")
Back to Journals » Psychology Research and Behavior Management » Volume 13
The Relationship Between Care Burden and Coping Strategies in Caregivers of Hemodialysis Patients in Kermanshah, Iran
Authors Menati L, Torabi Y , Andayeshgar B , Khatony A
Received 1 October 2019
Accepted for publication 21 January 2020
Published 5 February 2020 Volume 2020:13 Pages 133—140
DOI https://doi.org/10.2147/PRBM.S233103
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Lida Menati,1 Yousef Torabi,2 Bahare Andayeshgar,1 Alireza Khatony3
1Clinical Research Development Center, Imam Reza Hospital, Kermanshah University of Medical Sciences, Kermanshah, Iran; 2Student Research Committee, Kermanshah University of Medical Sciences, Kermanshah, Iran; 3Infectious Diseases Research Center, Kermanshah University of Medical Sciences, Kermanshah, Iran
Correspondence: Alireza Khatony
Clinical Research Development Center, Imam Reza Hospital, Kermanshah, Iran
Tel/Fax +98 38 279 394
Email [email protected]
Objective: The purpose of this study was to investigate the relationship between care burden and coping strategies in caregivers of hemodialysis patients.
Methods: This cross-sectional survey was conducted from September to December 2018 in Kermanshah, Iran. A total of 130 caregivers of patients admitted to the hemodialysis wards of Imam Reza and Imam Khomeini hospitals of Kermanshah, Iran were selected via convenience sampling. Data-collection tools included a demographic information form, caregiver-burden inventory, and coping inventory for stressful situations. Data were analyzed using descriptive and analytical tests.
Results: The mean age of the caregivers was 35.8± 13.7 years, and 71 (54.6%) were patients’ children. The mean caregiver-burden score was 58.5± 20.5 out of 96. Mean scores of time-dependent, evolutionary, physical, social, and emotion-dependent care burdens were 17.5± 5.3, 12.2± 6.3, 9.1± 4.7, 8.2± 4.0, and 11.4± 5.1, respectively. Mean scores of problem-focused, emotion-focused, and avoidance-oriented coping strategies were 46.0± 80.8, 43.1± 9.0, and 48.9± 9.5, respectively. Among the strategies, only the avoidance-oriented one had a significant positive relationship with total care burden and all its subscales.
Conclusion: Caregivers of hemodialysis patients experienced a relatively high care burden. However, they did not use appropriate coping strategies; therefore, they should be trained to select an effective coping strategy.
Keywords: avoidance-oriented coping strategy, burden, coping, family caregiver, hemodialysis
Introduction
Chronic kidney disease is a major and growing health concern worldwide.1 Based on data published in 2016, there were an estimated that 750 million people suffering from chronic kidney disease worldwide, about 3 million of whom were on dialysis.2 Hemodialysis reduces patients’ energy levels and affects their ability to work and perform daily activities, resulting in the disruption of patients' and caregivers’ daily routines.3 Chronic disorders and their associated psychological and financial complications in a family member can affect the entire family.4 Caregivers of hemodialysis patients are often family members or friends of patients, providing physical, mental, and social support.5,6 It is known that caregivers of hemodialysis patients experience a high level of care burden.7,8
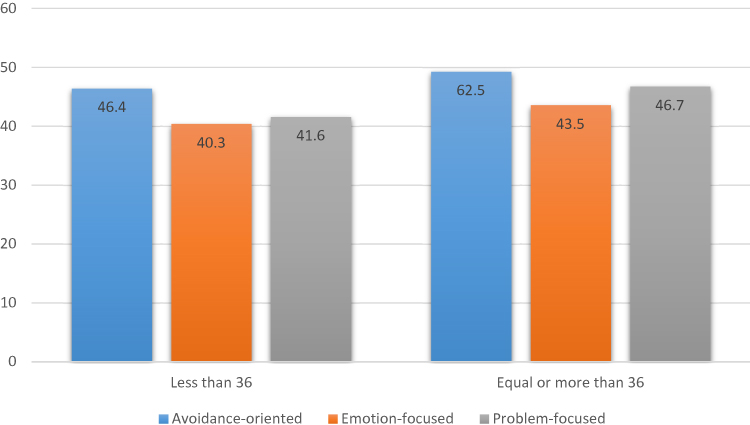 |
Figure 1 Comparison of coping strategies in caregivers of hemodialysis patients. |
Care burden is an uncomfortable experience for caregivers of patients, involving financial, social, psychological, and physical dimensions.9 It has been shown that some caregivers of hemodialysis patients are under a great care burden.9,10 Acceptance of the caregiver role and its associated changes, besides its positive effects on the patient and his/her family, can cause several negative consequences, such as reduced physical and mental health and worsened social relationships among caregivers. It can also cause a wide range of physical, emotional, and psychological problems for caregivers, exposing them to a variety of physical and psychological hazards.11
Family disruption, inadequate patient care, and ultimately lack of attention to the patient are other negative consequences of care burden.12–14 Care burden can also have devastating effects on caregivers and expose them to various diseases. The burden experienced by caregivers can lead to serious diseases,8 which are often overlooked.15 People usually use coping strategies in the face of stressful situations to reduce or manage them.10 Coping strategies generally include problem-focused, emotion-focused, and avoidance-oriented coping strategies.16,17
Problem-focused coping refers to deliberate efforts to solve a problem, reorganize the problem, or change the situation. Emotion-focused coping refers to emotional responses aimed at reducing stress, rather than rational problem-solving. On the other hand, avoidance-oriented coping is a set of behaviors to avoid a stressful situation by ignoring the problem or turning to the community as a means to relieve the stress.18,19 Among these coping strategies, the problem-focused strategy has a positive relationship with mental health. There is also an inverse relationship between mental health and emotion-focused coping.20
In this regard, Abbasi et al suggested that use of emotion-focused coping strategies by caregivers increases their care burden.21 Moreover, Myaskovsky et al indicated that caregivers who used emotion-focused coping strategies had a low quality of life.22 According to Abbasi et al, which was based on a study by Ardashirzade et al, there was a direct relationship between high care burden and use of emotion-focused coping strategies.21
The present study was designed and conducted considering the importance of maintaining and improving the physical and mental health of hemodialysis patients’ caregivers and lack of knowledge about the care burden and coping strategies of these caregivers. The aim of this study was to determine the relationship between coping strategies and care burden among caregivers of hemodialysis patients. We aimed to answer the following questions:
- What is the level of care burden in caregivers of hemodialysis patients?
- What are the most common coping strategies used by caregivers of hemodialysis patients?
- What kind of relationship is there between care burden and coping strategies in caregivers of hemodialysis patients?
Methods
Study Design
This cross-sectional study was conducted from September to December 2018 in Kermanshah, Iran.
Sample and Sampling Method
The study population included all caregivers of patients admitted to the hemodialysis wards of Imam Reza and Imam Khomeini hospitals. Sample size was estimated at 130, based on Jafari et al,9 who reported the proportion of caregivers under a care burden to be 0.374. Using the sample-size formula n=Z2pq/d2), the study had 95% confidence and error of 0.222×P. P represented the sample proportion, and was measured to be 0.387. Inclusion criteria were consent to participate in the study, ability to read and write, and direct responsibility for care of the patient. Convenience sampling was applied in this study.
Instrument
Data-collection tools comprised a personal information form, Caregiver Burden Inventory (CBI),23 and Coping Inventory for Stressful Situations (CISS).24 The personal information form for caregivers included six questions on age, sex, marital status, education, occupation, and relationship with the patient. Moreover, it included seven questions on age, sex, marital status, education, place of residence, occupation, and time on dialysis.
The CBI was designed by Novak and Guest in 1989,23 and its internal consistency was investigated by McCleery et al using Cronbach’s α (0.8).25 The Persian version of the CBI has been also validated in Iran by Abbasi et al, who reported a Cronbach’s α of 0.9.3 The CBI is a five-item scale with five subscale: time dependence (amount of time a caregiver spends daily on patient care), developmental (pressure during various stages of a caregiver’s life, such as puberty, due to caring for the patient), physical (physical strain and exhaustion experienced by the caregiver during patient care), social (burden of care that affects the social aspects of the caregiver’s life during patient care), and emotional (caregiving pressure that affects the caregiver’s emotions and feelings) care burdens. CBI items are scored on a five-point Likert scale: 0 = never, 1 = rarely, 2 = occasionally, 3 = frequently, and 4 = almost always. The total score ranges from 0 to 96, with scores >36 indicating a high care burden.23
The CISS was used to measure the frequency of coping strategies used by caregivers. This scale was designed by Andler and Parker to evaluate the types of coping strategies in stressful situations.24 The reliability of the CISS was evaluated by Hurt et al using Cronbach’s α and test–retest methods.26 The Persian version of the CISS has was also psychometrically evaluated by Shokri et al, and its internal consistency has been investigated using Cronbach’s α (0.75, 0.82, and 0.73 for problem-focused, emotion-focused, and avoidance strategies, respectively).26
The CISS is a 48-item scale containing 16 questions on problem-focused, emotion-focused, and avoidance-oriented coping strategies. It is scored on a five-point Likert scale: 1 = never, 2 = sometimes, 3 = usually, 4 = most often, and 5 = always. Problem-focused, emotion-focused, and avoidance coping strategies are scored from 16 to 80. The individual’s score represents the dominant coping strategy. In other words, each coping strategy with the highest score is used by the caregiver. Also, obtaining the same score for two strategies indicates the use of both strategies.24
Data Gathering
After obtaining approval from the ethics committee of the university, we visited the hemodialysis wards of Imam Reza and Imam Khomeini hospitals. The research objectives were explained to the participants. They also received information on how to complete the questionnaires. Finally, those who met the inclusion criteria were included in the study. The time and place for completing the questionnaires were different for the caregivers and patients. Questionnaires were then presented to the participants and collected after they had been completed.
Data Analysis
Data were analyzed in SPSS 16.0 using descriptive and inferential statistics. First, the Kolmogorov–Smirnov test was used to examine the normal distribution of care burden and coping strategies. The results of this test indicated that these variables had no normal distribution. The Mann–Whitney U test was also used to investigate the relationship between care burden and two-dimensional qualitative variables. Moreover, Spearman’s rank correlation coefficient was measured to examine the correlation of care burden and its subscales with the type of coping strategy.
Ethical Considerations
The Ethics Committee of Kermanshah University approved this study. Written informed consent was obtained from all participants, and they were assured of the confidentiality of their information. Three of the caregivers were aged <18 years and were able to consent on their own behalf. Participants were informed about the study objectives, and their questions were answered.
Results
The mean age of the caregivers was 35.8±13.7 years. A total of 82 (63.1%) caregivers were female, 63 (48.5%) married, 42 (32.3%) housewives, and 65 (50%) had a university education. In sum, 71 (54.6%) caregivers were the patients’ children. In terms of patients’ personal information, the mean age of hemodialysis patients was 58.7±15.1 years. The results showed that 76 (58.1%) patients were female, 105 (81.0%) married, 62 (48.4%) housewives, and 52 (44.4%) a had primary education. Also, 49 (43.8%) patients had a time on dialysis <20 months (Table 1).
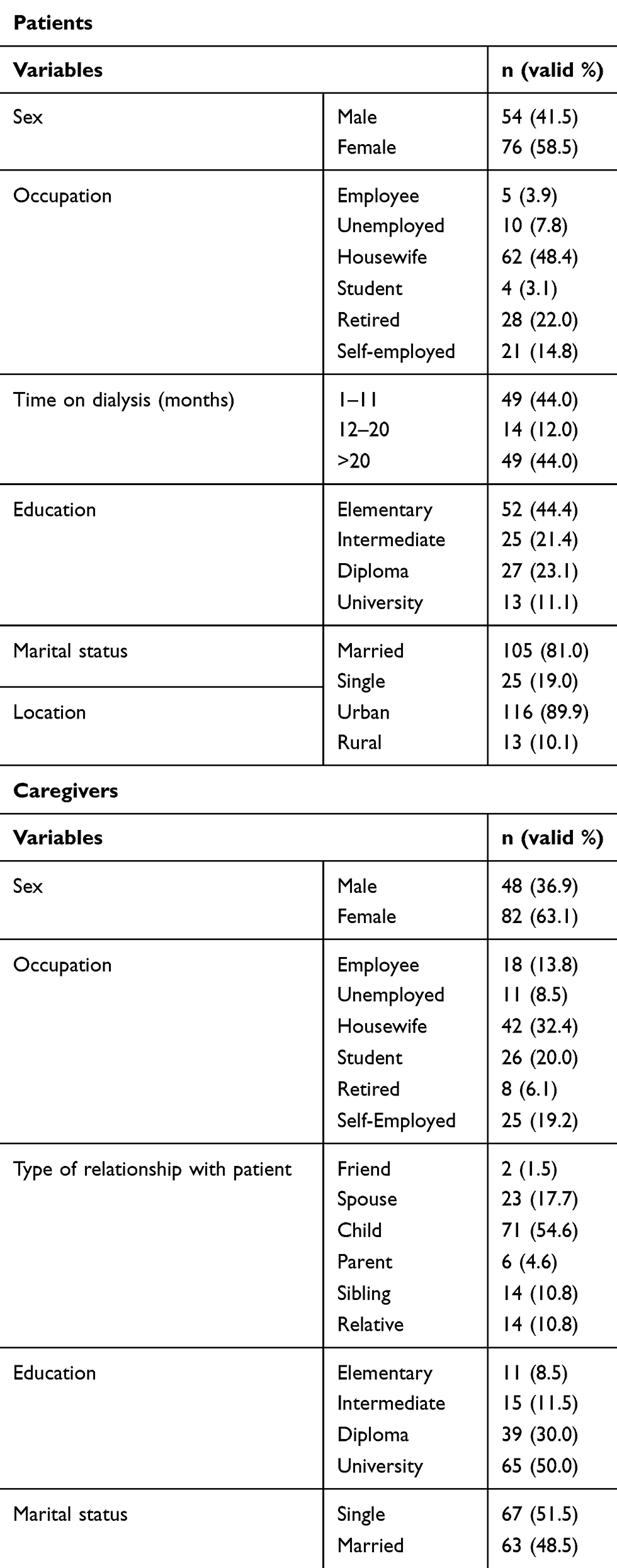 |
Table 1 Demographic characteristics of hemodialysis patients and their caregivers |
Based on the findings, 111 (86%) caregivers were experiencing a relatively high care burden. The mean total score of care burden was 58.5±20.5 out of 96. There was no significant relationship between the total burden of care and individual characteristics of caregivers (age, sex, marital status, education, occupation, or relationship with patient; Table 2). The mean scores of time-dependent, evolutionary, physical, social, and emotion-dependent care burdens were 17.5±5.3, 12.2±6.3, 9.1±4.7, 8.2±4.0, and 11.4±5.1, respectively. Also, the mean scores of problem-focused, emotion-focused, and avoidance-oriented coping strategies were 46.0±80.8, 43.1±9.0, and 48.9±9.5, respectively. The most common coping strategy used by the caregivers was avoidance (Figure 1 and Table 3). Among the strategies, only avoidance had a significant positive relationship with total care burden and all its subscales (Table 4).
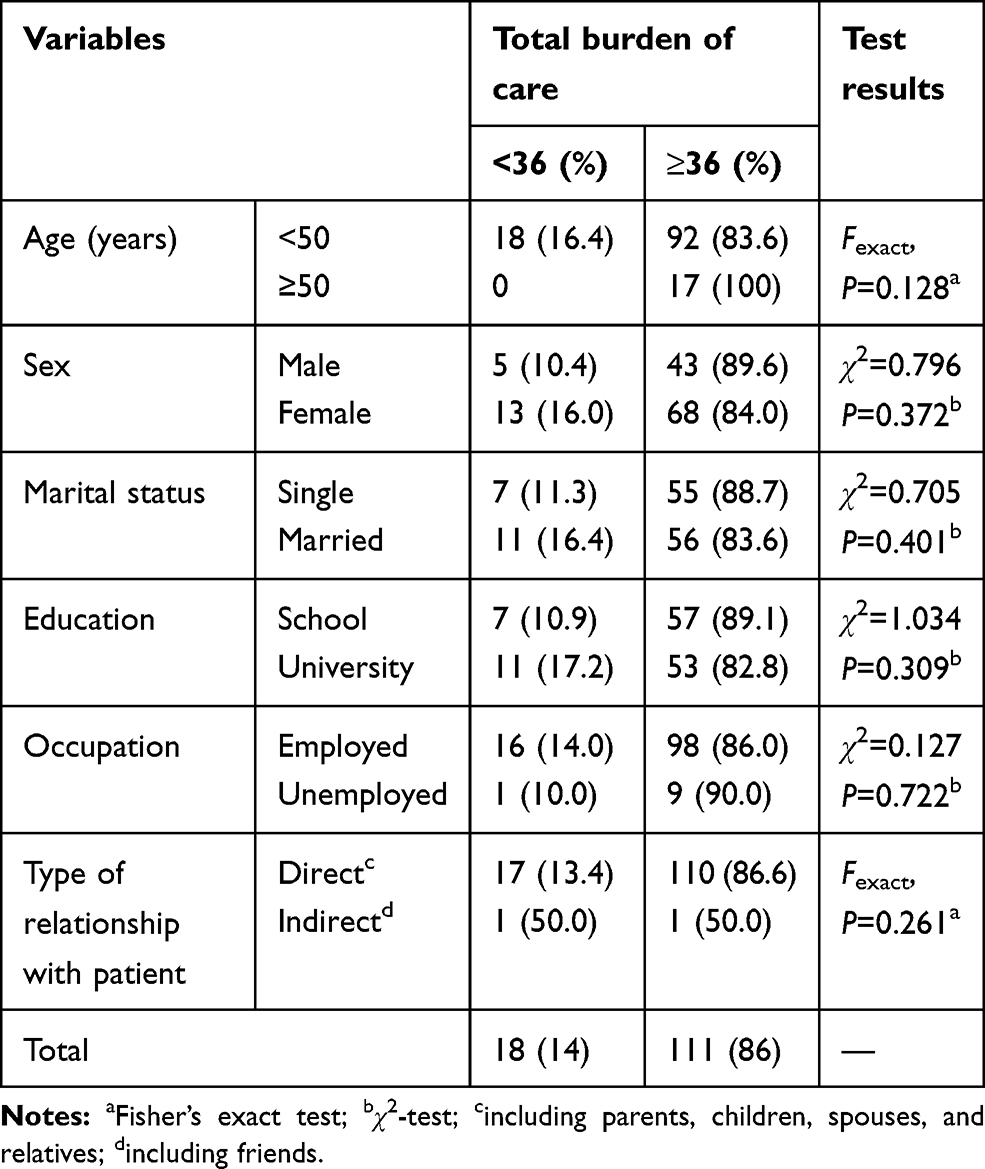 |
Table 2 Relationship between demographic characteristics and total burden of care in caregivers of hemodialysis patients |
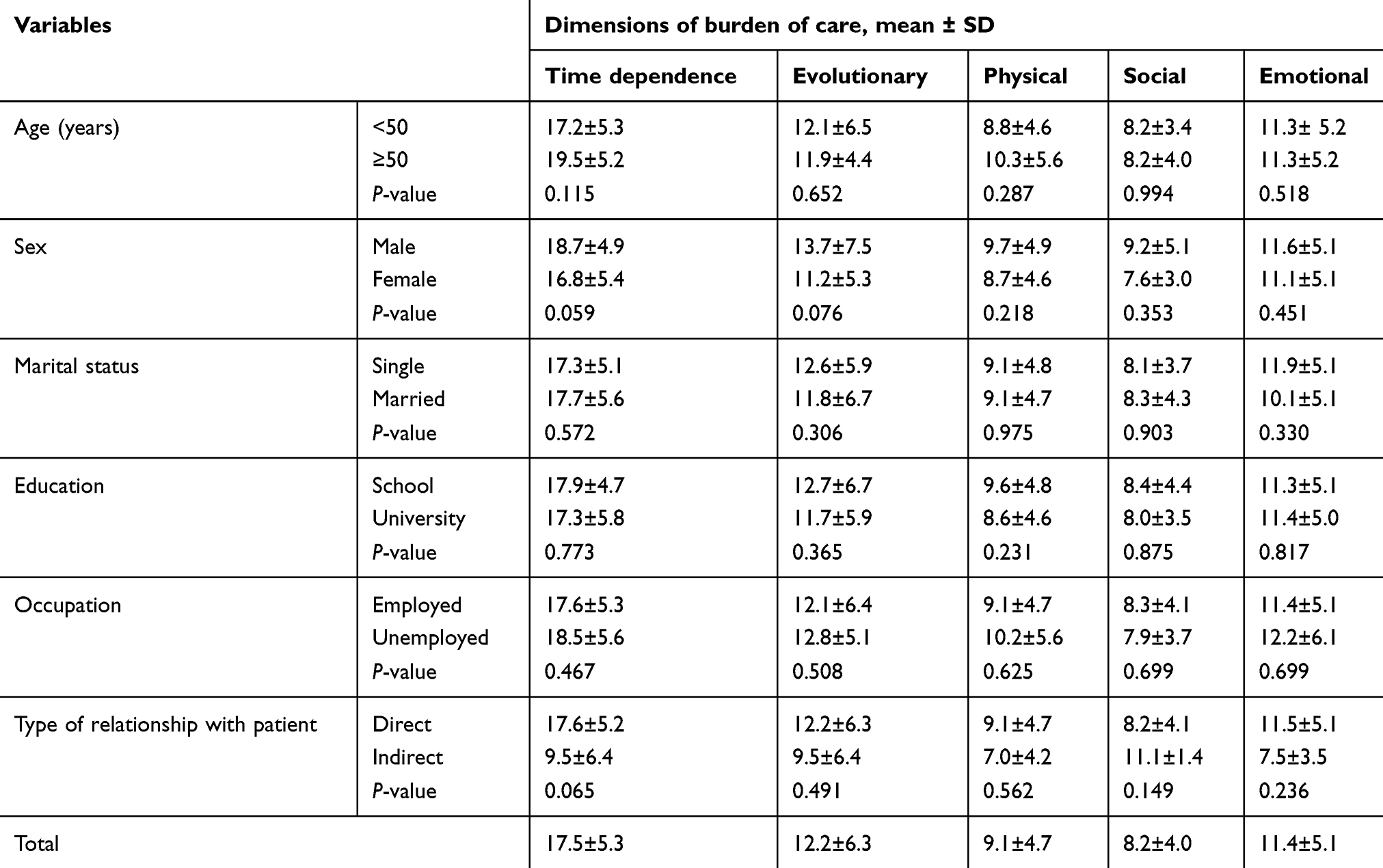 |
Table 3 Relationship between demographic characteristics and dimensions of care burden in caregivers of hemodialysis patients |
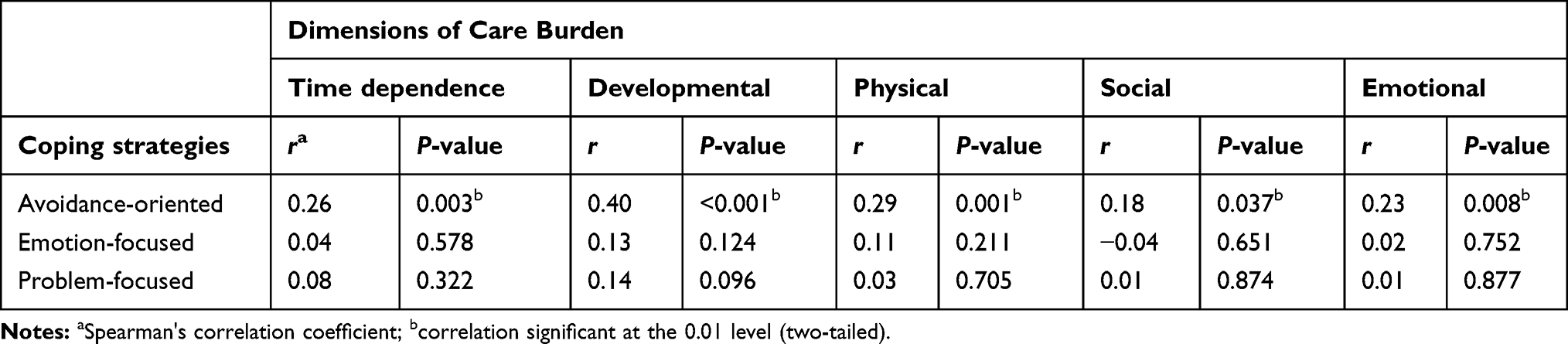 |
Table 4 Correlations between dimensions of care burden and coping strategies in caregivers of hemodialysis patients |
Discussion
The aim of this study was to determine the relationship between care burden and coping strategy in caregivers of hemodialysis patients. The total care burden was relatively high in the caregivers of hemodialysis patients, which is consistent with other studies on caregivers of hemodialysis patients.8,9,27,28 Overall, there is a higher level of care burden in developing countries, such as Iran, compared to developed countries, since the level of physical and spiritual support for caregivers is insufficient.29 Moreover, in Eastern countries, such as Iran, the family is responsible for patient, care due to the dominance of traditional culture; therefore, family members are exposed to care pressure.15
Caregivers of hemodialysis patients typically use different coping strategies, including problem-focused, emotion-focused, and avoidance-oriented coping strategies, to relieve their high care burden. Papastavrou et al showed that caregivers who experience a high level of care burden do not use problem-focused strategies.29 It seems that caregivers who use avoidance-oriented and emotion-focused strategies have higher levels of care burden.30 In this study, avoidance-oriented coping was the most common strategy used by the caregivers. This strategy is characterized by denial of problems and avoidance of stressful situations by ignoring the problem or turning to the community (or other individuals) for relieving stress.18,31
There is limited information regarding the effectiveness of avoidance-oriented coping strategies.32,33 It has been suggested that a problem-focused strategy is appropriate for managing problems.4 In this regard, Abbasi et al showed that using problem-focused coping significantly reduced the perceived caregiver burden. Caregivers who used problem-focused strategies also had less time-dependent care burden and less physical care stress.3 In addition, Ghane et al reported that the use of problem-focused coping reduced the care burden of hemodialysis patients’ caregivers.4
Such factors as sociocultural characteristics of caregivers and level of perceived care burden by caregivers are associated with the type of selected coping strategy.3,9 These factors can account for the discrepancy among the results of different studies. Generally, coping strategies need to be learned and trained. Since the most common coping strategy in the present study was avoidance-oriented, which is an inappropriate coping mechanism, it is necessary to establish training programs for caregivers of hemodialysis patients. On the other hand, given the effectiveness of the problem-focused strategy, it can be useful to teach this approach to caregivers of hemodialysis patients to reduce their care burden.
Chadda et al found a direct relationship between the emotion-focused coping strategy and total care burden and its subscales. In their study, caregivers who used emotion-focused coping strategies experienced more care burden.33 Given the ineffectiveness of emotion-focused strategies, caregivers should be educated about the unintended consequences of this approach and encouraged to use the problem-based approach. Therefore, holding educational classes or preparing educational materials can be a useful solution. Overall, such factors as sociodemographic differences and different care demands of hemodialysis patients are probably affected by the interaction between care-burden variables and coping strategies.
In the present study, there was no significant relationship between total care burden and demographic variables of caregivers. However, Jafari et al reported a significant positive relationship between care burden and caregivers’ age and education.9 In this regard, Bayoumi et alfound a negative correlation between total care burden and age and education of caregivers.7 Differences in results reported by different studies can be attributed to differences in individual characteristics of study samples and sample size.
This study had some limitations. First, it was cross-sectional, which does not explain the cause–effect relationship between the studied variables. Second, the self-administered method of data collection could have affected the accuracy of the results. Third, the caregivers’ psychological condition when completing the questionnaires might have affected their responses to the questions, which was beyond the control of the researchers. Another limitation was the small sample and statistical power of the study, which could have influenced the results. Finally, the lack of a control group to evaluate coping strategies was another limitation, which should be considered in future studies. Evaluating and comparing the relationship between care burden and coping strategies in other geographical regions is also suggested.
Conclusion
Caregivers of hemodialysis patients experienced a relatively high level of care burden, and avoidance-oriented coping was the most common coping strategy. Among all types of coping strategies, only avoidance-oriented coping had a significant relationship with total care burden and its subscales. Based on these findings, economic, social, and psychological support should be provided by governmental and nongovernmental organizations to reduce the care burden of caregivers of hemodialysis patients. Caregivers should be also trained to select an effective coping strategy.
Data-Sharing Statement
Data are available by contacting the corresponding author.
Acknowledgments
This work was supported by the Deputy of Research and Technology of KUMS. We would like to express our sincere gratitude to all the patients and their caregivers who participated in this research. We highly appreciate the Clinical Research Development Center of Imam Reza Hospital for their wise advice.
Disclosure
The authors declare that they do not have any conflicts of interest in this work.
References
1. Janssen IM, Gerhardus A, von Gersdorff GD, et al. Preferences of patients undergoing hemodialysis–results from a questionnaire-based study with 4,518 patients. Patient Prefer Adherence. 2015;9:847–855. doi:10.2147/PPA.S79559
2. Bikbov B, Perico N, Remuzzi G. Disparities in chronic kidney disease prevalence among males and females in 195 countries: analysis of the Global Burden of Disease 2016 study. Nephron. 2018;139(4):313–318. doi:10.1159/000489897
3. Abbasi A, Rahmani H, Shariati A, et al. The relationship between caring burden and coping strategies in hemodialysis patients caregivers. J Urmia Nurs Midwifery Fac. 2012;10(4):533–539.
4. Ghane G, Farahani MA, Seyedfatemi N, Haghani H. Effectiveness of problem-focused coping strategies on the burden on caregivers of hemodialysis patients. Nurs Midwifery Stud. 2016;5(2):e35594. doi:10.17795/nmsjournal35594
5. Alnazly EK. Burden and coping strategies among jordanian caregivers of patients undergoing hemodialysis. Hemodial Int. 2016;20(1):84–93. doi:10.1111/hdi.12318
6. Suri RS, Larive B, Hall Y, et al. Effects of frequent hemodialysis on perceived caregiver burden in the frequent hemodialysis network trials. Clin J Am Soc Nephrol. 2014;9(5):936–942. doi:10.2215/CJN.07170713
7. Bayoumi MM. Subjective burden on family carers of hemodialysis patients. Open J Nephrol. 2014;4(02):79–85. doi:10.4236/ojneph.2014.42011
8. Mashayekhi F, Pilevarzadeh M, Rafati F. The assessment of caregiver burden in caregivers of hemodialysis patients. Mater Sociomed. 2015;27(5):333–336. doi:10.5455/msm.2015.27.333-336
9. Jafari H, Ebrahimi A, Aghaei A, Khatony A. The relationship between care burden and quality of life in caregivers of hemodialysis patients. BMC Nephrol. 2018;19(1):321. doi:10.1186/s12882-018-1120-1
10. Belasco AG, Sesso R. Burden and quality of life of caregivers for hemodialysis patients. Am J Kidney Dis. 2002;39(4):805–812. doi:10.1053/ajkd.2002.32001
11. Belasco A, Barbosa D, Bettencourt AR, Diccini S, Sesso R. Quality of life of family caregivers of elderly patients on hemodialysis and peritoneal dialysis. Am J Kidney Dis. 2006;48(6):955–963. doi:10.1053/j.ajkd.2006.08.017
12. Zavagli V, Varani S, Samolsky-Dekel AR, Brighetti G, Pannuti F. Worry as a risk factor for mental and somatic diseases. A research on home-cared cancer patients family caregivers. G Ital Med Lav Ergon. 2012;34(2Suppl B):B17–B22.
13. Park B, Kim SY, Shin J-Y, et al. Prevalence and predictors of anxiety and depression among family caregivers of cancer patients: a nationwide survey of patient–family caregiver dyads in Korea. Support Care Cancer. 2013;21(10):2799–2807. doi:10.1007/s00520-013-1852-1
14. Chang H-Y, Chiou C-J, Chen N-S. Impact of mental health and caregiver burden on family caregivers’ physical health. Arch Gerontol Geriatr. 2010;50(3):267–271. doi:10.1016/j.archger.2009.04.006
15. Sajadi SA, Ebadi A. Quality of life among family caregivers of patients on hemodialysis and its relevant factors: a systematic review. Int J Community Based Nurs Midwifery. 2017;5(3):206–218.
16. Momeni K, Karami J, Rad AS. The relationship between spirituality, resiliency and coping strategies with students’ psychological well-being in Razi University of Kermanshah. J Kermanshah Univ Med Sci. 2013;16(8):626–634.
17. Abedini SM, Montazeri S, Khalatbari J. Comparing stress-coping styles in patients with multiple sclerosis and healthy people in east of Mazandaran. J Mazandaran Univ Med Sci. 2012;22(94):71–77.
18. Shoja-Kazemi M, Haqqani S, Saadati M, Khajehvand A. Relationship between family social support and coping styles in the improvement of breast cancer patients. J Breast Dis. 2014;6(4):35–40.
19. Ghazanfari F, Ghadam PE. The relationship between mental health and coping strategies in citizenship of Khoramabad city. The Quarterly Journal of Fundamentals of Mental Health. 2008;10(37):47–54.
20. Aqdasi AN, Eidi R. The relationship between mental health and coping strategies among spinal cord injury veterans in Tabriz. J Educ Sci. 2011;4(16):51–67.
21. Abbasi A, Shamsizadeh M, Asayesh H, et al. The relationship between caregiver burden with coping strategies in Family caregivers of cancer patients. J Psychiatr Nurs. 2013;1(3):62–71.
22. Myaskovsky L, Dew MA, Switzer GE, McNulty ML, DiMartini AF, McCurry KR. Quality of life and coping strategies among lung transplant candidates and their family caregivers. Soc Sci Med. 2005;60(10):2321–2332. doi:10.1016/j.socscimed.2004.10.001
23. Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29(6):798–803. doi:10.1093/geront/29.6.798
24. Endler NS, Parker JD. Multidimensional assessment of coping: a critical evaluation. J Pers Soc Psychol. 1990;58(5):844–854. doi:10.1037/0022-3514.58.5.844
25. McCleery A, Addington J, Addington D. Family assessment in early psychosis. Psychiatry Res. 2007;152(2–3):95–102. doi:10.1016/j.psychres.2006.07.002
26. Shokri O, Moradi A, Valiolah F, Sangari A, Ghanaee Z, Rezaee A. The role of personality traits and coping styles in mental health: causal models. J Cognit Sci News. 2004;1:28–38.
27. Jadhav BS, Dhavale HS, Dere SS, Dadarwala DD. Psychiatric morbidity, quality of life and caregiver burden in patients undergoing hemodialysis. Med J DY Patil Univ. 2014;7:722–727. doi:10.4103/0975-2870.144858
28. Abbasi A, Asayesh H, Rahmani H, Shariati A, Hosseini S, Rouhi G. The burden on cargivers from hemodialysis patients and related factors. J Res Dev Nurs Midwifery. 2011;8(1):26–33.
29. Papastavrou E, Charalambous A, Tsangari H. How do informal caregivers of patients with cancer cope: a descriptive study of the coping strategies employed. Eur J Oncol Nurs. 2012;16(3):258–263. doi:10.1016/j.ejon.2011.06.001
30. Wilks SE, Croom B. Perceived stress and resilience in Alzheimer’s disease caregivers: testing moderation and mediation models of social support. Aging Ment Health. 2008;12(3):357–365. doi:10.1080/13607860801933323
31. Kate N, Grover S, Kulhara P, Nehra R. Relationship of caregiver burden with coping strategies, social support, psychological morbidity, and quality of life in the caregivers of schizophrenia. Asian J Psychiatr. 2013;6(5):380–388. doi:10.1016/j.ajp.2013.03.014
32. Mausbach BT, Aschbacher K, Patterson TL, et al. Avoidant coping partially mediates the relationship between patient problem behaviors and depressive symptoms in spousal Alzheimer caregivers. Am J Geriat Psychiat. 2006;14(4):299–306. doi:10.1097/01.JGP.0000192492.88920.08
33. Chadda RK, Singh TB, Ganguly KK. Caregiver burden and coping. Soc Psychiatry Psychiatr Epidemiol. 2007;42(11):923–930. doi:10.1007/s00127-007-0242-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.