")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
The Relationship Between Baseline Clinical Symptom Characteristics and Working Ability in Japanese Patients Treated for Major Depressive Disorder and Painful Physical Symptoms
Authors Sugawara N , Yasui-Furukori N , Tsuji T , Hayashi S , Ajisawa Y , Ochiai T, Imagawa H, Shimoda K
Received 29 July 2020
Accepted for publication 20 November 2020
Published 11 December 2020 Volume 2020:16 Pages 3063—3070
DOI https://doi.org/10.2147/NDT.S274608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Norio Sugawara,1,* Norio Yasui-Furukori,1,* Toshinaga Tsuji,2 Shinji Hayashi,2 Yoshikazu Ajisawa,3 Toshimitsu Ochiai,3 Hideyuki Imagawa,4 Kazutaka Shimoda1
1Department of Psychiatry, Dokkyo Medical University School of Medicine, Tochigi, Japan; 2Medical Affairs Department, Shionogi & Co., Ltd., Osaka, Japan; 3Biostatistics Center, Shionogi & Co., Ltd., Osaka, Japan; 4Medicines Development Unit Japan, Eli Lilly Japan K.K., Kobe, Japan
*These authors contributed equally to this work
Correspondence: Norio Sugawara
Department of Psychiatry, Dokkyo Medical University School of Medicine, 880 Kitakobayashi, Mibu, Shimotsugagun, Tochigi 321-0293, Japan
Tel +81-28-287-2153
Fax +81-28-286-5187
Email [email protected]
Purpose: The objective of this post hoc analysis was to explore the relationship, including changes over time, between baseline clinical symptom characteristics and working ability, judged by investigators, after 12 weeks of antidepressant monotherapy in Japanese patients with major depressive disorder (MDD) and painful physical symptoms (PPS) in a real-world clinical setting.
Patients and Methods: This prospective, observational study in patients treated with duloxetine or selective serotonin reuptake inhibitors was conducted from 2014 to 2016. Both treatment groups were pooled and divided into 2 groups, “working ability recovered” or “working ability not recovered,” based on working ability at the end of the study. Patients were also divided into 4 subgroups by the presence or absence of previous depressive episodes and working ability. Main outcome measures included baseline demographics and clinical characteristics, and the 17-item Hamilton Rating Scale for Depression (HAM-D17).
Results: Comparison between “working ability recovered” (n=122) and “working ability not recovered” (n=91) showed that the percentage of patients with complications and psychotherapy at baseline, and baseline HAM-D17 total, insomnia, somatic, and anxiety scores, were significantly different. The results of subgroup analyses were mostly the same as the results analyzed by working ability alone. Although statistical differences were observed for some outcome measures, the differences at baseline, except use of psychotherapy, may not be applicable clinically, and there were no specific trends observed that could predict working ability.
Conclusion: This post hoc analysis suggested that most baseline clinical characteristics, including the presence or absence of previous depressive episodes, were not predictive of working ability recovery. However, the use of psychotherapy in parallel with antidepressant monotherapy may be positively associated with working ability recovery. All outcome measures improved over time, reinforcing the importance of continuous treatment and observation to improve and accurately judge working ability in patients with MDD and PPS.
Keywords: ability to work, antidepressants, depressive disorder, major, observational study, painful physical symptoms
Introduction
Major depressive disorder (MDD) is a chronic, recurrent disease that adversely affects quality of life (QoL).1,2 The median age of onset of mood disorders, including MDD, ranges between the late 20s and the early 40s,3 which is the primary working-age population. MDD can lead to loss of working ability, which has effects not only on individuals but also on social and economic activity,4,5 because MDD is a major reason for long-term sick leave and permanent work disability.6 Vietri et al reported that approximately 20% of MDD patients complained of painful physical symptoms (PPS) without clear physical causes.7 Further, MDD patients with PPS had a higher burden from the perspective of healthcare resources and costs, health-related QoL, and work productivity.7,8 Any characteristics that help identify those patients with MDD and PPS who can return to work after treatment, especially if assessed at an early stage of treatment, would be useful. However, there have been limited reports regarding the relationship between patients’ characteristics and working ability in patients with MDD,9,10 and no reports in patients with MDD and PPS.
A 12-week, prospective, observational study was previously conducted in Japanese patients with MDD and PPS to investigate the effectiveness of duloxetine or selective serotonin reuptake inhibitor (SSRI) monotherapy for PPS, depressive symptoms, and QoL.11,12 In a post hoc analysis of the study, a 17-item Hamilton Rating Scale for Depression (HAM-D17) score ≤6 after 12 weeks of treatment corresponded best with psychiatrists’ judgment of working ability.13 The objective of the current post hoc analysis was to explore the relationship, including changes over time, between baseline clinical symptom characteristics and working ability, as judged by investigators, after 12 weeks of antidepressant monotherapy in Japanese patients with MDD and PPS in a real-world clinical setting. An additional aim was to determine whether there were any differences in baseline clinical symptom characteristics between patient subgroups based on working ability in the presence or absence of previous depressive episodes before study entry.
Patients and Methods
Study Design
This was a prospective, observational study in Japanese patients with MDD and PPS treated with duloxetine or SSRIs for 12 weeks. The study was conducted at 39 psychiatric and psychosomatic outpatient/inpatient clinics/hospital sites from February 2014 to February 2016. Full study methods and results of the primary efficacy outcome analyses, preplanned subgroup analyses, and post hoc analyses have been published previously.11–13
Patients
In brief, patients were ≥20 years old, resided in Japan, and presented with a depressive episode of MDD without psychotic traits.14 Patients diagnosed with at least moderate levels of depression (Quick Inventory of Depressive Symptomatology-Self Report ≥16) and PPS (Brief Pain Inventory-Short Form [BPI-SF], average pain ≥3) were included. The duloxetine and SSRI (escitalopram, sertraline, paroxetine, or fluvoxamine) treatment groups were pooled before being divided into 2 groups, “working ability recovered” or “working ability not recovered,” based on working ability judged by investigators after the 12-week treatment period. Patients were also divided into 4 subgroups by the presence or absence of previous depressive episodes before starting the study (ie, the patient had experienced episodes before the presenting episode or the presenting episode was the patient’s first episode) and by working ability. Patients for whom the presence or absence of previous depressive episodes was unknown were excluded from this analysis.
Outcome Measures
Outcome measures for this post hoc analysis included baseline demographics and clinical characteristics, HAM-D1715 (total and subscale [core, insomnia, anxiety, somatic]16 scores) for depressive symptoms, BPI-SF (average pain score) for PPS, Social Adaptation Self-evaluation Scale (SASS) and the Global Assessment of Functioning (GAF) for social functioning, and EuroQol-5 Dimensions questionnaire (EQ-5D) for QoL at baseline and Weeks 2, 4, 8, and 12.
Statistical Analysis
All patients were included in the analysis except those who were able to work at baseline, those with working ability data missing at baseline or after 12 weeks of treatment, or those who were excluded from the effectiveness analysis population (eg, did not meet entry criteria, case report form not retrievable, administration of study drug could not be confirmed, no post-baseline visit, no post-baseline effectiveness data).
Data were summarized descriptively as mean ± standard deviation for continuous variables and percentages for categorical variables. Statistical tests were performed using Welch’s t-test for differences in means between groups for continuous variables, a chi-square test for differences in percentages in each category between groups for categorical variables, and the Wilcoxon rank sum test for the number of MDD episodes experienced (1, 2, 3 or more; excluding “unknown”) as the ordinal scale between groups, with a two-sided significance level of 0.05. No adjustments for multiplicity were made. Statistical analyses were performed using SAS® version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient Recruitment and Baseline Characteristics
Of 596 patients enrolled, 213 patients (122 working ability recovered, 91 working ability not recovered) were included in the analysis (Figure 1). Numbers of patients with working ability recovered without or with previous depressive episodes were 66 and 36, respectively. Numbers of patients with working ability not recovered without or with previous depressive episodes were 40 and 35, respectively.
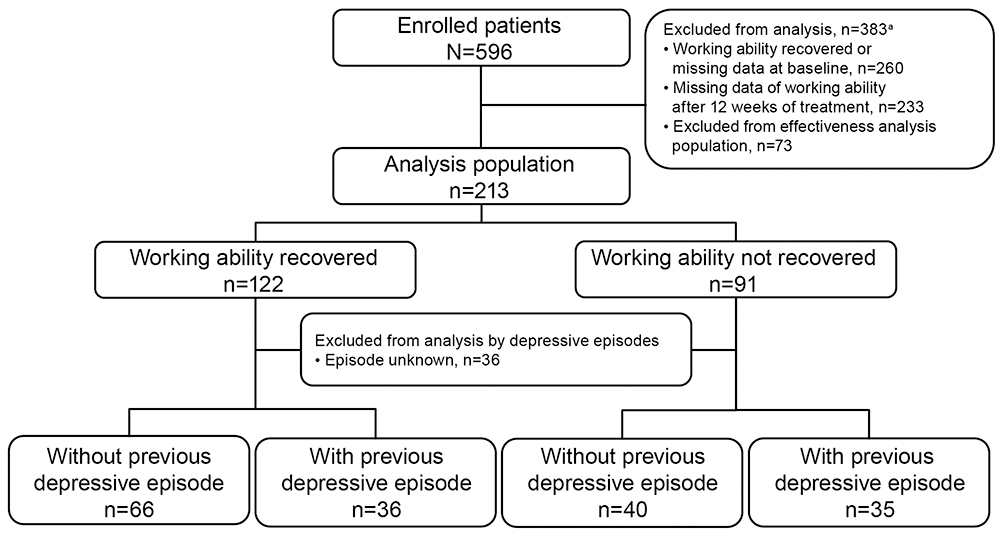 |
Figure 1 Patient recruitment. aMultiple reasons for exclusion from the analysis were possible. |
The baseline characteristics of patients with working ability recovered were similar to those of patients with working ability not recovered, except for the presence of complications and the use of psychotherapy (Table 1). The percentage of patients with complications was significantly lower in the working ability recovered group than the working ability not recovered group (8.2% vs 24.2%, p=0.0012). All complications were reported in ≤3 patients in each group, except for hypertension (2 patients [1.6%] with working ability recovered, 5 patients [5.5%] with working ability not recovered) (Supplementary Table). The percentage of patients with working ability recovered who had used psychotherapy was significantly greater than in patients with working ability not recovered (50.8% vs 28.6%, p=0.0011).
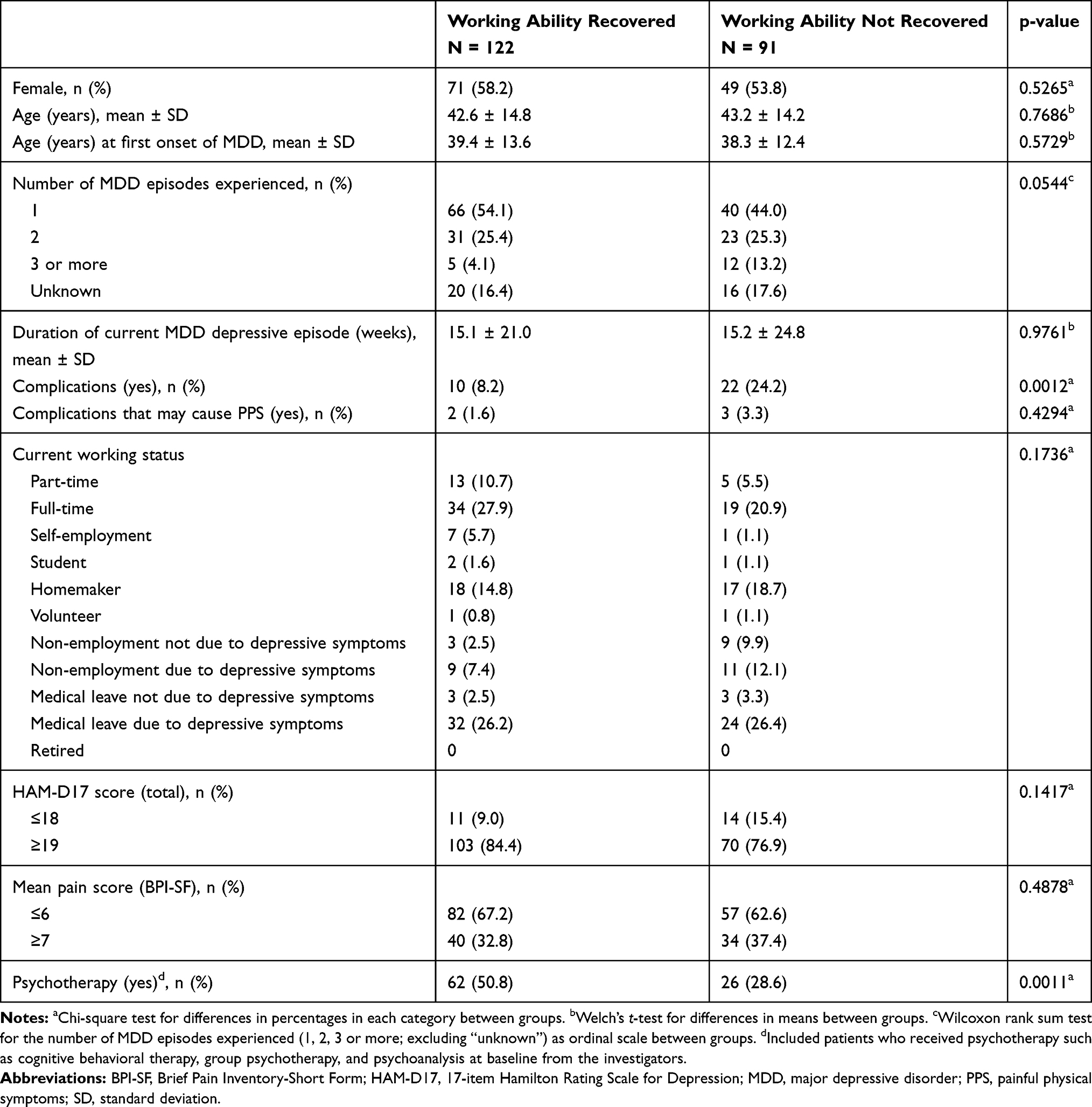 |
Table 1 Demographics and Baseline Clinical Characteristics |
Working Ability Recovered Group Compared with Working Ability Not Recovered Group
Depressive Symptoms
Baseline HAM-D17 total, insomnia, and anxiety scores were significantly higher (p<0.05), but the somatic score was significantly lower (p<0.05), in the working ability recovered group than in the working ability not recovered group (Supplementary Figure 1a–1e).
HAM-D17 total and all subscale (core, insomnia, anxiety, and somatic) scores at Weeks 8 and 12 were significantly lower in the working ability recovered group than in the working ability not recovered group (p<0.01 for all scores). HAM-D17 total and insomnia scores at Week 4, and core and somatic scores at Weeks 2 and 4, in the working ability recovered group were also significantly lower than in the working ability not recovered group (p<0.05 for core score at Week 2 and insomnia score at Week 4, p<0.01 for total and core scores at Week 4, and p<0.01 for somatic score at Weeks 2 and 4).
PPS
BPI-SF scores were lower in the working ability recovered group than in the working ability not recovered group throughout the treatment, with no significant difference at baseline but with significant differences at Weeks 4, 8, and 12 (p<0.05 for Week 4, p<0.01 for Weeks 8 and 12) (Supplementary Figure 1f).
Social Functioning
SASS scores were higher in the working ability recovered group than in the working ability not recovered group throughout the treatment, with no significant difference at baseline but with significant differences at Weeks 4, 8, and 12 (p<0.01 for all) (Supplementary Figure 1g).
GAF scores were higher in the working ability recovered group than in the working ability not recovered group throughout the treatment, with no significant difference at baseline but with significant differences at Weeks 2, 4, 8, and 12 (p<0.01 for all) (Supplementary Figure 1h).
QoL
EQ-5D scores were significantly higher in the working ability recovered group than in the working ability not recovered group at Weeks 4, 8, and 12 (p<0.01 for all), with no significant difference at baseline (Supplementary Figure 1i).
Working Ability Recovered Compared with Working Ability Not Recovered in Subgroups with and without Previous Depressive Episodes
Depressive Symptoms
Significant differences between working ability groups were observed in several baseline HAM-D17 subscales (Supplementary Figure 2a–2e). In patients without previous depressive episodes, insomnia score was higher in patients with working ability recovered than in patients with working ability not recovered (p<0.05). In patients with previous depressive episodes, somatic score was lower (p<0.05), but anxiety score was higher (p<0.01), in patients with working ability recovered than in patients with working ability not recovered.
At Weeks 8 and 12, HAM-D17 total and all subscale scores were lower in the working ability recovered group than in the working ability not recovered group, regardless of the presence or absence of previous depressive episodes.
PPS
BPI-SF scores did not differ at baseline or during the early part of treatment between patients with working ability recovered and patients with working ability not recovered, regardless of the presence or absence of previous depressive episodes (Supplementary Figure 2f).
Social Functioning
SASS scores were higher at Weeks 4, 8, and 12 in patients with working ability recovered than in patients with working ability not recovered, regardless of the presence or absence of previous depressive episodes (Supplementary Figure 2g).
GAF scores were consistently higher in the working ability recovered group than in the working ability not recovered group throughout the treatment, regardless of the presence or absence of previous depressive episodes, with no significant differences at baseline (Supplementary Figure 2h).
QoL
EQ-5D scores were higher at Weeks 8 and 12 in patients with working ability recovered than in patients with working ability not recovered, regardless of the presence or absence of previous depressive episodes, with no significant differences at baseline (Supplementary Figure 2i).
Discussion
In this post hoc analysis, we compared baseline clinical symptom characteristics of Japanese patients with MDD and PPS between those with or without working ability, as judged by investigators, after 12 weeks of antidepressant treatment in a real-world clinical setting. Patients who recovered working ability had fewer complications, used psychotherapy more frequently, and, unexpectedly, had higher baseline HAM-D17 total, insomnia, and anxiety scores, but lower somatic scores, than patients who did not recover working ability. Among patients without previous depressive episodes, the baseline HAM-D17 insomnia score was higher in those with working ability recovered, whereas among patients with previous depressive episodes, the anxiety score was higher, but the somatic score was lower, in those with working ability recovered.
Our comparison between the working ability recovered group and the working ability not recovered group showed that HAM-D17 total, insomnia, anxiety, and somatic scores at baseline were significantly different. However, these statistical differences may not be applicable clinically. Nevertheless, these outcome measures improved over time, and greater differences between the working ability groups were observed with longer treatment up to 12 weeks, with significant differences seen at Weeks 8 and 12. This suggests that continuous treatment and observation by healthcare professionals are important to improve depressive symptoms and to accurately judge working ability in patients with MDD and PPS.
The baseline characteristics of patients with working ability recovered were similar to those of patients with working ability not recovered, except for the presence of complications and the use of psychotherapy. No specific complications that may affect working ability between the groups were identified, although the impact of complications on working ability could not be excluded. Psychotherapy reduces sick leave in patients with common mental disorders, including depression, or musculoskeletal disorders, including low back pain and muscle pain,17 and early access to psychotherapy reduces the duration of sick leave in patients with mental disorders.18,19 On the other hand, one study reported that psychological care combined with antidepressants did not reduce medium- or long-term sick leave.20 Although the use of psychotherapy may be positively associated with working ability recovery, further research is needed. Other previous research reported that patients whose depressive symptoms clinically improved during initial treatment were more likely than nonresponders to have increased work productivity.21 In addition, some previous studies in patients with MDD reported that severity of depression at baseline predicted functional recovery,9,22,23 although a systematic review including 35 controlled studies reported that baseline disease severity did not predict functional improvement.24 Although these reports did not specifically target patients with MDD and PPS, an analysis of treatment history and the recovery of working ability by severity of MDD may also be worth considering in this patient population.
Baseline differences between working ability groups were seen in HAM-D17 insomnia score in patients without previous depressive episodes, and in HAM-D17 anxiety and somatic scores in patients with previous depressive episodes. The results of these subgroup analyses, including significant differences, were mostly the same as the results by working ability alone. Incomplete resolution of previous depressive episodes is a predictor of poor prognosis, including the severity, relapsing, and chronic course of depression.25 However, as with the main analysis, despite the observed statistical differences, these results may not be clinically useful for predicting recovery of working ability between patient subgroups in the presence or absence of previous depressive episodes.
A previous post hoc analysis of this study reported that a HAM-D17 total score ≤6 after 12 weeks of treatment corresponded with patients’ working ability.13 The results of the current analysis also showed that mean HAM-D17 total score in the group with working ability recovered was less than 6 only at Week 12, although improvements of all outcome measures were observed over time in all groups. In contrast, SASS and GAF scores for social functioning were significantly higher in the working ability recovered group than in the working ability not recovered group throughout the treatment up to Week 12. It is important to judge full recovery of social functioning including working ability, as well as remission of depressive symptoms, by continuous treatment and observation.
Several limitations need to be considered. This was a post hoc analysis of a nonrandomized observational study, and no adjustments for multiplicity were made. Working ability after 12 weeks of treatment was judged by investigators, and their judgment may have been influenced by the results of the HAM-D17 total score. The study enrolled Japanese patients with MDD and PPS; therefore, the results may not be generalizable to MDD patients without PPS, and there may be potential cultural or ethnic differences. In particular, it may be difficult to extrapolate the somatic score results seen in patients with MDD and PPS to patients without PPS.
Conclusions
This post hoc analysis suggests that most baseline clinical characteristics with significant differences were not clinically applicable to the prediction of working ability recovery, nor was the presence or absence of previous depressive episodes. However, the use of psychotherapy in parallel with antidepressant monotherapy may be positively associated with of working ability recovery, as judged by investigators after 12 weeks of antidepressant treatment. All outcome measures improved over time regardless of the baseline characteristics, reinforcing the importance of continuous treatment and observation to improve and accurately judge working ability in patients with MDD and PPS.
Abbreviations
BPI-SF, Brief Pain Inventory-Short Form; EQ-5D, EuroQol-5 Dimensions questionnaire for quality of life; GAF, Global Assessment of Functioning; HAM-D17, 17-item Hamilton Rating Scale for Depression; MDD, major depressive disorder; PPS, painful physical symptoms; QoL, quality of life; SASS, Social Adaptation Self-evaluation Scale; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor.
Ethics Approval and Informed Consent
The study was conducted in accordance with Good Post-marketing Study Practices for Drugs and applicable laws and regulations.26 The Japanese Ministry of Health, Labour and Welfare and the institutional review boards of Shionogi & Co., Ltd. and Dokkyo Medical University School of Medicine reviewed and approved the protocol. Patients provided written informed consent before enrollment.
Acknowledgments
The authors would like to thank all study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This post hoc analysis was sponsored by Shionogi & Co., Ltd. using data from a study co-sponsored by Shionogi & Co., Ltd. and Eli Lilly Japan K.K., who were involved in the preparation of the manuscript. Medical writing assistance was provided by Yukiko Homma and Rebecca Lew, PhD, CMPP, of ProScribe – Envision Pharma Group, and was funded by Shionogi & Co., Ltd. ProScribe’s services complied with international guidelines for Good Publication Practice (GPP3).
Disclosure
TT is a full-time employee of Shionogi & Co., Ltd. and holds stock in Shionogi & Co., Ltd. and Takeda Pharmaceutical Company Limited. SH is a full-time employee of Shionogi & Co., Ltd. and holds stock in Shionogi & Co., Ltd. and Takara Bio Inc. TO is a full-time employee of Shionogi & Co., Ltd. and holds stock in Shionogi & Co., Ltd. YA was a full-time employee of Shionogi & Co., Ltd. during the preparation of this manuscript. HI is a full-time employee of Eli Lilly Japan K.K. and holds stock in Eli Lilly and Company. NS has no conflicts of interest to declare. NYF has received grant/research support or honoraria from, and has been a speaker for, Dainippon Sumitomo Pharma Co., Ltd., Mochida Pharmaceutical Co., Ltd., MSD, and Otsuka Pharmaceutical Co., Ltd. KS has received research support from Novartis Pharma K.K., Dainippon Sumitomo Pharma Co., Ltd., Astellas Pharma Inc., Eisai Co., Ltd., Pfizer Inc., Otsuka Pharmaceutical Co., Ltd., and Daiichi Sankyo Company, Limited, and honoraria from Eisai Co., Ltd., Meiji Seika Pharma Co., Ltd., Janssen Pharmaceutical K.K., Dainippon Sumitomo Pharma Co., Ltd., Eli Lilly Japan K.K., and Pfizer Inc. The authors report no other potential conflicts of interest for this work.
References
1. Mueller TI, Leon AC, Keller MB, et al. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry. 1999;156(7):1000–1006.
2. Bromet E, Andrade LH, Hwang I, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9:90. doi:10.1186/1741-7015-9-90
3. Kessler RC, Angermeyer M, Anthony JC, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry. 2007;6(3):168–176.
4. de Graaf R, Tuithof M, van Dorsselaer S, Ten Have M. Comparing the effects on work performance of mental and physical disorders. Soc Psychiatry Psychiatr Epidemiol. 2012;47(11):1873–1883. doi:10.1007/s00127-012-0496-7
5. Ekman M, Granström O, Omérov S, Jacob J, Landén M. The societal cost of depression: evidence from 10,000 Swedish patients in psychiatric care. J Affect Disord. 2013;150(3):790–797. doi:10.1016/j.jad.2013.03.003
6. de Vries G, Hees HL, Koeter MWJ, Lagerveld SE, Schene AH. Perceived impeding factors for return-to-work after long-term sickness absence due to major depressive disorder: a concept mapping approach. PLoS One. 2014;9(1):e85038. doi:10.1371/journal.pone.0085038
7. Vietri J, Otsubo T, Montgomery W, Tsuji T, Harada E. The incremental burden of pain in patients with depression: results of a Japanese survey. BMC Psychiatry. 2015;15:104. doi:10.1186/s12888-015-0488-8
8. Vietri J, Otsubo T, Montgomery W, Tsuji T, Harada E. Association between pain severity, depression severity, and use of health care services in Japan: results of a nationwide survey. Neuropsychiatr Dis Treat. 2015;11:675–683.
9. Ervasti J, Joensuu M, Pentti J, et al. Prognostic factors for return to work after depression-related work disability: a systematic review and meta-analysis. J Psychiatr Res. 2017;95:28–36. doi:10.1016/j.jpsychires.2017.07.024
10. Laukkala T, Heikinheimo S, Vuokko A, Junttila IS, Tuisku K. Subjective and objective measures of function and return to work: an observational study with a clinical psychiatric cohort. Soc Psychiatry Psychiatr Epidemiol. 2018;53(5):537–540. doi:10.1007/s00127-017-1479-5
11. Kuga A, Tsuji T, Hayashi S, et al. An observational study of duloxetine versus SSRI monotherapy for the treatment of painful physical symptoms in Japanese patients with major depressive disorder: primary analysis. Neuropsychiatr Dis Treat. 2017;13:2105–2114. doi:10.2147/NDT.S131438
12. Kuga A, Tsuji T, Hayashi S, et al. An observational study of duloxetine versus SSRI monotherapy in Japanese patients with major depressive disorder: subgroup analyses of treatment effectiveness for pain, depressive symptoms, and quality of life. Neuropsychiatr Dis Treat. 2017;13:2115–2124. doi:10.2147/NDT.S136448
13. Kuga A, Otsubo T, Tsuji T, et al. Analysis of HAM-D scores and working ability in an observational study of Japanese patients with major depressive disorder and painful physical symptoms treated with duloxetine or SSRI monotherapy. Neuropsychiatr Dis Treat. 2019;15:809–817. doi:10.2147/NDT.S195445
14. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th Ed. Text Revision. Washington, DC: American Psychiatric Association; 2000.
15. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
16. Dombrovski AY, Cyranowski JM, Mulsant BH, et al. Which symptoms predict recurrence of depression in women treated with maintenance interpersonal psychotherapy? Depress Anxiety. 2008;25(12):1060–1066. doi:10.1002/da.20467
17. Finnes A, Enebrink P, Ghaderi A, Dahl J, Nager A, Öst LG. Psychological treatments for return to work in individuals on sickness absence due to common mental disorders or musculoskeletal disorders: a systematic review and meta-analysis of randomized-controlled trials. Int Arch Occup Environ Health. 2019;92(3):273–293. doi:10.1007/s00420-018-1380-x
18. Alonso S, Marco JH, Andani J. Reducing the time until psychotherapy initiation reduces sick leave duration in participants diagnosed with anxiety and mood disorders. Clin Psychol Psychother. 2018;25(1):138–143.
19. Marco JH, Alonso S, Andani J. Early intervention with cognitive behavioral therapy reduces sick leave duration in people with adjustment, anxiety and depressive disorders. J Ment Health. 2018:1–9.
20. Trivedi D. Cochrane review summary: interventions to improve return to work in depressed people. Prim Health Care Res Dev. 2018;19(2):107–109. doi:10.1017/S1463423617000482
21. Trivedi MH, Morris DW, Wisniewski SR, et al. Increase in work productivity of depressed individuals with improvement in depressive symptom severity. Am J Psychiatry. 2013;170(6):633–641. doi:10.1176/appi.ajp.2012.12020250
22. Rytsälä HJ, Melartin TK, Leskelä US, Lestelä-Mielonen PS, Sokero TP, Isometsä ET. Determinants of functional disability and social adjustment in major depressive disorder: a prospective study. J Nerv Ment Dis. 2006;194(8):570–576. doi:10.1097/01.nmd.0000230394.21345.c4
23. Novick D, Montgomery W, Vorstenbosch E, Moneta MV, Dueñas H, Haro JM. Recovery in patients with major depressive disorder (MDD): results of a 6-month, multinational, observational study. Patient Prefer Adherence. 2017;11:1859–1868. doi:10.2147/PPA.S138750
24. Sheehan DV, Nakagome K, Asami Y, Pappadopulos EA, Boucher M. Restoring function in major depressive disorder: a systematic review. J Affect Disord. 2017;215:299–313. doi:10.1016/j.jad.2017.02.029
25. Judd LL, Paulus MJ, Schettler PJ, et al. Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Am J Psychiatry. 2000;157(9):1501–1504. doi:10.1176/appi.ajp.157.9.1501
26. Ministry of Health, Labour and Welfare. Ministerial ordinance on good post-marketing study practices for drugs. No. 171; December 20, 2004.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.