")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
The Prevalence of Diabetes, Prediabetes and Associated Risk Factors in Hangzhou, Zhejiang Province: A Community-Based Cross-Sectional Study
Authors Shi M , Zhang X, Wang H
Received 5 December 2021
Accepted for publication 16 February 2022
Published 3 March 2022 Volume 2022:15 Pages 713—721
DOI https://doi.org/10.2147/DMSO.S351218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Mingming Shi,1,* Xiao Zhang,2,* Hui Wang1
1Center for Disease Control and Prevetion of Shangcheng District, Hangzhou, Zhejiang, 310000, People’s Republic of China; 2Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingming Shi, Email [email protected]
Objective: Little information is available on the prevalence and associated risk factors of diabetes and prediabetes in the community located in Hangzhou city, Zhejiang Province, southeast China. This study aims to investigate the prevalence of adult diabetes and prediabetes and their associated risk factors among a community population in Hangzhou.
Methods: A multistage sampling method was used in this study. Ten communities located in Shangcheng district of Hangzhou city were selected, and 3096 permanent residents (resident for ≥ 6 months) aged 18 years and above were enrolled into this study. Finally, a total of 2986 participants were included. A questionnaire interview and physical examination were conducted for all participants by trained investigators in a local medical center. Anthropometric measurements covered height, weight, waist circumference (WC) and blood pressure, while the blood tests included fasting blood glucose, an oral glucose tolerance test and fasting lipid profiles. The American Diabetes Association diabetes diagnosis criteria were used to discriminate among normal blood glucose, diabetes and prediabetes. The Rao–Scott adjusted χ2 test and complex sampling design-based unconditional multivariate logistic regression analysis were used to evaluate factors associated with diabetes and prediabetes. Descriptive and inferential statistics were calculated in Stata version 15. P-values < 0.05 indicate statistical significance.
Results: The overall prevalence of diabetes was 13.97%, of which 81.54% had prediagnosed diabetes and 18.46% were newly diagnosed with diabetes in the present study. The prevalence of prediabetes was 18.89%. Multivariable logistic regression analysis showed that age, education, once smoking, family history of diabetes, obesity, central obesity and hypertension were factors associated with diabetes, while age, smoking, drinking, central obesity and hypertension were significant factors related to prediabetes.
Conclusion: The prevalence of diabetes and prediabetes in adults in Hangzhou city remains high. Interventions aiming to modify risk factors such as drinking, obesity, central obesity and hypertension are urgently required.
Keywords: diabetes, prediabetes, prevalence, associated factors
Introduction
Diabetes mellitus is not only a well-known leading cause of death but also an increasing burden on healthcare worldwide.1,2 It was estimated that 451 million people aged 18–99 years had diabetes in 2017, and these figures are expected to reach 693 million by 2045.3 Studies have proved that elevated blood sugar levels are associated with an increased risk of cardiovascular disease and metabolic syndrome.4,5 The concept of prediabetes has been defined by the American Diabetes Association as the presence of impaired fasting glucose (IFG) (fasting plasma glucose [FPG] levels of 5.6–6.9 mmol/L) or impaired glucose tolerance (IGT) (2-hour values in the oral glucose tolerance test [OGTT] of 7.8–11.0 mmol/L).6 Previous research has shown that prediabetes increases the risk of developing type 2 diabetes; according to the Diabetes Prevention Program (DPP), around 11% of people with prediabetes become diabetic annually.7,8 Moreover, prediabetes is associated with an increased risk of cardiovascular disease and all-cause mortality in adults.9
There is a high prevalence of diabetes and prediabetes in China. In the latest nationally representative cross-sectional study, conducted in 2013, the overall prevalence of full diabetes was nearly 10.9%. The prevalence of prediabetes in China is 35.7%,10 higher than in India (5.7%), South Korea (22.7%) and Saudi Arabia (27.6%).11–13 Although several studies14–17 have focused on prediabetes and diabetes in China, marked ethical and geographical differences exist in the prevalence of both prediabetes and diabetes. Meanwhile, surveys have rarely been conducted on the prevalence of diabetes and prediabetes and their associated factors in community populations in Hangzhou, a city located in the Yangtze river delta, southeast China. To provide reliable data and suggestions to local medical policy makers, this study aims to estimate the prevalence of diabetes and prediabetes and explore their potential associated risk factors in Shangcheng district, Hangzhou city.
Design and Methods
Study Design
This community-based cross-sectional study was conducted in Shangcheng district, Hangzhou city, located in southeast China. This study adopted a multistage sampling method to select adult permanent residents in the target area. First, 10 communities were selected from 54 communities in this region using a simple random sampling method. Secondly, permanent residents (only people who had been living in Shangcheng district for at least 6 months) in the selected communities who were ≥18 years old were enrolled by a systematic sampling method. The following subjects were removed: 1) those who had been living in Shangcheng district for less than 6 months; and 2) those who had a mental illness that would prevent them from completing questionnaires and physical tests independently. In total, 3096 participants completed the interview; after excluding invalid questionnaires, 2986 participants were finally included in the study. Written informed consent was obtained from all subjects in the survey.
Questionnaire Investigation
The interview was conducted by trained investigators in a local health center using structured questionnaires. The questionnaires included questions on participants’ socio-demographic characteristics, health-related information and lifestyle information. Each questionnaire was examined by the interviewer through a parallel double-entry system after being completed by participants.
Physical Examination
Trained investigators conducted the physical examination, which consisted of anthropometric measurements, including weight and height, fasting blood glucose (FBG), blood pressure and blood lipid levels. Blood samples were collected from participants after an overnight fast of 10 hours or more. After collection, the samples were placed in a cold-chain system before being tested at a local medical center laboratory.
Definition of Variables
Diabetes: FBG ≥7.0 mmol/L, oral glucose tolerance test (OGTT-2h) ≥11.0 mmol/L plasma glucose or self-reported use of antidiabetic medication during the 2 weeks prior to the examination. Prediabetes: FBG 5.6–6.9 mmol/L, OGTT-2h 7.8–10.9 mmol/L.18
Hypertension: systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg.19
Dyslipidemia: total cholesterol (TC) ≥6.2 mmol/L and/or triglyceride (TG) ≥2.3 mmol/L and/or high-density lipoprotein cholesterol (HDL-C) ≤1.0 mmol/L and/or low-density lipoprotein cholesterol (LDL-C) ≥4.1 mmol/L.20
Body mass index (BMI): for the Chinese population, a BMI of 18.5–23.9 kg/m2 is defined as normal, underweight is defined as a BMI <18.5 kg/m2, overweight is defined as a BMI of 24–27.9 kg/m2 and obesity as a BMI ≥28 kg/m2.21
Central obesity: for the Chinese population, central obesity is defined as a waist circumference (WC) measurement of >85 cm for females and >90 cm for males.22
Age groups: three categories of young (18–44 years), middle (45–59 years) and old (60 years and older).
Smoking: a smoker was defined as a person who smoked at least one cigarette per day within the last 6 months; once smoking was defined as a person who smoked at least one cigarette per day in the past, but was no longer a smoker.
Secondhand smoker: a person who has been exposed to secondhand smoke in a typical week.23
Drinker: a person who consumed at least one alcoholic drink per week was defined as a drinker; a once-drinker was defined as a person who consumed at least one alcoholic drink per week in the past, but was no longer a drinker.
Exercise: participants were divided into “never or rare”, meaning those who did not exercise or rarely exercised; those who exercised one or two times a week were defined as “sometimes exercise”; and those with an exercise frequency of more than three times a week were defined as “exercise frequently”.24
Statistical Analyses
Data analysis was performed in Stata 15.0 software (Stata Corporation LLC, College Station, TX, USA). Descriptive analysis included the estimation of mean values and standard deviations for numerical variables. Frequency and percentage were displayed for categorical variables and prevalence values. The Rao–Scott adjusted χ2 test was used to compare the factors between diabetes or prediabetes and normal blood glucose. A complex sampling design based on unconditional multivariate logistic regression analysis was carried out to estimate the independent effect of the factors on diabetes and prediabetes. For all analyses, a P-value <0.05 was considered to be statistically significant.
Results
A total of 3096 participants were initially recruited and 2986 participants were finally included in this study, with a 96.5% response rate. The general characteristics are shown in Table 1. There were 1345 men (45%) and 1641 women (55%) in the present study. The mean age of the study population was 55.71 (SD: 18) years. Less than 15% of participants had an educational level of primary school and below. Subjects with prediabetes, diabetes and normal blood glucose had similar patterns of demographic characteristics, with the majority being married/cohabiting, never smoking, never drinking and not being secondhand smokers. In total, 408 subjects (13.6%) had a family history of diabetes. The mean BMI of those with normal blood glucose, prediabetes and diabetes was 22.54, 23.60 and 24.36 kg/m2, respectively. The prevalences of hypertension, dyslipidemia and obesity were higher in participants with prediabetes or diabetes than in the normal blood glucose group.
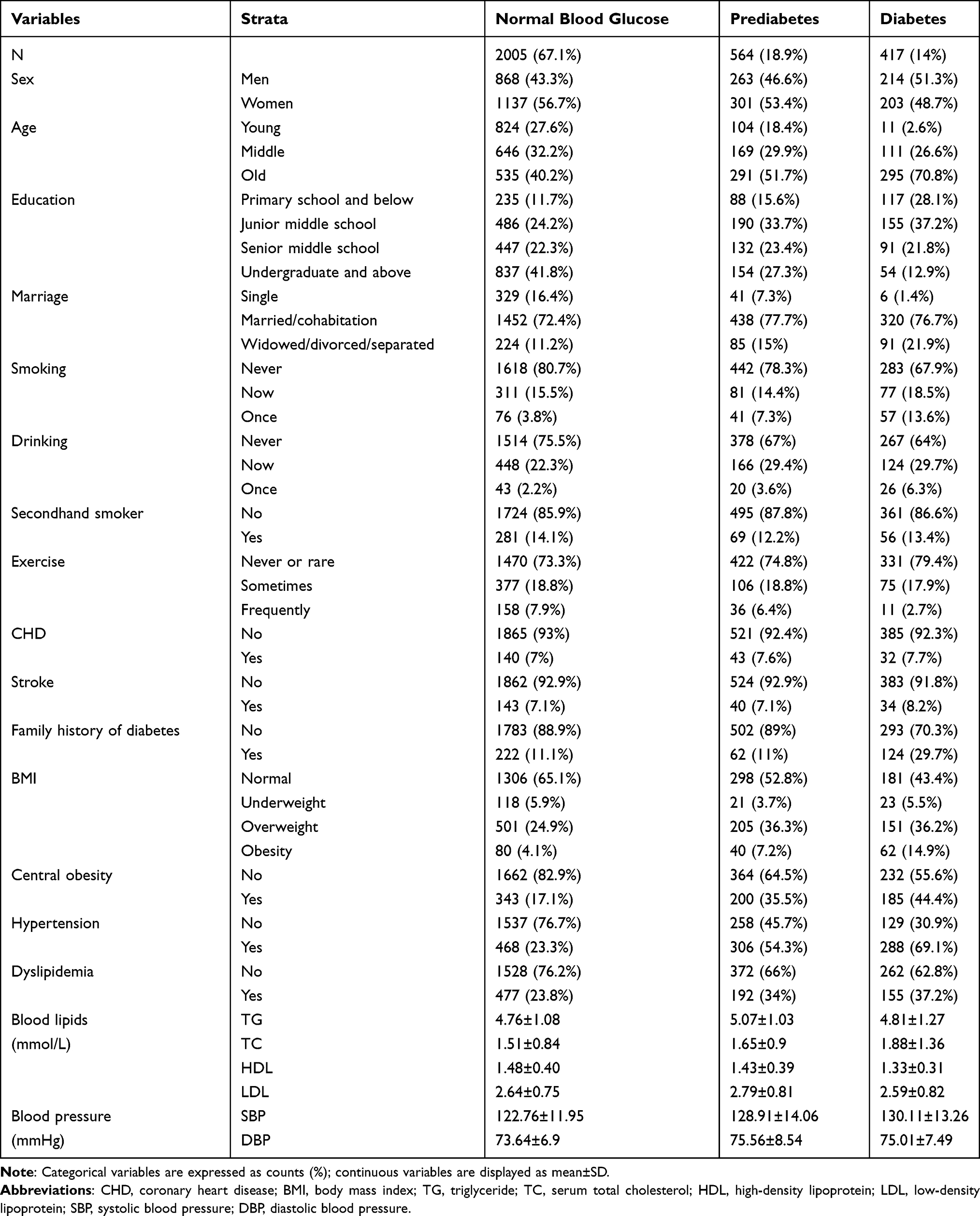 |
Table 1 General Characteristics of the Community Adult Population in Hangzhou City |
Among the participants in the present survey, the estimated prevalences of diabetes and prediabetes were 13.97% and 18.89%, respectively. Among the diabetic participants, 81.54% were previously diagnosed diabetic patients and 18.46% were newly diagnosed in this study. Older participants showed a higher prevalence of prediabetes and diabetes than young or middle-aged participants. Women showed a higher prevalence of prediabetes than men, while for men a higher prevalence of diabetes was observed compared with women (Table 1).
As shown in Table 2, the significant factors for prediabetes were age, education, marriage, smoking, drinking, BMI, central obesity, hypertension and dyslipidemia. Significant differences were observed in sex, age, education, marriage, smoking, drinking, exercise, family history of diabetes, BMI, central obesity, hypertension and dyslipidemia between the diabetes group and the normal blood glucose group (Table 2).
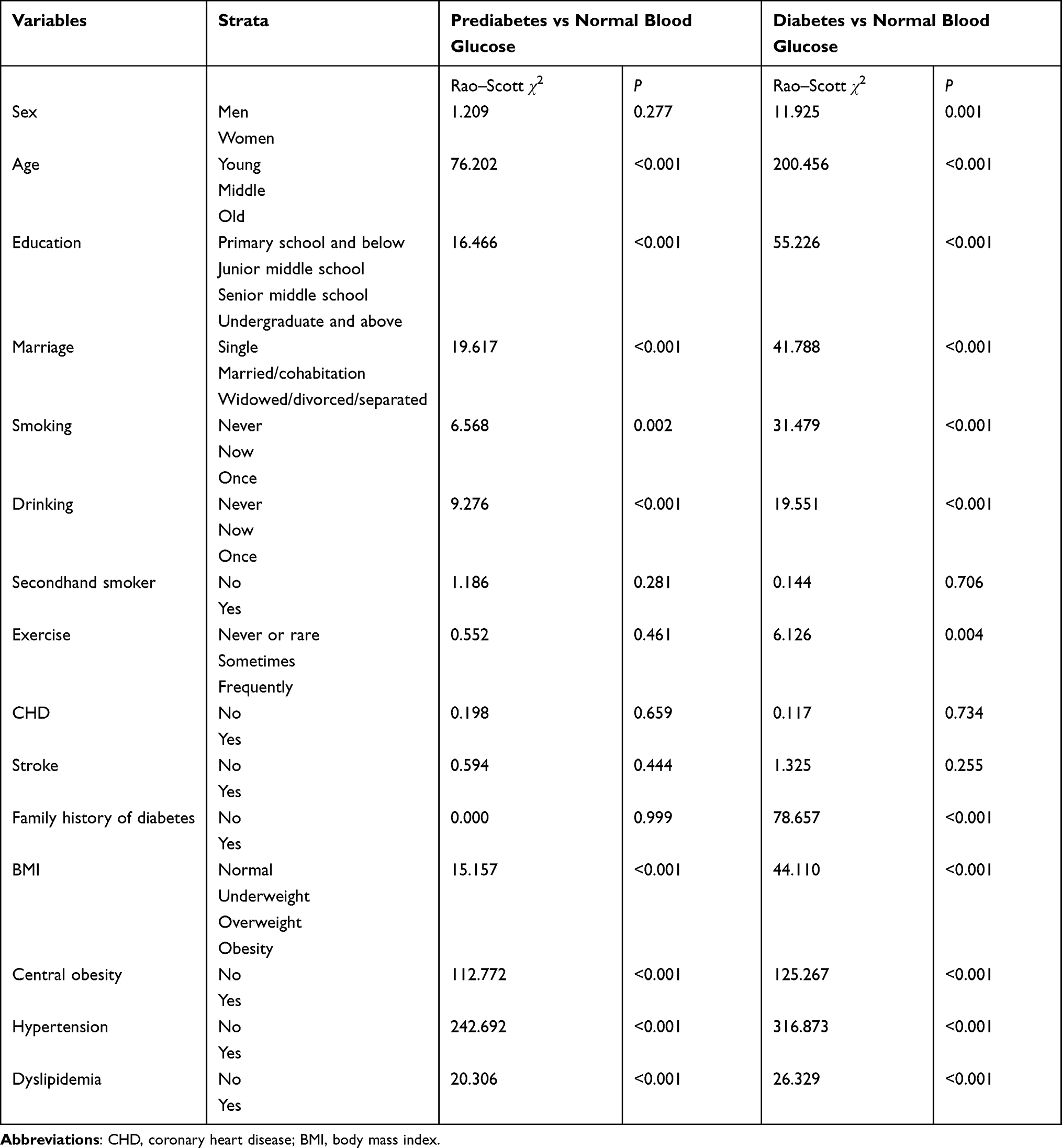 |
Table 2 Comparison of Factors Between the Normal Blood Glucose Group and the Prediabetes or Diabetes Group |
The complex sampling design-based unconditional multivariate logistic regression analysis uncovered that the significant factors associated with prediabetes were age, smoking, drinking, central obesity and hypertension. The significant factors associated with diabetes were age, educational level of undergraduate and above, once smoking, family history of diabetes, obesity, central obesity and hypertension (Table 3).
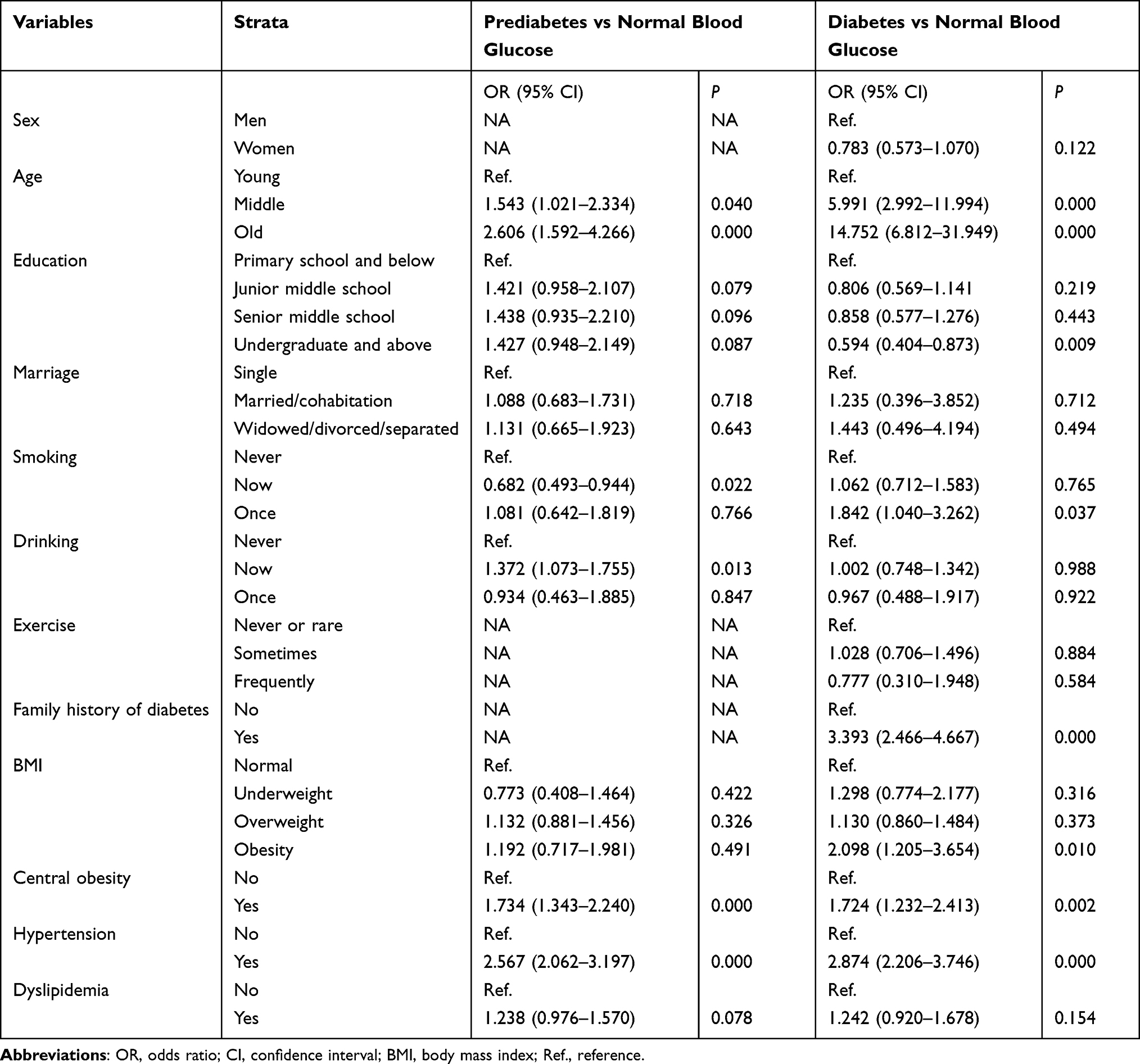 |
Table 3 Multivariable Logistic Regression of Factors Associated with Prediabetes and Diabetes |
Discussion
The prevalence of diabetes in the present study participants was 13.97%. According to a previous study, the prevalence of total diabetes was 10.9% (95% CI, 10.4–11.5%) in a nationally representative cross-sectional survey conducted in mainland China with 170,287 participants, which is lower than the prevalence of diabetes in this study.10 The prevalence of prediabetes in the current study was higher than in populations in other Asian countries. A study in Pakistan reported a prevalence of prediabetes of 14.4% in 2016–2017,25 and a cross-sectional study in Malaysia showed that the level of prediabetes reached 10.12%.26 In this study, the prevalence of prediabetes was 18.89%, almost 1.5 times the percentage of participants with diabetes. In a sample of 18,362 Chinese adults in 2018, the prevalence of prediabetes was 19.8%,27 which is slightly higher than our observations. This reveals that in Hangzhou, nearly one in five adults have prediabetes, and since it is a high-risk factor for the development of diabetes, the Chinese government should pay more attention to prediabetic populations.
This study illustrated that increasing age, a family history of diabetes and obesity were factors significantly associated with diabetes, which has a sound basis in the literature.28 In this study, a higher level of education is a protective factor for diabetes, which may be related to the understanding of diabetes and the inclination to maintain a healthy lifestyle.29 In addition, this study showed that central obesity (WC), hypertension and once smoking were also significant risk factors for diabetes. People with an excess WC are more likely to have not only a metabolic disease but also an increased risk of premature death.30,31 As an early signal of chronic disease, central obesity is more sensitive than BMI.32 In line with previous studies, our study also supported that diabetes is associated with a high prevalence of hypertension.33 The exact pathway through which hypertension increases the risk of diabetes has been illustrated in a previous study.34 Comorbid hypertension and diabetes not only increases the risk of cardiovascular diseases among patients,35 but also significantly impacts the management of both conditions. Community-based efforts such as the national basic health service project have been implemented by Ministry of Health China to improve the screening, diagnosis and treatment of chronic diseases (such as hypertension and diabetes), and will have an impact on early detection, prompting the management and prevention of complications that negatively affect the quality of life of patients. Similarly to a previous study, our study found that smoking cessation did not reduce the risk of diabetes; on the contrary, adults who quit smoking had an increased risk for diabetes, which may be related to weight gain and systemic inflammation.36
Age, central obesity, hypertension and drinking were significant factors associated with prediabetes in our study. Similarly to the current study, a study conducted in Jilin, a province in northeast China, demonstrated that increasing age and central obesity were the factors associated with prediabetes.27 In our study, it was found that not drinking is a protective factor for prediabetes. Compared to the normal blood glucose group, the prediabetes group had a larger prevalence of hypertension. Current recommendations and our study suggest a need to focus on the comorbidity of diabetes and hypertension. However, the effect of combined prediabetes and hypertension on all-cause mortality may be stronger among young and middle-aged people.37 A previous study, performed as part of the China Patient-Centered Evaluative Assessment of Cardiac Events Million Persons Project, which enrolled 898,929 young and middle-aged participants, showed a level of hypertension of 26.15%.38 It showed that more than one in four young and middle-aged people in China had hypertension. Considering the comorbidity of prediabetes and hypertension in young and middle-aged people, the Chinese government needs to pay attention to prediabetes and to provide proper policies to reduce the trend of prediabetes and hypertension in the population, especially in young and middle-aged people.
We were surprised that current smoking was negatively correlated with prediabetes. Two possible explanations for this are given. 1) Despite the inflammatory burden imposed by smoking, nicotine and its metabolites, through 7-nicotinic acetylcholine receptors, may exert anti-inflammatory effects. These effects have been documented elsewhere in leukocyte cells and adipocytes, both in vitro39 and in vivo.40 2) A previous study showed that patients with predisposing hypertension, who were newly diagnosed with diabetes, showed a higher tendency to continue smoking.41 In the present study, 54.26% of the patients diagnosed with prediabetes also had hypertension, while only 23.3% of the normoglycemic population also had hypertension. The association between smoking and prediabetes may be due to the high prevalence of smoking in a hypertensive population. Further study is necessary to confirm the relationship between smoking and prediabetes.
Our study has several strengths. First, compared to previous studies from this region,42–44 this is the first study looking at the prevalence and risk factors of prediabetes among a community population in Hangzhou city. The large and representative study sample allowed us to estimate the prevalence of diabetes and prediabetes in this region. The sample analyzed in this study was obtained with a multistage random sampling method to guarantee that the sample was representative of the population in this region. The response rate was very high, and the use of a standardized training manual to train the research assistants allowed a consistent and systematic method of collecting the data, which increased the reliability of the measurements. Secondly, statistical methods matched to the study design were used to accurately derive factors associated with diabetes or prediabetes. Finally, the study reached conclusions about the relationship between smoking and prediabetes that are inconsistent with other studies,45,46 and these may provide us with some ideas for future research. Nonetheless, there are several limitations in our study. The use of self-reported information, such as drinking, smoking and taking exercise, may lead to recall bias. The inherent features of the cross-sectional design of the study limit any potential inference of causality and temporal relationships between the variables, which may lead to selection bias. In addition, the study did not distinguish between type I and type 2 diabetes, although most participants had type 2 diabetes, and considering the small number of cases of newly diagnosed diabetes, we did not explore this further. Future research with a larger sample of these individuals is needed to explore newly diagnosed diabetes and its associated risk factors.
Conclusion
The level of prediabetes and diabetes in Shangcheng district, Hangzhou city, that we show in this study indicates that the medical authority needs to increase its focus on this area and appropriate actions need to be taken. Given the link between blood sugar levels and the incidence of cardiometabolic disorders, education on a healthy lifestyle is needed at a community level, and participants with prediabetes and diabetes should monitor their health regularly.
Data Sharing Statement
To protect the participants’ identities, the dataset will not be shared.
Ethical Consideration
Ethical clearance and approval for this study was obtained from Institutional Review Board (IRB) of the Center for Disease Control and Prevention, Shangcheng District. Written consent was obtained from all participants after detailed clarification of the aim of the study. They had been given the right to refuse and assured of the confidentiality of the response. The privacy of the participants was kept by using unique codes. The outcomes of the laboratory results were delivered to the study participants and those in need of medical attention were recommended to visit health institutions. Participants’ informed consent included publication of anonymized responses, and that this study was conducted in accordance with the Declaration of Helsinki.
Disclosure
Mingming Shi and Xiao Zhang are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Al Kaabi J. Epidemiology of Type 2 diabetes - global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–111. PMID: 32175717; PMCID: PMC7310804. doi:10.2991/jegh.k.191028.001
2. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. PMID: 32901098; PMCID: PMC7478957. doi:10.1038/s41598-020-71908-9
3. Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. PMID: 29496507. doi:10.1016/j.diabres.2018.02.023
4. Huebschmann AG, Huxley RR, Kohrt WM, Zeitler P, Regensteiner JG, Reusch JEB. Sex differences in the burden of type 2 diabetes and cardiovascular risk across the life course. Diabetologia. 2019;62(10):1761–1772. PMID: 31451872; PMCID: PMC7008947. doi:10.1007/s00125-019-4939-5
5. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. PMID: 29459239; PMCID: PMC5953551. doi:10.1016/j.cjca.2017.12.005
6. Rayburn WF. Diagnosis and classification of diabetes mellitus: highlights from the American Diabetes Association. J Reprod Med. 1997;42(9):585–586. PMID: 9336756.
7. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: a high-risk state for diabetes development. Lancet. 2012;379(9833):2279–2290. PMID: 22683128; PMCID: PMC3891203. doi:10.1016/S0140-6736(12)60283-9
8. Knowler WC, Fowler SE, Hamman RF, et al.; Diabetes Prevention Program Research Group. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374(9702):1677–1686. PMID: 19878986; PMCID: PMC3135022. doi:10.1016/S0140-6736(09)61457-4
9. Huang Y, Cai X, Mai W, Li M, Hu Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953. PMID: 27881363; PMCID: PMC5121106. doi:10.1136/bmj.i5953
10. Wang L, Gao P, Zhang M, et al. Prevalence and ethnic pattern of diabetes and prediabetes in China in 2013. JAMA. 2017;317(24):2515–2523. PMID: 28655017; PMCID: PMC5815077. doi:10.1001/jama.2017.7596
11. Subramani SK, Yadav D, Mishra M, Pakkirisamy U, Mathiyalagen P, Prasad G. Prevalence of Type 2 diabetes and prediabetes in the Gwalior-Chambal Region of Central India. Int J Environ Res Public Health. 2019;16(23):4708. PMID: 31779187; PMCID: PMC6926613. doi:10.3390/ijerph16234708
12. Lee JE, Jung SC, Jung GH, et al. Prevalence of diabetes mellitus and prediabetes in Dalseong-gun, Daegu City, Korea. Diabetes Metab J. 2011;35(3):255–263. PMID: 21785746; PMCID: PMC3138089. doi:10.4093/dmj.2011.35.3.255
13. Aldossari KK, Aldiab A, Al-Zahrani JM, et al. Prevalence of prediabetes, diabetes, and its associated risk factors among males in Saudi Arabia: a Population-Based Survey. J Diabetes Res. 2018;2018:2194604. PMID: 29850599; PMCID: PMC5941814. doi:10.1155/2018/2194604
14. Shen XM, Huang YQ, Zhang XY, Tong XQ, Zheng PF, Shu L. Association between dietary patterns and prediabetes risk in a middle-aged Chinese population. Nutr J. 2020;19(1):77. PMID: 32731880; PMCID: PMC7393887. doi:10.1186/s12937-020-00593-1
15. Yang W, Lu J, Weng J; China National Diabetes and Metabolic Disorders Study Group. Prevalence of diabetes among men and women in China. N Engl J Med. 2010;362(12):1090–1101. PMID: 20335585. doi:10.1056/NEJMoa0908292
16. Song Y, Zhang X, Zhang H, et al. Prevalence of diabetes and prediabetes in adults from a third-tier city in Eastern China: a Cross-Sectional Study. Diabetes Ther. 2019;10(4):1473–1485. PMID: 31254225; PMCID: PMC6612348. doi:10.1007/s13300-019-0655-x
17. Yu X, Duan F, Lin D, et al. Prevalence of diabetes, prediabetes, and associated factors in an adult Chinese population: baseline of a Prediabetes Cohort Study. Int J Endocrinol. 2020;2020:8892176. PMID: 33299413; PMCID: PMC7707990. doi:10.1155/2020/8892176
18. Petersmann A, Müller-Wieland D, Müller UA, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes. 2019;127(S 01):S1–S7. PMID: 31860923. doi:10.1055/a-1018-9078
19. Shen Y, Chang C, Zhang J, Jiang Y, Ni B, Wang Y. Prevalence and risk factors associated with hypertension and prehypertension in a working population at high altitude in China: a cross-sectional study. Environ Health Prev Med. 2017;22(1):19. PMID: 29165123; PMCID: PMC5664790. doi:10.1186/s12199-017-0634-7
20. Guo C, Cao H, Shan G, et al. Elevated lipoprotein(a) and risk of coronary heart disease according to different lipid profiles in the general Chinese community population: the CHCN-BTH study. Ann Transl Med. 2021;9(1):26. PMID: 33553319; PMCID: PMC7859748. doi:10.21037/atm-20-3899
21. Chen C, Lu FC; Department of Disease Control Ministry of Health, PR China. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed Environ Sci. 2004;17 Suppl:1–36. PMID: 15807475.
22. Hou XG, Wang C, Ma ZQ, et al. Optimal waist circumference cut-off values for identifying metabolic risk factors in middle-aged and elderly subjects in Shandong Province of China. Biomed Environ Sci. 2014;27(5):353–359. PMID: 24827716. doi:10.3967/bes2014.060
23. Zheng Y, Ji Y, Dong H, Chang C. The prevalence of smoking, second-hand smoke exposure, and knowledge of the health hazards of smoking among internal migrants in 12 provinces in China: a cross-sectional analysis. BMC Public Health. 2018;18(1):655. PMID: 29793454; PMCID: PMC5968586. doi:10.1186/s12889-018-5549-8
24. Wang R, Zhang P, Lv X, et al. Association between passive smoking and mental distress in adult never-smokers: a cross-sectional study. BMJ Open. 2016;6(7):e011671. PMID: 27473950; PMCID: PMC4985981. doi:10.1136/bmjopen-2016-011671
25. Basit A, Fawwad A, Qureshi H, Shera AS; NDSP Members. Prevalence of diabetes, pre-diabetes and associated risk factors: second National Diabetes Survey of Pakistan (NDSP), 2016–2017. BMJ Open. 2018;8(8):e020961. doi:10.1136/bmjopen-2017-020961
26. Rahim FF, Abdulrahman SA, Kader maideen SF, Rashid A. Prevalence and factors associated with prediabetes and diabetes in fishing communities in Penang, Malaysia: a cross-sectional study. PLoS One. 2020;15(2):e0228570. doi:10.1371/journal.pone.0228570
27. Wang R, Zhang P, Li Z, et al. The prevalence of pre-diabetes and diabetes and their associated factors in Northeast China: a cross-sectional study. Sci Rep. 2019;9(1):2513. doi:10.1038/s41598-019-39221-2
28. Zhao M, Lin H, Yuan Y, et al. Prevalence of pre-diabetes and its associated risk factors in rural areas of Ningbo, China. Int J Environ Res Public Health. 2016;13(8):808. PMID: 27517947. doi:10.3390/ijerph13080808
29. McWilliams JM, Meara E, Zaslavsky AM, Ayanian JZ. Differences in control of cardiovascular disease and diabetes by race, ethnicity, and education: u.S. trends from 1999 to 2006 and effects of medicare coverage. Ann Intern Med. 2009;150(8):505–515. PMID: 19380852. doi:10.7326/0003-4819-150-8-200904210-00005
30. Bugge A, Möller S, Westfall DR, et al. Associations between waist circumference, metabolic risk and executive function in adolescents: a cross-sectional mediation analysis. PLoSOne. 2018;13(6):e0199281. PMID: 29912925; PMCID: PMC6005548. doi:10.1371/journal.pone.0199281
31. Cameron AJ, Romaniuk H, Orellana L, et al. Combined influence of waist and hip circumference on risk of death in a large cohort of European and Australian adults. J Am Heart Assoc. 2020;9(13):e015189. PMID: 32602397; PMCID: PMC7670538. doi:10.1161/JAHA.119.015189
32. Ross R, Neeland IJ, Yamashita S, et al. Waist circumference as a vital sign in clinical practice: a Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat Rev Endocrinol. 2020;16(3):177–189. PMID: 32020062; PMCID: PMC7027970. doi:10.1038/s41574-019-0310-7
33. Lago RM, Singh PP, Nesto RW. Diabetes and hypertension. Nature clinical practice. Endocrinol Metab. 2007;3:667. doi:10.1038/ncpendmet0638
34. Sarzani R, Salvi F, Dessì-Fulgheri P, Rappelli A. Renin-angiotensin system, natriuretic peptides, obesity, metabolic syndrome, and hypertension: an integrated view in humans. J Hypertens. 2008;26(5):831–843. PMID: 18398321. doi:10.1097/HJH.0b013e3282f624a0
35. Jadhav AN, Tarte PR. Acute cardiovascular complications in patients with diabetes and hypertension: management consideration for minor oral surgery. J Korean Assoc Oral Maxillofac Surg. 2019;45(4):207–214. PMID: 31508353; PMCID: PMC6728621. doi:10.5125/jkaoms.2019.45.4.207
36. Yeh HC, Duncan BB, Schmidt MI, Wang NY, Brancati FL. Smoking, smoking cessation, and risk for type 2 diabetes mellitus: a cohort study. Ann Intern Med. 2010;152(1):10–17. PMID: 20048267; PMCID: PMC5726255. doi:10.7326/0003-4819-152-1-201001050-00005
37. Huang YQ, Liu L, Huang JY, et al. Prediabetes and risk for all-cause and cardiovascular mortality based on hypertension status. Ann Transl Med. 2020;8(23):1580. PMID: 33437779; PMCID: PMC7791204. doi:10.21037/atm-20-1155
38. Mahajan S, Feng F, Hu S, et al. Assessment of prevalence, awareness, and characteristics of isolated systolic hypertension among younger and middle-aged adults in China. JAMA NetwOpen. 2020;3(12):e209743. PMID: 33289843; PMCID: PMC7724558. doi:10.1001/jamanetworkopen.2020.9743
39. Rehani K, Scott DA, Renaud D, et al. Cotinine-induced convergence of the cholinergic and PI3 kinase-dependent anti-inflammatory pathways in innate immune cells. BiochimBiophysActa. 2008;1783(3):375–382. PMID: 18178163. doi:10.1016/j.bbamcr.2007.12.003
40. Wittebole X, Hahm S, Coyle SM, Kumar A, Calvano SE, Lowry SF. Nicotine exposure alters in vivo human responses to endotoxin. Clin Exp Immunol. 2007;147(1):28–34. PMID: 17177960; PMCID: PMC1810444. doi:10.1111/j.1365-2249.2006.03248.x
41. Cho MH, Kim SM, Lee K, et al. Factors associated with continued smoking after the diagnosis of type 2 diabetes: a retrospective study in the Korean cohort. BMJ Open. 2018;8(6):e020160. PMID: 29961006; PMCID: PMC6042621. doi:10.1136/bmjopen-2017-020160
42. Wang M, Hu RY, Gong WW, et al. Trends in prevalence of gestational diabetes mellitus in Zhejiang Province, China, 2016–2018. Nutr Metab. 2021;18(1):12. PMID: 33468171; PMCID: PMC7814615. doi:10.1186/s12986-020-00539-8
43. Wang H, Chen L, Shen D, et al. Association of daytime napping in relation to risk of diabetes: evidence from a prospective study in Zhejiang, China. Nutr Metab. 2021;18(1):18. PMID: 33557863; PMCID: PMC7869458. doi:10.1186/s12986-021-00545-4
44. Zhang X, Chen X, Gong W. Type 2 diabetes mellitus and neighborhood deprivation index: a spatial analysis in Zhejiang, China. J Diabetes Investig. 2019;10(2):272–282. PMID: 30040249; PMCID: PMC6400165. doi:10.1111/jdi.12899
45. Yang A, Cheng N, Pu H, et al. Occupational metal exposures, smoking and risk of diabetes and prediabetes. Occup Med. 2017;67(3):217–223. PMID: 27418044; PMCID: PMC5927150. doi:10.1093/occmed/kqw078
46. Munkhaugen J, Hjelmesæth J, Otterstad JE, et al. Managing patients with prediabetes and type 2 diabetes after coronary events: individual tailoring needed-across-sectional study. BMC Cardiovasc Disord. 2018;18(1):160. PMID: 30075751; PMCID: PMC6091110. doi:10.1186/s12872-018-0896-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.