")
Back to Journals » Patient Preference and Adherence » Volume 10
The psychometric properties of Chinese version of SCI Exercise Self-Efficacy Scale in patients with stroke
Authors Dong X, Liu Y, Wang A, Wang M
Received 23 February 2016
Accepted for publication 19 May 2016
Published 18 July 2016 Volume 2016:10 Pages 1235—1241
DOI https://doi.org/10.2147/PPA.S106938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Xiaofang Dong,1 Yanjin Liu,2 Aixia Wang,1 Min Wang1
1Neurology Department, 2Nursing Department, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan Province, People’s Republic of China
Objective: To test the Chinese version of the SCI Exercise Self-Efficacy Scale (C-ESES) in stroke patients and evaluate its validity and reliability.
Background: Physical inactivity is a well established and changeable risk factor for stroke, and regular exercise of 3–7 days per week is essential for stroke survivors and the general population. Though regular exercise is beneficial, it has been proved that duration, frequency, and intensity of exercise are generally low in stroke survivors.
Methods: The performance of the instrument was assessed in 350 Chinese stroke survivors and repeated in 50 patients to examine test–retest reliability. Questionnaires included a form on demographic and socioeconomic characteristics, C-ESES, and the Chinese version of the General Self-Efficacy Scale. The AMOS 20.0 and SPSS 17.0 were chosen to evaluate their validity and reliability.
Results: Even though 350 participants answered the questionnaires in the present study, useful data were obtained from 321 participants (response rate: 91.71%). Correlation between item and the total scale score (Item–Total Correlation) ranged from 0.551 to 0.718, indicating that no item needed to be omitted; two factors, with factor loading 0.620 and 0.806, were obtained from an exploratory principal components analysis, assuming 59.745% of the total variance. The two factors were named internal motivation and external motivation. A confirmatory factor analysis supported the results with a suitable model (χ2=291.157; df=185; P<0.001; root mean square error of approximation =0.044; goodness-of-fit index =0.938; adjusted goodness-of-fit index =0.914; comparative fit index =0.858). The C-ESES correlated well with the validated General Self-Efficacy Scale (r=0.827, P<0.01). Good internal consistency (Cronbach’s α=0.757 to 0.879) and test–retest reliability (r=0.750, P<0.01) were obtained.
Conclusion: The C-ESES is a short, easy to understand, and psychometrically sound measurement to evaluate exercise self-efficacy in Chinese-speaking stroke survivors.
Keywords: psychometrics testing, self-efficacy, stroke, survey designs, chronic illness
Introduction
The estimated recurrence of stroke and the disability rate have been found to be higher in the Chinese population as compared to that observed in Western countries.1 It is well known that less exercise is a modifiable risk factor for stroke and recurrent stroke.2 The protective effects of exercise have been seen in a large study.3 Exercise plays an important role in decreasing blood pressure, losing and maintaining weight, and promoting good mental health.4,5 Therefore, the American Heart Association recommends that stroke patients spend 20–60 minutes on exercising, 3–7 days a week.6
Despite evidence for the long- and short-term advantages of regular exercise, the estimated duration and intensity of physical activity have been reported to be low in stroke survivors. A meta-analysis reported that the estimated step count for stroke survivors was 4,355.2 steps/day (95% confidence interval: 3,210.4 to 5,499.9),7 which was well below that reported for a healthy elderly population (6,000 steps/day)8 and even much fewer than the commendatory steps everyday for population with chronic diseases (6,500–8,500 steps/day).9 Psychological aspects, such as self-efficacy, were reported to have an effect on exercise.10 Self-efficacy, a key concept in the social cognitive theory, means the “belief in one’s abilities to scheme and perform the courses of situation requested to conduct given accomplishment.”11 It has been reported that a high level of exercise self-efficacy can predict the start and sustenance of exercise over time in patients with cerebrovascular diseases.12
The SCI Exercise Self-Efficacy Scale (ESES), a self-reported scale invented by Kroll,13 measures self-efficacy to perform exercise in spite of numerous difficult situations. Even though the ESES is firstly invented to measure self-efficacy in spinal cord injury patients,13 the items on this scale are fairly general, and it has been used with pregnant women14 and elite wheelchair-dependent athletes.15 However, the biggest problem is whether this scale can be used with other populations, such as people with stroke.
Therefore, the present study aimed to evaluate the psychometric properties of ESES in Chinese-speaking stroke population.
Materials and methods
Participants
This study was conducted in the neurology department between April and September 2015. There was a total of 350 participants according to the criteria: 1) were diagnosed with stroke; 2) were 18–75 years old; 3) had formally agreed to participate; and 4) were independent in daily activities measured by a score ≤3 on the modified Rankin Scale.16 Participants with serious psychiatric illnesses (schizophrenia, schizoaffective disorder, or bipolar disorder) were excluded.
Instruments
A form on demographic and socioeconomic characteristics
This form comprised eight questions assessing the participants’ demographic and socioeconomic information. Additionally, patients’ comorbid conditions and the modified Rankin Scale score were evaluated.
The ESES
The ESES, a ten-item self-report measure researched by Kroll,13 requires respondents to point out whether they could persist in an exercise plan, even though the situations could be tough, such as “When I am confronted with a barrier to physical activity or exercise” and “When I am tired.” Respondents are instructed to choose one option that reflects their confidence when doing regular exercise. A higher mean of all the items indicates a higher degree of exercise self-efficacy.
The C-GSE
The Chinese version of the General Self-Efficacy Scale (C-GSE) measures one’s competence when managing tough situations,17 with the grade ranging from 10 to 40. It has been reported that the C-GSE has good psychometric properties (Cronbach’s α=0.96).18
Translation and adaptation of the scale
After got translation permission from Thilo Kroll, the instrument was interpreted persisting in Brisling’s translation model19: A) Translation and back-translation: original ESES was interpreted into Chinese by two researchers who are bilingual. Incongruity of the two copies were reviewed and discussed until consensus was reached. The instrument was then blind back-translated into English by two researchers in the nursing field. Both of them had work experience in English-speaking countries. Again, the two versions were compared and verified by a qualified, bilingual expert who specializes in design and cross-cultural validation of study questionnaires. B) An expert panel, whose members were selected for their experience and professional knowledge, was asked to evaluate the content validity of the tool. The expert panel included two specialists in neurology, one rehabilitation therapist, one professor in a nursing school, and two advanced-practice nurses specialized in stroke nursing. Experts rated each item for the relevance and repetition using a content validity index. According to the experts’ rating, the content validity index of the Chinese version of the SCI Exercise Self-Efficacy Scale (C-ESES) can reach 0.95, demonstrating perfect content. C) Pilot study: in total, 15 Chinese stroke survivors evaluated if the C-ESES was easy to understand and answer. Psychometric testing of the scale was performed after completion of all these steps.
Data collection
Questionnaires were administered on the day of discharge. Participants finished the questionnaires on their own after they signed a written consent form, and assistance was provided if participants had difficulty to read the questions and write their answers independently. In addition, 50 stroke survivors who agreed to take the survey again were selected for the retest 10 days later.
Statistical analysis
The AMOS 20.0 and SPSS 17.0 were chosen to performing the data analysis.
Item analysis
The following criteria were chosen to distinguish the items to be omitted: A) a correlation between item and the total scale score (Item–Total Correlation) of less than 0.30 and B) no decrease in the Cronbach’s α if the item is deleted.20 Construct validity was first evaluated through EFA and then proved through confirmatory factor analysis with maximum likelihood. Items with a factor loading of 0.40 or greater were considered to adequately measure a factor. Goodness-of-fit criteria, including the chi-square/degree of freedom ratio (χ2/df) <3.00; root mean square error of approximation <0.08; and goodness-of-fit index, adjusted goodness-of-fit index, and comparative fit index ≥0.90, were used to determine the overall data-model fitness.21 Convergent validity was calculated using the correlation coefficients of the C-ESES and C-GSE.22
Internal consistency
A Cronbach’s α between 0.7 and 0.8 is considered minimally receivable, that from 0.8 to 0.9 respectable, and that more than 0.9 quite perfect.23
Test–retest reliability
A third approach used to evaluate reliability in our study was to determine the stability over time,24 which was conducted by calculating a correlation coefficient between the baseline test and retest 10 days later. Considering the drawback of using the Pearson’s correlation coefficient, the bias and 95% limits of agreement from a Bland–Altman plot were also reported.
Ethical considerations
Approval was obtained from the First Affiliated Hospital of Zhengzhou University’s ethics committee. Patients signed a consent form after the researchers explained the study protocols and explained that the study complied with information privacy principles and confirmed all the responses would be used for scientific research alone. The patients were free to withdraw from the study at any time, if they wished to.
Results
Sample characteristics
Even though 350 participants answered the questionnaires in the present study, useful data were obtained from 321 participants (response rate: 91.71%). Most of these stroke participants were male (63.86%), married (60.44%), and had one to two comorbid conditions (44.7%). The average age was 56.50 years. The social, demographic, and disease information of the participants is shown in Table 1.
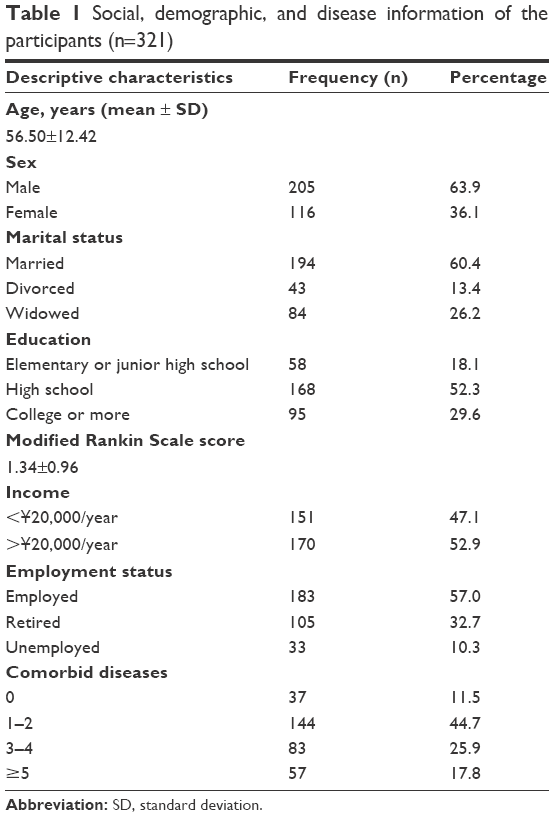 | Table 1 Social, demographic, and disease information of the participants (n=321) |
Item analysis
The average of each item score was from 2.95 to 3.48, which is shown in Table 2. Item–total correlations ranged from 0.551 to 0.718, indicating moderate to strong correlation. The deletion of any items in the scale would not have improved the Cronbach’s α of the scale (Table 2).
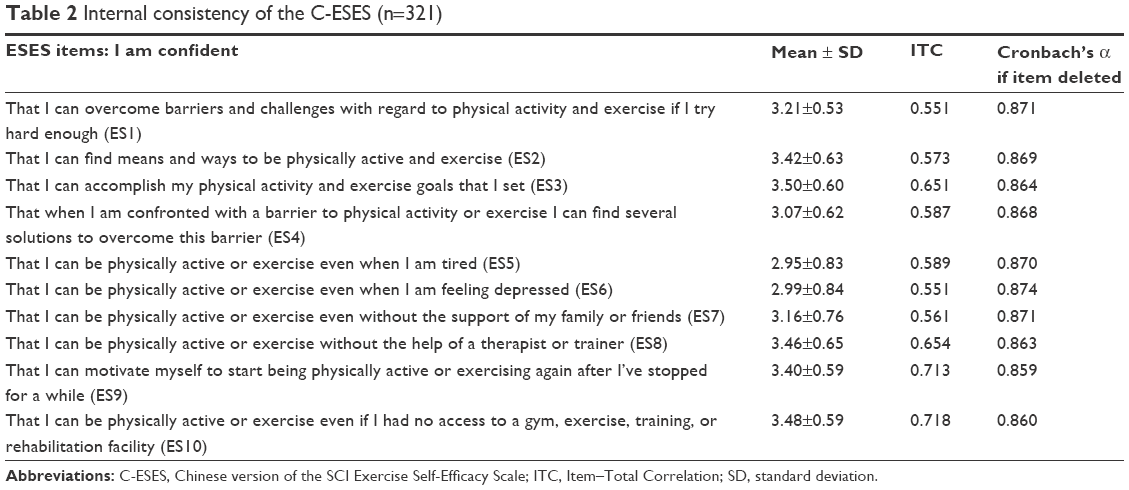 | Table 2 Internal consistency of the C-ESES (n=321) |
Exploratory principal components analysis
Before performing EFA, Kaiser–Meyer–Olkin, as well as Bartlett’s test of sphericity, was conducted to check if the data can be subjected to an EFA.25 The Kaiser–Meyer–Olkin measure was 0.841, which was better than the minimal admissible level of 0.50; Bartlett’s test was also admissible (χ2=1559.012; P<0.01), showing the suitability of an EFA.26 The principal component factor analysis showed that two underlying factors had Eigen values over 1, which accounted for 49.543% and 10.202% of the total variance, respectively. Table 3 shows the results of the component factor analysis using varimax rotation. All factor loadings, ranging from 0.620 to 0.806, were statistically significant in the two-factor model and greater than 0.4 (Table 3). The two-factor model was thus chosen to perform further tests, with the names given as internal motivation and external motivation.
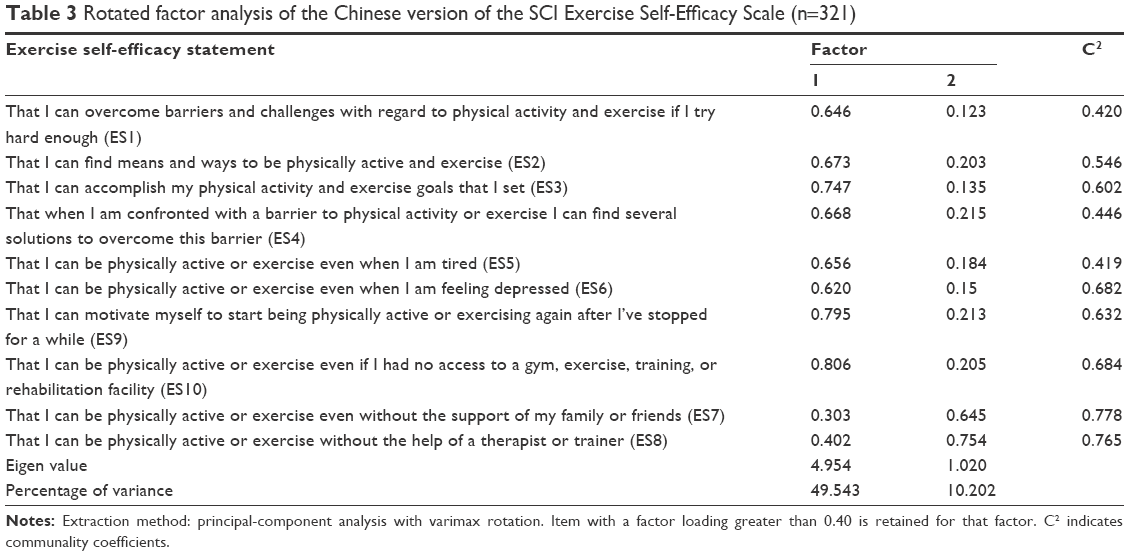 | Table 3 Rotated factor analysis of the Chinese version of the SCI Exercise Self-Efficacy Scale (n=321) |
To further test the structure of the C-ESES, the two-factor model derived from the EFA was compared with the original one-factor model suggested by Kroll et al.13 The latter model did not provide an acceptable fit to the data (χ2=398.625; df=193; P<0.001; root mean square error of approximation =0.081; goodness-of-fit index =0.825; adjusted goodness-of-fit index =0.789; comparative fit index =0.820), but the two-factor model did (χ2=291.157; df=185; P<0.001; root mean square error of approximation =0.044; goodness-of-fit index =0.938; adjusted goodness-of-fit index =0.914; comparative fit index =0.858).
Convergent validity
Pearson’s correlation coefficient of the C-ESES and C-GSE had a statistical significance (r=0.496, P<0.01), indicating the C-ESES had sound convergent validity when evaluating with C-GSE.
Internal consistency and split-half reliability
Cronbach’s α of the scale and its factors were 0.879, 0.872, and 0.757, respectively. We also assessed the split-half reliability of the tool, and acceptable internal consistency was proved in the split-half reliability assessment (split-half coefficient =0.911).
Test–retest reliability
Test–retest reliability of the C-ESES was optimal when the test was administered after 10 days later on 50 stroke survivors. The correlation coefficient between the baseline and 10-day follow-up test was 0.750 (P<0.01). Considering the drawback of Pearson’s correlation coefficient, a Bland–Altman plot was also used to report the bias and 95% limits of agreement. The mean differences and limit of agreements between the two methods were −1.28 (−7.47 to 4.91).
Discussion
It is of importance to find a validated measurement to evaluate exercise self-efficacy in stroke patients, especially in the People’s Republic of China. In our study, we performed the psychometric properties of the C-ESES in 321 Chinese stroke patients. The results demonstrated that C-ESES presented adequate validity and reliability to evaluate the exercise self-efficacy in patients with stroke in a comprehensive hospital.
An exploratory principal component factor analysis determined ten items loaded on two factors, which explained 59.745% of the total variance. Each item had a factor loading of 0.40 or higher, which was considered acceptable.27 However, these results were a little different from those reported in studies conducted by Bland et al14 and Kroll et al13 who suggested that exercise self-efficacy, assessed by ESES scale, was one-dimensional. However, the two-factor model was according to Hall’s theory of self-efficacy,28 which reported that work-related situations contain two factors (personal and environmental). Items 1–6, 9, and 10 should be included in the personal factor because these items mainly emphasize on one’s own efforts and self-awareness. The environmental factor assesses respondent’s self-efficacy from social support, including expectations and support from others. Items 7 and 8 could be categorized under the environmental factor because the two items mainly evaluated persistence of effort without assistance.
The C-ESES demonstrated acceptable convergent validity, which was the connection between two various scales evaluating an identical feature.29 A statistically significant connection between C-ESES and C-GSE was found (r=0.496, P<0.01), which revealed that the C-ESES performed with an excellent convergent validity when assessed against the C-GSE. The results were the same with the original version13 in which the connection was 0.316. Therefore, it was concluded that this scale was sensitive enough to evaluate the same feature as the C-GSE.
The Cronbach’s α of the scale and two factors, ranging from 0.757 to 0.879, showed an acceptable internal consistency; The result of split-half internal consistency test, with a correlation of 0.837 between the two halves, also proved the sound reliability of C-ESES.30 The results were consistent with the English version13 in which the Cronbach’s α and correlation between the two halves were 0.926 and 0.791. It was a pity that test–retest reliability had not been examined in the original version. Therefore, the test–retest reliability test was conducted to decide the steadiness of reliability as time went by. The C-ESES showed good reliability after a 10-day interval, with a correlation coefficient of 0.750 (P<0.01). Time interval between baseline test and retest might influence the test–retest reliability. A shorter time interval may generate cross-reaction, whereas a longer interval may increase the possibility for unexpected changes in scores.31 With reference to the suitable time interval to evaluate test–retest reliability, experts suggest a time interval ranging from hours to years, according to the aims. However, an interval of 2–14 days is considered optimal. In this research, 10 days was chosen because stroke survivors usually visit the hospital for a follow-up 10 days after discharge, which was consistent with the recommended interval.
Limitations
Some limitations of this study deserve emphasis. Firstly, regular exercise was measured using self-report, which was inclined to result in a misestimate of exercise level as compared with more objective measurements.32 Secondly, we included only cases with complete data in our analyses. Cases with more than one missing value on any of the variables were deleted, which restricts the generalizability of these results. In addition, in this study, the translation procedure was conducted by the authors themselves, which may have been less accurate as compared with that conducted by a professional bilingual translator, or by using multiple techniques.
Conclusion
The results of this study prove the use of the 10-item C-ESES to evaluate exercise self-efficacy in Chinese-speaking stroke survivors. Moreover, the ten item C-ESES is comparatively simplified and easy to understand. Usage of C-ESES may urge health care professionals to better know stroke survivors’ exercise self-efficacy and utilize psychological methods to improve their physical activity.
Acknowledgments
We thank Thilo Kroll (Universities of Dundee and St Andrews, School of Nursing and Health Sciences) for authorizing the cross-cultural translation of the scale into Chinese. We also thank all the professors for their essential contribution and support.
Disclosure
The authors report no conflicts of interest in this work.
References
Zhao JJ, He GQ, Gong SY, He L. Status and costs of primary prevention for ischemic stroke in China. J Clin Neurosci. 2013;20(10):1427–1432. | ||
Hackam DG, Spence JD. Combining multiple approaches for the secondary prevention of vascular events after stroke: a quantitative modeling study. Stroke. 2007;38(6):1881–1885. | ||
Sacco RL, Gan R, Boden-Albala B, et al. Leisure-time physical activity and ischemic stroke risk: the Northern Manhattan stroke study. Stroke. 1998;29(2):380–387. | ||
Soares-Miranda L, Siscovick DS, Psaty BM, Longstreth WT, Mozaffarian D. Physical activity and risk of coronary heart disease and stroke in older adults: The cardiovascular health study. Circulation. 2016;133(2):147–155. | ||
Roberts V, Maddison R, Simpson C, Bullen C, Prapavessis H. The acute effects of exercise on cigarette cravings, withdrawal symptoms, affect, and smoking behaviour: systematic review update and meta-analysis. Psychopharmacology (Berl). 2012;222(1):1–15. | ||
Gordon NF, Gulanick M, Costa F, et al. Physical activity and exercise recommendations for stroke survivors: An American heart association scientific statement from the council on clinical cardiology, subcommittee on exercise, cardiac rehabilitation, and prevention; the council on cardiovascular nursing; the council on nutrition, physical activity, and metabolism; and the stroke council. Circulation. 2004;109(16):2031–2041. | ||
Field M, Gebruers N, Shanmuga Sundaram T, Nicholson S, Mead G. Phsical activity after stroke: a systematic review and meta-analysis. ISRN Stroke. 2013;2013:1–13. | ||
Tudor-Locke C, Jones R, Myers AM, Paterson DH, Ecclestone NA. Contribution of structured exercise class participation and informal walking for exercise to daily physical activity in community-dwelling older adults. Res Q Exerc Sport. 2002;73(3):350–356. | ||
Tudor-Locke C, Craig CL, Brown WJ, et al. How many steps/day are enough? For adults. Int J Behav Nutr Phys Act. 2011;8:79. | ||
Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: review and update. Med Sci Sports Exerc. 2002;34(12):1996–2001. | ||
Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. | ||
Nicholson SL, Donaghy M, Johnston M, et al. A qualitative theory guided analysis of stroke survivors’ perceived barriers and facilitators to physical activity. Disabil Rehabil. 2014;36(22):1857–1868. | ||
Kroll T, Kehn M, Ho PS, Groah S. The SCI Exercise Self-Efficacy Scale (ESES): development and psychometric properties. Int J Behav Nutr Phys Act. 2007;4:34. | ||
Bland HW, Melton BF, Marshall ES, Nagle JA. Measuring exercise self-efficacy in pregnant women: psychometric properties of the pregnancy-exercise self-efficacy scale (P-ESES). J Nurs Meas. 2013;21(3):349–359. | ||
Fliess-Douer O, Vanlandewijck YC, van der Woude LH. Reliability and validity of perceived self-efficacy in wheeled mobility scale among elite wheelchair-dependent athletes with a spinal cord injury. Disabil Rehabil. 2013;35(10):851–859. | ||
Bamford JM, Sandercock PA, Warlow CP, Slattery J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1989;20(6):828. | ||
Cheung SK, Sun SY. Assessment of optimistic self-beliefs: further validation of the Chinese version of the general self-efficacy scale. Psychol Rep. 1999;85(3 Pt 2):1221–1224. | ||
Leung DY, Leung AY. Factor structure and gender invariance of the Chinese general self-efficacy scale among soon-to-be-aged adults. J Adv Nurs. 2011;67(6):1383–1392. | ||
Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. | ||
Ferketich S. Focus on psychometrics. Aspects of item analysis. Res Nurs Health. 1991;14(2):165–168. | ||
Byrne BM. Structural Equation Modeling with LISREL, PRELIS and SIMPLIS: Basic Concepts, Applications, and Programming. New Jersey: Lawrence Erlbraum Associates; 1998. | ||
Portney LG, Watkins MP. Foundations of Clinical Research. Applications to Practice. 3rd ed. New Jersey: Pearson Education, Inc; 2009. | ||
Nunnally JC, Bernstein RL. Psychometric Theory. 3rd ed. New York: McGraw-Hill; 1994. | ||
Kramer MS, Feinstein AR. Clinical biostatistics. LIV. The biostatistics of concordance. Clin Pharmacol Ther. 1981;29(1):111–123. | ||
Norusis M. SPSS 15.0 Guide to Data Analysis. Prentice Hall: Upper Saddle River; 2007. | ||
George D, Mallery P. SPSS for Windows Step by Step: A Simple Guide and Reference. 6th ed. Boston: Allyn & Bacon; 2006. | ||
Mulaik SA. Foundations of Factor Analysis. 2nd ed. New York: Chapman & Hall; 2009. | ||
Hall GSM. Self-efficacy at work: a quality analysis of personal and environmental factors contributing to personal efficiency during job-task change. Dissertation Abstracts International A (Humanities and Social Sciences). 2000;61(3–A):916. | ||
Polit DF, Beck CT. Nursing Research: Principle and Method. Philadelphia: Lippincott Williams & Wilkins; 2004. | ||
Toronto B. Fundamentals of Biostatistics. 7th ed. Toronto: Cengage Learning Inc; 2010. | ||
Streiner DL, Norman GR. Health Measurement Scales: A Practical Guide to their Development and Use. 4th ed. New York: Oxford Scholarship; 2008. | ||
Hagstromer M, Oja P, Sjostrom M. Physical activity and inactivity in an adult population assessed by accelerometry. Med Sci Sports Exerc. 2007;39(9):1502–1508. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.