")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
The Predictive Value of Midscalp Hair Density and Terminal Hair Percentage in the Severity Evaluation of FPHL Assessed by Trichoscan in a Sample of Chinese Population
Authors Yang X , Yu W, Qiao R, Sun J, Jiang Y
Received 24 September 2022
Accepted for publication 7 December 2022
Published 13 December 2022 Volume 2022:15 Pages 2675—2684
DOI https://doi.org/10.2147/CCID.S390148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Xianhong Yang,1,* Wanting Yu,2,* Rui Qiao,1 Jianfang Sun,1 Yiqun Jiang1
1Department of Dermatopathology, Hospital for Skin Diseases, Institute of Dermatology, Chinese Academy of Medical Sciences & Peking Union Medical College, Nanjing, People’s Republic of China; 2Department of Dermatology, Hangzhou Third Hospital Affiliated to Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yiqun Jiang, Email [email protected]
Background: Female pattern hair loss (FPHL) is the most common hair loss disorder in women, which may impair patient’s self-identity. It presents as a diffuse reduction in hair density at the mid and frontal regions of the scalp with preservation of the frontal hairline. TrichoScan can be used as a diagnostic tool and for monitoring patients in male pattern hair loss, but little is known in FPHL with Chinese population.
Objective: To explore the predictive value of various TrichoScan characteristics at different areas of the scalp in the diagnosis and evaluation of FPHL.
Materials and Methods: A total of 261 FPHL subjects were divided into three groups according to Ludwig classification. Together with 108 healthy controls, they were evaluated by computer-assisted TrichoScan. Various hair parameters were analyzed in the frontal, midscalp, vertex, parietal, and occipital areas of the scalp.
Results: Declining hair densities, terminal hair percentage, hair follicular unit density, mean hair diameter, and average hair/unit combined with increased intermediate hair percentage, and vellus hair percentage were observed across all areas of the scalp for FPHL subjects. Hair density and terminal hair percentage in the midscalp area were the factors most affecting Ludwig classification. The two parameters combined achieved 85.12% correct classification rate and an area under the ROC curve of 0.88 in the diagnosis of FPHL. Additionally, we reported a unique type of FPHL which mostly affected the parietal area, occurring with or without traditional midline changes.
Conclusion: FPHL in a Chinese population presented characteristics of reduced hair density and miniaturization of hair follicles in the midline scalp and to a lesser extent in the parietal area. Hair density and terminal hair percentage in the midscalp exhibited the greatest predictive value of Ludwig classification. Our results may further provide the basis for quantitative classification of FPHL.
Keywords: FPHL, TrichoScan, hair density, terminal/intermediate/vellus hair percentage, Ludwig classification, predictive value, parietal area hair loss
Introduction
Hair plays an important role in body image and self-identity for women, though it has a more social and psychological significance than biological relevance. Female pattern hair loss (FPHL) is the most common hair loss disorder in women.1 Studies in women of white European ethnicity in the USA, UK and Australia record a prevalence of 3–12% in the third decade of life, rising to 14–28% in the sixth decade. Reported prevalence rates in East Asian women are lower, reaching 12–25% in the over 70 group. As such, the overall prevalence of FPHL in Chinese women was 3.1%.2
FPHL typically presents as a diffuse reduction in hair density at the mid and frontal regions of the scalp with preservation of the frontal hairline.3,4 It may present with three different patterns:5 (1) diffuse thinning of the crown region with preservation of the frontal hairline (two scales are used to describe this: the 3-point Ludwig scale6 and the 5-point Sinclair scale7); (2) thinning and widening of the central part of the scalp with breach of frontal hairline (described by the Olsen scale: Christmas tree pattern8); and (3) thinning associated with bitemporal recession (described by the Hamilton-Norwood scale).9 Ludwig classification is the most widely used hair loss classification system, divided into three degrees: Ludwig I – lighter form with thinning on the top of the head; Ludwig II – moderate form; and Ludwig III – severe form.6,10
Accurate and consistent Ludwig classification is not always obtained in the clinic since the classification system requires skilled experience and is not the most sensitive for treatment assessment. A more quantitative scoring system is thus needed. TrichoScan is a system that combines epiluminescence microscopy and automated digital image analysis. It allows the estimation of the number and density of hairs, the percentage of terminal and vellus hairs, and the percentage of hairs in the anagen and telogen phases by mathematical approximation. TrichoScan can be used as a diagnostic tool and for monitoring patients in hair loss treatment.10,11
In this study, we aimed to evaluate the hair parameters of FPHL at different scalp areas compared to healthy controls, evaluating the diagnostic assessment value of TrichoScan in FPHL. Additionally, we explored the characteristics of a unique type of FPHL, which presented hair loss predominantly in the parietal areas mentioned by Rohirunsakool and Suchionwanit (2018).12
Subjects and Methods
Subjects
A total of 261 subjects diagnosed by three experienced dermatologists with FPHL according to Ludwig classification and 108 healthy female controls without androgenetic alopecia were recruited to participate in the study between August 2020 and April 2021 at the Institute of Dermatology, Chinese Academy of Medical Sciences (Figure 1). Excluding criterion included chronic dermatologic conditions of the scalp; other types of hair loss, including acute telogen effluvium, were excluded by medical history, clinical examination and, where necessary, by relevant clinical tests such as complete blood count, iron, total iron-binding capacity, ferritin, thyroid hormones and antinuclear antibody titres.
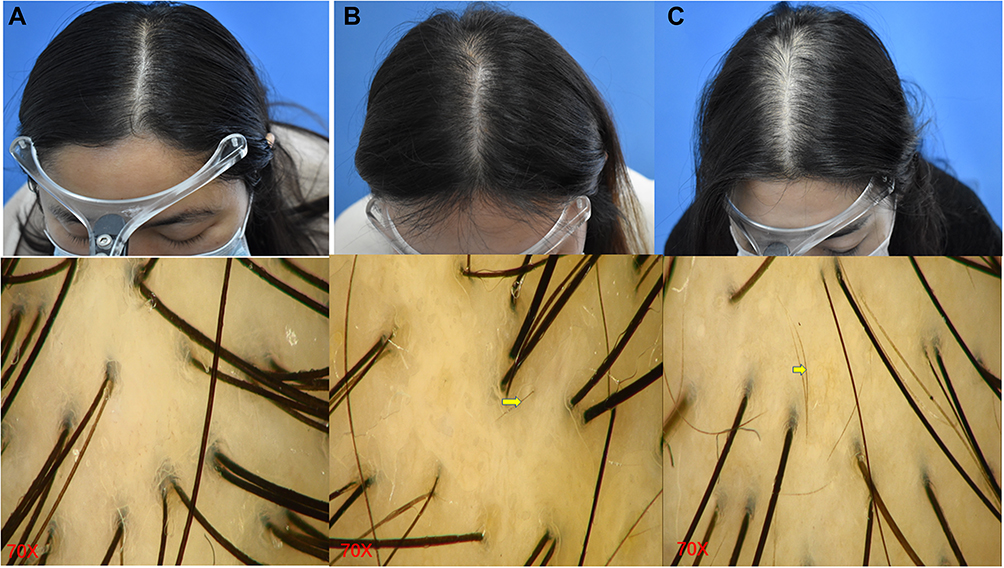 |
Figure 1 Hair images taken by camera and TrichoScan at 70X magnification for FPHL subjects and healthy controls. ((A) Healthy controls; (B) subjects of Ludwig I; (C) subjects of Ludwig II; yellow arrow shows vellus hair). |
Written informed consent was obtained from all participants, and the study protocol was approved by the ethical committees of Institute of Dermatology, Chinese Academy of Medical Sciences. Participants under 18 years of age in the control group required parental informed consent to participate.
Methods
Five different areas of each subject’s scalp were evaluated (Figure 2). Three sites on the scalp were then measured at 12, 24, and 30 cm from the glabella, similar to Kanchana et al’s study, which were identified as the frontal, vertex, and occipital area.13 The midscalp area was an imaginary line between the left and right external auditory ear canals. The parietal area was the area 7 cm above both external auditory ear canals.12 Trichoscopic pictures were taken by TrichoScan (FotoFinder Bodystudio ATBM, Germany) at these five sites. All hair parameters were evaluated, including hair density (hair number in 1cm2 area), terminal hair percentage (hair diameter >0.06mm), intermediate hair percentage (0.03mm < hair diameter ≤ 0.06mm), vellus hair percentage (hair diameter ≤0.03mm), hair follicular unit density, mean hair diameter, and average hair/unit. All hair parameters were analyzed at 70-fold magnification, and images were analyzed by a combination of manual labeling and computer assisted counting (Figure 1). All hair parameters were evaluated three times, independently, to calculate average scores.
 |
Figure 2 Marked points (red dot) at different scalp areas. (A) Green arrow shows frontal area, blue arrow shows midscalp area and yellow arrow shows vertex area. (B) Parietal area; (C) occipital area. |
Statistical Analysis
The statistical software package SPSS version 23 (IBM Inc, Armonk, New York) was used for all analyses. Different parameters were compared across groups by one-way analysis of variance (ANOVA). Logistic analysis, prediction and the Confusion matrix were performed by stataSE64. Data were showed as mean ± standard deviation (SD). P-value <0.05 denoted a statistically significant difference.
Results
Demographic Characteristics
A total of 261 FPHL subjects with a mean age of 30.4±7.83 (ranged 18–62 years old) and 108 healthy female controls with a mean age of 31.9±10.18 (ranged 16–58 years old) were recruited to participate in the study. The FPHL subjects were divided into three groups according to Ludwig classification, including 182 in Ludwig I, 74 in Ludwig II, and 5 in Ludwig III (Table 1). Ludwig III females were excluded from further analysis due to small sample size.
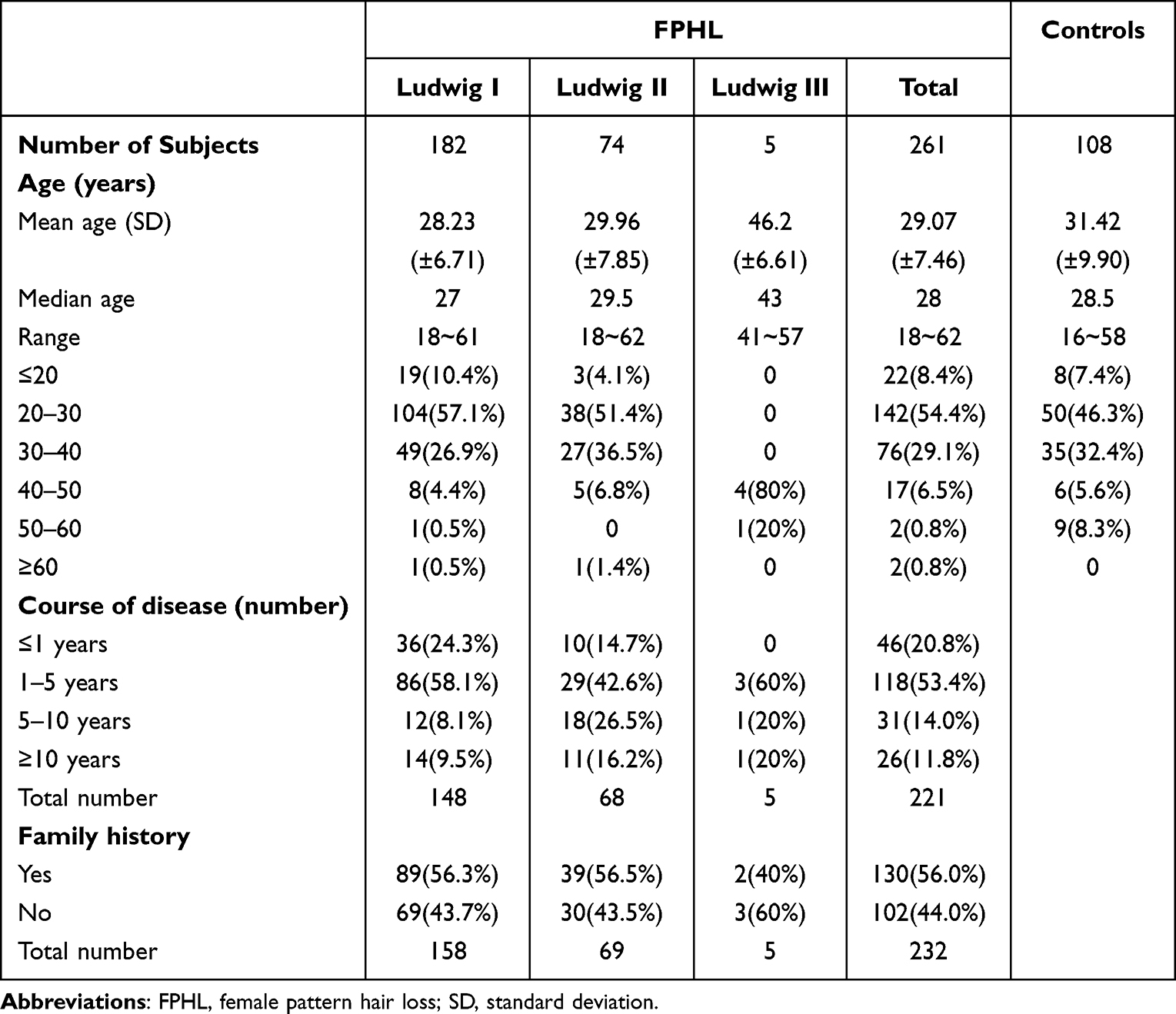 |
Table 1 Demographic Characteristics of FPHL Subjects and Healthy Controls |
The total number of FPHL subjects was 261, with 232 of these recording a family history of FPHL, other 29 participants did not record (Table 1). Participants in the Ludwig I group (n = 158) included 89 (56.3%) which reported a family history of FPHL, while the remaining 69 (43.7%) did not. Of the 69 participants in the Ludwig II group, 39 (56.5%) reported a family history of FPHL with the remaining 30 (43.5%) did not. There was no statistically significant differences between the groups (P > 0.05).
Hair Parameters at Different Scalp Regions in FPHL Subjects and Normal Controls
Hair Density
Hair density of different scalp sites at distinct clinical stages is shown in Figure 3A and described in Table 2. Hair density in 108 healthy females demonstrated clear regional differences. Specifically, the midscalp area presented the highest hair density, followed by vertex, occipital, and frontal regions, while the parietal area observed the lowest density. When comparing mean hair density between Ludwig classification groups and healthy controls, all five scalp areas displayed a tendency toward decreasing hair density with increased severity of FPHL stage. Statistically significant differences were detected for Ludwig I (p < 0.001) and Ludwig II (p < 0.001) groups across all five areas.
 |
Table 2 Comparison of Hair Parameters in Different Scalp Areas Between FPHL Subjects and Healthy Female Controls |
 |
Figure 3 The hair density, terminal hair percentage and vellus hair percentage of FPHL subjects and healthy controls across different scalp areas. (A) Compared with healthy controls, hair density presented decreasing tendency with improving severity of FPHL stage. (B) Compared with healthy controls, all the scalp sites except for frontal showed a tendency of decreasing terminal hair percentage with higher Ludwig stage. (C) Compared with healthy controls, vellus hair percentage showed a positive correlation with increased Ludwig classification at all areas except for the frontal region. (** represented P < 0.01, Ludwig I or Ludwig II VS normal controls at the same scalp area). |
Hair Percentage (Terminal/Intermediate/Vellus)
The highest terminal hair percentage in normal females was observed at the occipital site, followed by the vertex, midscalp, and parietal areas Figure 3B. Compared to controls, the midscalp, vertex, occipital and parietal sites demonstrated statistically significant decreases in terminal hair percentage for Ludwig I participants (p < 0.05), with enhanced decreases seen in Ludwig II participants (p < 0.001). On the other hand, decreased terminal hair percentage in the frontal scalp area was only detected in Ludwig II females (p < 0.01).
Intermediate hair percentages in normal controls were highest in the frontal site and lowest in the occipital site (Supplementary 1A). Compared with normal controls, midscalp, vertex, and occipital areas showed statistically significant increases of the middle hair percentage in both Ludwig I (p < 0.001) and Ludwig II (p < 0.001) groups. Frontal and parietal sites only displayed significant increases in the Ludwig II group (p = 0.04, p < 0.001).
Controls observed the highest vellus hair percentage in the frontal area, followed by the temporal, midscalp, and vertex regions. In contrast, the occipital site showed the lowest (Figure 3C). Vellus hair percentage showed an increasing tendency in parallel with advancing Ludwig classification at all areas except for the frontal region. The midscalp and vertex showed statistically significant increases in the vellus hair percentage for Ludwig I (p < 0.001) and Ludwig II (p < 0.001) groups. The parietal region showed similar significant increases for Ludwig I (p = 0.01) and Ludwig II (P < 0.001) groups. On the other hand, the occipital site only demonstrated statistically significant increases in vellus hair percentage in the Ludwig II (P < 0.001) group.
Mean Hair Diameter
The vertex site had the highest mean hair diameter, followed by the occipital, midscalp, parietal and frontal area in normal control group (Supplementary 1B). Mean hair diameter in all areas of the scalp (except for frontal) tended to decrease as the severity of Ludwig classification increased. When comparing the normal group against each Ludwig stage, the midscalp, vertex and occipital regions showed significantly lower mean hair diameters in Ludwig I (P < 0.001) and Ludwig II (P < 0.001) groups. Similarly, the parietal area saw significant differences in Ludwig I (P = 0.01) and Ludwig II (P < 0.001) groups. Mean hair diameters on the frontal area were the lowest in the Ludwig I (P = 0.02) group.
Hair Follicular Unit Density
In the normal controls, the frontal area observed the highest hair follicular unit density, followed by the midscalp, vertex, parietal and occipital regions (Supplementary 1C). The frontal, midscalp and occipital sites demonstrated significant decreases in hair follicular unit density in both the Ludwig I (p < 0.01) and Ludwig II (p < 0.01) groups. Meanwhile, the vertex region only observed this pattern in the Ludwig I (P = 0.01) group and the parietal region in the Ludwig II (P = 0.03) group.
Average Hair/Unit
Control participants observed the highest average hair/unit at the occipital site followed by the vertex, midscalp, parietal and frontal regions (Supplementary 1D). Compared to controls, FPHL cases demonstrated lower average hair/unit across the vertex and midscalp in Ludwig I (P < 0.001) and Ludwig II (P < 0.001) groups, demonstrating a severity-based decline. On the occipital site, significant differences in average hair/unit were found only in Ludwig II (P = 0.003) group.
Hair Parameters in the Parietal Region Seriously Affected FPHL Patients
A total of 15 FPHL subjects in this study presented characteristics of seriously affected parietal area hair loss compared to conventional FPHL patients, which presented most hair loss in the frontal and vertex areas (Figure 4). This small sub-group consisted of all three Ludwig classifications, with Ludwig I, II, and III comprised of 9, 5, and 1 subject, respectively. The mean age in this sub-group was 30.67 years with SD 7.5 (Supplementary 2).
 |
Figure 4 Clinical images in FPHL subjects with parietal area seriously affected. (A) Left lateral view; (B) right lateral view; yellow arrows show sparse hairs in parietal areas. |
Hair parameters across different scalp regions for parietal area seriously affected FPHL subjects are summarized in Table 3. Hair density decreased on all five scalp sites in this group compared to normal controls (P < 0.01). Terminal hair rate decreased in this group, while middle hair rate and vellus hair rate increased across all five scalp sites compared with normal controls. The regional differences observed in hair densities, terminal/intermediate/vellus hair percentage, were more severe than differences observed in the Ludwig I (P < 0.05) group, while similar to but less severe than Ludwig II (P > 0.05) characteristics. The mean hair diameter in vertex, parietal and occipital areas of the parietal area seriously affected subgroup fell somewhere between the Ludwig I and Ludwig II parameters.
 |
Table 3 Comparison of Hair Parameters in the Parietal Region Seriously Affected FPHL Patients with Healthy Controls |
Predictive Value of Hair Density and Terminal Hair Percentage in the Midscalp
Multi-Logistic Regression
We have collected data including age, family history, disease course and all potentially relevant hair parameters. All 38 variables were considered in order to find the appropriate subsets which contains variables that strike a balance between the number of variables and the performance of fitting. After some experiments by multi-logistic regression, we determined that hair density and the terminal hair rate in the midscalp were the optimum candidates. With the estimated coefficients of the multi-logistic model (Supplementary 3), the model correctly predicted (73+147+44)/364 = 72.5% of cases among the Ludwig I, Ludwig II classifications, as well as healthy controls (Supplementary 4).
Next, we ran a 10-fold cross validation to deal with potential overfitting and make use of the entire data set. After 10-fold cross validation, the model correctly predicted (73+143+39)/364 = 70.1% of classes, only slightly lower than the previous rate of 72.5% (Supplementary 5). This demonstrates that the model is very robust in predicting class assignment.
Binary Response
We combined the two Ludwig classes (I and II) into one category, creating a binary classification. Subsequently, we fit a logistic regression model to run the prediction. The estimated coefficients for hair density and terminal hair rate in the midscalp are shown in Supplementary 6. The two parameters can achieve 85.12% correctly classified rate, with area under the ROC curve of 0.88 in the binary classification of FPHL (Figure 5) (Supplementary 7).
 |
Figure 5 The ROC curve and area under ROC curve of Binary classification in FPHL. |
Discussion
In our study, a total of 261 FPHL subjects were included with 182 in Ludwig I and 74 in Ludwig II. Only 5 cases showed severe sign of Ludwig III, which were excluded in the next study because of small number. This result was in keeping with characteristics of Japanese women and another report of southern Chinese women.14,15 The most affected age group of FPHL patients in our study came from 20~40 years old. This result seems to conflict with previous reports that the incidence of FPLH steadily increased with age across all ethnicities.16 In general, FPHL onset presents during the reproductive years. The second peak incidence typically occurs at menopause, between 50 and 60 years of age. However, increasing evidence suggests the incidence of severe cases may become noticeable as early as puberty. The potential effects of the large number of 20–40 years old patients may be due to greater demand for treatment among patients aged 25–40 years.10,17 Additionally, Silke et al4 have reported that the locus of AR/EDA2R in FPHL may represent a common genetic factor for early-onset FPHL.
Genetic susceptibility can influence the development of male androgenetic alopecia, but relatively little is known regarding the genetic basis and inheritance pattern of FPHL.3 An Australian gene-wide association study of white women suggested that the aromatase gene (CYP19A1) may contribute to FPHL.18 The CYP19A1 gene encodes the enzyme aromatase, responsible for the conversion of androgens to oestrogens, thus regulating the balance of sex steroid hormone levels in hair follicles.19 While multiple genes may contribute to the susceptibility of FPHL,3 no definitive familial inheritance pattern has been identified.
Our study also demonstrated that FPHL patients presented with decreased hair density, mean hair diameter, terminal hair percentage and increased intermediate hair percentage and vellus hair percentage. Moreover, their parameters were positively correlated with the severity of clinical Ludwig staging. The biological cycle of the hair follicles is divided into three phases: anagen (growth phase), catagen (regression) and telogen (resting phase). This process is not synchronized among the adjacent units, assuming a mosaic pattern in the scalp.20 Around 80–90% of hair is expressed in the anagen phase, 10–20% in the telogen phase and 1–2% in the catagen phase in normal adult scalps. FPHL patients observe a reduction in the duration of the anagen phase and a delay between the end and start of a new anagen phase.21 Additionally, FPHL patients experience gradual decreases in capillary density and follicle miniaturization in affected areas.10 The altered hair follicle cycling and miniaturization of hair follicles lead to the transformation from terminal to vellus hair follicles.22
Our results confirmed that the entire scalp is involved in the progression of FPHL patients, but the most affected areas were the midscalp, followed by the vertex, consistent with previously published reports.12,14,23 One hypothesis for regional hair loss differences in FPHL is the variable embryonal derivation of the scalp regions. The dermis of the frontal and parietal scalp is of neural crest origin, while that of the occipital scalp is of mesodermal origin.24,25 Follicular units from different regions of the scalp vary in their susceptibility to undergo terminal to vellus hair transformation, leading to macroscopic and microscopic patterns of hair loss, respectively.26
In our observation, there were a small quantity of FPHL patients who presented with serious hair loss in the parietal area. The hair parameters presented were somewhere between Ludwig I and Ludwig II (but closer to Ludwig II). The pathophysiology of this special FPHL subgroup may have some relationship with the increased 5α-reductase enzyme in this area compared to other scalp sites. Similar mechanisms occurring in the frontal scalp have been described before.12,27 However, the exact mechanism is not entirely clear and more research must be carried out to clarify the pathogenesis.
Multi-logistic regression showed that hair density and terminal hair percentage in the midscalp area obtained best predictive accuracy of Ludwig classification of FPHL. This was in accordance with the clinical manifestation and pathophysiological aspect of FPHL. The Ludwig rating system bears limitations to precisely classifying intermediate stages. By combining dermoscopic and TrichoScan parameters, we correctly classified FPHL more precisely regardless of regions and patterns. The binary classification using hair density and terminal hair percentage in the midscalp area particularly can help clinicians identify early-onset FPHL patients and assign timely treatments.
There are some limitations in our study, including the single-center population which may not represent characteristics of FPHL in Chinese individuals in general. Additionally, the consistency of measurements used in our study was not compared with others. In the future, more populations should be included and the consistency of different measuring tools should be compared.
Conclusion
Our study analyzed hair parameters of Chinese FPHL as well as healthy controls and indicated that hair density and terminal hair percentage in the scalp site exhibited the best predictive values in the Ludwig classification. We also reported a small quantity of female patients manifesting mainly parietal area hair loss were in moderate-to-severe stage in FPHL.
Ethics Statement
We confirm that our study complies with the Declaration of Helsinki.
Funding
This work was supported by the Nanjing Incubation Program for National Clinical Research Center [2019060001] and CAMS Innovation Fund for Medical Sciences (2021-I2M-C&T-B-087).
Disclosure
The authors report that no conflicts of interest in this work and confirm they do not hold stock or shares in any entity that may gain financial benefit or detriment as a result of the deliberations set out in or the conclusions of the study.
References
1. Harfmann KL, Bechtel MA. Hair loss in women. Clin Obstet Gynecol. 2015;58(1):185–199. doi:10.1097/GRF.0000000000000081
2. Xu F, Sheng YY, Mu ZL, et al. Prevalence and types of androgenetic alopecia in Shanghai, China: a community-based study. Br J Dermatol. 2009;160(3):629–632. doi:10.1111/j.1365-2133.2008.08909.x
3. Yip L, Rufaut N, Sinclair R. Role of genetics and sex steroid hormones in male androgenetic alopecia and female pattern hair loss: an update of what we now know. Australas J Dermatol. 2011;52(2):81–88. doi:10.1111/j.1440-0960.2011.00745.x
4. Redler S, Messenger AG, Betz RC. Genetics and other factors in the aetiology of female pattern hair loss. Exp Dermatol. 2017;26(6):510–517. doi:10.1111/exd.13373
5. Blume-Peytavi U, Blumeyer A, Tosti A, et al. S1 guideline for diagnostic evaluation in androgenetic alopecia in men, women and adolescents. Br J Dermatol. 2011;164(1):5–15. doi:10.1111/j.1365-2133.2010.10011.x
6. Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97(3):247–254. doi:10.1111/j.1365-2133.1977.tb15179.x
7. Gan DC, Sinclair RD. Prevalence of male and female pattern hair loss in Maryborough. J Investig Dermatol Symp Proc. 2005;10(3):184–189. doi:10.1111/j.1087-0024.2005.10102.x
8. Olsen EA. Current and novel methods for assessing efficacy of hair growth promoters in pattern hair loss. J Am Acad Dermatol. 2003;48(2):253–262. doi:10.1067/mjd.2003.81
9. Hamilton JB. Patterned loss of hair in man; types and incidence. Ann N Y Acad Sci. 1951;53(3):708–728. doi:10.1111/j.1749-6632.1951.tb31971.x
10. Ramos PM, Miot HA. Female Pattern Hair Loss: a clinical and pathophysiological review. An Bras Dermatol. 2015;90(4):529–543. doi:10.1590/abd1806-4841.20153370
11. Dhurat R, Saraogi P. Hair evaluation methods: merits and demerits. Int J Trichology. 2009;1(2):108–119. doi:10.4103/0974-7753.58553
12. Rojhirunsakool S, Suchonwanit P. Parietal scalp is another affected area in female pattern hair loss: an analysis of hair density and hair diameter. Clin Cosmet Investig Dermatol. 2018;11:7–12. doi:10.2147/CCID.S153768
13. Leerunyakul K, Suchonwanit P. Evaluation of hair density and hair diameter in the adult Thai population using quantitative trichoscopic analysis. Biomed Res Int. 2020;2020:2476890. doi:10.1155/2020/2476890
14. Mai W, Sun Y, Liu X, Lin D, Lu D. Characteristic findings by phototrichogram in southern Chinese women with Female pattern hair loss. Skin Res Technol. 2019;25(4):447–455. doi:10.1111/srt.12672
15. Ueki R, Tsuboi R, Inaba Y, Ogawa H. Phototrichogram analysis of Japanese female subjects with chronic diffuse hair loss. J Investig Dermatol Symp Proc. 2003;8(1):116–120. doi:10.1046/j.1523-1747.2003.12184.x
16. Chan L, Cook DK. Female pattern hair loss. Austr J General Pract. 2018;47(7):459–464. doi:10.31128/AJGP-02-18-4498
17. Ioannides D, Lazaridou E. Female pattern hair loss. Curr Probl Dermatol. 2015;47:45–54.
18. Yip L, Zaloumis S, Irwin D, et al. Gene-wide association study between the aromatase gene (CYP19A1) and female pattern hair loss. Br J Dermatol. 2009;161(2):289–294. doi:10.1111/j.1365-2133.2009.09186.x
19. Simpson ER, Davis SR. Minireview: aromatase and the regulation of estrogen biosynthesis--some new perspectives. Endocrinology. 2001;142(11):4589–4594. doi:10.1210/endo.142.11.8547
20. Paus R, Cotsarelis G. The biology of hair follicles. N Engl J Med. 1999;341(7):491–497. doi:10.1056/NEJM199908123410706
21. Cotsarelis G, Millar SE. Towards a molecular understanding of hair loss and its treatment. Trends Mol Med. 2001;7(7):293–301. doi:10.1016/S1471-4914(01)02027-5
22. Tobin DJ, Gunin A, Magerl M, Handijski B, Paus R. Plasticity and cytokinetic dynamics of the hair follicle mesenchyme: implications for hair growth control. J Invest Dermatol. 2003;120(6):895–904. doi:10.1046/j.1523-1747.2003.12237.x
23. Ekmekci TR, Sakiz D, Koslu A. Occipital involvement in female pattern hair loss: histopathological evidences. J Eur Acad Dermatol Venereol. 2010;24(3):299–301. doi:10.1111/j.1468-3083.2009.03411.x
24. Chai Y, Maxson RE. Recent advances in craniofacial morphogenesis. Dev Dyn. 2006;235(9):2353–2375. doi:10.1002/dvdy.20833
25. Heo JH, Yeom SD, Byun JW, Shin J, Choi GS. Significant relationship between temporal hair loss and other scalp areas in female pattern hair loss. J Dermatol. 2020;47(4):334–341. doi:10.1111/1346-8138.15220
26. Yazdabadi A, Magee J, Harrison S, Sinclair R. The Ludwig pattern of androgenetic alopecia is due to a hierarchy of androgen sensitivity within follicular units that leads to selective miniaturization and a reduction in the number of terminal hairs per follicular unit. Br J Dermatol. 2008;159(6):1300–1302. doi:10.1111/j.1365-2133.2008.08820.x
27. Sawaya ME, Price VH. Different levels of 5 alpha-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. J Invest Dermatol. 1997;109(3):296–300. doi:10.1111/1523-1747.ep12335779
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.