")
Back to Journals » Clinical Interventions in Aging » Volume 17
The P.R.OS.T.A.T.E Nomogram for the Preoperative Prediction of Clinical Efficacy of Transurethral Resection of the Prostate in Benign Prostatic Hyperplasia Patients
Authors Tian Y , Zhang H, Cao Y, Yang L, Luo G
Received 6 March 2022
Accepted for publication 14 May 2022
Published 23 May 2022 Volume 2022:17 Pages 845—855
DOI https://doi.org/10.2147/CIA.S365282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Ye Tian,1,2 Heng Zhang,1,2 Ying Cao,2 Lu Yang,3 Guangheng Luo1
1Department of Urology, Guizhou Provincial People’s Hospital, Guiyang, People’s Republic of China; 2Guizhou University School of Medicine, Guiyang, People’s Republic of China; 3Department of Urology, West China Hospital, Sichuan University, Chengdu, People’s Republic of China
Correspondence: Guangheng Luo, Tel +86-173-8501-5539, Fax +86-851-8562 1836, Email [email protected]
Purpose: Transurethral resection of the prostate (TURP) is often indicated for benign prostatic hyperplasia (BPH). Some patients, however, fail to adequately respond to these interventions. Accordingly, a powerful prediction model for TURP efficacy is warranted. This study aimed to create a nomogram with preoperative parameters for the prediction of individual TURP efficacy.
Methods: Clinical data from 356 BPH subjects who underwent TURP were retrospectively collected between November 2015 and June 2021 for nomogram development. The prediction model was developed using multivariable logistic regression analysis and presented as a nomogram. Nomogram performance was assessed through calibration curves and the concordance index (C-index). An independent validation cohort containing 177 consecutive patients in the corresponding period was used for external validation. The optimal cutoff value was determined through receiver operating characteristic curve (ROC) analysis by maximizing the Youden index, and its accuracy was assessed through sensitivity, specificity and predictive values.
Results: In multivariate analysis of the primary cohort, the independent factors for TURP efficacy were age, International Prostate Symptom Score (IPSS), intravesical prostatic protrusion (IPP), bladder wall thickness (BWT), peripheral zone thickness (PT) and transitional zone thickness (TT), all of which were included in the nomogram. The calibration curve for survival probability showed good agreement between the nomogram predictions and actual observations. The C-index for predicting TURP efficacy was 0.860 (95% confidence interval [CI], 0.808– 0.911). The optimal cutoff total nomogram score was 177, with a maximum Youden index of 0.643. The sensitivity, specificity, positive predictive value, and negative predictive value for predicting TURP efficacy were 70.6%, 75.6%, 90.6%, and 43.7% in the validation cohort, respectively. Logistic regression analysis in the validation cohort demonstrated that the area under the curve (AUC) was 0.806 (95% CI, 0.733– 0.879).
Conclusion: The P.R.OS.T.A.T.E nomogram objectively and accurately predicted TURP efficacy, thereby facilitating the clinical decision-making process.
Keywords: nomogram, benign prostatic hyperplasia, lower urinary tract symptoms, transurethral resection of prostate, efficacy
Introduction
Benign prostatic hyperplasia (BPH) results in a benign enlargement of the transitional zone (TZ) and periurethral area.1 The management of men with BPH and bothersome lower urinary tract symptoms (LUTS) may initially start with conservative measures or medical therapies.2 Many patients have symptomatic progression that is refractory to these therapies, necessitating surgical intervention.2–4 Transurethral resection of the prostate (TURP) removes the obstruction adenoma related to benign enlargement and is still regarded as the surgical standard for treating moderate to severe bothersome LUTS secondary to benign prostatic obstruction (BPO).3,5
Some patients, however, fail to adequately respond to surgical interventions.3,4 Age, baseline LUTS prior to TURP, intravesical prostatic protrusion (IPP) and some biomarkers have been regarded as predictors of LUTS following TURP. Kim et al3 suggested that when counseling patients prior to TURP, it would be helpful to use preoperative characteristics to stratify their risk for reduced TURP efficacy, and the authors believed it was necessary to precisely predict which patients would benefit from TURP.
Owing to the lack of a specific and practical predictive method, a predictive model that incorporates factors associated with TURP efficacy that can be assessed preoperatively is needed. Some scholars have attempted to build models to predict BPH surgical efficacy.6,7 However, these studies are unsatisfactory because of their small size, variable selection limitations, the lack of external validation and the unsatisfactory results. In the present study, we aimed to identify clinical factors associated with TURP efficacy using a large cohort of patients. In particular, we sought to create and internally validate nomograms for individual predictions of TURP efficacy.
Subjects and Methods
Subjects
Ethical approval from the Ethics Committee of the Guizhou Provincial People’s Hospital (No. 2021-66) was obtained, and the informed consent requirement was waived due to the retrospective nature. Patient data were confidentially accessed, and the study fully complied with the Helsinki Declaration. The data of a consecutive series of BPH patients treated with TURP between November 2015 and June 2021 were retrospectively collected at Guizhou Provincial People’s Hospital and West China Hospital, Sichuan University.
The subjective symptoms of all patients were scored according to the International Prostate Symptom Score (IPSS) and quality of life (QoL) score. In addition, physical examinations including digital rectal examination (DRE), prostate-specific antigen (PSA) level, transabdominal kidney-bladder ultrasound, transrectal ultrasound (TRUS) (Philips EPIQ 5 ultrasound machine, Amsterdam, Netherlands), postvoid residual urine (PVR), and maximum flow rate (Qmax) were performed for all patients. Patients with suspected prostate cancer also underwent ultrasound-guided transrectal 12-core needle biopsy to confirm the BPH diagnosis.
The exclusion criteria were as follows: incomplete medical records; previous bladder, prostate, or urethra operation; urethral stricture; IPSS ≤ 7; prostate or bladder cancer; bladder stones; acute or chronic urinary tract infection; neurogenic bladder dysfunction; uncontrolled diabetes mellitus; and any comorbidities that could affect the patient’s voiding function. Patients with an unmeasurable peripheral zone thickness (PT) and/or transitional zone thickness (TT) were also excluded.
Assessment of Clinical Variables
Total prostate volume (TPV) and transitional zone volume (TZV) were calculated from TRUS measurements of the prostate using the prostate ellipsoid formula (height × width × length × π/6). The transitional zone index (TZI) was calculated by dividing the TZV by the TPV. PT was defined as the longest distance between the outer and inner margins of the peripheral zone when a straight line was drawn from the center of the transitional zone to the outer margin of the peripheral zone on image sections showing the maximal TZV, as described by Kwon et al8,9 TT was defined by a straight line passing through the center of the transitional zone from one margin to the other. The transitional/peripheral zone index (TPI) was calculated by dividing the TT by the PT. IPP was measured as previously reported by Franco et al.10 Briefly, IPP was calculated as the vertical distance from the tip of the protrusion to the circumference of the bladder at the base of the prostate gland in the midsagittal plane using transabdominal ultrasonographic imaging. Bladder wall thickness (BWT) was measured in the horizontal direction at maximum magnification. A minimum of three measurements were made from the anterior or lateral walls and averaged to obtain the BWT. All ultrasonographic procedures were performed by two experts blinded to the clinical variables.
TURP Efficacy Evaluation
Postoperative reevaluation was arranged 3–6 months after TURP at the outpatient clinic and included uroflowmetry, TRUS, IPSS and QoL assessments. The study endpoint was an evaluation of treatment efficacy using the follow-up criteria (pre/postoperative changes in IPSS, QoL, Qmax and TPV) (Table 1). Treatment was defined to be effective when two or more of the postoperative results were excellent or good and ineffective otherwise.11,12
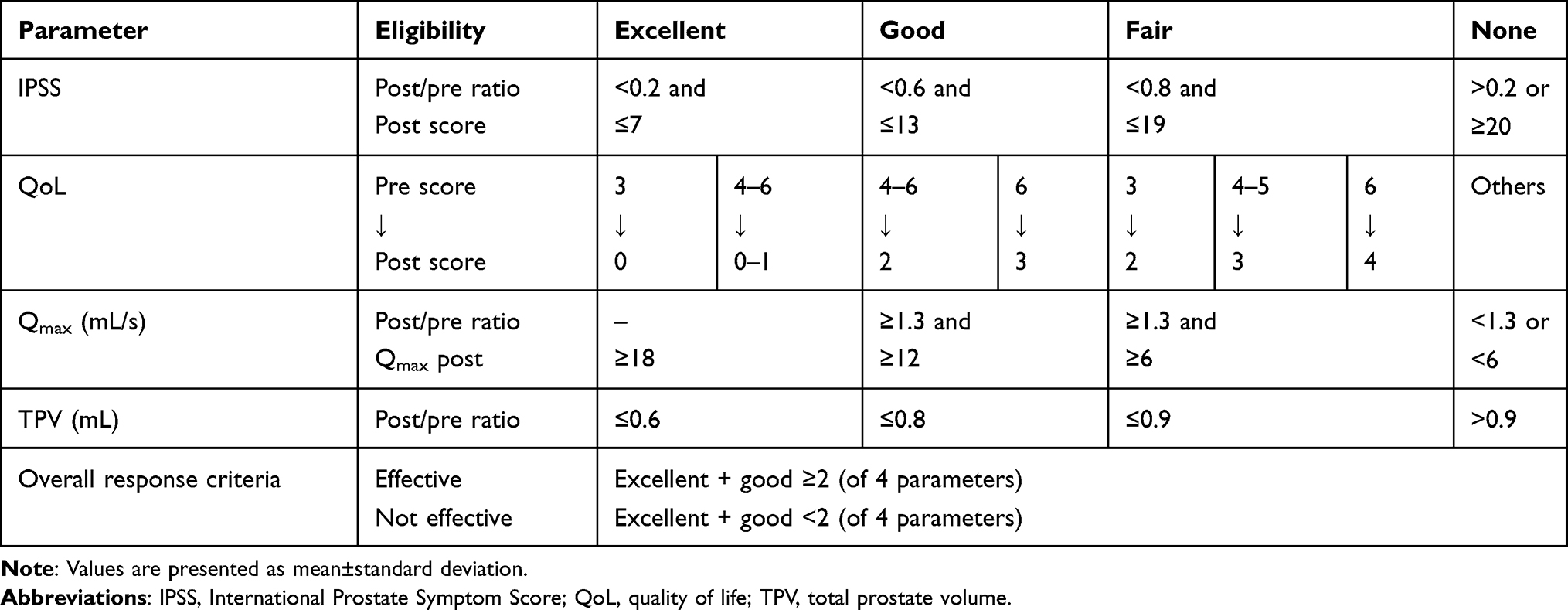 |
Table 1 Response Criteria for Individual Patient |
Statistical Analysis
Baseline clinical data including age, PSA, IPSS, QoL, Qmax, PVR, IPP, BWT, TPV, TZV, TZI, TT, PT and TPI were derived or calculated from medical records. Continuous variables are reported as the mean±standard deviation and were compared between the primary and validation cohorts using an unpaired, two-tailed t-test. Variables were also compared between the effective and ineffective groups in the primary cohort. The significance of each variable in the primary cohort was assessed by univariate regression analysis to identify the potential risk factors affecting TURP efficacy. All variables significantly associated with TURP efficacy were candidates for stepwise multivariate logistic analysis for further evaluation as potential predictors. The statistical analyses described above were performed using SPSS 22.0 for Windows (SPSS, Chicago, IL). A P < 0.05 was considered statistically significant.
A nomogram was constructed based on the results of the multivariate logistic analysis using the rms package in R 4.1.1 (http://www.r-project.org). The performance of the nomogram was measured by the C-index (which is equivalent to the area under the receiver operating characteristic curve) and through receiver operating curve (ROC) analysis; the larger the C-index is, the more accurate the prognostic prediction. Bootstrapping with 1000 resamples was used for these analyses to decrease the overfit bias.
Internal validation was performed using calibration curves. The stability of the prediction models was confirmed with the validation cohort. During external validation of the nomogram and clinical use of the model, the total scores of each patient were calculated with the nomogram. ROC analysis was used to calculate the optimal cutoff values, which were determined by maximizing the Youden index (ie, sensitivity + specificity - 1). The accuracy of the optimal cutoff value was assessed by sensitivity, specificity and predictive values.
Results
Patient Characteristics
After applying the exclusion criteria, 533 eligible patients were included. In total, 356 patients who received TURP in Guizhou Provincial People’s Hospital were included in the primary cohort to develop the nomogram, and the other 177 patients from West China Hospital were assigned to the validation cohort. The characteristics of the patients in the primary and validation cohorts are listed in Table 2. There were no significant differences between the two cohorts regarding age (P=0.841), PSA level (P=0.816), IPSS (P=0.718), QoL score (P=0.407), Qmax (P=0.261), PVR (P=0.289), IPP (P=0.271), BWT (P=0.079), TPV (P=0.128), TZV (P=0.359), TZI (P=0.525), PT (P=0.258), TT (P=0.195) and TPI (P=0.750). In the primary cohort, surgery was considered effective in 289 patients (81.2%) and ineffective in 67 (18.8%) (Table 3). Those who responded to TURP were younger (P<0.001), had worse IPSS (P<0.001) and Qmax (P=0.006) values, and had more significant IPP (P<0.001) but thinner BWT (P=0.030). The TPV (P<0.001), TZV (P<0.001), TZI (P<0.001), TT (P<0.001) and TPI (P<0.001) were larger for the patients who responded to TURP. The PT, however, was thicker for patients who did not respond to TURP (P<0.001).
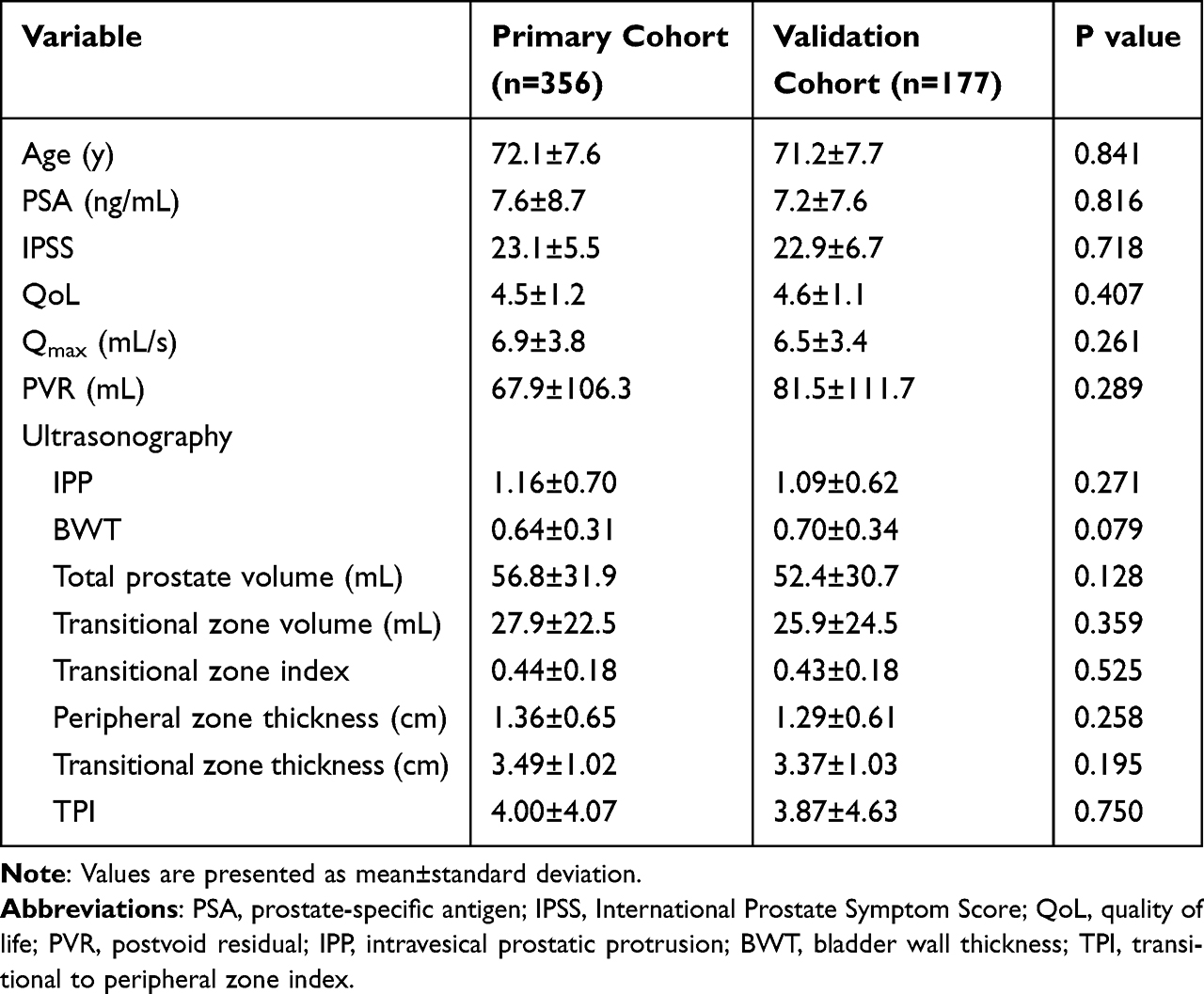 |
Table 2 Clinical Characteristics of the Patients in Primary Cohort and Validation Cohort |
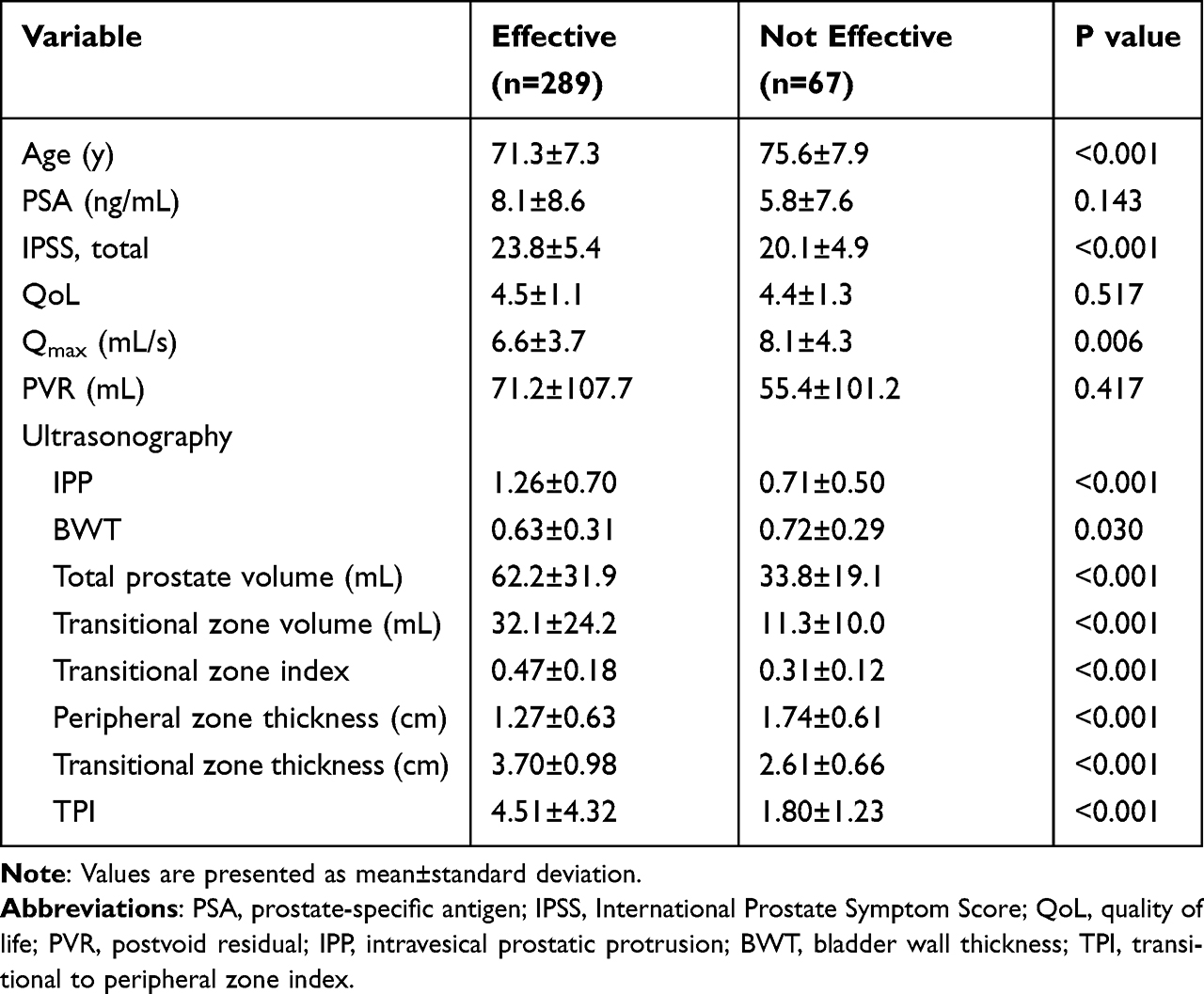 |
Table 3 Clinical Characteristics of the Patients Treated with TURP in the Primary Cohort (n=356) |
Correlation Analysis Between TURP Efficacy and Clinical Variables in the Primary Cohort
All variables listed above were entered for univariate and multivariate logistic regression analysis. The predictors of TURP efficacy are listed in Table 4. Multivariate logistic regression analysis showed that age (odds ratio (OR), 0.886; 95% confidence interval (CI), 0.841–0.934), IPSS (OR, 1.173; 95% CI, 1.089–1.264), IPP (OR, 2.707; 95% CI, 1.172–6.250), BWT (OR, 0.128; 95% CI, 0.037–0.443), PT (OR, 0.516; 95% CI, 0.277–0.962) and TT (OR, 3.468; 95% CI, 1.866–6.446) were independent predictors of TURP efficacy.
 |
Table 4 Logistic Regression Analysis for TURP Efficiency of BPH Patients in the Primary Cohort |
Development and Validation of a Nomogram Predicting TURP Efficacy
The independently associated risk factors were used to form a nomogram to predict TURP efficacy (Figure 1). The probability of effective TURP can be determined by assigning points for each variable by drawing a line upward from the corresponding variable to the points line, summing the points, and identifying the prediction associated with the total points line. The nomogram demonstrated good accuracy in estimating the likelihood of TURP efficacy, with a C-index (which was equivalent to the area under the curve (AUC)) of 0.860 (95% CI, 0.808–0.911) (Figure 2A). In addition, calibration plots graphically showed good agreement between the nomogram prediction and the actual TURP efficacy determined through follow-up (Figure 3), again indicating that the current model has great prediction value.
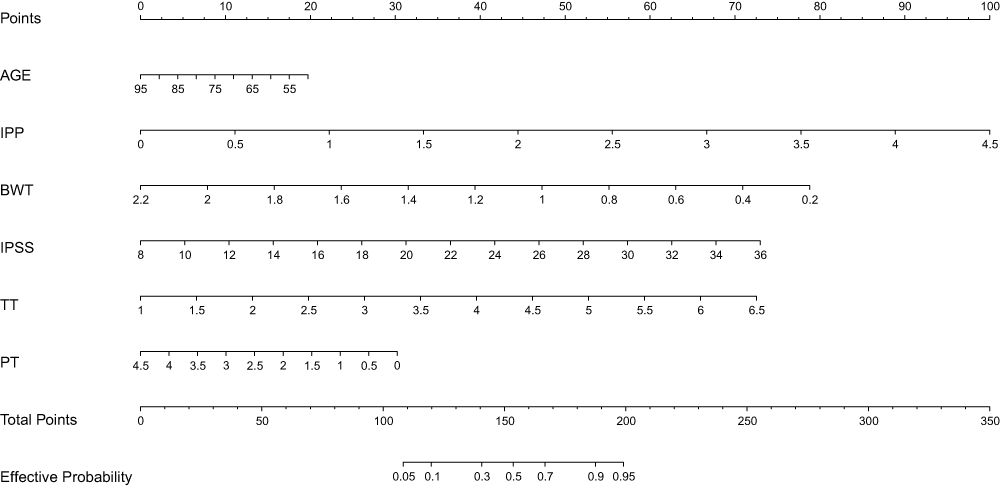 |
Figure 1 The nomogram to predict TURP efficacy. The nomogram was created based on six independent prognostic factors. Points are assigned for each variable by drawing a line upward from the corresponding variable to the points line. The sum of the points plotted on the total points line corresponds with the predicted probability for effective TURP. |
 |
Figure 2 The ROC curves of the prediction models for TURP efficacy. (A) The ROC curve of the prediction model for TURP efficacy in the primary cohort. (B) The ROC curve of the prediction model for TURP efficacy in the validation cohort. The AUC (equivalent to the C-index) of the model was 0.860 (95% CI, 0.808–0.911) in the primary cohort and 0.806 (95% CI, 0.733–0.879) in the validation cohort. |
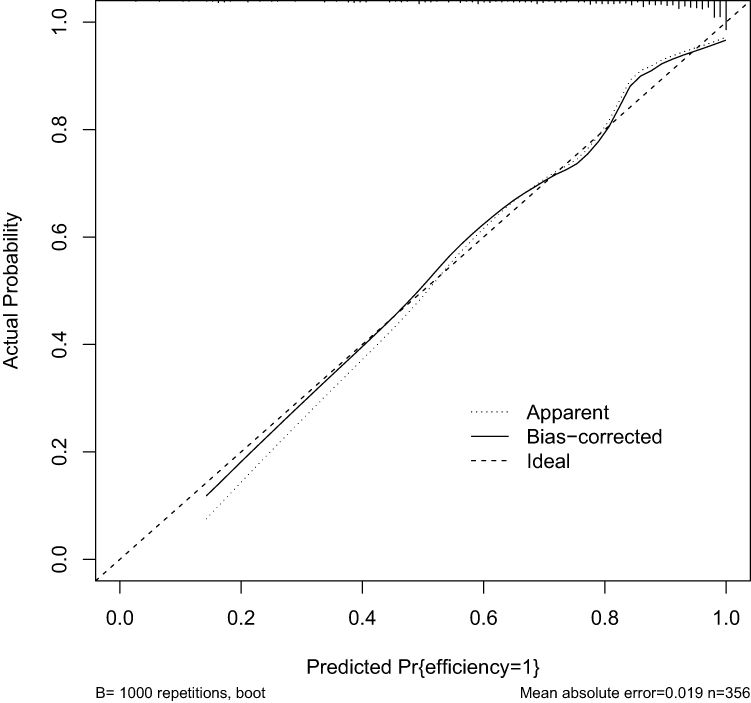 |
Figure 3 Validity of the predictive performance of the nomogram in predicting TURP efficacy in the primary cohort (n=356). The calibration curves of the prediction model for TURP efficacy. The nomogram-predicted probability is plotted on the x-axis, and the actual probability is plotted on the y-axis. |
To further assess the discriminative ability of the nomogram, external validation was performed (validation data were independently collected in West China Hospital). The optimal cutoff value of the total nomogram score was determined to be 177, with a maximum Youden index of 0.643. The sensitivity, specificity, positive predictive value, and negative predictive value when using this cutoff to predict TURP efficacy were 79.2% (95% CI, 74.0–84.1%), 85.1% (95% CI, 81.2–88.8%), 90.8% (95% CI, 86.1–94.7%), and 62.3% (95% CI, 58.6–65.8%) in the primary cohort and 70.6% (95% CI, 66.5–74.4%), 75.6% (95% CI, 72.6–78.4%), 90.6% (95% CI, 87.1–93.7%), and 43.7% (95% CI, 39.5–46.8%) in the validation cohort, respectively (Table 5). ROC curves based on the logistic regression analysis of the validation cohort demonstrated that the AUC was 0.806 (95% CI, 0.733–0.879) (Figure 2B).
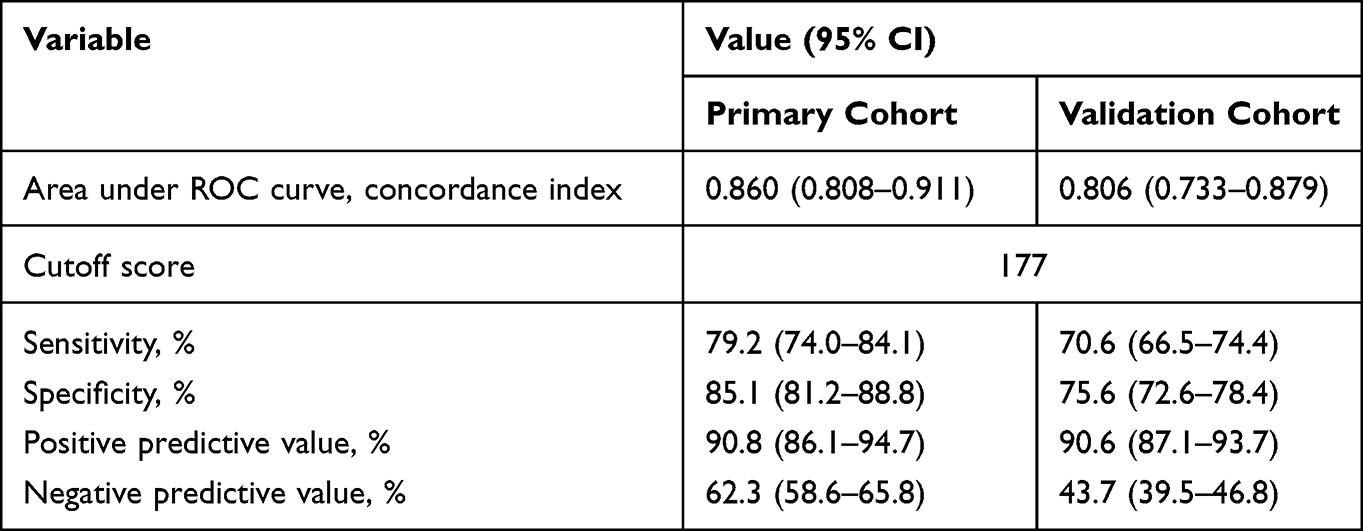 |
Table 5 Accuracy of the Prediction Score of the Nomogram for Estimating the TURP Efficacy |
Discussion
TURP has been used for more than nine decades, defining the cornerstone of surgical treatment for LUTS/BPH. However, a small portion of BPH patients experience persistent LUTS following TURP.3 Identifying which patients are unlikely to benefit from TURP is critical but far from being achieved. In the current study, multivariate logistic regression analysis revealed that age, IPSS, IPP, BWT, PT and TT (comprehensive and easily available preoperative variables) were independent predictors of TURP efficacy. Therefore, we developed and validated a nomogram based on clinical characteristics that incorporated these six items to predict the clinical efficacy of TURP in BPH patients. The nomogram performed well in estimating the probability for effective TURP, and its prediction was supported by the C-index (0.860 and 0.806 for the primary and validation cohorts, respectively) and the calibration curve. This nomogram can correspond to using the acronym P.R.OS.T.A.T.E where P stands for protrusion (IPP), R refers to the radius (thickness) of the TZ (TT), OS is short for overall symptoms (IPSS), T quantifies the bladder wall thickness (BWT), A represents the age of the patients (age), and E refers to the external (peripheral) zone thickness (PT).
Antunes et al13 studied 46 patients with bladder outlet obstruction (BOO) due to BPH who were treated with TURP, and they found that patients with persistent detrusor overactivity were significantly older than those successfully treated. Similarly, Seki et al14 believed that older males experienced less improvement of nocturia symptoms after undergoing TURP. These conclusions were reinforced by the findings of Choi et al15 and De Nunzio et al6 who also demonstrated that age was consistently and independently associated with persistent storage symptoms after TURP. Although not necessarily widely accepted, these findings may reflect the importance of bladder aging in functional changes regarding homeostatic reserve and sensory mechanisms.16 In this study, our results indicated that younger age was associated with better responses to TURP, which was consistent with these publications.
Rhodes et al17 calculated a 1.6% average annual increase in prostatic volume in the Olmstead study. However, it remains unclear whether prostate volume is correlated with symptom scores and QoL scores.18,19 Researchers have suggested that transitional zone growth is the main contributor to total prostate growth, while no age-related increases have been found with regard to peripheral zone volume (PZV). The more the TZV increases, the higher the obstructive pressure and the thinner the peripheral zone (PZ) becomes.8,18,19 Milonas et al12 reported that a lower TZI was an independent predictor of ineffective surgery. Furthermore, they detected a significant correlation between removed tissue weight and TZV. In our study, TPV, TZV, TZI and TT were positively correlated with TURP efficacy in univariate logistic regression analysis, whereas only TT showed significance in the multivariate logistic regression analysis. The results could be attributed to the collinearity among these variables.20 In the current study, PT was negatively correlated with TURP efficacy in both univariate and multivariate logistic regression analyses, which agrees with the findings of Matsugasumi et al21 and our previous results9 to a certain extent.
The degree of preoperative LUTS and improvement observed following TURP remain controversial. Choi et al15 showed that an initially worse degree of storage symptoms was consistently associated with persistent storage symptoms. However, some publications22 have reported no significant differences in postoperative storage symptom scores between patients with and without detrusor overactivity. This study excluded patients with bladder dysfunction comorbidities, but we demonstrated that a worse baseline IPSS was associated with a better response to surgery. These results could be interpreted as indicating that patients with moderate baseline IPSS were less likely to benefit most from TURP.
IPP is a phenomenon in which the prostate lobe enlarges into the bladder along the plane of least resistance. It has been reported that IPP is a more useful predictor of BOO caused by BPH than TPV, TZV, TZI, and PSA.10 Matsukawa et al23 suggested that IPP was a strong factor for predicting the therapeutic effects of silodosin. Nevertheless, Lin et al24 showed that prostate artery embolization resulted in both significant IPP reduction and significant symptomatic improvement, and these improvements were positively correlated. Not surprisingly, our results were in accordance with these studies and demonstrated that IPP was positively correlated with surgical efficacy. Protrusion of the prostate results in a ball-valve-type obstruction, disrupting the funneling effect of the neck of the bladder and resulting in an increase in urethral resistance during micturition, although the detailed mechanism remains incompletely understood. In addition, median lobe hypertrophy may cause dyskinetic movement during micturition.25 Accordingly, we propose that removing the portion of the prostate with intravesical protrusion may represent one of the essential points of the surgical protocol.
There is evidence that increased BWT has the potential to serve as a noninvasive parameter for the evaluation of detrusor activity.10,26 Detrusor muscle hypertrophy, which can be recognized as increased BWT, is a well-recognized clinical finding seen in obstructive disorders such as neurogenic bladder dysfunction and BPH. De Nunzio et al26 indicated that BWT can noninvasively predict the presence of detrusor underactivity in patients with LUTS and BPO using a multivariable logistic age-adjusted regression model. The importance of BWT on TURP outcome was reaffirmed in our current study.
Generally, Qmax is regarded as an obstruction indicator of BPH without bladder dysfunction. De Nunzio et al6 established a nomogram for predicting the outcome after TURP, and they believed Qmax was an independent risk factor. However, Qmax was negatively correlated with TURP efficacy in only the univariate logistic regression analysis but not multivariate logistic regression analysis. We speculate that this might be partly attributed to the differences in study methods, as this discrepancy is somewhat surprising.
Consistent response criteria for determining therapeutic efficacy for BPH have not been standardized, although many definitions of a successful outcome exist in the literature. In the present study, a simplified and validated four-parameter (IPSS, QoL, TPV and Qmax) form proposed by Homma et al27 was adopted. These subjective and objective parameters are routinely used for both treatment option decision-making and efficacy evaluation and are also fairly accurate, simple, and practical. This form, therefore, may represent a standard method for assessing the clinical efficacy of TURP.
Recently, De Nunzio et al6 enrolled 232 BPH patients and developed a nomogram with consideration of Qmax and IPSS. TURP success was defined as a rise in Qmax of at least 100% and an IPSS reduction of at least 50%. The nomogram presented an AUC of 0.77 (95% CI: 0.70–0.83). At the best cutoff value, the sensitivity was 62%, the specificity was 73%, the positive predictive value was 81%, and the negative predictive value was 52%. However, it should be noted that the study omitted bladder and prostate factors. Another limitation of that study is that the variable selection procedure was not clear. Nevertheless, the absence of external validation limits the clinical use of the nomogram, and the model cannot be applied to all patients undergoing TURP. Another study7 enrolled 96 BPH patients who received holmium laser enucleation of the prostate (HoLEP), and a prediction model was established based on preoperative age, PVR, IPSS-voiding/storage score ratio, IPP and Qmax. However, the study population was small, and the surgical efficacy evaluation was subjective as only IPSS and QoL were considered. Moreover, no external validation of the nomogram was performed.
Nomograms are advantageous because they provide individualized risk assessments in a user-friendly and dynamic manner. To the best of our knowledge, the present study is the first to develop a prediction model to consider potential risk variables and assess them independently for their inclusion in a formal nomogram for TURP efficacy. This study has several advantages. First, the study cohort was relatively large, as 533 patients (356 in the primary cohort and 177 in the validation cohort) were included. Second, the TURP response criteria used in the study are from a validated assessment system that consists of both subjective and objective parameters. Furthermore, the nomogram was validated in a cohort from another institution, which strengthens its reliability and applicability. Finally, when compared with other prediction systems, our nomogram showed better accuracy and performance for predicting TURP efficacy.6,7
There are some limitations to the current study. First, this study was based on data from a retrospective analysis, and patients who did not complete follow-up were excluded, which may lead to bias. A prospective study is required to further confirm the reliability of the nomogram. Second, all included patients were Chinese. Several studies have shown significantly smaller prostate size and higher tolerance of TURP in Asian men than in Caucasian men,28 and the nomogram should be used with caution for patients of other ethnicities. Third, heterogeneity in the patients’ medication history was not evaluated. In particular, 5α-reductase inhibitors have been deemed to alter the prostate zone anatomy because these drugs target glandular epithelial tissue.29 Kwon et al8 however, found similar PT and clinical variable correlations in BPH patients between those with and without a history of using such medications. Another point should be noted, as patients included in this study were treated with TURP, it remains uncertain whether patients who receive HoLEP or other procedures could be evaluated with the current nomogram. Furthermore, the nomogram achieved good predictive accuracy; at a cutoff point of 177, the nomogram had a sensitivity and specificity of 79.2% and 85.1% in the primary cohort and 70.6% and 75.6% in the validation cohort, respectively. However, the negative predictive value was unsatisfactory, at only 62.3% in the primary cohort and 43.7% in the validation cohort. The overwhelming number of effective surgeries in our study further illustrates the nomogram’s weakness to identify patients who are less likely to benefit from TURP. Therefore, we recommend that patients should not refuse TURP based on the current nomogram.
Conclusions
By combining 6 preoperative risk factors, the P.R.OS.T.A.T.E nomogram proposed in this study objectively and accurately predicted TURP efficacy, thereby facilitating the clinical decision-making process for both clinicians and patients. Additional studies are required to determine whether the nomogram can be applied to other patient groups (such as patients who received HoLEP) and patients of other ethnicities.
Acknowledgments
This study was supported by grants from the research program of the National Science Foundation of China (No. 81860141 and 82160149), Science and Technology Foundation of Guizhou Province (No. [2021]378 and [2019]2797) and Doctoral Foundation of Guizhou Provincial People’s Hospital (No. GZSYBS[2016]11).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare no competing interests in this work.
References
1. McNeal J. Pathology of benign prostatic hyperplasia. Insight into etiology. Urol Clin North Am. 1990;17(3):477–486. doi:10.1016/S0094-0143(21)00961-7
2. Bortnick EM, Simma-Chiang V, Kaplan SA. Long-term consequences of medical therapy for benign prostatic hyperplasia. Rev Urol. 2019;21(4):154–157.
3. Kim SJ, Al Hussein Alawamlh O, Chughtai B, et al. Lower urinary tract symptoms following transurethral resection of prostate. Curr Urol Rep. 2018;19(10):85–91. doi:10.1007/s11934-018-0838-4
4. Zhao Y, Liu W, Guralnick M, et al. Predictors of short-term overactive bladder symptom improvement after transurethral resection of prostate in men with benign prostatic obstruction. Int J Urol. 2014;21(10):1035–1040. doi:10.1111/iju.12482
5. Stoddard MD, Zheng X, Mao J, et al. Safety and efficacy of outpatient surgical procedures for the treatment of benign prostatic enlargement in New York State and California (2005–2016). J Urol. 2021;205(3):848–854. doi:10.1097/JU.0000000000001401
6. De Nunzio C, Lombardo R, Nacchia A, et al. Young Academic Urologists’ benign prostatic obstruction nomogram predicts clinical outcome in patients treated with transurethral resection of prostate: an Italian cohort study. Minerva Urol Nefrol. 2018;70(2):211–217. doi:10.23736/S0393-2249.17.03008-9
7. Chen X, Man Q, Wei X, et al. Predictive value of preoperative comprehensive evaluation on the efficacy of HoLEP. Transl Androl Urol. 2020;9(4):1603–1610. doi:10.21037/tau-20-504
8. Kwon JK, Han JH, Choi HC, et al. Clinical significance of peripheral zone thickness in men with lower urinary tract symptoms/benign prostatic hyperplasia. BJU Int. 2016;117(2):316–322. doi:10.1111/bju.13130
9. Tian Y, Liu HM, Yang B, et al. Prostatic anatomical parameters correlate with clinical characteristics suggestive of benign prostatic hyperplasia. Asian J Androl. 2021;23(1):64–68. doi:10.4103/aja.aja_47_20
10. Franco G, De Nunzio C, Leonardo C, et al. Ultrasound assessment of intravesical prostatic protrusion and detrusor wall thickness–new standards for noninvasive bladder outlet obstruction diagnosis? J Urol. 2010;183(6):2270–2274. doi:10.1016/j.juro.2010.02.019
11. Aso Y, Homma Y. Clinical research criteria: response criteria for evaluating efficacy of treatments for benign prostatic hypertrophy. Br J Urol. 1995;76(Suppl 1):69–73.
12. Milonas D, Saferis V, Jievaltas M. Transition zone index and bothersomeness of voiding symptoms as predictors of early unfavorable outcomes after transurethral resection of prostate. Urol Int. 2008;81(4):421–426. doi:10.1159/000167840
13. Antunes AA, Iscaife A, Reis ST, et al. Can we predict which patients will experience resolution of detrusor overactivity after transurethral resection of the prostate? J Urol. 2015;193(6):2028–2032. doi:10.1016/j.juro.2014.12.095
14. Seki N, Yuki K, Takei M, et al. Analysis of the prognostic factors for overactive bladder symptoms following surgical treatment in patients with benign prostatic obstruction. Neurourol Urodyn. 2009;28(3):197–201. doi:10.1002/nau.20619
15. Choi H, Kim JH, Shim JS, et al. Prediction of persistent storage symptoms after transurethral resection of the prostate in patients with benign prostatic enlargement. Urol Int. 2014;93(4):425–430. doi:10.1159/000357626
16. Smith PP, DeAngelis A, Kuchel GA. Detrusor expulsive strength is preserved, but responsiveness to bladder filling and urinary sensitivity is diminished in the aging mouse. Am J Physiol Regul Integr Comp Physiol. 2012;302(5):R577–R586. doi:10.1152/ajpregu.00508.2011
17. Rhodes T, Girman CJ, Jacobsen SJ, et al. Longitudinal prostate growth rates during 5 years in randomly selected community men 40 to 79 years old. J Urol. 1999;161(4):1174–1179. doi:10.1097/00005392-199904000-00033
18. Eckhardt MD, van Venrooij GE, Boon TA. Symptoms and quality of life versus age, prostate volume, and urodynamic parameters in 565 strictly selected men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Urology. 2001;57(4):695–700. doi:10.1016/S0090-4295(00)01101-8
19. Simon RM, Howard LE, Moreira DM, et al. Does prostate size predict the development of incident lower urinary tract symptoms in men with mild to no current symptoms? Results from the REDUCE trial. Eur Urol. 2016;69(5):885–891. doi:10.1016/j.eururo.2015.12.002
20. St SJ, Jacobson DJ, Girman CJ, et al. Correlations between longitudinal changes in transitional zone volume and measures of benign prostatic hyperplasia in a population-based cohort. Eur Urol. 2006;50(1):105–111. doi:10.1016/j.eururo.2006.01.013
21. Matsugasumi T, Fujihara A, Ushijima S, et al. Morphometric analysis of prostate zonal anatomy using magnetic resonance imaging: impact on age-related changes in patients in Japan and the USA. BJU Int. 2017;120(4):497–504. doi:10.1111/bju.13823
22. Tanaka Y, Masumori N, Itoh N, et al. Is the short-term outcome of transurethral resection of the prostate affected by preoperative degree of bladder outlet obstruction, status of detrusor contractility or detrusor overactivity? Int J Urol. 2006;13(11):1398–1404. doi:10.1111/j.1442-2042.2006.01589.x
23. Matsukawa Y, Ishida S, Majima T, et al. Intravesical prostatic protrusion can predict therapeutic response to silodosin in male patients with lower urinary tract symptoms. Int J Urol. 2017;24(6):454–459. doi:10.1111/iju.13333
24. Lin YT, Amouyal G, Thiounn N, et al. Intra-vesical Prostatic Protrusion (IPP) can be reduced by prostatic artery embolization. Cardiovasc Interv Radiol. 2016;39(5):690–695. doi:10.1007/s00270-015-1235-8
25. Kuo HC. Clinical prostate score for diagnosis of bladder outlet obstruction by prostate measurements and uroflowmetry. Urology. 1999;54(1):90–96. doi:10.1016/S0090-4295(99)00092-8
26. De Nunzio C, Lombardo R, Cicione A, et al. The role of bladder wall thickness in the evaluation of detrusor underactivity: development of a clinical nomogram. Neurourol Urodyn. 2020;39(4):1115–1123. doi:10.1002/nau.24327
27. Homma Y, Imajo C, Kawabe K, et al. Response criteria for the therapeutic efficacy of treatment for benign prostatic hyperplasia. Int J Urol. 1995;2(1):33–38. doi:10.1111/j.1442-2042.1995.tb00617.x
28. Choi J, Ikeguchi EF, Lee SW, et al. Is the higher prevalence of benign prostatic hyperplasia related to lower urinary tract symptoms in Korean men due to a high transition zone index? Eur Urol. 2002;42(1):7–11. doi:10.1007/978-3-642-78185-8_11
29. Marks LS, Roehrborn CG, Wolford E, et al. The effect of dutasteride on the peripheral and transition zones of the prostate and the value of the transition zone index in predicting treatment response. J Urol. 2007;177(4):1408–1413. doi:10.1016/j.juro.2006.11.095
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.