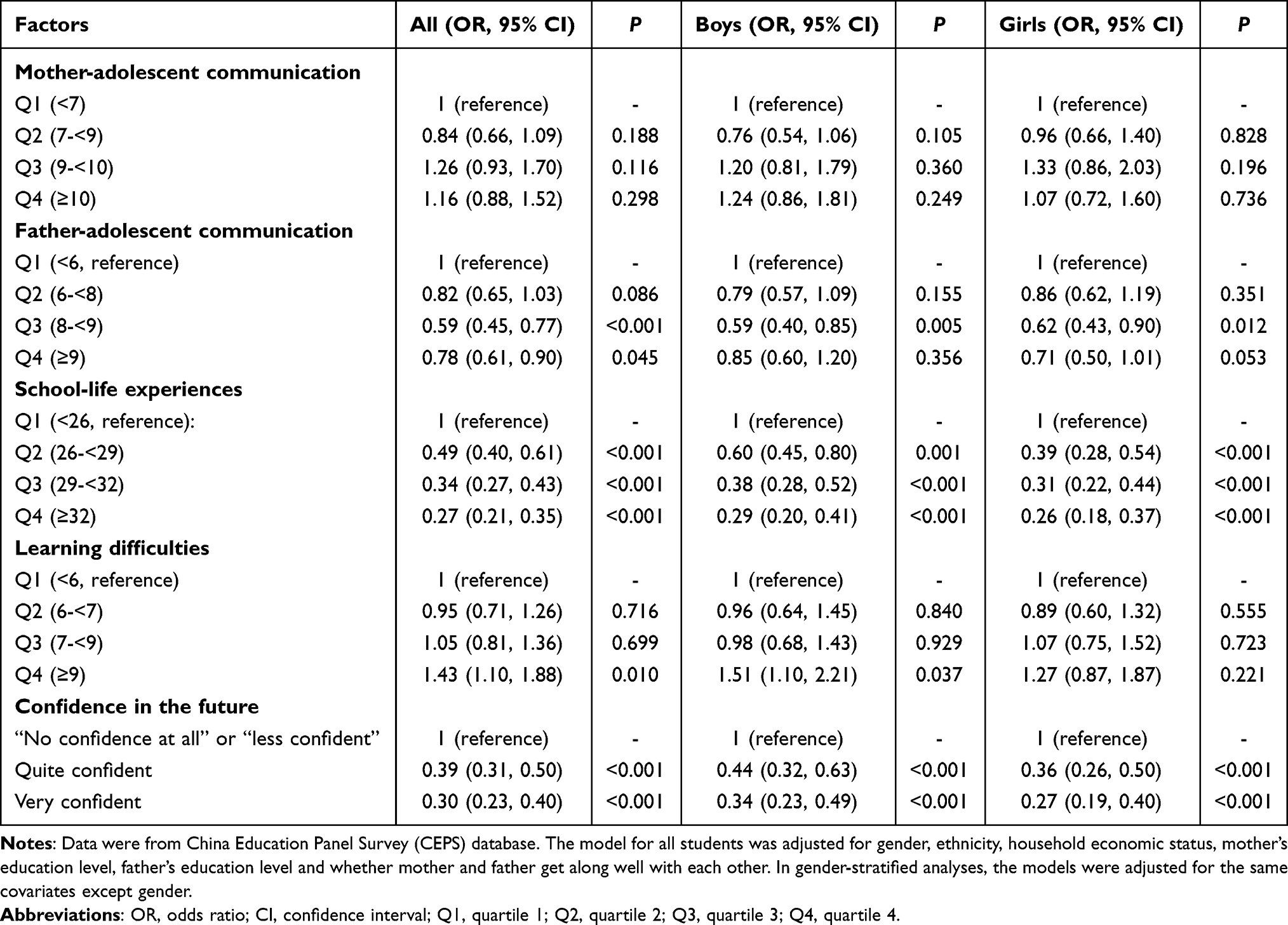 |
Table 3 Effects of Mother-Adolescent Communication, Father-Adolescent Communication, School-Life Experience, Learning Difficulties, and Confidence in the Future on Depressive Symptoms by the Mixed Effects Model |
In Supplementary Table 1, parent-adolescent communication was not significantly associated with “probable depression” among all adolescents, boys, and girls.
The Results of Mediation Analysis
Parent-adolescent communication, father-adolescent communication, and mother-adolescent communication had indirect effects on depressive symptoms through school-life experiences, learning difficulties, and confidence in the future among all boys and girls (Figure 1, Supplementary Figures 1 and 2).
For father-adolescent communication, the mediating effect sizes (percentage of the total effect size) of school-life experiences on depressive symptoms were −0.047 (56.63%) in all students, −0.054 (59.34%) in boys, and −0.042 (51.85%) in girls. The mediating effect sizes (percentage of the total effect size) of learning difficulties on depressive symptoms were −0.010 (21.74%) in all students, −0.008 in boys and −0.012 in girls. The mediating effect sizes (percentage of the total effect size) of confidence in the future were −0.014 (28.00%) in all students, −0.013 in boys and −0.015 in girls (Table 4).
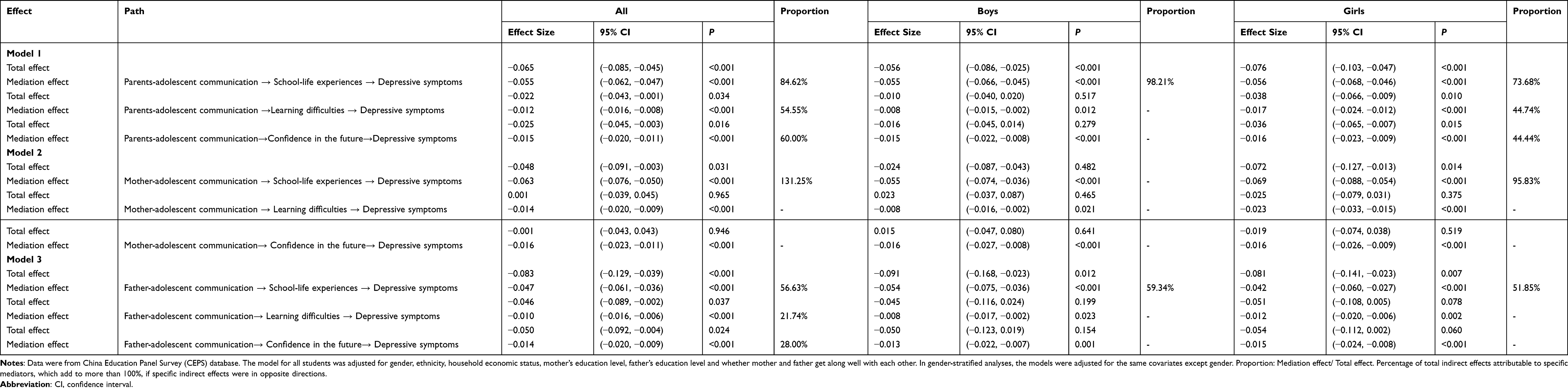 |
Table 4 The Mediation Effect Sizes of School-Life Experiences, Learning Difficulties and Confidence in the Future on the Relationship Between Parent-Adolescent Communication and Depressive Symptoms |
For mother-adolescent communication, the mediating effect sizes (percentage of the total effect size) of school-life experiences on depressive symptoms were −0.063 (131.25%) in all students, −0.055 in boys, and −0.069 (95.83%) in girls. The mediating effect sizes of learning difficulties were −0.014 in all students, −0.008 in boys, and −0.023 in girls, and the mediating effect sizes of confidence in the future were −0.016 in all students, −0.016 in boys, and −0.016 in girls (Table 4).
For parent-adolescent communication, the mediating effects (percentage of the total effect size) of school-life experiences were −0.055 (84.62%) in all students, −0.055 (98.21%) in boys, and −0.056 (73.68%) in girls. The mediating effects (percentage of the total effect size) of learning difficulties were −0.012 (54.55%) in all students, −0.008 in boys, and −0.017 (44.74%) in girls. The mediating effects (percentage of the total effect size) of confidence in the future were −0.015 (60.00%) in all students, −0.015 in boys, and −0.016 (44.44%) in girls (Table 4).
Discussion
In the current study, father-adolescent communication, school-life experiences, learning difficulties, and confidence in the future were found to be associated with depressive symptoms in Chinese adolescents. In addition, parent-adolescent communication, father-adolescent communication, and mother-adolescent communication had indirect effects on depressive symptoms through school-life experiences, learning difficulties, and confidence in the future.
In our study, parent-adolescent communication was not statistically associated with depressive symptoms. However, many previous studies have shown that positive parent-adolescent communication is a protective factor for children’s psychological and behavioral problems,13 and negative parent-adolescent communication was strongly associated with increased depressive symptoms, risky sexual behavior and lower life satisfaction,46–50 which was not consistent with our results. In the current study, father-adolescent communication was associated with adolescent depressive symptoms in the mixed-effect model, but mother-adolescent communication was not statistically significant. It is still controversial whether both father-adolescent communication and mother-adolescent communication have significant effects on depressive symptoms. A study including 809 adolescents in Ethiopia found that both good mother-adolescent communication and father-adolescent communication played positive roles in reducing the risk of depression,51 which was not entirely consistent with our results. Another study showed that the father-adolescent relationship played a more important role in psychological well-being than the mother-adolescent relationship in Finland.52 The different effects on depression between mother- and father-adolescent communication might be explained by the different roles that fathers and mothers play in their children’s adolescence. Mothers are traditionally in charge of daily care and give emotional comfort to their children.53,54 However, mothers are found to be more concerned about closeness and intimacy, which might not fully meet the needs for adolescents’ individuality and autonomy.55,56 Fathers tend to engage in children’s playtime and encourage children to face challenges and difficulties.57 Compared with mothers, fathers are more likely to provide more problem-solving strategies and autonomy support and help children regulate their negative emotions and improve their internalizing symptoms.56,58–60 However, in traditional Chinese culture, fathers are the head of family and have authority to supervise children’s behavior and to require them to be obedient. Due to less emotional expression in father-child communication, Chinese fathers usually have low attachment and bonding with their children,61 which is not beneficial for the children’s mental health.
In the current study, positive school-life experiences helped to reduce depressive symptoms. Peer relationships, teacher-student relationships, and school climate are major components of school-life experiences. Good peer relationships play a positive role in alleviating anxiety and depression in adolescence,62,63 whereas conflict with friends is a consistent risk for depression across adolescence.64 Good relationships with classmates can help foster a good learning climate and make adolescents feel supported and accepted when facing difficult tasks in school and friendship; in contrast, poor relationships with classmates create a competitive and hostile climate, which increases stress, anxiety, and depressive symptoms.65 In addition, higher perceived teacher support has been associated with a lower level of depression.66–68 Teacher support can make students feel loved, cared for, and inspired (when students believe that their teachers understand their inner feelings, give them a chance to make choices, support and help them solve problems);69,70 this support leads to an increase in students’ feelings of liking school, belonging, and interest and enjoyment in school.71 Teacher support can also help students improve their social adaptation, learning engagement, and adaptation to school, which directly correlates with students’ mental health.72–76 Therefore, a good school climate can provide a safe and orderly environment and reduce aggressive behavior such as bullying and sexual harassment, which are closely linked to more depressive symptoms in victims.
In our study, severe learning difficulties played a positive role in increasing depressive symptoms in adolescents, which has been confirmed by some theories, such as hopelessness theory adapted for the academic context and competence model.77–79 Learning at school is the major task during adolescence, and school performance is considered an important predictor of future success.80,81 Learning difficulties can cause feelings of academic failure and negative attitudes toward school, and then these negative effects continue to accumulate, eventually leading to feelings of being exhausted and overwhelmed.82,83 In contrast, adolescents who are academically successful often receive positive feedback from teachers, parents and classmates, which gives them satisfaction and self-confidence. China is a country that highly values education.35,36 As China has a large population, academic competition among students is very cruel. In some provinces, approximately 50% of junior high school students will not be able to attend ordinary high school because they cannot pass the entrance exam. They can only choose technical school or vocational high school or even drop out from school,84 which means they will be in lower-paying occupations in the future. Therefore, under this cruel education system, children with learning difficulties or with poor grades feel a lot of pressure. Our path analysis results also indicated that more parent-adolescent communication helped alleviate the feelings associated with learning difficulties. Children with learning difficulties may receive care, encouragement or problem-solving strategies from their parents, which is helpful for their mental health.
In the current study, higher confidence in the future was associated with a lower level of depressive symptoms. A longitudinal study in Finland involving 101,257 adults also obtained consistent results.37 Although studies on the association between confidence in the future and depression are very limited, there are many studies on the association of depression with optimism, self-esteem and self-efficacy, which are closely connected with confidence in the future. Persons with high self-efficacy and optimism tend to regard failure as a challenge that deepens their perseverance in achieving their goals; in contrast, those with low self-efficacy may feel helpless and less motivated when failure happens, triggering depressive symptoms.63
In our study, through mediation analysis, we found that parent-adolescent communication, father-adolescent communication and mother-adolescent communication can indirectly affect depressive symptoms through their effects on learning difficulties, confidence in the future and school-life experiences. Our results indicated that more adolescent-parent communication helped promote many aspects of children’s lives that had effects on depressive symptoms. Parent-adolescent communication may provide children with an outlet for releasing anxiety and stress and a chance to obtain support and suggestions from their parents, directly increasing their confidence in the future, school experiences and ability to face learning difficulties. However, in Chinese culture, adolescents are less likely to communicate openly about conflicts and disagreements with their parents because they are trained to be obedient.85 Chinese parents express less positive affection for their children than Western parents.86 Chinese parents attach more importance to educating and nurturing their children, but they often ignore communicating with their children. This situation is expected to be valued and changed.
There are some study limitations in our research. First, the questions that measure depression could only reflect certain depressive symptoms but not a clinical diagnosis of depression. Mood and psychotic symptoms often co-occur, and the differential diagnosis may be rather imprecise. There exists an emerging notion that mood disorders lie on a spectrum or a dimensional view. These conditions are not discrete categories and may form at least part of a continuum or affective disorder spectrum.87 Therefore, depressive symptoms in this study are not necessarily representative of clinically diagnosed depression. Second, in our study, parent-adolescent communication reflected the frequency and content of parent-adolescent communication, but it did not include the pattern of communication such as positive or negative communication, active or passive communication, warm or rigid communication, which was confirmed to have an influence on adolescent depressive symptoms.49,88–90 Third, although this study was a longitudinal study, the interval between follow-ups was only one year. Fourth, we examined the effects of parent-adolescent communication on depressive symptoms through confidence, learning difficulties, and school-life experiences. However, it is possible that changes in confidence, learning difficulties and school-life experiences lead to changes in parent-adolescent communication, but we did not test the reverse causality of these three factors on parent-adolescent communication. Fifth, variables in this study might be influenced by other factors that were not observed in the investigation. Personal features such as personality disorders and autism spectrum disorder influence academic performance and social functioning. Genetic factors, the mental situation of parents, behaviors of parents and negative events such as sexual abuse and childhood maltreatment also have an impact on academic performance, social ability and adolescent depression. Therefore, mediating factors might be complex and interactive. Longitudinal studies with more detailed information on parent-adolescent communication, more comprehensive factors and more accurate diagnoses are needed to determine the role of parent-child communication on adolescent depression.
Conclusion
In conclusion, more father-adolescent communication, better school-life experiences, fewer academic difficulties, and higher confidence in the future were associated with a decreased risk of depression. Parent-adolescent communication could indirectly reduce depressive symptoms through the mediating effects of school-life experiences, learning difficulties, and confidence in the future. Therefore, parent-adolescent communication should be greatly advocated to reduce adolescent depression.
Ethics Approval and Consent to Participate
Ethical approval for this study was granted by Institutional Review Board (IRB) of Renmin University of China and IRB of Dalian Medical University (Ethics Approval No. [2021] 002). Participation in the study was voluntary, and informed consent from guardians and verbal assent from children were received. This study complied with the Declaration of Helsinki.
Acknowledgments
We thank all participants in the survey and CEPS research team for collecting data and managing the CEPS database. The CEPS data can be requested at http://ceps.ruc.edu.cn/.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Mental Health: Facing the Challenges, Building Solutions: Report from the WHO European Ministerial Conference. WHO Regional Office Europe; 2005.
2. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196. doi:10.1016/S0140-6736(12)61729-2
3. Verboom CE, Sijtsema JJ, Verhulst FC, Penninx BW, Ormel J. Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Dev Psychol. 2014;50(1):247. doi:10.1037/a0032547
4. Brent DA, Birmaher B. Adolescent depression. N Engl J Med. 2002;347(9):667–671. doi:10.1056/NEJMcp012249
5. Newman DL, Moffitt TE, Caspi A, Magdol L, Silva PA, Stanton WR. Psychiatric disorder in a birth cohort of young adults: prevalence, comorbidity, clinical significance, and new case incidence from ages 11 to 21. J Consult Clin Psychol. 1996;64(3):552–562. doi:10.1037//0022-006X.64.3.552
6. Wyatt LC, Ung T, Park R, Kwon SC, Trinh-Shevrin C. Risk factors of suicide and depression among Asian American, Native Hawaiian, and Pacific Islander youth: a systematic literature review. J Health Care Poor Underserved. 2015;26(20):191. doi:10.1353/hpu.2015.0059
7. Liang WD, Yang J, Chen KY. Depressive symptoms and the influencing factors among middle school students. Med J Chin People’s Health. 2013;25(19):19–22. In Chinese.
8. Gao Q, Wu M, Wang GH, et al. Prevalence of depression and its influencing factors among middle school students in Liaoning province. Chin J Sch Health. 2020;41(09):1362–1364. In Chinese. doi:10.16835/j.cnki.1000-9817.2020.09.022
9. Ma L, Gao L, Chiu DT, Ding Y, Wang W, Wang Y. Depressive symptoms prevalence, associated family factors, and gender differences: a national cohort study of middle school students in China. J Affect Disord. 2020;274:545–552. doi:10.1016/j.jad.2020.05.128
10. Li Y, Hu T, Ge T, Auden E. The relationship between home-based parental involvement, parental educational expectation and academic performance of middle school students in Mainland China: a mediation analysis of cognitive ability. Int J Educ Res. 2019;97:139–153. doi:10.1016/j.ijer.2019.08.003
11. Hemati Z, Abbasi S, Oujian P, Kiani D. Relationship between parental communication patterns and self-efficacy in adolescents with parental substance abuse. Iran j Child Neurol. 2020;14(1):49.
12. Barnes HL, Olson DH. Parent-adolescent communication and the circumplex model. Child Dev. 1985;56(2):438–447. doi:10.2307/1129732
13. Guilamo-Ramos V, Jaccard J, Dittus P, Bouris AM. Parental expertise, trustworthiness, and accessibility: parent‐adolescent communication and adolescent risk behavior. J Marriage Fam. 2006;68(5):1229–1246. doi:10.1111/j.1741-3737.2006.00325.x
14. Ying L, Zhou H, Yu S, et al. Parent-child communication and self-esteem mediate the relationship between interparental conflict and children’s depressive symptoms. Child Care Health Dev. 2018;44(6):908–915. doi:10.1111/cch.12610
15. Wang L, Feng Z, Yang G, et al. The epidemiological characteristics of depressive symptoms in the left-behind children and adolescents of Chongqing in China. J Affect Disord. 2015;177:36–41. doi:10.1016/j.jad.2015.01.002
16. Lewis G, Collishaw S, Thapar A, Harold GT. Parent-child hostility and child and adolescent depression symptoms: the direction of effects, role of genetic factors and gender. Eur Child Adolesc Psychiatry. 2014;23(5):317–327. doi:10.1007/s00787-013-0460-4
17. Moitra T, Mukherjee I. Parent-adolescent communication and delinquency: a Comparative study in Kolkata, India. Eur J Psychol. 2012;8(1):74–94. doi:10.5964/ejop.v8i1.299
18. Le Chanu M, Marcos H. Father-child and mother-child speech: a perspective on parental roles. Eur J Psychol Educ. 1994;9(1):3–13. doi:10.1007/bf03172881
19. Ioffe M, Pittman LD, Kochanova K, Pabis JM. Parent-adolescent communication influences on anxious and depressive symptoms in early adolescence. J Youth Adolesc. 2020;49(8):1716–1730. doi:10.1007/s10964-020-01259-1
20. Fan W, Williams CM. The effects of parental involvement on students’ academic self-efficacy, engagement and intrinsic motivation. Educ Psychol. 2010;30(1):53–74. doi:10.1080/01443410903353302
21. Onabamiro AA, Omoruyi AA, Soyingbe AA, Rosiji CO. Psycho-social factors predicting secondary school students’ academic self-efficacy in Lagos State, Nigeria. Int J Humanit Soc Sci Invent. 2013;2(4):10–17.
22. Ugoji FN. Family closeness, social physique anxiety and sexual coercion as determinants of academic self-efficacy among female undergraduate students in a Nigerian University. Int J Appl Psychol. 2013;3(2):25–30. doi:10.5923/j.ijap.20130302.01
23. Lv B, Lv L, Yan Z, Luo L. The relationship between parental involvement in education and children’s academic/emotion profiles: a person-centered approach. Child Youth Serv Rev. 2019;100:175–182. doi:10.1016/j.childyouth.2019.03.003
24. Liu L, He X, Li C, Xu L, Li Y. Linking parent-child relationship to peer relationship based on the parent-peer relationship spillover theory: evidence from China. Child Youth Serv Rev. 2020;116:105200. doi:10.1016/j.childyouth.2020.105200
25. Masselam VS, Marcus RF, Stunkard CL. Parent-adolescent communication, family functioning, and school performance. Adolescence. 1990;25(99):725–737.
26. Morin AJS, Janosz M, Larivée S. The Montreal Adolescent Depression Development Project (MADDP): school life and depression following high school transition. Psychiatry Res J. 2009;1(3):1–50.
27. Askeland KG, Bøe T, Breivik K, et al. Life events and adolescent depressive symptoms: protective factors associated with resilience. PLoS One. 2020;15(6):e0234109. doi:10.1371/journal.pone.0234109
28. Eccles JS, Lord S, Midgley C. What are we doing to early adolescents? The impact of educational contexts on early adolescents. Am j Educ. 1991;99(4):521–542. doi:10.1086/443996
29. Mortimore P. The positive effects of schooling. In: Teaching, Learning and the Curriculum in Secondary Schools. Routledge; 2005:247–272.
30. Eccles JS, Wigfield A, Midgley C, Reuman D, Iver DM, Feldlaufer H. Negative effects of traditional middle schools on students’ motivation. Elem Sch J. 1993;93(5):553–574. doi:10.1086/461740
31. Janosz M, Georges P, Parent S.Socioeducative environment in secondary school : a theoretical model to guide the assessment of the environment. Revue canadienne de psycho-éducation. 1998;27(2):285–306.(In French)
32. Wertz FJ. Adolescent underachievers: evaluating psychodynamic and environmental stresses. N Y State J Med. 1963;63:3524–3529.
33. de Lima RF, Ciasca SM. Depression symptoms and neuropsychological function in children with learning difficulties. Rev Neurocienc. 2010;18(3):314–319. doi:10.34024/rnc.2010.v18.8455
34. Snowling MJ, Hulme C. Annual research review: the nature and classification of reading disorders–a commentary on proposals for DSM-5. J Child Psychol Psychiatry. 2012;53(5):593–607. doi:10.1111/j.1469-7610.2011.02495.x
35. Ng FFY, Wei J. Delving into the minds of Chinese parents: what beliefs motivate their learning-related practices? Child Dev Perspect. 2020;14(1):61–67. doi:10.1111/cdep.12358
36. Li H. The ‘secrets’ of Chinese students’ academic success: academic resilience among students from highly competitive academic environments. Educ Psychol. 2017;37(8):1001–1014. doi:10.1080/01443410.2017.1322179
37. Joutsenniemi K, Härkänen T, Pankakoski M, et al. Confidence in the future, health-related behaviour and psychological distress: results from a web-based cross-sectional study of 101 257 Finns. BMJ open. 2013;3(6):e002397. doi:10.1136/bmjopen-2012-002397
38. Mosing MA, Zietsch BP, Shekar SN, Wright MJ, Martin NG. Genetic and environmental influences on optimism and its relationship to mental and self-rated health: a study of aging twins. Behav Genet. 2009;39(6):597–604. doi:10.1007/s10519-009-9287-7
39. Rasmussen HN, Scheier MF, Greenhouse JB. Optimism and physical health: a meta-analytic review. Ann Behav Med. 2009;37(3):239–256. doi:10.1007/s12160-009-9111-x
40. Akram M. Feelings of parental absence and level of confidence. SSRN Electron J. 2015. doi:10.2139/ssrn.2584561
41. Bulanda RE, Majumdar D. Perceived parent-child relations and adolescent self-esteem. J Child Fam Stud. 2009;18(2):203–212. doi:10.1007/s10826-008-9220-3
42. Ladd GW, Kochenderfer BJ. Linkages between friendship and adjustment during early school adjustment. Child Dev. 1996;67(3):235–251.
43. Ki P. School adjustment and academic performance: influences of the interaction frequency with mothers versus fathers and the mediating role of parenting behaviours. Early Child Dev Care. 2020;190(7):1123–1135. doi:10.1080/03004430.2018.1518904
44. Li M, Xue H, Wang W, Wang Y. Parental expectations and child screen and academic sedentary behaviors in China. Am J Prev Med. 2017;52(5):680–689. doi:10.1016/j.amepre.2016.12.006
45. MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi:10.1037/1082-989x.7.1.83
46. Atienzo EE, Walker DM, Campero L, Lamadrid-Figueroa H, Gutiérrez JP. Parent-adolescent communication about sex in Morelos, Mexico: does it impact sexual behaviour? Eur J Contracept Reprod Health Care. 2009;14(2):111–119. doi:10.1080/13625180802691848
47. Rogers AA, Ha T, Stormshak EA, Dishion TJ. Quality of parent-adolescent conversations about sex and adolescent sexual behavior: an observational study. J Adolesc Health. 2015;57(2):174–178. doi:10.1016/j.jadohealth.2015.04.010
48. Liu YL. Parent–child interaction and children’s depression: the relationships between Parent-Child interaction and children’s depressive symptoms in Taiwan. J Adolesc. 2003;26(4):447–457. doi:10.1016/S0140-1971(03)00029-0
49. Chiariello MA, Orvaschel H. Patterns of parent-child communication: relationship to depression. Clin Psychol Rev. 1995;15(5):395–407. doi:10.1016/0272-7358(95)00022-h
50. Levin KA, Currie C. Family structure, mother-child communication, father-child communication, and adolescent life satisfaction: a cross-sectional multilevel analysis. Health Educ. 2010;110(3):152–168. doi:10.1108/09654281011038831
51. Bireda AD, Pillay J. Perceived parent-child communication and well-being among Ethiopian adolescents. Int J Adolesc Youth. 2018;23(1):109–117. doi:10.1080/02673843.2017.1299016
52. Sallinen M, Rönkä A, Kinnunen U, Kokko K. Trajectories of depressive mood in adolescents: does parental work or parent-adolescent relationship matter? A follow-up study through junior high school in Finland. Int J Behav Dev. 2007;31(2):181–190. doi:10.1177/0165025407074631
53. Ho DYF. Fatherhood in Chinese culture. In: The Father’s Role: Cross-Cultural Perspectives. Routledge; 1987:227–245.
54. Shek DTL. Paternal and maternal influences on the psychological well-being of Chinese adolescents. Genet Soc Gen Psychol Monogr. 1999;125(3):269.
55. Liu M, Chen X, Rubin KH, et al. Autonomy-vs. connectedness-oriented parenting behaviours in Chinese and Canadian mothers. Int J Behav Dev. 2005;29(6):489–495. doi:10.1177/01650250500147063
56. Huang Q, Sun J, Tang Y. Chinese parents’ scaffolding and children’s initiative in mother–child and father–child interactions across different types of problem-solving activities. Early Educ Dev. 2021;32(2):249–271. doi:10.1080/10409289.2020.1752591
57. Grossmann K, Grossmann KE, Fremmer-Bombik E, Kindler H, Scheuerer-Englisch H, Zimmermann P. The uniqueness of the child-father attachment relationship: fathers’ sensitive and challenging play as a pivotal variable in a 16-year longitudinal study. Soc Dev. 2002;11(3):301–337. doi:10.1111/1467-9507.00202
58. Lamb ME, Lewis C. Father-child relationships. In: Handbook of Father Involvement: Multidisciplinary Perspectives. Routledge; 2013:119–135.
59. López EE, Ochoa GM, Olaizola JH. The role of family communication and school adjustment on adolescent mental health. Salud Mental. 2005;28(4):81–89.
60. Wilson KR, Prior MR. Father involvement and child well-being. J Paediatr Child Health. 2011;47(7):405–407. doi:10.1111/j.1440-1754.2010.01770.x
61. Shek TL, Sun RCF. Parenting in Hong Kong: traditional Chinese cultural roots and contemporary phenomena. In: Parenting Across Cultures: Childrearing, Motherhood and Fatherhood in Non-Western Cultures. Springer; 2014:25–38.
62. Cambron MJ, Acitelli LK, Steinberg L. When friends make you blue: the role of friendship contingent self-esteem in predicting self-esteem and depressive symptoms. Pers Soc Psychol Bull. 2010;36(3):384–397. doi:10.1177/0146167209351593
63. Cattelino E, Chirumbolo A, Baiocco R, Calandri E, Morelli M. School achievement and depressive symptoms in adolescence: the role of self-efficacy and peer relationships at school. Child Psychiatry Hum Dev. 2021;52(4):571–578. doi:10.1007/s10578-020-01043-z
64. Yang Y, Chen L, Zhang L, Ji L, Zhang W. Developmental changes in associations between depressive symptoms and peer relationships: a four-year follow-up of Chinese adolescents. J Youth Adolesc. 2020;49(9):1913–1927. doi:10.1007/s10964-020-01236-8
65. Kutsyuruba B, Klinger DA, Hussain A. Relationships among school climate, school safety, and student achievement and well-being: a review of the literature. Rev Educ. 2015;3(2):103–135. doi:10.1002/rev3.3043
66. Kent BV, Bradshaw M. Adolescent context and depressive symptom trajectories in a national sample: ages 13 to 34. Int J Ment Health Addict. 2020;1–17. doi:10.1007/s11469-020-00236-w
67. Mizuta A, Suzuki K, Yamagata Z, Ojima T. Teachers’ support and depression among Japanese adolescents: a multilevel analysis. Soc Psychiatry Psychiatr Epidemiol. 2017;52(2):211–219. doi:10.1007/s00127-016-1320-6
68. Li W, Gao WY, Fu WD. When does teacher support reduce depression in students? The moderating role of students’ status as left-behind children. Front Psychol. 2021;12:42. doi:10.3389/fpsyg.2021.608359
69. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310. doi:10.1037/0033-2909.98.2.310
70. Mageau GA, Vallerand RJ. The coach–athlete relationship: a motivational model. J Sports Sci. 2003;21(11):883–904. doi:10.1080/0264041031000140374
71. Joyce HD. Does school connectedness mediate the relationship between teacher support and depressive symptoms? Child Sch. 2019;41(1):7–16. doi:10.1093/cs/cdy024
72. Shokeen A. A study of mental health and social adjustment of senior secondary students. Educ Appl Soc Sci. 2017;8(1):33–36. doi:10.5958/2230-7311.2017.00006.X
73. Roorda DL, Koomen HMY, Spilt JL, et al. The influence of affective teacher–student relationships on students’ school engagement and achievement: a meta-analytic approach. Rev Educ Res. 2011;81(4):493–529. doi:10.3102/0034654311421793
74. Sun Y, Qiu Y. Teacher-student relationship: the support source of junior middle school students school adjustment. J Northeast Normal Univ. 2010;157–160. doi:10.16164/j.cnki.22-1062/c.2010.02.029
75. Longobardi C, Prino LE, Marengo D, et al. Student-teacher relationships as a protective factor for school adjustment during the transition from middle to high school. Front Psychol. 2016;7:1988. doi:10.3389/fpsyg.2016.01988
76. Cattley G. The impact of teacher-parent-peer support on students’ well-being and adjustment to the middle years of schooling. Int J Adolesc Youth. 2004;11(4):269–282. doi:10.1080/02673843.2004.9747935
77. Au RCP, Watkins D, Hattie J, Alexander P. Reformulating the depression model of learned hopelessness for academic outcomes. Educ Res Rev. 2009;4(2):103–117. doi:10.1016/j.edurev.2009.04.001
78. Sideridis GD. Understanding low achievement and depression in children with learning disabilities: a goal orientation approach. Int Rev Res Ment Retard. 2006;31:163–203. doi:10.1016/S0074-7750(05)31005-6
79. Spreen O. The relationship between learning disability, emotional disorders, and neuropsychology; some results and observations. J Clin Exp Neuropsychol. 1989;11(1):117–140. doi:10.1080/01688638908400880298-306
80. Van Voorhees BW, Paunesku D, Kuwabara SA, et al. Protective and vulnerability factors predicting new-onset depressive episode in a representative of US adolescents. J Adolesc Health. 2008;42(6):605–616. doi:10.1016/j.jadohealth.2007.11.135
81. Westrick PA, Le H, Robbins SB, Radunzel JM, Schmidt FL. College performance and retention: a meta-analysis of the predictive validities of ACT® scores, high school grades, and SES. Educ Assess. 2015;20(1):23–45. doi:10.1080/10627197.2015.997614
82. Marsh HW, Trautwein U, Lüdtke O, Koller O, Baumert J. Academic self-concept, interest, grades, and standardized test scores: reciprocal effects models of causal ordering. Child Dev. 2005;76(2):397–416. doi:10.1111/j.1467-8624.2005.00853.x
83. Wigfield A, Eccles JS. The development of competence beliefs, expectancies for success, and achievement values from childhood through adolescence. Dev Achievement Motivation. 2002;91–120. doi:10.1016/b978-012750053-9/50006-1
84. Shi Y, Zhang L, Ma Y, et al. Dropping out of rural China’s secondary schools: a mixed-methods analysis. China Q. 2015;224:1048–1069. doi:10.1017/s0305741015001277
85. Zhang Q. Family communication patterns and conflict styles in Chinese parent-child relationships. Commun Q. 2007;55(1):113–128. doi:10.1080/01463370600998681
86. Zhang Q, Wills M. A US-Chinese comparison of affectionate communication in parent-child relationships. Commun Res Rep. 2016;33(4):317–323. doi:10.1080/08824096.2016.1224166
87. Ng QX, Lim DY, Chee KT. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020;22(6):638–639. doi:10.1111/bdi.12960
88. McCauley E, Pavlidis K, Kendall K. Developmental precursors of depression: the child and the social environment; 2001.
89. Kapetanovic S, Rothenberg WA, Lansford JE, et al. Cross-cultural examination of links between parent–adolescent communication and adolescent psychological problems in 12 cultural groups. J Youth Adolesc. 2020;49(6):1225–1244. doi:10.1007/s10964-020-01212-2
90. Zhang Q, Shek DTL, Pan Y. Parent-child discrepancies in perceived parent-child communication and depressive symptoms in early adolescents in China. Int J Environ Res Public Health. 2021;18(22):12041. doi:10.3390/ijerph182212041
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.