")
Back to Journals » International Journal of General Medicine » Volume 15
The Relationship Between Lateral Femoral Condyle Index and Noncontact Anterior Cruciate Ligament Rupture
Authors Li R , Zhang J, Chen X, Fang Z
Received 2 December 2021
Accepted for publication 2 February 2022
Published 18 February 2022 Volume 2022:15 Pages 1789—1794
DOI https://doi.org/10.2147/IJGM.S347742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ruibo Li, Jianjun Zhang, Xi Chen, Zhi Fang
Department of Orthopaedics, Peoples’ Hospital of Deyang City, Deyang, 618000, Sichuan Province, People’s Republic of China
Correspondence: Ruibo Li; Xi Chen, Department of Orthopaedics, Peoples’ Hospital of Deyang City, No. 173, Section 3, North Taishan Road, Deyang, 618000, Sichuan Province, People’s Republic of China, Tel +86 18280366719 ; +86 8382148102, Email [email protected]; [email protected]
Purpose: The purpose of this study was to examine the relationship between distal femoral morphology and noncontact anterior cruciate ligament (ACL) rupture and the differences between digital X-ray imaging systems (DR) and magnetic resonance imaging (MRI) to evaluate distal femoral morphology.
Methods: A retrospective case-control study was performed on 120 patients. Two age- and sex-matched cohorts (each n = 60) were analyzed: primary ACL ruptures and a control group consisting of isolated meniscal tears. The lateral femoral condyle index (LFCI) was measured by DR and by MRI to quantify femoral sphericity. Differences among two groups were compared, and diagnostic performance of the risk factors was assessed. In addition, differences between DR and MRI to evaluate LFCI were examined.
Results: The LFCI by MRI was smaller in the knees with primary ACL rupture (median, 0.71; range, 0.62– 0.78) than that of the control group (median, 0.77; range, 0.66– 0.85) (p < 0.01). The LFCI was also significantly smaller in the knees with primary ACL rupture (median, 0.72; range, 0.63– 0.77) than that of the control group (median, 0.79; range, 0.65– 0.84) (p < 0.01) by DR. A cutoff of 0.74 of MRI yielded a sensitivity of 77% and a specificity of 78% to predict an ACL rupture, and of 0.75 of DR yield a sensitivity of 87% and a specificity of 77% to predict an ACL rupture.
Conclusion: This study showed that a decreased LFCI is associated with an ACL rupture, and both DR and MRI measurements can effectively predict the risk of ACL rupture. This helps expand the scope of the application of the LFCI and helps clinicians identify susceptible individuals who may benefit from targeted ACL rupture prevention counseling and intervention.
Keywords: anterior cruciate ligament, knee, lateral femoral condyle, femur
Introduction
Anterior cruciate ligament (ACL) rupture is common in young and active patients, and it can seriously affect the quality of life of young patients and athletes, bringing a certain social and economic burden.1–3 Some studies suggest that the causes of ACL injuries are related to social, environmental, anatomical, hormonal, neuromuscular and biomechanical factors.4–6 Anatomic factors such as the angle of the tibial plateau retrograde, the width of the intercondylar fossa of the femur, and the matching relationship between the tibial plateau and the femoral condyle have been proved to have a clear correlation with the rupture of the ACL.7,8 Although posterior femoral condylar offset reportedly influences range of motion and other aspects of knee joint kinematics, and this offset has an influence on ACL rupture,9–11 there is still a lack of independent and accurate method to evaluate the shape of femoral condyle.
Hodel et al quantified posterior femoral condylar depth as the lateral femoral condyle index (LFCI), and demonstrated that the decreased LFCI is a risk factor for primary ACL rupture.12 However, due to the high cost of MRI, this method is difficult to be widely applied, and the sample size of previous studies is small, so further study is still needed.
The principal aim of this study was to assess the relationship between LFCI and primary ACL rupture. The secondary aim was to compare the accuracy of measurement by MRI with that by DR.
Materials and Methods
A retrospective analysis was performed on 420 patients who received arthroscopic knee surgery for non-contact simple ACL rupture or isolated meniscus tear in authors’ hospital from 2015 to 2018, and they were divided into 2 groups: (1) primary ACL ruptures, (2) a control group consisting of patients with isolated meniscal tears. The ACL rupture cases were matched to control group according to sex and age and then assessed for the eligibility criteria listed in Figure 1. The minimum follow-up time was 24 months for all the patients. All patients underwent preoperative X-ray and MRI examination, and were evaluated by radiologists and surgeons to determine the presence of ACL rupture or meniscus tear. All patients included in the study underwent knee arthroscopy, and the presence of combined injury was reconfirmed during the operation.
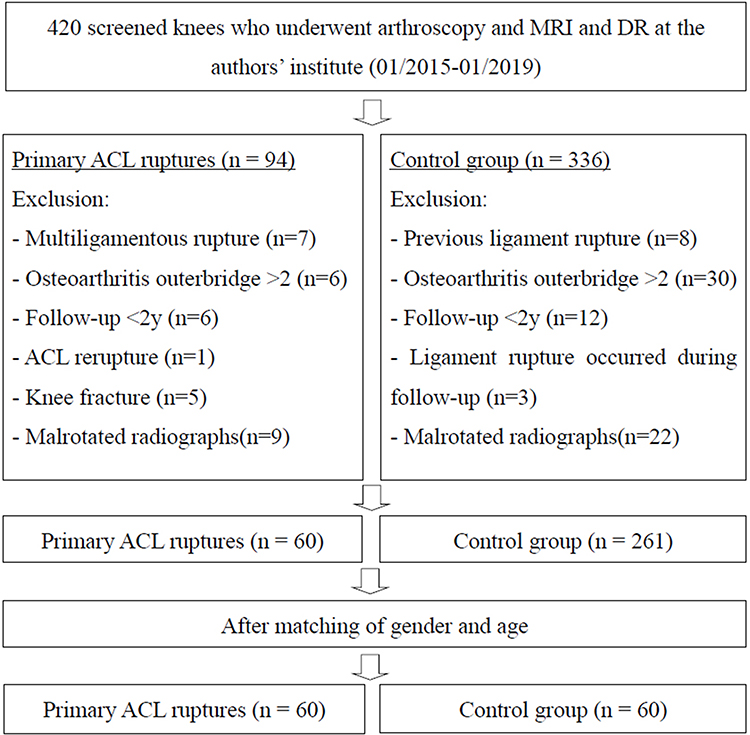 |
Figure 1 Flowchart and eligibility. Abbreviations: ACL, anterior cruciate ligament; MRI, magnetic resonance imaging; DR, digital X-ray imaging systems. |
MRI Measurements
All patients enrolled in the study underwent MRI 3.0T (Philips Ingenia 3T) examination before surgery. The imaging consisted of three standard imaging planes (sagittal, coronal, and cross-sectional), each of which was 3mm thick. Measurement of LFCI based on the method proposed by Hodel12 (Figure 2).
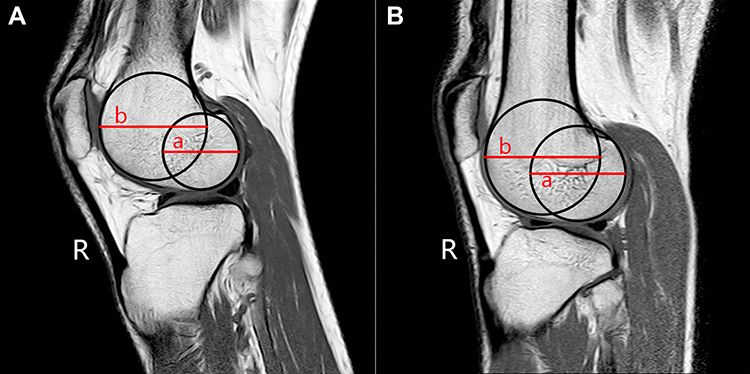 |
Figure 2 Lateral femoral condyle index (LFCI) measurement by MRI. On the midsagittal image of the lateral condyle, the anterior and posterior profiles of the lateral condyle of the femur are approximately circular. The best-fitting circle is drawn to the subchondral bone from most inferior point to most anterior point (extension circle, b)-respectively, most inferior point and most posterior point (flexion circle, a)- and give them the most consistent overlap with the spherical profile of the lateral condyle of the femur. The diameter of the flexion circle was divided by the diameter of the extension circle to calculate the LFCI as follows: LFCI = a/b. Example of LFCI in (A) ACL rupture group of 0.69 and (B) control group of 0.83. |
DR Measurements
All patients completed lateral X-ray images of the knee using the Siemens DR system, and the knee flexion was 30°. According to the calculation method of Pfeiffer et al,10 X-ray images of the medial and lateral femoral condyle and posterior condyle overlap <6mm were included in the study (Figure 3).
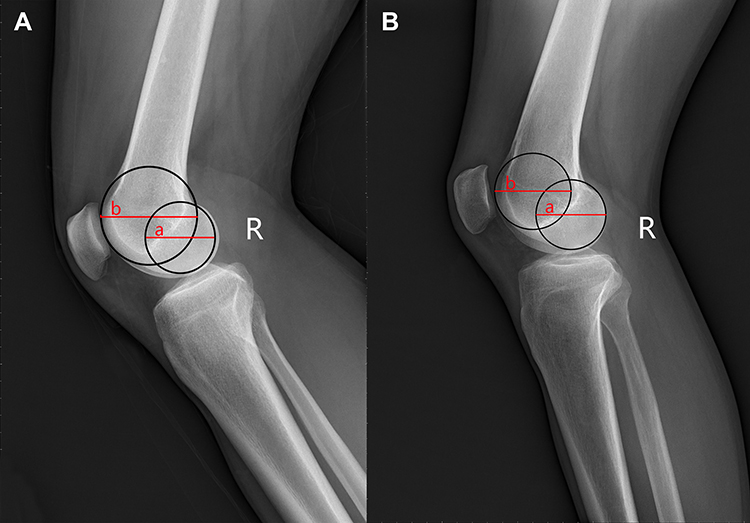 |
Figure 3 Lateral femoral condyle index (LFCI) measurement by DR. The best-fitting circle is drawn to the subchondral bone with reference to the method of MRI measurement, and the LFCI was calculated as follows: LFCI = a/b. Example of LFCI in (A) ACL rupture group of 0.69 and (B) control group of 0.89. |
Statistical Analysis
Statistical analyses were performed using SPSS software (version 24; IBM). According to the preliminary results, G*power (version 3.1.9.4; Franz Faul) was used to calculate the sample size of at least 29 patients in each group (α, 0.05; power, 0.8). Case controls were matched by sex (exact match) and age (maximum fluctuation range within 2 years). Students t test was used to analyze the differences between groups, and to analyze whether there are differences in ACL rupture prediction based on MRI and DR. The receiver operating characteristic curve (ROC) was used to determine the optimal threshold of femoral condyle index to predict ACL rupture. The Youden index was used to determine the ideal critical points for sensitivity and specificity.
Results
A total of 120 patients who met the inclusion criteria were included in the final analysis (60 with primary ACL rupture, 60 controls). Each group consisted of 44 male patients and 12 female patients. The median age of the ACL rupture group was 35 years old (range, 21–56), while the median age of the control group was 37 years old (range, 22–55).
Measurements by MRI: The LFCI was smaller in the knees with primary ACL rupture (median, 0.71; range, 0.62–0.78) than that of the control group (median, 0.77; range, 0.66–0.85) (p<0.01). The area under the curve (AUC) was 0.83 (95% CI, 0.73–0.94), with a sensitivity of 77% and specificity of 78% to predict an ACL rupture. The calculated cutoff of 0.74 (Youden index, 0.53) was associated with an increased risk for ACL rupture.
Measurements by DR: The LFCI was also significantly smaller in the knees with primary ACL rupture (median, 0.72; range, 0.63–0.77) than that of the control group (median, 0.79; range, 0.65–0.84) (p < 0.01). The AUC was 0.84 (95% CI, 0.73–0.95), with a sensitivity of 87% and specificity of 77% to predict an ACL rupture. The calculated cutoff of 0.75 (Youden index, 0.63) was associated with an increased risk for ACL rupture.
Discussion
Data from this study showed that a decrease in the LFCI was associated with an increased risk of ACL rupture. Specifically, patients with primary non-contact ACL rupture had a smaller index of the external femoral condyle than the control group. Moreover, the critical value of MRI measurement is 0.74, the critical value of DR is 0.75, Both MRI and DR measurements have good diagnostic value.
It has been shown that there is a significant relationship between the shape of the distal femur and the movement of the knee joint. The asymmetry of the internal and external condyles of the distal femur contributes to the rotation of the knee joint during flexion and extension.13–16 The increase in the depth of the posterior condyle of the femur will lead to the increase in the length of the lateral and anterolateral knee joint structures, so there will be greater asymmetry and increased degree of rotation in the flexion of the knee joint, which may increase the risk of ACL rupture.10,16
Fernandes et al17 have confirmed that the increase in antepartum diameter of the lateral femoral condyle can increase the risk of ACL rupture, and the study by Pfeiffer and Burnham9,10 showed that the increase in posterior condylar depth of the lateral femoral condyle can also increase the risk of ACL rupture.
In this study, we refer to Hodel’s method to transform the hemispheric shape of the lateral femoral condyle into the LFCI.12 We found that the smaller the LFCI, the higher the risk of ACL rupture. The higher LFCI, the more consistent anterior and posterior femoral condyle. The smaller the LFCI, the more prominent the posterior femoral condyle. Therefore, the smaller the femoral condyle index is, the larger the offset the femoral condyle is. This asymmetry might be associated with more excessive gliding of the flattened anterior part of the condyle over the convex lateral tibial plateau, thereby resulting in a greater pivoting mechanism.12 The authors of this study confirmed in previous studies that a higher ratio of anteroposterior diameter to height of the lateral femoral condyle was associated with a greater risk of ACL injury.18 Therefore, when LFCI decreases, the risk of ACL fracture will increase.
The advantage of the LFCI lies in its independence in evaluating the hemispheric morphology of lateral condyle of femur, which is not affected by the morphology of tibia. In order to expand its clinical application, we simultaneously measured the lateral DR images of the knee of the same patients, and the statistical analysis results showed that the results obtained by MRI were similar to those obtained by DR. Both DR and MRI measurements can effectively predict the risk of ACL rupture and the critical value of LFCI that increases the risk of ACL rupture. Therefore, future studies or clinical applications can consider using knee joint DR for evaluation, because DR costs less, is more acceptable, and has a wider range of applications, making it more suitable for screening patients at risk of ACL rupture. This helps expand the scope of the application of the LFCI and helps clinicians identify individuals susceptible to ACL rupture. At the same time, it may help clinicians to formulate ACL reconstruction strategies and plans more accurately and reduce the risk of ACL re-rupture after reconstruction.
Limitations of this study include the retrospective nature. Although accurate matches were made, the measurement results are still biased to some extent. Prospective studies with a larger sample size are needed in the future to better evaluate the relationship between hemispheric morphology of the lateral femoral condyle and ACL rupture.
Conclusions
This study showed that a decreased LFCI is associated with an ACL rupture, and both DR and MRI measurements can effectively predict the risk of ACL rupture. This helps expand the scope of the application of the LFCI and helps clinicians identify susceptible individuals who may benefit from targeted ACL rupture prevention counseling and intervention.
Abbreviations
ACL, anterior cruciate ligament; DR, digital X-ray imaging systems; MRI, magnetic resonance imaging; LFCI, lateral femoral condyle index.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Human Investigation Committee of Deyang People’s Hospital (No. 2021-04-013-K01). Due to the study was a retrospective analysis, patient consent to review their medical records was not required by the Human Investigation Committee of Deyang People’s Hospital. All data were anonymized to comply with the provisions of personal data protection legislation. This study adhered to the tenets of the Declaration of Helsinki.
Funding
There was no funding/support for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Saltzman BM, Cvetanovich GL, Nwachukwu BU, Mall NA, Bush-Joseph CA, Bach BR. Economic analyses in anterior cruciate ligament reconstruction: a qualitative and systematic review. Am J Sports Med. 2016;44(5):1329–1335. doi:10.1177/0363546515581470
2. Mather RC, Koenig L, Kocher MS, et al. Societal and economic impact of anterior cruciate ligament tears. J Bone Joint Surg Am. 2013;95(19):1751–1759. doi:10.2106/JBJS.L.01705
3. Essen C, McCallum S, Barenius B, Eriksson K. Acute reconstruction results in less sick-leave days and as such fewer indirect costs to the individual and society compared to delayed reconstruction for ACL injuries. Knee Surg Sports Traumatol Arthrosc. 2020;28(7):2044–2052. doi:10.1007/s00167-019-05397-3
4. Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8(3):141–150. doi:10.5435/00124635-200005000-00001
5. Zebis MK, Andersen CH, Bencke J, et al. Neuromuscular coordination deficit persists 12 months after ACL reconstruction but can be modulated by 6 weeks of Kettlebell training: a case study in women’s Elite Soccer. Case Rep Orthop. 2017;2017:1–7. doi:10.1155/2017/4269575
6. Faltstrom A, Hagglund M, Magnusson H, Forssblad M, Kvist J. Predictors for additional anterior cruciate ligament reconstruction: data from the Swedish national ACL register. Knee Surg Sports Traumatol Arthrosc. 2016;24(3):885–894. doi:10.1007/s00167-014-3406-6
7. Eck CF, Martins CAQ, Vyas SM, Celentano U, Dijk CN, Fu FH. Femoral intercondylar notch shape and dimensions in ACL-injured patients. Knee Surg Sports Traumatol Arthrosc. 2010;18(9):1257–1262. doi:10.1007/s00167-010-1135-z
8. Vasta S, Andrade R, Pereira R, et al. Bone morphology and morphometry of the lateral femoral condyle is a risk factor for ACL injury. Knee Surg Sports Traumatol Arthrosc. 2018;26(9):2817–2825. doi:10.1007/s00167-017-4761-x
9. Burnham JM, Pfeiffer T, Shin JJ, Herbst E, Fu FH. Bony morphologic factors affecting injury risk, rotatory stability, outcomes, and re-tear rate after anterior cruciate ligament reconstruction. Ann Joint. 2017;2(44):1–10. doi:10.21037/aoj.2017.06.11
10. Pfeiffer TR, Burnham JM, Hughes JD, Kanakamedala AC, Musahl V. An increased lateral femoral condyle ratio is a risk factor for anterior cruciate ligament injury. J Bone Joint Surg Am Vol. 2018;100(10):857–864. doi:10.2106/JBJS.17.01011
11. Grassi A, Signorelli C, Urrizola F, et al. Anatomical features of tibia and femur: influence on laxity in the anterior cruciate ligament deficient knee. Knee. 2018;25(4):577–587. doi:10.1016/j.knee.2018.03.017
12. Hodel S, Kabelitz M, Tondelli T, Vlachopoulos L, Sutter R, Fucentese S. Introducing the lateral femoral condyle index as a risk factor for anterior cruciate ligament injury. Am J Sports Med. 2019;47(10):2420–2426. doi:10.1177/0363546519858612
13. Eckhoff D, Dwyer T, Bach J, Spitzer V, Reinig K. Three-dimensional morphology of the distal part of the femur viewed in virtual reality. J Bone Joint Surg Am. 2001;83(2):43–50. doi:10.2106/00004623-200100021-00010
14. Eckhoff DG, Bach JM, Spitzer VM, et al. Three-dimensional mechanics, kinematics, and morphology of the knee viewed in virtual reality. J Bone Joint Surg Am. 2005;87(Suppl 2):71–80. doi:10.2106/JBJS.E.00440
15. Eckhoff DG, Bach JM, Spitzer VM, et al. Three-dimensional morphology and kinematics of the distal part of the femur viewed in virtual reality. Part II. J Bone Joint Surg Am. 2003;85-A(Suppl 4):97–104. doi:10.2106/00004623-200300004-00012
16. Pfeiffer T, Burnham J, Herbst E, Shafizadeh S, Musahl V. A Tomahawk shape of the femur predicts greater rotatory knee laxity in patients with anterior cruciate ligament ruptures. Orthop J Sports Med. 2018;6(4suppl2). doi:10.1177/2325967118S00030
17. Fernandes MS, Pereira R, Andrade R, et al. Is the femoral lateral condyle’s bone morphology the trochlea of the ACL? Knee Surg Sports Traumatol Arthrosc. 2017;25(1):1–8. doi:10.1007/s00167-016-4159-1
18. Li R, Yuan X, Fang Z, Liu Y, Chen X, Zhang J. A decreased ratio of height of lateral femoral condyle to anteroposterior diameter is a risk factor for anterior cruciate ligament rupture. BMC Musculoskelet Disord. 2020;21(1):402. doi:10.1186/s12891-020-03440-w
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.