")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 15
The Prevalence and Significance of Fissured Tongue in Kabul City Among Dental Patients
Authors Ehsan H , Azimi S , Yosufi A , Yousufi R
Received 22 October 2022
Accepted for publication 14 February 2023
Published 23 February 2023 Volume 2023:15 Pages 21—29
DOI https://doi.org/10.2147/CCIDE.S391498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Video abstract presented by Hedayatullah Ehsan.
Views: 140
Hedayatullah Ehsan,1 Shamila Azimi,2 Abubakr Yosufi,2 Roqia Yousufi2
1Department of Oral Medicine, School of Stomatology, Kabul University of Medical Sciences, Ali-Abad University Hospital, Kabul, Afghanistan; 2Department of Oral Medicine, School of Stomatology, Kabul University of Medical Sciences, Kabul, Afghanistan
Correspondence: Hedayatullah Ehsan, Tel +93775816022, Email [email protected]
Background: The tongue is known as the mirror of oral and general health. Some diseases may show signs in the tongue. Fissured is approximately an asymptomatic condition characterized by grooves and fissures of varying depth on the dorsal surface of the tongue. Epidemiologically, its prevalence is varied based on different factors, but most of them report 10– 20%.
Methods: In the department of oral medicine at Ali-Abad University Hospital of Kabul University of Medical Sciences, a cross-sectional study was conducted among 400 patients. This fissured tongue is first diagnosed based on clinical appearance (fissures) on each side of tongue. Meanwhile, the whole medical and dental histories were taken for the rest of the leading factors.
Results: Out of 400 patients (124 males and 276 females) seen and checked, which 142 cases were fissured tongue [45 (31.7%) males and 97 (68.3%) females]. The fissures were found to be least in the > 10 – 19-year age group, 23 (16.3%) and it was most prevalent in the 20 − 39 age group, 73 (51.8%), followed by 40 − 59, 35 (24.8%) and 60< age group, 10 (7.1%). The most prevalent type of pattern of fissures was found to be superficial, multiple and not connected fissures, 46.32% (33.3% males, 32.3% females), followed by superficial, multiple and connected fissures, 25.5% (26.7% males, 25% females), and whereas 6.4% of patients with (single and deep type of fissure) was the lowest prevalent type of fissured tongue. In our study, more than half of patients asymptomatic (51.6% females and 71.1% males), 17.9% complained from tongue dryness, 14.3% soreness, 6.4% halitosis, 1.4% tongue swelling and 2.1% had all the signs.
Conclusion: The prevalence of fissured tongue was 35.5%. A significant difference between genders was reported with female predominance in all cases observed. The most prevalent age groups were 20– 29 and 30– 39 in both gender groups. Superficial, multiple, and not connected fissures 46.32% were the most common type of fissure.
Keywords: prevalence, tongue disorders, fissured tongue, oral diseases
Introduction
The tongue is known as the mirror of oral and general health. Some diseases may show signs in the tongue. Fissured tongue is an illness transferred from generation to generation and manifested with grooves in a tongue that can vary in depth.1 Fissured Tongue (lingua plicata; LP) is a disorder that manifests with multiple grooves or furrows on the dorsal surface of the tongue ranging from 2 to 6 mm in depth. Most reports in the literature indicate a prevalence of 10–20%, although there is marked variation.2 This condition is usually asymptomatic unless the debris is entrapped within the fissure. Patients may also be present with complaints of burning and soreness in the tongue. The mucosa of the dorsal surface of the tongue has filiform papillae, the hairs of which may shelter the superficial epithelial cells from mechanical stress.3
Even though this disorder mostly occurs on the dorsal surface of the tongue (Supplementary 1–5), but it can occur on lateral and ventral surfaces as well. It has different types like: long single-line fissure (Central longitudinal fissure), multiple lines fissure (Double fissure), continuous (Supplementary 2 and 3) and noncontinuous fissures (Supplementary 1 and 4). In most cases on dorsal surface there are loads of food particles or coated tongue.
Diagnosis of fissured tongue is based on clinical examination; biopsies are rarely taken. The tongue has to be protruded to unfold the fissures so that the fissures are visible.4 Variable range of prevalence rates has been reported in different parts of the world. A definite etiology does not exist, but a polygenic mode of inheritance is postulated. In general, fissured tongue occurs more frequently in males as compared to females5,6 and it increases with age in both genders.7,8 The aim of the present study was to determine the most prevalent pattern of fissured tongue and also to assess the possible association between the occurrence of fissured tongue with age, gender, systemic conditions. Meanwhile, this study tries to find the specific foods, which are triggers of fissured tongue and their oral hygiene condition that may lead to LP.
Objectives: 1. To determine the prevalence of fissured tongue abnormalities in relation to gender, and age and to assess the relationship of systemic diseases with this tongue abnormality among patients. 2. To assess the most prevalent pattern of fissured tongue in patients visiting a dental clinic.
Method and Materials
This study is a descriptive-analytic type based on examination and interview to gain data from 400 patients who were coming to Ali-Abad Dental Clinic aged 10–70 years with different oral diseases. All 400 patients were examined and interviewed for more than 3 months in the examination room of Ali-Abad Dental Clinic with the supervision of the oral medicine department. The data was collected through questionnaires, which consist of the following parts: demographic information and details regarding the medical history, smoking, spicy foods consumption, types of the fissured tongue, systemic problems, oral hygiene, prosthesis, and drug allergy.
Interviews and examinations of all patients for fissured tongue were done by senior students of dentistry faculty of Kabul University of medical sciences with patients’ consent. Their mouths and tongues were examined with a sterilized mouth mirror, explorer, and tweezer. Meanwhile, some of them were recorded for their severe condition of fissured tongues with taking pictures of their tongues as glossary.
Our team of research were willing to use the data, which recorded and documented via questionnaire for analyzation. So, for the analyzation we used SPSS software.
Results
Among the 400 people who were included in this research, 258 of them had normal tongue and 142 people had fissured tongue comprising 45 (31.7%) males and 97 (68.3%) females. Fissured tongue was most prevalent among the age groups of 20–29 years (29.8%) and 30–39 years (22%) in both genders. 43.2% (60) patients were aware of the fissure existence on their tongues surfaces and 56.8% were not (Table 1).
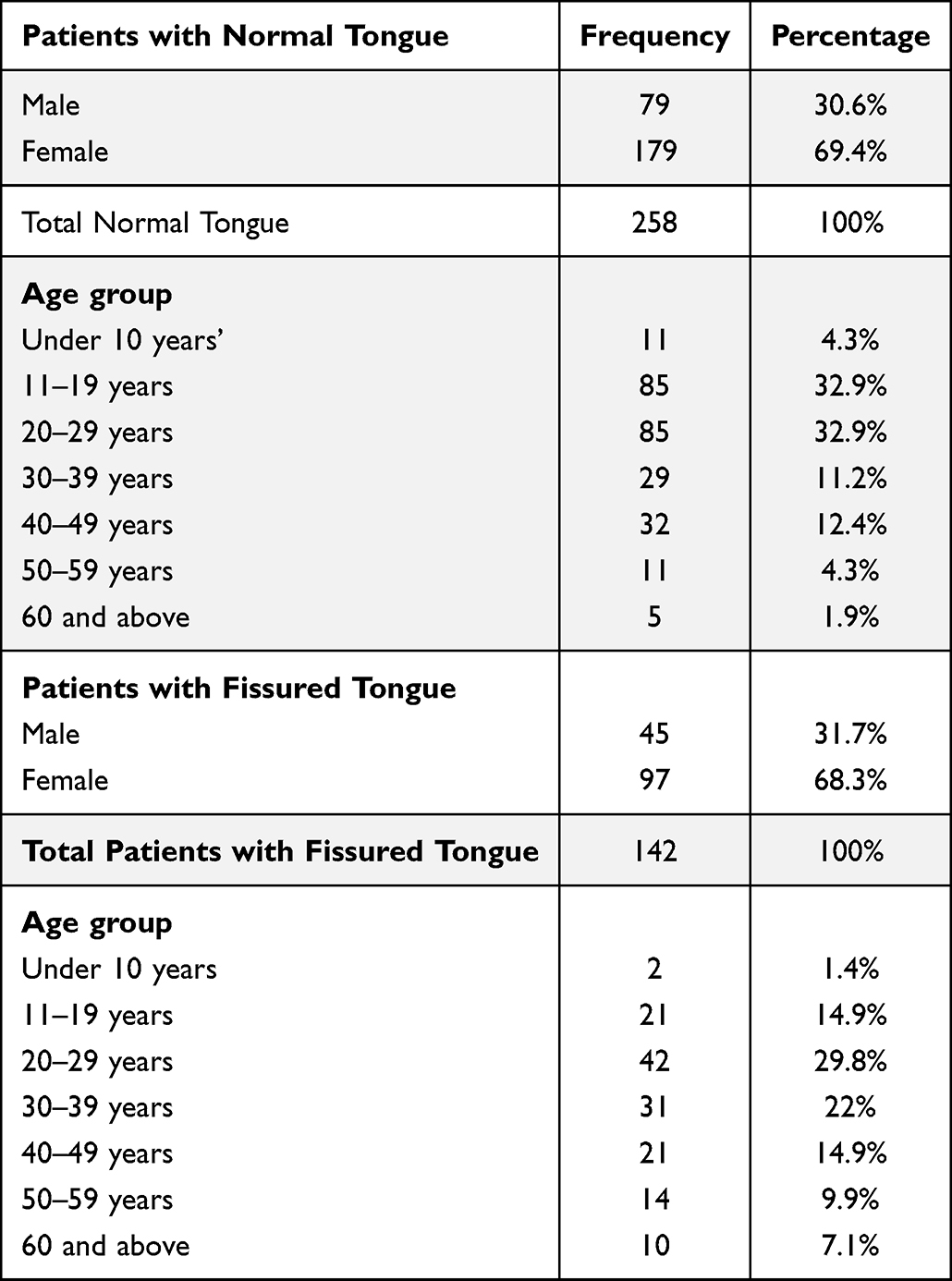 |
Table 1 Frequencies of Normal and Fissured Tongue Among Study’s Population |
Overall, 46.32% of patients (33.3% males, 32.3% females) had (superficial, multiple and not connected fissures) (Figure 1) (Supplementary 1) which makes it the most common type of fissured tongue. 25.5% of the cases (26.7% males, 25% females) were presented with (superficial, multiple and connected fissures) (Figure 2) (Supplementary 2) which makes it the second most prevalent type of fissured tongue. Whereas 6.4% of patients with (single and deep type of fissure) (Figures 3 and 4) was the lowest prevalent type of fissured tongue (Table 2).
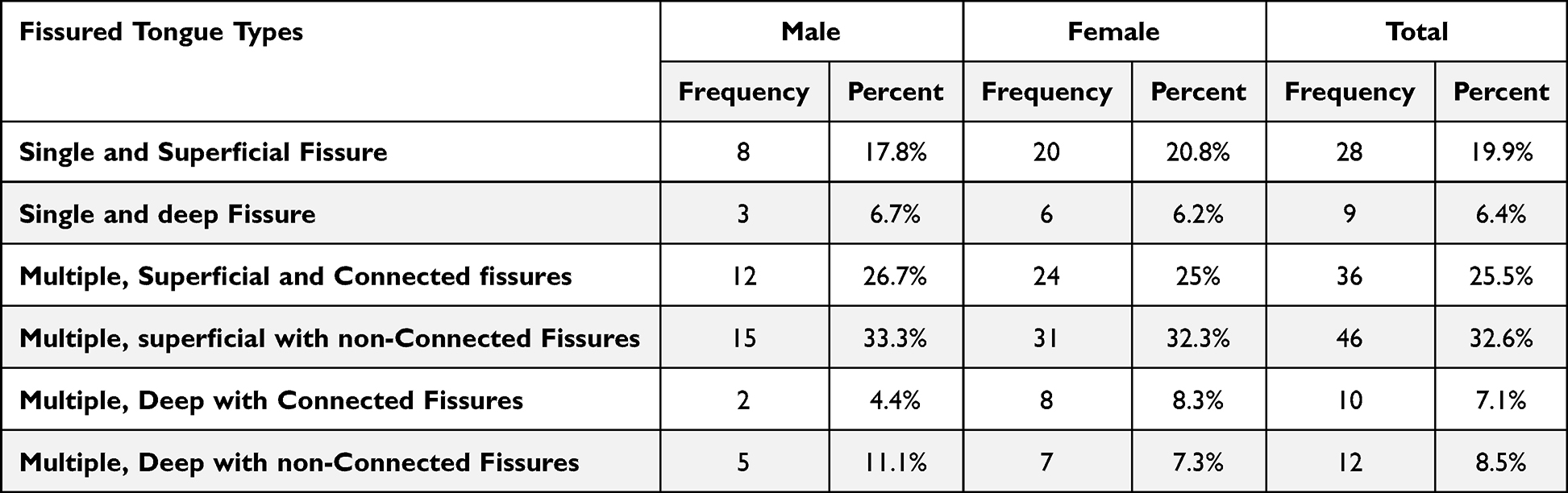 |
Table 2 Frequencies and Percentage of Different Types of Fissured Tongue |
 |
Figure 1 Superficial, multiple and non-connected fissures. |
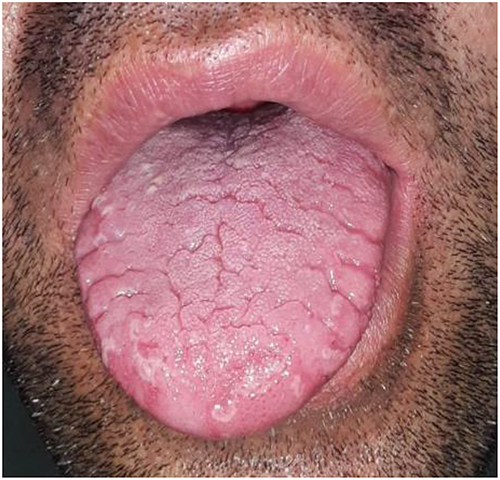 |
Figure 2 Superficial, multiple and connected fissures with geographic appearance. |
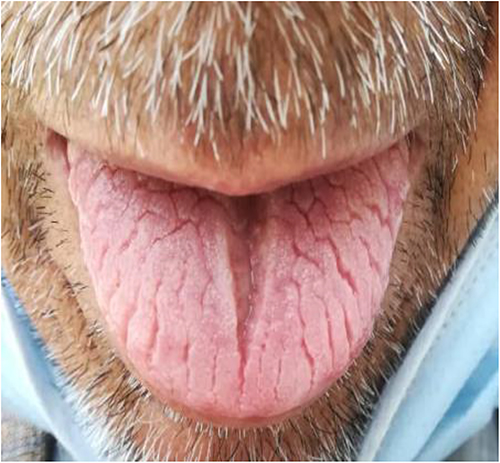 |
Figure 3 Deep fissures. |
 |
Figure 4 Single and superficial fissure. |
According to affected area of tongue, 75.9% (107) of fissures were on the dorsal surface (Supplementary 1–4), 18.4% (26) had fissure on both (lateral and dorsal) part of the tongue and 5.7% (8) were in lateral part of the tongue. As reported in Table 3, 48.9% fissures were permanent, 10.8% fissures were temporary and 40.3% of patients did not know whether the fissures were permanent or temporary.
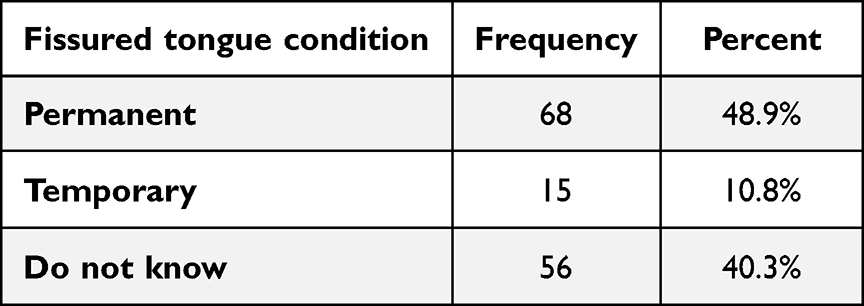 |
Table 3 Frequency and Percentage of Fissured Tongue Conditions |
2.8% (4) of patients had geographic tongue (Figures 2 and 5) (Supplementary 1), 14.9% (21) of patients with fissured tongue at the same time had coated tongue (Figure 6) (Supplementary 4), and 81.6% (115) had no any other abnormality on their tongue except the fissures.
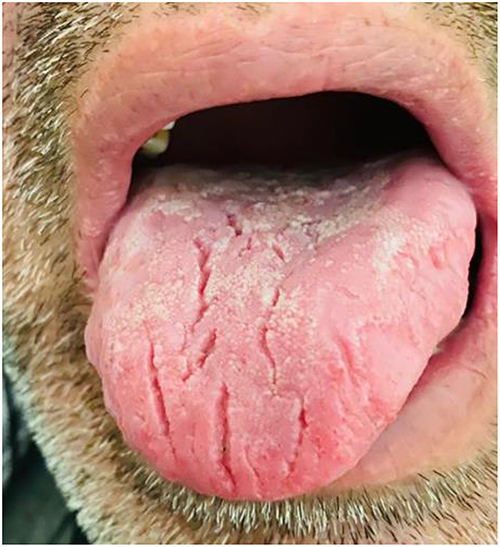 |
Figure 5 Coated tongue with non-connected fissures. |
 |
Figure 6 Geographic tongue. |
More than half of patients did not have complains of any sign (51.6% females and 71.1% males), 17.9% complained from tongue dryness, 14.3% soreness, 6.4% halitosis, 1.4% tongue swelling and 2.1% had all the signs. 14.3% of all patients were dental prosthesis users.
37.1% (54) of patients with fissured tongues had one or more systemic diseases including 27.1% with the gastroesophageal disease, 5% with diabetes, 3.6% with hypertension, mental and blood problems.
27.9% (39) of patients answered YES when asked whether specific foods cause fissures burning or irritation and 71.1% (101) of answers were NO. Eggplant, walnut, melon, pepper, lemon, spinach, date, chips, and tomato were the most irritants.
22.2% of male’s patients were smokers, 22.2% were consumed beverages in higher amounts and 13.3% consumed acidic foods. 42.2% had no harmful habit. 35.8% used to consumed more acidic foods, 8.9% using beverages and 55.8% of females had no habit. 28.6% were used to brush their tongue and 70.4% were not (Table 4).
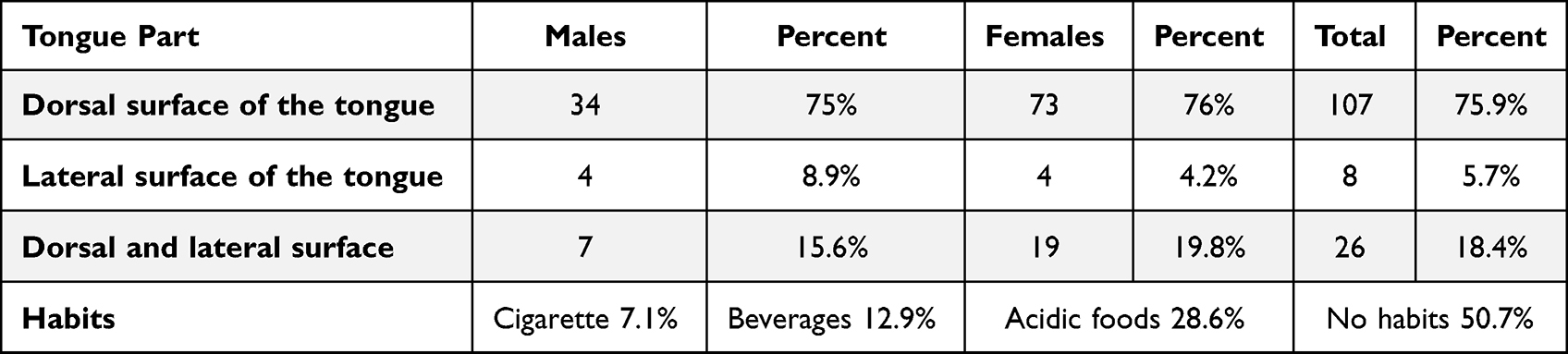 |
Table 4 Frequencies of fissures on different surfaces of tongue |
Discussion
It is obvious that all kinds of lesions on different parts of the tongue have different origins and causes but can be a sign of systemic medical conditions like hypertension, hematological problems (Supplementary 6), diabetes (Supplementary 7), digestive disorders, and psychological effects. Meanwhile, other leading factors can cause these lesions as well like smoking, xerostomia, poor oral hygiene, some specific foods especially spicy foods, and some medications as their side effects these findings of our study slightly match with the findings of the study of Mistretta CM and Kumari A.9
Among lesions of tongue, fissured tongue is an asymptomatic sign and not malignant condition, which prevalent in most people of world. Albeit, most previous studies reported that this condition has no any symptoms, but we found some related symptoms and signs like; More than half of participants not complains of any sign (51.6% females and 71.1% males), 17.9% complain from tongue dryness, 14.3% soreness, 6.4% halitosis, 1.4% tongue swelling and 2.1% had all signs. Based on different studies it has shown that this condition does not have specific factor but it can be a multifactorial or unknown condition, which different factors can be involved in including hereditary as well.4 Its distribution among age groups, sex groups, and parts of tongue are varying.
The prevalence of fissured tongue is different based on the differences in ethnicity, age, race, region, sex, different examination criteria by examiners, and different types of studies which are done by researchers. All these variations in its prevalence are shown according to published studies in different regions of the world. In this study, the prevalence of fissured tongue is 35.5%, which is approximately similar to the study of Dos Santos et al10 in Brazil (27.3%) and the study of Byahatti and Ingafou among Lybian adults (48.4%).12 But there are also several other studies in which the prevalence of fissured tongue them are lower than our study. The research report of Khozeimeh and Rasti shows an 11.8% prevalence of fissured tongue among Iranian people.11 The same finding in an Indian study which was conducted by Mathew et al in 2017, was 13% among the 500 south Indian population.12
According to various age groups, the fissured tongue had a slightly more prevalence among the age groups of 20–29 years (29.8%) and 30–39 years (22%) compared to the low prevalence among the 10–19-year (14.9%) age group. Meanwhile, our findings closely catch up with the findings of the Bhat et al study which the prevalence of fissured tongue among the age group of 21–40 years was 37.0% and the 0–20-year age group was 4%.13 Another study by Mathew et al12 with the same findings reported that among the 10–20-year age group the fissures are least (3%), while the prevalence of it in the 21–40-year age group is so high (38.46%). It is evident and clear based on these studies that by increasing age the prevalence of fissures is also going high which recommends that in elder and adult people the immune system’s response is coming to reduce, xerostomia due to salivary hypofunction, mineral and vitamin deficiencies, atrophy of oral tissues and oral different infectious diseases like candidiasis are all the triggers of the fissured tongue.
In our study, the prevalence of fissured tongue among women (68.3%) was higher than among men (31.7%) which is similar findings of Darwazeh and Almelaih.14 Additionally, other studies15,16 found the same result that females were more affected. While other studies have challenged our findings like Kelsch et al17 and Patil et al.6
The location of fissures can be different, but dorsal and lateral surfaces of tongue are the most influenced areas of fissures.18 Based on our study, 75.9% fissures located on the dorsal surface, 18.4% had fissure on both (lateral and dorsal) part of the tongue and 5.7% lateral part of the tongue.
Among the systemic diseases, diabetes mellitus and hypertension are frequently reported with fissured tongue. In a study by Mathew Al, 10.8% and 20% of fissure tongue cases were found in patients with hypertension and diabetes mellitus respectively. In another study by Maloth et al, 22% and 19.5% of fissured tongue cases were observed in patients with diabetes and hypertension. Whereas in our study, we found only 5% and 3.6% of fissure tongue patients had diabetes mellitus and hypertension, respectively.
Our study found that 22.2% of male patients were smokers. Our study is in contrast with the studies by Maloth et al and Mathew AL who reported 4.5% and 1.1% of fissure tongue patients having a bad habit of smoking and consuming tobacco.
Conclusion
The prevalence of fissured tongue was 35.5%. A significant difference between genders was reported with female predominance in all cases observed. The most prevalent age groups were 20–29 and 30–39 in both gender groups. Superficial, multiple, and not connected fissures 46.32% were the most common type of fissure. 43.2% of patients were aware of the fissure existence on their tongue surface and 56.8% were not aware. Meanwhile, regarding medical conditions, the most significant relationship of the fissured tongue with systemic diseases, based on our study has shown that most patients with gastrointestinal diseases have this kind of tongue. Not only gastrointestinal diseases, but other medical conditions have a relationship with this type of tongue; diabetes mellitus, hypertension, digestive disorders, and psychological problems.
Ethics and Informed Consent Statements
Prior to the start this study, the research protocol (proposal in local language) was submitted for review to research ethics committee of Kabul University of Medical Sciences. This committee usually consists of qualified experts from different faculties including curative medicine, dentistry, public health, midwifery, and nursing who transparently provide comment, guidance, and approval of research. This study was supervised and confirmed based on the ethical principles (10 specific principles of Helsinki; scientific requirements and research protocols, informed consent, privacy and confidentiality, research registration and publications, and so on) of this committee. All data of this study in conjunction with the participants’ informed consent are stored for ethical issues with this committee.
Acknowledgment
The authors are extremely grateful to the completion of our study would not have been possible without the support and nurturing of our research mentors (Prof. Razia Rabizada, MD and Assistant Prof. Tamana Barakaty, MD, MsCs) for guiding us.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Zargari O. The prevalence and significance of fissured tongue and geographical tongue in psoriatic patients. Clin Exp Dermatol. 2006;31(2):192–195. doi:10.1111/j.1365-2230.2005.02028.x
2. Feil ND, Filippi A. Frequency of fissured tongue (lingua plicata) as a function of age. Swiss Dent J. 2016;126(10):886–897.
3. Kullaa‐mikkonen AR, Tenovuo J, Sorvari T. Changes in composition of whole saliva in patients with fissured tongue. Eur J Oral Sci. 1985;93(6):522–528. doi:10.1111/j.1600-0722.1985.tb01350.x
4. Silverman S, Eversole LR, Truelove EL. Essentials of oral medicine (1st edn). PMPH. 2001;2001:252–259.
5. Darwazeh AM, Almelaih AA. Tongue lesions in a Jordanian population. Prevalence, symptoms, subject’s knowledge and treatment provided; 2011. Available from: http://hdl.handle.net/10550/60090.
6. Patil S, Kaswan S, Rahman F, Doni B. Prevalence of tongue lesions in the Indian population. J Clin Exp Dent. 2013;5(3):e128. doi:10.4317/jced.51102
7. Järvinen J, Mikkonen JJ, Kullaa AM. Fissured tongue: a sign of tongue edema. Med Hypotheses. 2014;82(6):709–712. doi:10.1016/j.mehy.2014.03.010
8. Reichart PA. Oral mucosal lesions in a representative cross‐sectional study of aging Germans. Community Dent Oral Epidemiol. 2000;28(5):390–398. doi:10.1034/j.1600-0528.2000.028005390.x
9. Mistretta CM, Kumari A. Tongue and taste organ biology and function: homeostasis maintained by hedgehog signaling. Annu Rev Physiol. 2017;79:335. doi:10.1146/annurev-physiol-022516-034202
10. Dos Santos PJB, Bessa CFN, De Aguiar MCF, Do Carmo MAV. Cross‐sectional study of oral mucosal conditions among a central Amazonian Indian community, Brazil. J Oral Pathol Med. 2004;33(1):7–12. doi:10.1111/j.1600-0714.2004.00003.x
11. Khozeymeh F, Rasti A. The Prevalence of Tongue Abnormalities Among the School Children in Borazjan, Iran. DRJ; 2006.
12. Mathew A, Cherian S, Daniel M, Abraham T, Mathew R. Prevalence of fissured tongue in a South Indian population-A cross-sectional study. J Oral Med. 2017;1(1):9.
13. Bhat Z, Hamid R, Wani B, Chalkoo A. Fissured tongue: a cross-sectional study. Int J Appl Dent Sci. 2018;4:133–135.
14. Darwazeh AM, Almelaih AA. Tongue lesions in a Jordanian population. Prevalence, symptoms, subject’s knowledge and treatment provided; 2011. Available from: http://www.medicinaoral.com/medoralfree01/v16i6/medoralv16i6p745.pdf.
15. Vieira-Andrade RG, Zuquim Guimarães FDF, Vieira CDS, Freire STC, Ramos-Jorge ML, Fernandes AM. Oral mucosa alterations in a socioeconomically deprived region: prevalence and associated factors. Braz Oral Res. 2011;25:393–400. doi:10.1590/S1806-83242011000500004
16. Bánóczy J, Rigó O, Albrecht M. Prevalence study of tongue lesions in a Hungarian population. Community Dent Oral Epidemiol. 1993;21(4):224–226. doi:10.1111/j.1600-0528.1993.tb00761.x
17. Kelsch RD, James WD, Ortonne JP, et al. Fissured tongue. Medscape Reference; 2014.
18. Sudarshan R, Sree Vijayabala G, Samata Y, Ravikiran A. Newer classification system for fissured tongue: an epidemiological approach. J Trop Med. 2015;2015:1–5. doi:10.1155/2015/262079
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.