")
Back to Journals » Journal of Inflammation Research » Volume 14
The Prognostic Significance of Novel Pancreas Cancer Prognostic Index in Unresectable Locally Advanced Pancreas Cancers Treated with Definitive Concurrent Chemoradiotherapy
Authors Topkan E , Selek U , Pehlivan B , Kucuk A , Haksoyler V , Kilic Durankus N, Sezen D , Bolukbasi Y
Received 15 July 2021
Accepted for publication 18 August 2021
Published 4 September 2021 Volume 2021:14 Pages 4433—4444
DOI https://doi.org/10.2147/JIR.S329611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Erkan Topkan,1 Ugur Selek,2,3 Berrin Pehlivan,4 Ahmet Kucuk,5 Veysel Haksoyler,6 Nulifer Kilic Durankus,2 Duygu Sezen,2 Yasemin Bolukbasi2,3
1Department of Radiation Oncology, Baskent University Medical Faculty, Adana, Turkey; 2Department of Radiation Oncology, Koc University Faculty of Medicine, Istanbul, Turkey; 3Division of Radiation Oncology, The University of Texas MD Anderson Cancer Center, Houston, TX, USA; 4Department of Radiation Oncology, Bahcesehir University, Istanbul, Turkey; 5Radiation Oncology Clinics, Mersin City Hospital, Mersin, Turkey; 6Clinics of Medical Oncology, Medline Hospital, Adana, Turkey
Correspondence: Erkan Topkan
Department of Radiation Oncology, Baskent University Medical Faculty, Adana, 01120, Turkey
Tel +90 533-7381069
Fax +90 322-3444452
Email [email protected]
Purpose: We evaluated the prognostic quality of the novel pancreas cancer prognostic index (PCPI), a combination of CA 19-9 and systemic inflammation response index (SIRI), on the outcomes of locally advanced pancreas adenocarcinoma (LAPAC) patients who received concurrent chemoradiotherapy (C-CRT).
Methods: This retrospective analysis covered 152 unresectable LAPAC patients treated from 2007 to 2019. Receiver operating characteristic (ROC) curve analysis was used to define ideal cutoff thresholds for the pretreatment CA 19-9 and SIRI measurements, individually. The associations between the PCPI groups and progression-free- (PFS) and overall survival (OS) comprised the respective primary and secondary endpoints.
Results: The ROC curve analysis distinguished the respective rounded optimal cutoffs at 91 U/m/L (< versus ≥ 90) and 1.8 (< versus ≥ 1.8) for CA 19-9 and SIRI, arranging the study cohort into two significantly different survival groups for each, with resultant four likely groups: Group-1: CA 19-9< 90 U/m/L and SIRI< 1.8, Group-2: CA 19-9< 90 U/m/L but SIRI≥ 1.8, Group-3: CA 19-9≥ 90 U/m/L but SIRI< 1.8, and Group-4: CA 19-9≥ 90 U/m/L and SIRI≥ 1.8. Since the PFS (P=0.79) and OS (P=0.86) estimates of the groups 2 and 3 were statistically indistinct, we merged them as one group and created the novel three-tiered PCPI: PCPI-1: CA 19-9< 90 U/m/L and SIRI< 1.8, PCPI-2: CA 19-9< 90 U/m/L but SIRI≥ 1.8 or CA 19-9≥ 90 U/m/L but SIRI< 1.8, and PCPI-3: CA 19-9≥ 90 U/m/L and SIRI≥ 1.8, respectively. Comparative analyses unveiled that the PCPI-1 and PCPI-3 groups had the respective best and worst PFS (17.0 versus 7.5 versus 4.4 months; P< 0.001) and OS (26.1 versus 15.1 versus 7.4 months; P< 0.001) outcomes, while the PCPI-2 group posed in between. The multivariate analysis outcomes confirmed the novel three tired PCPI’s independent prognostic significance on either of the PFS [HR: 5.38 (95% confidence interval (CI): 4.96-5.80); P< 0.001)] and OS [HR: 5.67 (95% CI: 5.19-6.15); P< 0.001] endpoints, separately.
Conclusion: The new PCPI introduced here can be used as an independent and reliable prognostic indicator to divide LAPAC patients into three subgroups with discrete survival results.
Keywords: locally advanced pancreas cancer, concurrent chemoradiotherapy, prognosis, survival outcomes, pancreas cancer prognostic index
Introduction
Systemic chemotherapy, sequential chemoradiotherapy (CRT), and definitive concurrent CRT (C-CRT) constitute the current treatment standards for medically fit unresectable locally advanced pancreas adenocarcinomas (LAPACs), which account for one-third of all PACs.1–3 Regrettably, the prognosis of such patients perseveres bleak, with an expected median overall survival (OS) range of only 9 to 13 months, as an essential result of limited responsiveness of the LAPACs to the current anti-cancer treatment options and ensuing extensive distant metastases (DM).4–8 Accenting the pressing need to identify new biologic markers that may serve valuably in better prognostic stratification LAPACs, these patients exhibit significantly different response rates and survival times after standard therapies negligent of whether they present with practically indistinguishable performance status, local and regional stages, and prognostic variables.7–10 Such significant clinical outcome differences among LAPAC patients might be attributed to the present TNM (tumor-node-metastasis) staging framework’s apparent disregard of biological indicators. Hence, the acquisition of novel biological markers to supplement the TNM staging framework may reasonably be valuable in the more reliable prognostic classification of such individuals.
The carbohydrate antigen 19-9 (CA 19-9), also known as Sialyl Lewis-a, and immunoinflammatory markers like systemic inflammation response index (SIRI) are among such neglected biomarkers remiss of their proven prognostic roles in PACs. The CA 19-9 is over expressed in a broad spectrum of gastrointestinal and extra-gastrointestinal benign and malignant diseases.11–17 However, given that its primary implications were discovered for PACs, the CA 19-9 prevails as an essential biomarker in routine clinical use for the diagnosis, staging, management, and prognostication of PAC patients undergoing various anti-cancer treatments.16–18 Concerning the prognostic value of CA 19-9, several investigations have found a significant association between the diminished survival results and higher CA 19-9 levels, even though variable cutoffs were adopted in these studies.19–23 In this respect, the researchers of the benchmark Charité Onkologie 001 (CONKO-001) randomized trial used the CA 19-9 ≤ 90 U/mL threshold level for eligibility in their study, which compared adjuvant chemotherapy with gemcitabine against observation in 368 patients undergoing curative-intent resection of PACs.16 Later the validity of this cutoff was established by the results of the Radiation Therapy Oncology Group (RTOG) randomized Phase III trial 9704 comparing the use of either continuous infusion 5-fluorouracil (5-FU) or gemcitabine before and after concurrent CRT with 5-FU in patients with resected PACs.17
Systemic inflammation, the seventh cancer hallmark, has essential roles in all stages of carcinogenesis, including initiation, growth, invasion, resistance to apoptotic signals, evasion from the immune system, and metastatic dissemination steps.24,25 Furthermore, available research demonstrated a clear link between increased systemic inflammatory responses and a reduced patient prognosis following alternate therapy regimens.26,27 The simplest and cheapest approach to evaluate the degree of systemic inflammation is to measure the associated blood-borne markers in the peripheral bloodstream: neutrophils, monocytes, platelets, lymphocytes, albumin, and C-reactive protein, all of which have been widely investigated in PAC patients. The findings of such studies revealed consistent and substantial correlations between these indicators and patient outcomes, regardless of whether the analyses used a single component or composite index.7,9,28–34 Qi et al shown that the SIRI is one composite measure that successfully stratifies PAC patients into two separate prognosis groups following chemotherapy in terms of time to progression and survival results.35 Similarly, SIRI was observed to be linked with clinical outcomes of metastatic PAC patients who underwent FOLFIRINOX (fluorouracil, leucovorin, irinotecan, and oxaliplatin) chemotherapy in a subsequent study.36 Furthermore, Topkan et al recently reported that the SIRI < 1.6 was connected with considerably better survival results in LAPAC patients managed with definitive C-CRT.10
Surprisingly, despite the abundance of such compelling evidence, to our soundest information, the prognostic value of the blend of SIRI and CA 19-9 has never been investigated for its prognostic relevance in unresectable LAPAC patients undergoing definitive C-CRT. Consequently, we herein endeavored to retrospectively examine the prognostic implications of the combination of pretreatment SIRI and CA 19-9 as a novel prognostic index in these patients, namely the Pancreas Cancer Prognostic Index (PCPI).
Patients and Methods
Study Population
A retrospective review of patients who underwent definitive C-CRT for unresectable LAPAC from January 2007 to December 2019 was conducted at the Department of Radiation Oncology, Baskent University Faculty of Medicine. The AJCC 8th edition staging system was utilized to define unresectable LAPC patients at the time of referral. In brief, unresectable primary tumors included the celiac axis and/or superior mesenteric artery plus/minus regional lymphatic involvement: stage III (T4N0-2M0) disease. Our conventional diagnostic and staging workup for unresectable LAPACs were as previously detailed elsewhere (7, 37), which comprised abdominal magnetic resonance imaging (MRI), magnetic resonance cholangiopancreatography (MRCP), and endoscopic ultrasonography (in case of open abdominal exploration) for abdominal disease staging; diagnostic thoracic computed tomography (CT), and brain MRI in all patients. The 8F-fluorodeoxyglucose (FDG)-positron emission tomography (PET)-CT scanning was also standardly performed in each patient to distinguish the likely DMs. Further qualification criteria include: age 18 to 80 years, Eastern Cooperative Oncology Group (ECOG) performance status 0–1, proven adenocarcinoma histology, no chemotherapy/RT history, body mass index (BMI) > 20 kg/m2; and available pre-C-CRT routine complete blood count, biochemistry, and CA 19-9 tests. Colorectal, lung, liver, and ovarian cancers, as well as benign illnesses, such as hepatobiliary system diseases, bronchiectasis, pneumonia, pleural effusion, renal failure, pancreatitis, cholangitis, and systemic lupus erythematosus, may lead to high CA 19-9 levels. As a result, to avoid potential biases in the results, such patients were judged ineligible for the study.
Ethics, Consent and Permissions
The present retrospective study design was approved by the Institutional Review Board of Baskent University before the acquisition of any patient information. All procedures were carried out per the ethical standards of our institutional research committee, as well as the Helsinki Declaration of 1964 and succeeding revisions. As per our institutional norms, all patients, either themselves or legitimately approved representatives, provided written informed consent before the commencement of treatment to collect and analyze blood samples, pathological specimens and publish their results.
Treatment
Each patient received radical C-CRT with a dose of 45 Gy RT (1.8 Gy/fraction, 5-days/week, for 5-weeks) and continuously infused 5-fluorouracil (225 mg/m2/day) over the course of RT, followed by 2 to 6 cycle of maintenance gemcitabine (1000 mg/m2 intravenously on days 1 and 8 every 21 days) as previously described.9 Only the main tumor site and nodes were included in the RT field, and elective nodal irradiation was strictly prohibited.
Measures of CA19-9 and SIRI
The pretreatment CA19-9 and SIRI measures were determined by using the tumor markers and complete blood count tests obtained within the past 1-week and the first day of the C-CRT, respectively. For each patient, the CA19-9 values mirrored right the measured quantities, while the SIRI was calculated by using the Qi’s original formula; SIRI= Monocytes (M) × Neutrophil (N)/Lymphocyte (L), respectively.36
Response Evaluation
Each patient was discussed by institutional tumor board members at six weeks following the C-CRT course and at the end of the adjuvant chemotherapy course for eligibility for conversion surgery, which included radiation oncologists, medical oncologists, radiologists, and surgeons. The main criteria for conversion surgery comprised the patient’s performance status, tumor extent surrounding the major vessels as defined by the AJCC staging framework, and the absence of evident metastases. After the first evaluation for conversion surgery, the treatment response was assessed every 3- and 6-monthly intervals for the first two years and beyond, respectively. Restaging PET/CT and abdominal MRI/CT (after confirmation of a complete metabolic response on PET-CT) scans were used for this objective, with the reported response indicating the best result per EORTC 1999 guidelines. Additionally, plain chest X-ray, total blood count and biochemistry tests, serum CA 19-9 concentrations were obtained at each visit. Any of the abdominal ultrasonography, chest CT, cranial MRI, and/or bone scintigraphy assessments were not regularly needed and were restricted to cases with clinically suspected DMs.
Statistical Methods
The primary endpoint of the present research was the impact of PCPI on the overall survival (OS) results: the interval between the first day of the C-CRT and the date of death or last follow-up. The progression-free survival (PFS: the interim between the first day of the C-CRT and the dates of any disease progression/death/last follow-up) constituted the secondary endpoint. Categorical and continuous variables were described with the frequency distributions and medians plus ranges, respectively. Accessibility of pre-C-CRT CA 19-9 and SIRI cutoffs that may group the study population into two separate bunches with distinctive OS and PFS results was searched for by performing receiver operating characteristic (ROC) curve analyses. Student’s t-tests, Chi-square tests, or Spearman correlation analyses were endeavored to test correlations between patients’ groups, as indicated. The study population was stratified into two or more groups for intergroup comparisons, as needed. Kaplan-Meier curves were drawn for PFS and OS and compared with Log rank tests. The Multivariate Cox proportional hazard model was utilized to survey probable interactions between these variables and survival outcomes. All two-tailed P-values < 0.05 were considered significant for the comparisons between any two groups. However, the treatment weights were adjusted for multiplicity by employing Bonferroni corrections and ensuing P-values for comparisons between three or more subgroups to limit the random false-positive results for simultaneously performed multiple subgroup analyses, such as the PCPI groups.
Results
A sum of 152 qualified LAPAC patients who underwent definitive C-CRT at our institution was included in this analysis (Table 1). The median age was 59 years (range: 27–79), with 22.4% of them being elderly patients per the commonly cited age cutoff of 70 years. Male gender (78.3%) and pancreas head tumors (80.9%) were predominant. Overall, 46.8% and 56.6% of patients had metastatic lymph node(s) and significant weight loss (WL: ≥5% at past 6 months before the C-CRT). The median pre-C-CRT CA 19-9 measure was 91.8 U/mL (range: 19.4–785.2) which decreased to 64.6 U/mL (range: 15.6–817.3) at the end of adjuvant chemotherapy. The CA 19-9 measure was found to decrease to our laboratory normal levels of 37.0 U/mL in only 14 (9.9%) of 141 patients presenting with high (≥37.0 U/mL) CA 19-9 measures after the adjuvant chemotherapy. Only 14 (9.9%) of 141 patients presenting with high (37.0 U/mL) CA 19-9 levels had their CA 19-9 levels drop to our laboratory normal values of 37.0 U/mL following the adjuvant chemotherapy. One-hundred and twelve (73.7%) of the 152 patients received all 4 to 6 cycles of prescribed adjuvant chemotherapy, with a median of 4 cycles (range: 1–6).
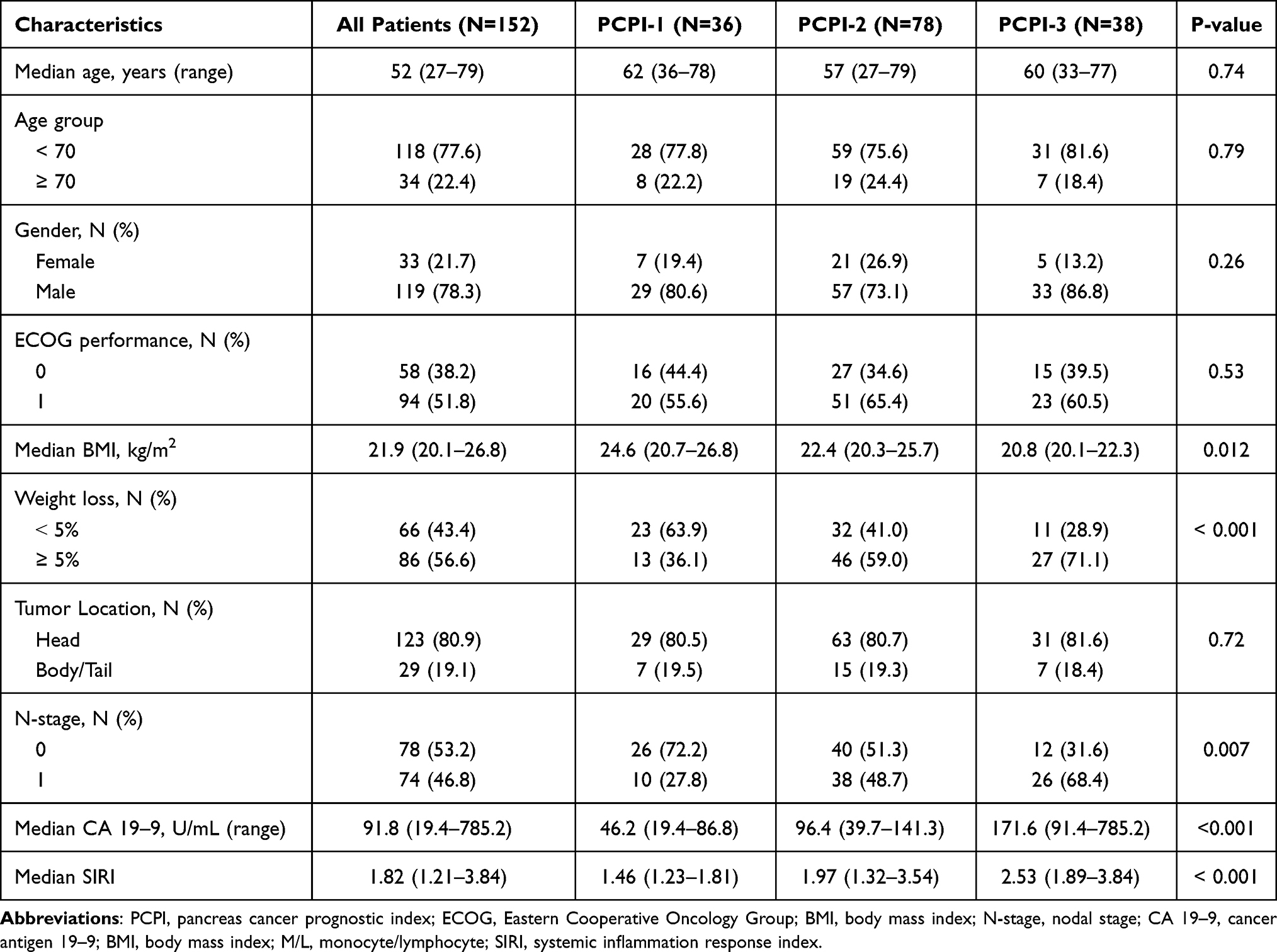 |
Table 1 Pretreatment Patient and Disease Characteristics |
During the time of the current analysis, 47 (30.9%) patients were alive, of whom 24 (15.8%) were free of disease progression at a median follow-up of 18.5 months (range: 3.2–91.3 months). The median and 5-year PFS and OS rates were 7.5 months [95% confidence interval (CI: 6.1–8.9)] and 9.3%, and 14.8 months (CI: 11.9 −17.7) and 16.1%, individually, for the entire cohort. The respective 5-year actuarial locoregional control (LRC) and freedom from DM (FFDM) rates were 19.7% and 15.8%. Conversion surgery was deemed feasible for only 16 (10.5%) cases at 6-weeks evaluations after the CCRT, with R0 resection being possible only in 7 (4.6%) of them. Unfortunately, no additional patients become viable for conversion surgery at the end of the planned chemotherapy cycles.
We sought conceivable ROC curve analysis cutoff points for continuous variables including the age, BMI, CA 19-9, and SIRI that may interact with the clinical outcomes. As illustrated in Figure 1, the ROC curve analyses uncovered significance at a rounded cutoff of 91.0 U/m/L [Area under the curve (AUC): 71.8%; sensitivity: 70.8%; specificity: 69.1%] and 1.8 (AUC: 72.6%; sensitivity: 71.9%; specificity: 70.7%) for the association between the CA 19-9 and SIRI levels and the PFS and OS results, distinctly, but none for the age (AUC: 70.7%) or BMI (AUC: 52.1%). Given that the current CA 19-9 cutoff of 91.0 U/m/L identified herein was strikingly comparable to the CONKO-01 and RTOG 97-04 trials’ 90 U/m/L (16, 17), we utilized the 90 U/m/L as the preferred cutoff for further analyses. Grouping the whole investigation cohort per these cutoffs exposed that the patients with CA 19-9 < 90 U/m/L (10.5 vs 6.5 months; HR: 1.59; P= 0.008 for PFS and 20.6 vs 12.2 months; HR: 1.76; P= 0.002 for OS) and SIRI < 1.8 (11.0 vs 5.7 months; HR1.88; P < 0.001 for PFS and 20.7 vs 10.9 months; HR: 1.98 for OS) had significantly longer PFS and OS durations than their CA 19-9 ≥ 90 U/m/L and SIRI ≥ 1.8 counterparts, respectively.
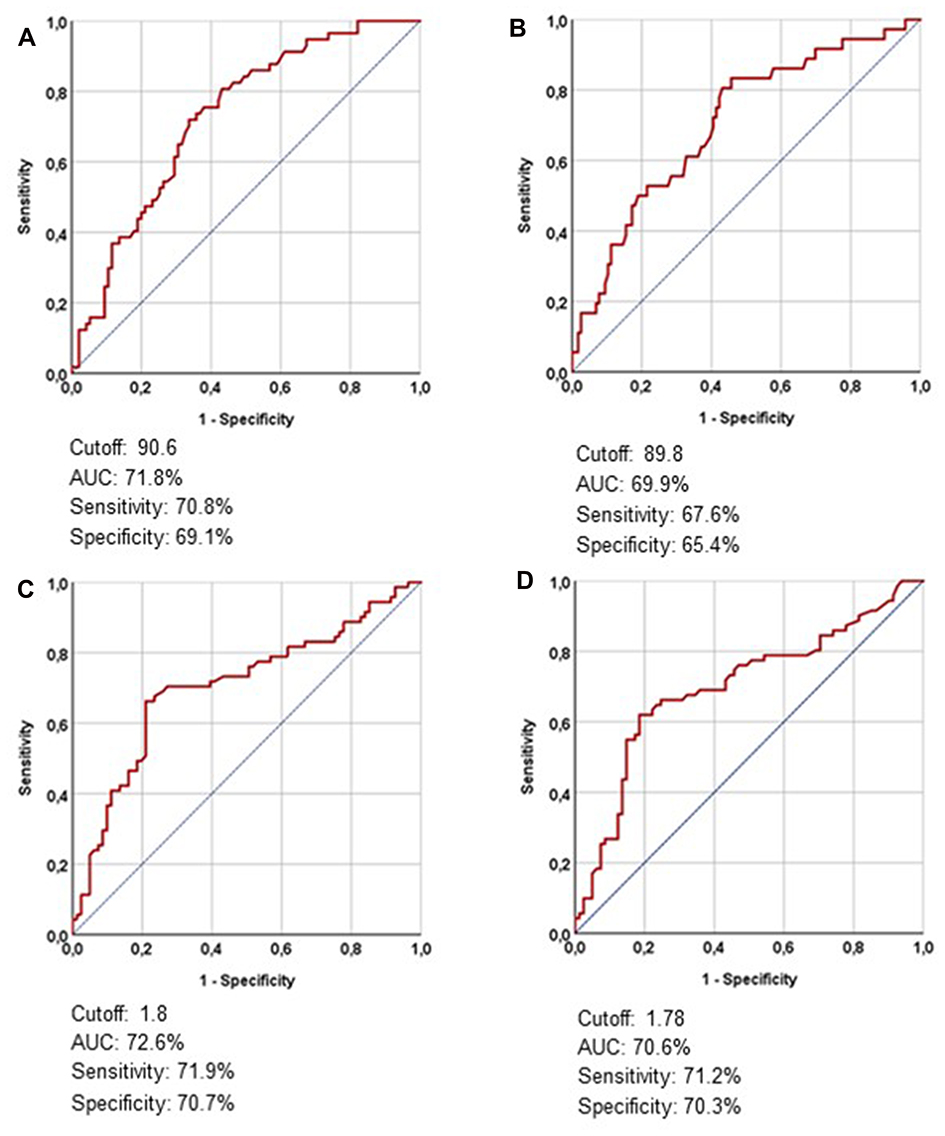 |
Figure 1 Receiver operating characteristic curve analyses outcomes per pretreatment CA 19-9 and systemic inflammation response index measures: (A) CA 19-9 and progression-free survival, (B) CA 19-9 and overall survival, (C) Systemic inflammation response index and progression-free survival, and (D) Systemic inflammation response index and overall survival. |
To address the significance of different combinations of the CA 19-9 and SIRI per respective cutoffs, we created four probable groups as shown in Table 2. Bonferroni corrected P-values (P< 0.0083 for significance) revealed that either of the earlier groups had significantly superior PFS and OS outcomes than the latter groups except for the Group 2 versus 3 (Table 3). Because the survival results were interchangeable between Groups 2 and 3, we have combined these two groups into one and built the novel PCPI with three respective groups: PCPI-1: CA 19-9 < 90 U/m/L and SIRI < 1.8; PCPI-2: CA 19-9 < 90 U/m/L but SIRI ≥ 1.8, or SIRI < 1.8 but CA 19-9 ≥ 90 U/m/L; and PCPI-3: CA 19-9 ≥ 90 U/m/L and SIRI ≥ 1.8, respectively (Table 2). As shown in Table 1, baseline patient and disease characteristics were in general well balanced between the three PCPI groups except for gradually increasing rates of significant WL (≥5% at past 6-months) (P<0.001) and N1-2 (P= 0.007) nodal status from PCPI-1 to PCPI-3 groups, respectively. The Bonferroni corrected P-values (P<0.0167) for significance exhibited that the PCPI-1 and PCPI-3 groups embodied the best and worst PFS (17.0 versus 7.5 versus 4.4 months; P<0.001 for each comparison) and OS (26.1% versus 15.1% versus 7.4%; P<0.001 for each comparison) outcome groups, while the PCPI-2 group posed between them (Table 4 and Figure 2). The matching 5-year PFS (25.4% versus 13.3% versus 0%) and OS (38.2% versus 22.1% versus 0%) rates were likewise superior in the earlier groups.
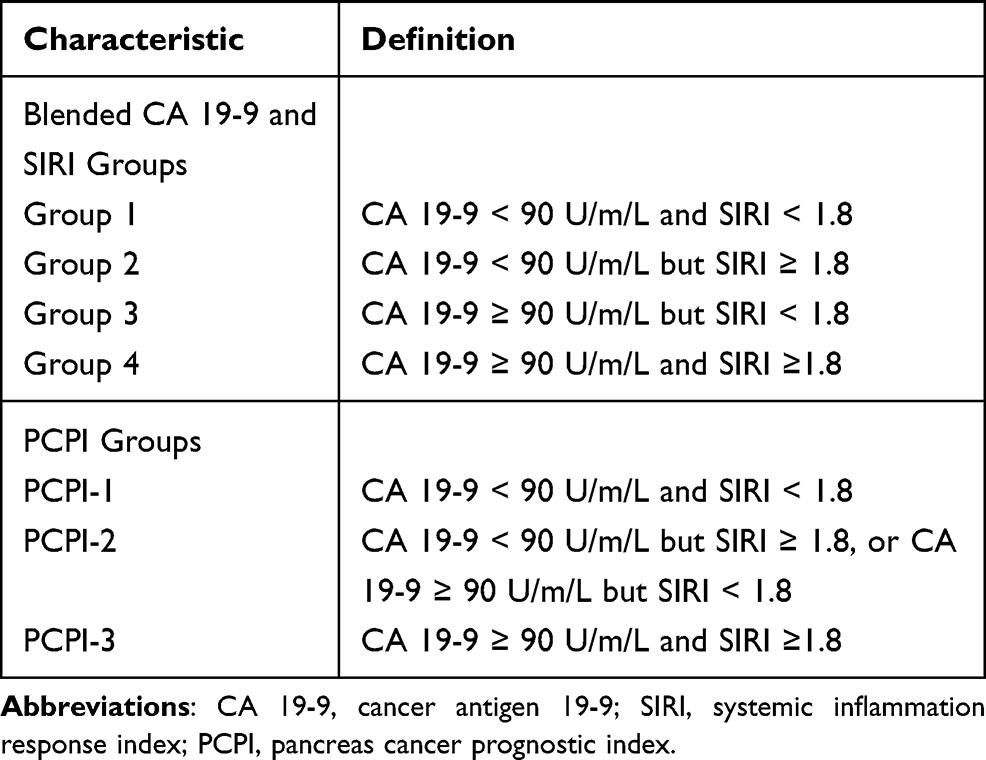 |
Table 2 Definition of Blended CA 19–9 and Systemic Inflammation Response Index Groups, and Pancreas Cancer Prognostic Index |
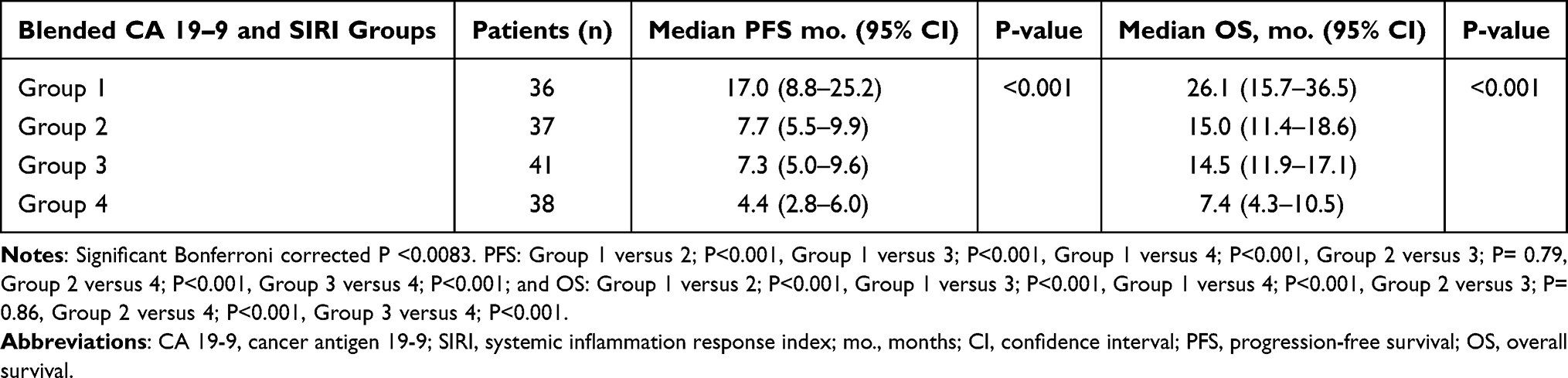 |
Table 3 Survival Outcomes per Blended CA 19-9 and Systemic Inflammation Response Index Groups |
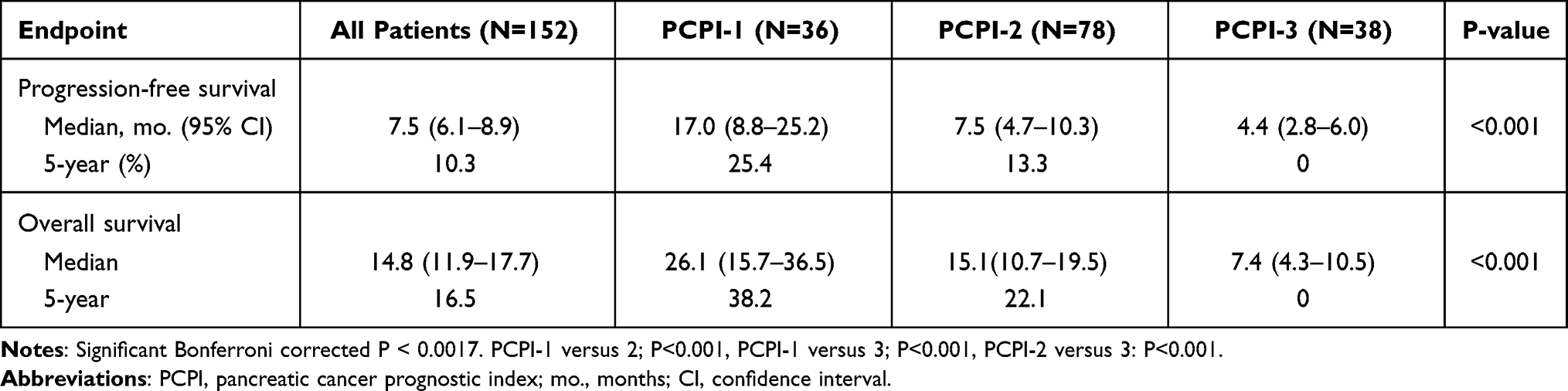 |
Table 4 Survival Outcomes per Pancreatic Cancer Prognostic Index Groups |
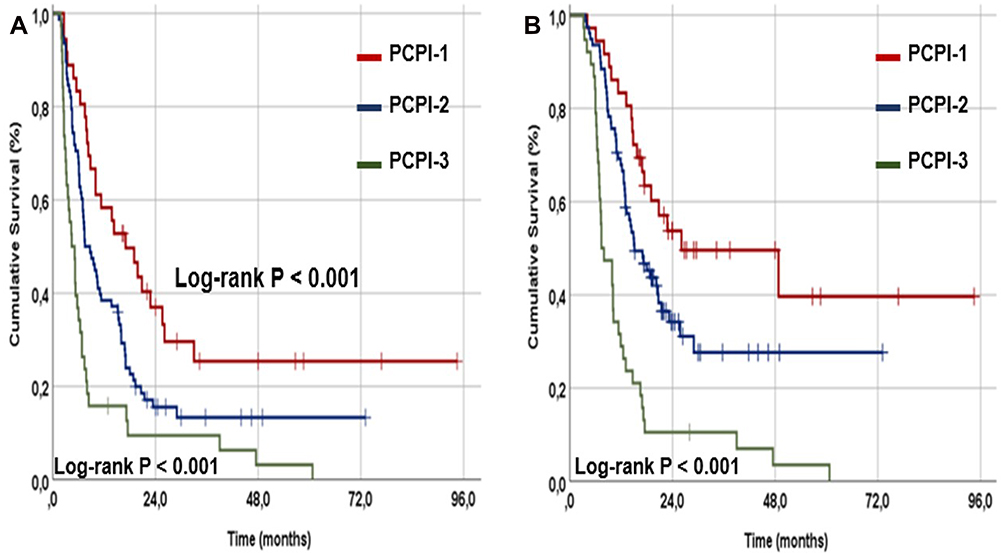 |
Figure 2 Survival outcomes per pancreas cancer prognostic index (PCPI) groups: (A) Progression-free survival, and (B) Overall survival (Red line: PCPI-1; Dark blue line: PCPI-2; and Dark green line: PCPI-3). |
The results of univariate analysis uncovered the N0 stage (versus N1-2), <5% WL at past 6-months before the C-CRT (versus WL≥5%), CA 19-9 ≤ 90 U/mL (versus > 90 U/mL), SIRI<1.8 (versus ≥ 1.8) and lower PCPI groups (PCPI-1 versus PCPI-2 versus PCPI-3) as the variables to connect with significantly longer PFS and OS results, as well as numerically superior 5-year PFS and OS rates (Tables 5 and 6). Because the CA 19-9 and SIRI comprised the components of the PCPI, we confined the multivariate analysis to the N-stage, WL status, and PCPI groups, which revealed that all three factors had independent prognostic significance on both of the PFS (Bonferroni corrected P<0.0083, for each variable) and OS (Bonferroni corrected P<0.0083 for each variable) results, respectively (Table 5).
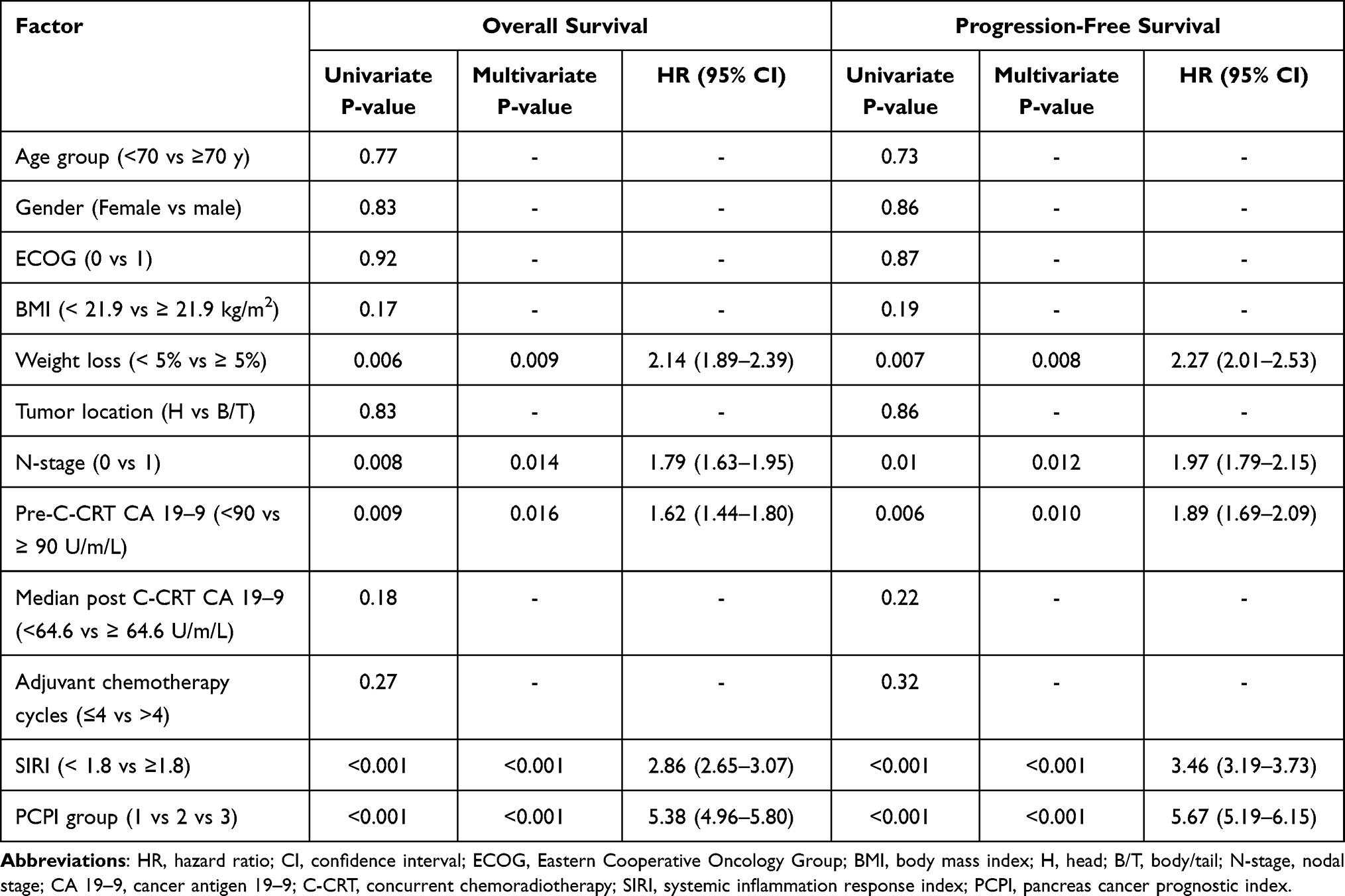 |
Table 5 Results of Uni- and Multivariate Analyses |
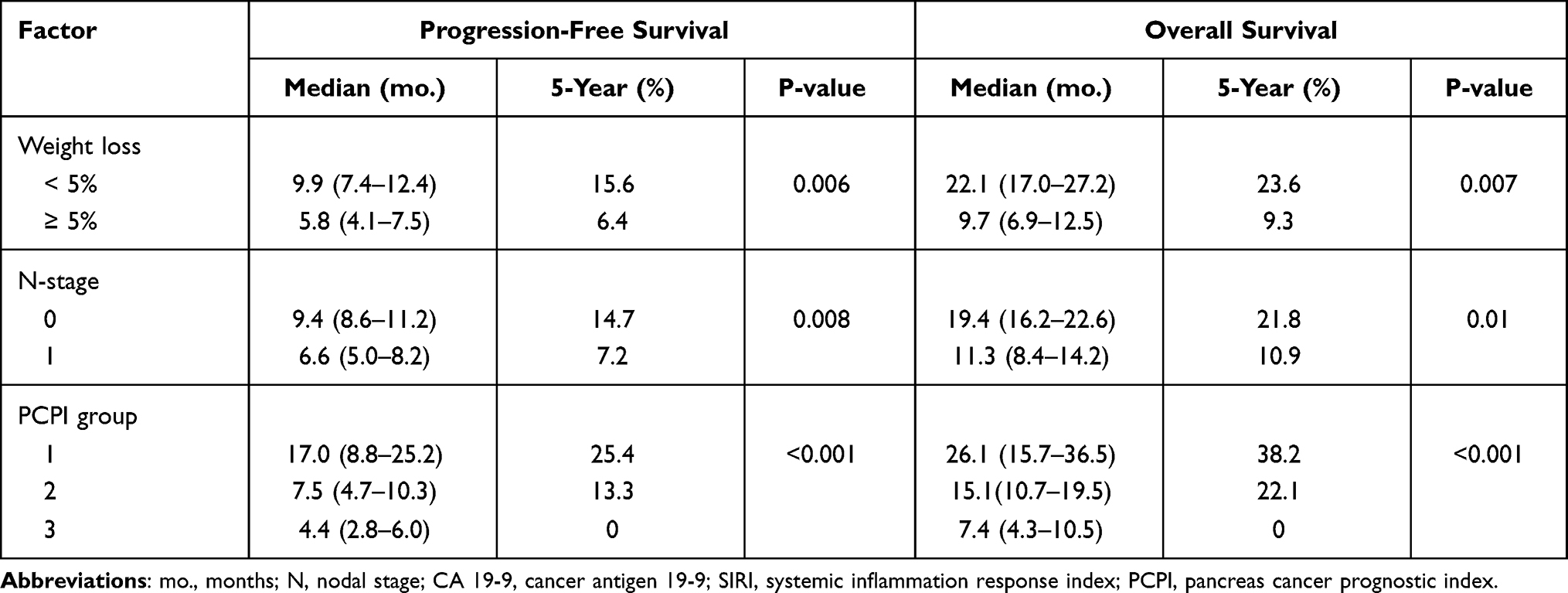 |
Table 6 Survival Outcomes per Factors Showing Independent Prognostic Significance in Multivariate Analyses |
Discussion
The present study sought the prognostic worth of the blended pretreatment SIRI and CA 19-9 levels, namely the PCPI, as a novel prognostic index in unresectable LAPC patients treated with definitive C-CRT. Other than confirming the independent prognostic merits of the N-stage, WL status, SIRI, and CA 19-9, we uncovered that the PCPI was an independent prognostic biomarker, which was superior to both SIRI and CA 19-9, respectively. Of utmost significance, PCPI was able to stratify the LAPAC patients into three groups with significantly distinctive survival outcomes, with the PCPI-1, PCPI-2, and PCPI-3 groups manifesting PFS and OS results those appear to be nearly identical with the published results for resectable earlier stage PAC-, average unresectable LAPAC-, and metastatic (stage IV) PAC patients, respectively.
The underlying inflammation, which is implicitly withheld by almost all cancers, has become the seventh hallmark of cancer, given its requisite functions in practically all means of initiation of carcinogenesis, malignant progression, and distant spread.24,25 Both local and systemic inflammatory responses provoke tumor angiogenesis, suppress antitumor immunity, expedite escape from immune response, hasten the metastatic process, induce resistance to anticancer therapies, increase treatment-related toxicities, and reduce patients’ treatment tolerance.24,25 Accessible proof illuminated that the circulating cellular biomarkers or their blends, including the neutrophils, monocytes, macrophages, lymphocytes, and platelets were involved in the inflammatory response of LAPACs.7,9,10,26–36 The prognostic competence of various blended systemic inflammation markers has been asserted by past inquiries in LAPAC patients, to be specific the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), prognostic nutritional index (PNI), Glasgow prognostic index (GPS), advanced lung cancer inflammation index (ALI), systemic immune-inflammation index (SII), and systemic immune response index (SIRI).3,7,9,10,31–33,35 Similarly, CA 19-9 has been extensively studied for its prognostic significance in PAC patients undergoing various oncological treatments, with proven efficacy for accurate prediction of pretreatment tumor stage and resectability status, response to therapy, PFS, and OS outcomes, despite various cutoffs being used in these researches.16–23 Surprisingly, establishing rational grounds for the present investigation, the blend of these two potent biomarkers had never been tested before for its prognostic significance in unresectable LAPAC patients who underwent exclusive C-CRT albeit SIRI was first formulated for PAC patients and the CA 19-9 demonstrates its chief utility in PACs.
Despite recognizing the difficulties in the comparison of studies with different methodologies, the individual median and 5-year PFS and OS results of the current retrospective cohort analysis in 152 LAPAC patients treated with definitive C-CRT accord well with previous C-CRT reports in these patients.18,19,37,38 Besides, results from multivariate analyses appeared to strengthen previously established independent unfavorable prognostic influence of the N1-2 stage, presenting WL>5%, CA19-9 > 90 U/mL, and SIRI>1.6. However, the chief contribution of our critical research to the LAPAC literature was the display of the PCPI (a blend of CA 19-9 and SIRI) as an innovative and independent prognostic factor that uniquely merges a tumor marker and an immune-inflammation biomarker that efficiently stratifies the LAPAC patients into three unique PFS and OS groups beyond that of accessible prognosticators following radical C-CRT. It is laborious to allot these remarkable discoveries to exact causes in the apparent lack of similarly outlined past LAPAC studies, but we can still infer some impartial explanations by interpreting the well-proven prognostic utilities of CA- 19-9 and SIRI, namely the active components of the novel PCPI. The advancing literature has established the prognostic value of CA 19-9 in LAPAC patients managed with chemotherapy or C-CRT plus/minus surgery.16–23 Although different CA 19-9 cutoffs were utilized, results of past investigations confirmed the significant association between higher CA 19-9 levels and reduced survival results in PAC patients.19–23 Like our study, the researchers of the aforementioned landmark Charité Onkologie 001 (CONKO-001) and RTOG 97-04 randomized trials chose the CA 19-9 ≤ 90 U/mL as the cutoff level for prognostic stratification of such patients.16,17 Authenticating the CA 19-9 as a prognostic factor, Choi et al reported that the pretreatment higher CA 19-9 levels were associated with significantly reduced survival outcomes in their three-tiered nomogram consolidating the SUVmax, radiotherapy dose, and CA 19-9 in a gathering of 426 LAPAC patients undergoing C-CRT.39 Additionally, Ferrone et al proposing a critical connection between the pancreas tumor burden and pretreatment CA 19-9 levels, reported that 80–90% of the stages III–IV PAC patients had CA 19-9 levels > 100 U/mL, with higher T and N-stages related to meaningfully higher CA 19-9 measures.40 Bolstering this verdict, Herreros-Villanueva et al demonstrated that a pretreatment CA19-9> 500 U/mL was linked to significantly depreciated resectability rates (18% versus 60%; P<0.05).41 Regarding the SIRI, our results manifested that SIRI could capably stratify LAPAC patients into two significantly different median PFS and OS groups at a cutoff of 1.8, which appears to be accordant with the historic chemotherapy series and a recently published C-CRT study.10,35,36 In the first definitive C-CRT study examining the prognostic worth of pretreatment SIRI in LAPAC patients, Topkan et al showed that SIRI<1.6 patients had significantly superior PFS and OS outcomes than the SIRI≥1.6 patients.10 The authors further committed these unique findings to the particular immune and inflammatory functions of the monocytes, neutrophils, and lymphocytes components of the SIRI formula, as they account for nearly half of the cellular burden of the LAPAC mass.42 Hence, past proofs and the results introduced here altogether reasonably indicate that the novel PCPI may serve valuably in three-laddered prognostic stratification of unresectable LAPAC patients treated with conclusive C-CRT by combining the tumor burden marker CA 19-9 and the immune-inflammation biomarker SIRI.
Another striking revelation of our study was the exhibit of three exceptionally distinct LAPC groups in either term of PFS and OS outcomes with the novel PCPI introduced here, where PCPI-1, PCPI-2, and PCPI-3 groups appear to represent resectable early-stage patients treated with surgery plus adjuvant chemotherapy, average LAPC patients undergoing chemotherapy or C-CRT, and hopeless stage IV patients commonly treated with palliative systemic chemotherapy with no expected long-term survivors. This finding is of particular significance as it affirms the importance of tumor and systemic immune response biomarkers as the predictors of treatment outcomes, as well as the robust discriminative prognostic capability of our novel PCPI in LAPAC patients who were allocated to the same TNM stage and underwent the same C-CRT protocol. Because the widespread DM was the reason for death in 36 (94.7%) of 38 PCPI-3 patients with a PFS duration of just 4.4 months, our discovery unequivocally commands that most PCPI-3 patients had already harbored occult metastatic foci before the commencement of C-CRT, those were undetectable with the current resolution capability of accessible staging tools, including the MRI and PET-CT. This command is harmonious with the research outcomes proposing increased rates of occult DM as a direct result of inflammation-induced chemotherapy and radiotherapy resistance of the index cancer via numerous mechanisms, including the uninhibited autophagy in aggravated inflammatory conditions.43,44 Albeit the explicit mechanism(s) might be more perplexing, this finding still highlights the imperative requirement for the advancement of more persuasive staging tools and the addition of more potent systemic therapies to the staging and individualized management algorithms of this particular patient group, either to enhance their therapies or to save them from futile aggressive treatments. Considering the early DMs in this group, it may be prudent to start with induction chemotherapy and reserve the aggressive C-CRT for those individuals who do not experience DMs at the end of systemic treatment. Conversely, the 26.1 and 17.0 months of median OS and PFS durations together with the corresponding 5-year rates of 38.2% and 25.4% for PCPI-1 patients, which agree well with the reported respective ranges for resectable early-stage PAC patients,45 clearly imply the presence of a chance for enhanced survival lengths or even cure for those LAPACs presenting with lower tumor and systemic inflammation loads. If our current results are ascertained with further large-scale studies, in the absence of ablative systemic chemotherapies, it may be wise to consider stereotactic ablative body radiotherapy boost after the C-CRT for suitably sized and located PCPI-1 LAPCs to increase the local control rates, which behave as the source of overt DMs and cancer-related deaths.
The present research possesses certain limitations. First, our results should be rendered as hypothesis-generating, not credible recommendations, apprehending the unpredictable biases of retrospective small cohort analysis of any single institution. Hence, the results of well-designed prospective investigations in larger cohorts are called to authenticate the results presented here. Second, the current results may not be echoing the whole real-world practices in LAPAC patients managed with definitive C-CRT due to the omnipresence of a selection bias risk, as we have deliberately included only the patients with an excellent performance status (ECOG 0-1). Third, although the baseline demographic and treatment characteristics were indistinguishable, the impending practice varieties in adjuvant and rescue treatment phases may yet have favored one PCPI gathering over the others. And fourth, we focused solely on the single time-point pre-C-CRT CA 19-9 and SIRI values, albeit both embody dynamic cancer and immune-inflammation biomarkers that may fluctuate broadly throughout the C-CRT process and follow-up. Hence, further research results on this particular topic may labor usefully in discerning conceivably more trustworthy cutoff(s) for each variable. Conversely, this study is powered by specifically including LAPAC patients with a strict staging process; including contrast-enhanced abdominal CT, MRI, MRCP, PET-CT, laparotomy/laparoscopy, and histopathologic dismissal of suspected metastases in any metabolically active lesion, and use of a particular C-CRT standard for all eligible patients. Conjointly, these traits warrant the relative homogeneity of our research population, which uplifts the congruity of the results presented here.
Conclusions
The current results indicate that the novel PCPI, a unique blend of CA 19-9 and SIRI, can be used as a reliable prognostic indicator for unresectable LAPCs by dividing patients into three subgroups with peculiar PFS and OS results, which may guide individualized treatment decisions for such patients.
Data Sharing Statement
The data cannot be shared publicly because the data is owned and saved by Baskent University Medical Faculty. Data are available from the Baskent University Radiation Oncology Institutional Data Access/Ethics Committee (contact via Baskent University Ethics Committee) for researchers who meet the criteria for access to confidential data: contact address, [email protected].
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have declared no conflicts of interest for this work.
References
1. Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362:1605–1617. doi:10.1056/NEJMra0901557
2. Huguet F, Girard N, Guerche CS, Hennequin C, Mornex F, Azria D. Chemoradiotherapy in the management of locally advanced pancreatic carcinoma: a qualitative systematic review. J Clin Oncol. 2009;27:2269–2277. doi:10.1200/JCO.2008.19.7921
3. Russo S, Butler J, Ove R, Blackstock AW. Locally advanced pancreatic cancer: a review. Semin Oncol. 2007;34:327–334. doi:10.1053/j.seminoncol.2007.05.007
4. Von Hoff DD, Goldstein D, Renschler MF. Albumin-bound paclitaxel plus gemcitabine in pancreatic cancer. N Engl J Med. 2014;370:479–480.
5. Heinemann V, Haas M, Boeck S. Neoadjuvant treatment of border line resectable and non-resectable pancreatic cancer. Ann Oncol. 2013;24:2484–2492. doi:10.1093/annonc/mdt239
6. Gastrointestinal Tumor Study Group. Radiation therapy combined with adriamycin or 5-fluorouracil for the treatment of locally unresectable pancreatic carcinoma. Cancer. 1985;56(11):2563–2568. doi:10.1002/1097-0142(19851201)56:11<2563::AID-CNCR2820561104>3.0.CO;2-0
7. Haksoyler V, Topkan E, Caronna R. Prognostic utility of Prechemoradiotherapy albumin-to-alkaline phosphatase ratio in unresectable locally advanced pancreatic carcinoma patients. Gastroenterol Res Pract. 2021;2021:6647145. doi:10.1155/2021/6647145
8. Yildirim BA, Özdemir Y, Colakoglu T, Topkan E. Impact of presence and degree of pretreatment weight loss in locally-advanced pancreatic cancer patients treated with definitive concurrent chemoradiotherapy. Pancreatology. 2016;16(4):599–604. doi:10.1016/j.pan.2016.03.006
9. Topkan E, Mertsoylu H, Ozdemir Y, et al. Prognostic usefulness of advanced lung cancer inflammation index in locally-advanced pancreatic carcinoma patients treated with radical chemoradiotherapy. Cancer Manag Res. 2019;11:8807–8815. doi:10.2147/CMAR.S222297
10. Topkan E, Mertsoylu H, Kucuk A. Low systemic inflammation response index predicts good prognosis in locally advanced pancreatic carcinoma patients treated with concurrent chemoradiotherapy. Gastroenterol Res Pract. 2020;2020:5701949. doi:10.1155/2020/5701949
11. Goh BK, Tan YM, Thng CH, et al. How useful are clinical, biochemical, and cross-sectional imaging features in predicting potentially malignant or malignant cystic lesions of the pancreas? J Am Coll Surg. 2008;206:17–27. doi:10.1016/j.jamcollsurg.2007.06.312
12. Kajbafzadeh AM, Elmi A, Talab SS, Emami H, Esfahani SA, Saeedi P. Urinary and serum carbohydrate antigen 19-9 as a biomarker in ureteropelvic junction obstruction in children. J Urol. 2010;183:2353–2360. doi:10.1016/j.juro.2010.02.031
13. Dyckhoff G, Warta R, Gonnermann A, Plinkert PK, Flechtenmacher C, Volkmann M. Carbohydrate antigen 19-9 in saliva: possible preoperative marker of malignancy in parotid tumors. Otolaryngol Head Neck Surg. 2011;145:772–777. doi:10.1177/0194599811414512
14. Roy S, Dasgupta A, Kar K. Comparison of urinary and serum CA 19-9 as markers of early-stage urothelial carcinoma. Int Braz J Urol. 2013;39:631–638. doi:10.1590/S1677-5538.IBJU.2013.05.04
15. Kim S, Park BK, Seo JH, et al. Carbohydrate antigen 19-9 elevation without evidence of malignant or pancreatobiliary diseases. Sci Rep. 2020;10:8820. doi:10.1038/s41598-020-65720-8
16. Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA. 2007;297(3):267–277. doi:10.1001/jama.297.3.267
17. Berger AC, Winter K, Hoffman JP, et al. Five-year results of US intergroup/RTOG 9704 with postoperative CA 19-9 ≤90 U/mL and comparison to the CONKO-001 trial. Int J Radiat Oncol Biol Phys. 2012;84(3):e291–e297. doi:10.1016/j.ijrobp.2012.04.035
18. Lee T, Teng TZJ, Shelat VG. Carbohydrate antigen 19-9 - tumor marker: past, present, and future. World J Gastrointest Surg. 2020;12(12):468–490. doi:10.4240/wjgs.v12.i12.468
19. Xu P, Wang X, Qian J, Li Z, Yao J, Xu A. The prognostic evaluation of CA19-9, D-dimer and TNFAIP3/A20 in patients with pancreatic ductal adenocarcinoma. Medicine (Baltimore). 2021;100(6):e24651. doi:10.1097/MD.0000000000024651
20. Kowalchuk RO, Lester SC, Graham RP, et al. Predicting Adverse pathologic features and clinical outcomes of resectable pancreas cancer with preoperative CA 19-9. Front Oncol. 2021;11:651119. doi:10.3389/fonc.2021.651119
21. Ye C, Sadula A, Ren S, et al. The prognostic value of CA19-9 response after neoadjuvant therapy in patients with pancreatic cancer: a systematic review and pooled analysis. Cancer Chemother Pharmacol. 2020;86(6):731–740. doi:10.1007/s00280-020-04165-2
22. Liu H, Zenati MS, Rieser CJ, et al. CA19-9 change during neoadjuvant therapy may guide the need for additional adjuvant therapy following resected pancreatic cancer. Ann Surg Oncol. 2020;27(10):3950–3960. doi:10.1245/s10434-020-08468-9
23. Reni M, Peretti U, Zanon S, et al. Time to CA19-9 nadir: a clue for defining optimal treatment duration in patients with resectable pancreatic ductal adenocarcinoma. Cancer Chemother Pharmacol. 2020;85(4):641–650. doi:10.1007/s00280-020-04047-7
24. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
25. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
26. MacDonald N. Cancer cachexia and targeting chronic inflammation: a unified approach to cancer treatment and palliative/supportive care. J Support Oncol. 2007;5(4):157–162.
27. Zambirinis CP, Pushalkar S, Saxena D, Miller G. Pancreatic cancer, inflammation, and microbiome. Cancer J. 2014;20(3):195–202. doi:10.1097/PPO.0000000000000045
28. Steele CW, Jamieson NB, Evans TRJ, et al. Exploiting inflammation for therapeutic gain in pancreatic cancer. Br J Cancer. 2013;108(5):997–1003. doi:10.1038/bjc.2013.24
29. Shimizu T, Taniguchi K, Asakuma M, et al. Lymphocyte-to-monocyte ratio and prognostic nutritional index predict poor prognosis in patients on chemotherapy for unresectable pancreatic cancer. Anticancer Res. 2019;39(4):2169–2176. doi:10.21873/anticanres.13331
30. McMillan DC. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat Rev. 2013;39(5):534–540. doi:10.1016/j.ctrv.2012.08.003
31. Yamada S, Fujii T, Yabusaki N, et al. Clinical implication of inflammation-based prognostic score in pancreatic cancer: Glasgow Prognostic Score is the most reliable parameter. Medicine (Baltimore). 2016;95(18):e3582. doi:10.1097/MD.0000000000003582
32. Xiao Y, Xie Z, Shao Z, et al. Prognostic value of post-diagnostic inflammation-based scores in short-term overall survival of advanced pancreatic ductal adenocarcinoma patients. Medicine (Baltimore). 2017;96(50):e9247. doi:10.1097/MD.0000000000009247
33. Shirai Y, Shiba H, Haruki K, et al. Preoperative platelet-to-albumin ratio predicts prognosis of patients with pancreatic ductal adenocarcinoma after pancreatic resection. Anticancer Res. 2017;37(2):787–793. doi:10.21873/anticanres.11378
34. Jomrich G, Gruber ES, Winkle D, et al. Systemic immune-inflammation index (SII) predicts poor survival in pancreatic cancer patients undergoing resection. J Gastrointest Surg. 2020;24(3):610–618. doi:10.1007/s11605-019-04187-z
35. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
36. Pacheco-Barcia V, Mondéjar Solís R, France T, et al. A systemic inflammation response index (SIRI) correlates with survival and predicts oncological outcome for mFOLFIRINOX therapy in metastatic pancreatic cancer. Pancreatology. 2020;20(2):254–264. doi:10.1016/j.pan.2019.12.010
37. Hammel P, Huguet F, van Laethem J, et al. Effect of chemoradiotherapy vs chemotherapy on survival in patients with locally advanced pancreatic cancer controlled after 4 months of gemcitabine with or without erlotinib: the LAP07 randomized clinical trial. JAMA. 2016;315(17):1844–1853. doi:10.1001/jama.2016.4324
38. Ioka T, Furuse J, Fukutomi A, et al. Randomized Phase II study of chemoradiotherapy with versus without induction chemotherapy for locally advanced pancreatic cancer: Japan Clinical Oncology Group trial, JCOG1106. Jpn J Clin Oncol. 2021;51(2):235–243. doi:10.1093/jjco/hyaa198
39. Choi SH, Park SW, Seong J. A nomogram for predicting survival of patients with locally advanced pancreatic cancer treated with chemoradiotherapy. Radiother Oncol. 2018;129(2):340–346. doi:10.1016/j.radonc.2018.08.006
40. Ferrone CR, Finkelstein DM, Thayer SP, Muzikansky A, Fernandez-delCastillo C, Warshaw AL. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J Clin Oncol. 2006;24(18):2897–2902. doi:10.1200/JCO.2005.05.3934
41. Herreros-Villanueva M, Ruiz-Rebollo L, Montes M, et al. CA19-9 capability as predictor of pancreatic cancer resectability in a Spanish cohort. Mol Biol Rep. 2020;47(3):1583–1588. doi:10.1007/s11033-020-05245-5
42. Balkwill FR, Capasso M, Hagemann T. The tumor microenvironment at a glance. J Cell Sci. 2012;125(23):5591–5596. doi:10.1242/jcs.116392
43. Yang S, Wang X, Contino G, et al. Pancreatic cancers require autophagy for tumor growth. Genes Dev. 2011;25(7):717–729. doi:10.1101/gad.2016111
44. Aghajan M, Li N, Karin M. Obesity, autophagy and the pathogenesis of liver and pancreatic cancers. J Gastroenterol Hepatol. 2012;27(Suppl 2):10–14. doi:10.1111/j.1440-1746.2011.07008.x
45. Versteijne E, Vogel JA, Besselink MG, et al. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br J Surg. 2018;105(8):946–958. doi:10.1002/bjs.10870
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.