")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
The Predictive Value of Contrast-Enhanced Ultrasound Combined with Serum miR-124 Level in Acute Cerebral Infarction and Their Correlation with the Contrast Enhancement of Carotid Atherosclerotic Plaque
Authors Zhao P, Xu E, Yuan R, Zhou R, Pan J
Received 6 May 2022
Accepted for publication 28 June 2022
Published 11 July 2022 Volume 2022:18 Pages 1397—1403
DOI https://doi.org/10.2147/NDT.S372557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jun Chen
Ping Zhao,1 Erdong Xu,1 Rui Yuan,1 Ruhai Zhou,1 Jianlian Pan2
1Department of Ultrasound Medicine, Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, 315040, People’s Republic of China; 2Clinical Application Department, Shenzhen Mindray Bio-Medical Electronics Co, Ltd, Shenzhen, Guangzhou, 518057, People’s Republic of China
Correspondence: Ping Zhao, Department of Ultrasound Medicine, Affiliated People’s Hospital of Ningbo University, No. 251 Baizhang East Road, Ningbo, Zhejiang, 315040, People’s Republic of China, Email [email protected]
Objective: To investigate the predictive value of contrast-enhanced ultrasound (CEUS) combined with serum miR-124 level in acute cerebral infarction (ACI) and their association with the contrast enhancement of carotid atherosclerotic plaque.
Methods: Totally 60 patients diagnosed with ACI and 60 controls were included in the study. All the subjects had carotid atherosclerotic plaques, and all of them were examined by CEUS and were tested for serum miR-124 levels.
Results: Time to peak (TTP) and mean transit time (MTT) in the ACI group were significantly shorter than those in the control group (P < 0.05), but the peak intensity ratio (PIR), the area under the curve (AUC), and relative expression levels of serum miR-124 were notably greater in the ACI group (P < 0.05). There were statistically significant differences in TTP, MTT, PIR, AUC, and serum miR-124 expression in patients with different cerebral infarct areas in the ACI group (P < 0.05). Besides, the sensitivity and specificity of serum miR-124 levels for the prediction of ACI were 71.67% and 90.00%, respectively, with a cut-off value of 1.52, and the sensitivity was 86.67% and specificity was 93.33% of CEUS combined with serum miR-124 in the prediction of ACI. The ACI group showed a higher proportion of grades 2 and 3 (P < 0.001). Pearson correlation analysis showed that the intraplaque contrast enhancement was negatively related to TTP and MTT but had a positive correlation with PIR, AUC, and serum miR-124 levels.
Conclusion: Grades 2 and 3 intraplaque contrast enhancement and serum miR-124 level of 1.52 had high sensitivity and specificity to predict ACI. Moreover, the CEUS parameters combined with serum miR-124 level could improve the performance in predicting ACI and had auxiliary value in evaluating the stability of carotid atherosclerotic plaques.
Keywords: contrast-enhanced ultrasound, miR-124, acute cerebral infarction, carotid atherosclerotic plaque
Introduction
Acute cerebral infarction (ACI) is a neurological disorder caused by hypoxia and ischemia of local brain tissue due to insufficient blood supply.1 ACI mainly occurred in elderly people, and it is the leading cause of adult disability, cognitive impairment, and mortality worldwide, which seriously threatens human health.2 The risk of ACI lies not only in carotid artery lumen stenosis caused by atherosclerotic plaque but also in plaque stability.3 Pelisek et al pointed out that intraplaque neovascularization and inflammation are the two main characteristics of vulnerable plaques, and their vulnerability increases the risk of ACI.4 Limited by detection techniques, there is a lack of accurate and effective methods to detect neovascularization. For instance, computed tomography (CT) examination cannot show the ischemic focus well in the early stage of infarction, while magnetic resonance imaging (MRI) examination requires a high magnetic resonance signal and is not applicable for patients with metal stents.5,6 Although 18-FDG PET-CT is an accurate imaging modality for detecting atherosclerotic plaque inflammation, its clinical use is limited owing to its high cost and radiation exposure.7 Contrast-enhanced ultrasound (CEUS) as a noninvasive technique provides direct visualization of the intraplaque neovascularization.8 CEUS is featured with simplicity, and high spatial and temporal resolution.9 It has been demonstrated that the histological density of neovessels was positively related to the presence of neovascularization within the carotid plaques.10 The degree of enhancement of intraplaque neovascularization is associated with cerebrovascular and cardiovascular events.11,12 However, few studies have compared the CEUS parameters and intraplaque contrast enhancement assessed by CEUS among carotid atherosclerotic plaque patients with or without ACI.
MicroRNAs (miRNAs) are short, single-stranded RNAs consisting of 18–24 nucleotides.13 miR-124 is a brain-specific miRNA, which is highly expressed in the neurons throughout the brain.14 It has been reported that miR-124 is involved in the central nervous system development, neuronal immunity and differentiation, stroke, and brain cancers.15 Xu et al showed that the CEUS parameters and high sensitivity C-reactive protein level might be used for plaque risk stratification in ACI patients.16 Inspired by this study, we hypothesized that CEUS parameters and serum miR-124 might play an important role in predicting ACI.
Therefore, we conducted the present study to systemically evaluate the predictive value of CEUS parameters combined with serum miR-124 expression level in ACI and their correlation with the intraplaque contrast enhancement, providing a reference for the prediction and early diagnosis of ACI.
Materials and Methods
Patients
Sixty patients with ACI admitted to our hospital from January 2021 to December 2021 were recruited into the ACI group (36 males and 24 females; average age 66.78±7.29 years). Inclusion criteria: (1) meeting the diagnostic criteria of ACI16 or with carotid stroke and confirmed by CT and MRI examination; (2) within the first 48h after the first onset; (3) age > 60 years old; (4) without other treatment before admission; (5) with carotid atherosclerotic plaque. Exclusion criteria: (1) with intracerebral hemorrhage; (2) with a previous history of intracerebral hemorrhage; (3) with Alzheimer’s disease and Parkinson’s disease; (4) with malignant tumors; (5) with intracerebral infection. The infarct area of patients was calculated using the Pullicino formula.17 Patients with an infarct area <3 cm3 were included in the small infarction group (n=23), 3 cm3 ≤an infarct area ≤5 cm3 in the middle infarction group (n=22), and infarct area >5 cm3 in the large infarction group (n=15). There were 60 patients with carotid atherosclerotic plaque but no ACI during the same period in the control group, including 38 males and 22 females with an average age of 67.11±6.49 years. No statistical significance was observed in gender and age between the ACI and control groups (P >0.05) (data are not shown). This study was approved by the hospital ethics committee and informed consent was obtained from all the patients.
Standard Carotid Ultrasound and CEUS Examination
First, a standard carotid ultrasound was performed using a RESONA 7 color Doppler ultrasound diagnostic instrument and the supporting system (probe L11-3U, frequency 3–11 MHz) (Mindray, Shenzhen). The patients were asked to remain in a supine position with adequate exposure to the neck. The common carotid artery, carotid bifurcation as well as internal carotid arteries were visualized in longitudinal and transverse sections to observe the presence of plaque, and the thickness, length, and classification of the plaque. If the patient had more than one plaque, the thickest one on the relevant side (in the ACI group) and on either side (in the control group) was selected as the target plaque.
Then, patients underwent CEUS examination with the same machine. The contrast agent SonoVue (Bracco, Milan, Italy) was mixed with 5 mL of saline and shaken to homogeneity. A dose of 2 mL contrast agent was injected into the median cubital vein immediately, followed by a saline (5 mL) bolus. The synchronous real-time CEUS mode was turned on for dynamically observing the presence of plaques and their character and grading. The intraplaque contrast enhancement was classified as follows:18 grade 0: no visible microbubbles; grade 1: a small number of microbubbles; grade 3: many constant microbubbles; grade 2: microbubbles between grade 1 and 3. Scans were analyzed in CEUS by two experienced radiologists who had no prior knowledge of the patients’ clinical information. Inconsistent grading was discussed and the final result was determined by both radiologists. Meanwhile, the following parameters were measured: time to peak (TTP), peak intensity ratio (PIR), the area under the curve (AUC), and mean transit time (MTT).
Detection of Serum miR-124 Level
After enrollment, all participants fasted for 8–12 h, and about 5 mL of venous blood was drawn from the cubital vein the following morning, and serum was obtained by centrifugation at 3000 r/min for 10 min at 4 °C. Total RNA was extracted using the mirVana miRNA isolation kit (Ambion, USA). Then, the samples were stored in a −80℃ refrigerator. Following reverse transcription by TaqqManmicro reverse transcription kit (Ambion, USA), miR-124 was quantified by TaqMan MicroRNA Assays (Applied Biosystems, Carlsbad, CA, USA) according to the manufacturer’s instructions.
Statistical Analysis
Statistical analysis was performed by the SPSS software (version 17.0, USA). All continuous variables, tested as the normal distribution, were expressed by mean ± standard deviation (SD). A t-test was used for comparison between two groups, and a comparison of multiple groups was conducted with a one-way analysis of variance (ANOVA). Categorical data were presented as frequencies (n) and percentages (%) and were analyzed using the chi-square test. The receiver operating characteristic (ROC) curve was applied to evaluate the predictive efficacy of CEUS parameters and miR-124 level. Pearson correlation analysis was performed to determine the association of CEUS parameters and serum miR-124 level with intraplaque contrast enhancement. P <0.05 was considered statistically significant.
Results
Comparison of CEUS Parameters and Serum miR-124 Levels Between ACI and Control Groups
The TTP and MTT in the ACI group were significantly lower than those in the control group, while the PIR and AUC were remarkably higher (all P <0.05). In addition, the serum miR-124 levels of ACI patients and controls were 2.65±0.60 and 1.04±0.31, respectively, and the difference was statistically significant (P <0.05) (Table 1).
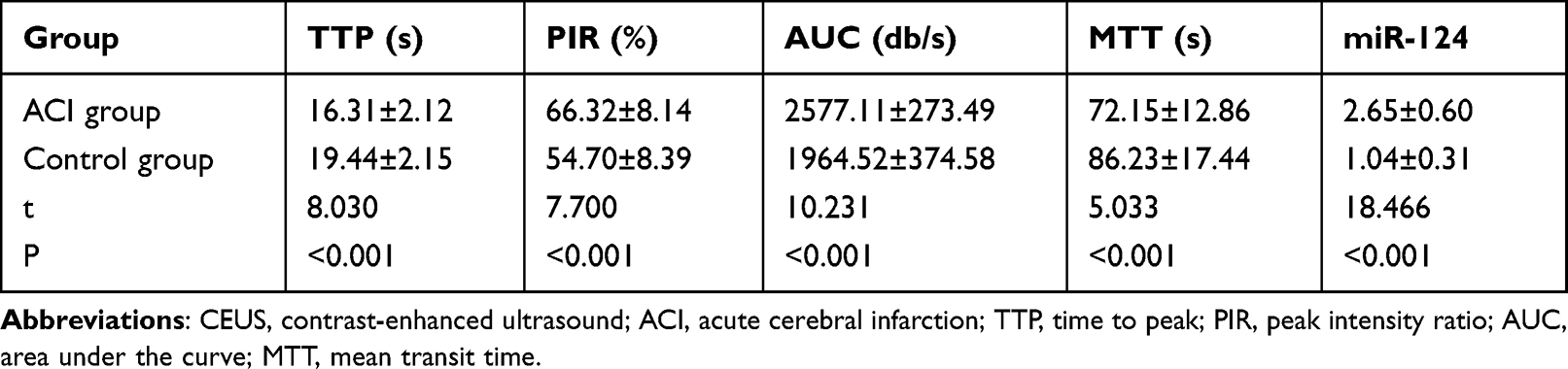 |
Table 1 Comparison of CEUS Parameters and Serum miR-124 Levels Between ACI and Control Groups |
Comparison of CEUS Parameters and Serum miR-124 Levels in ACI Patients with Different Infarct Areas
Compared with ACI patients with small infarct areas, those with middle and large infarct areas had significantly shorter TTP and MTT, but higher PIR, and AUC (P <0.05). TTP and MTT were also shorter in large infarct areas than those in middle infarct areas, but PIR and AUC were higher with statistically significant differences (P <0.05). Moreover, the relative expression level of miR-124 in patients with middle and large infarct areas was significantly higher than that in those with small infarct areas, and its expression in patients with large infarct areas was notably higher than that in those with middle infarct areas (P <0.05) (Table 2).
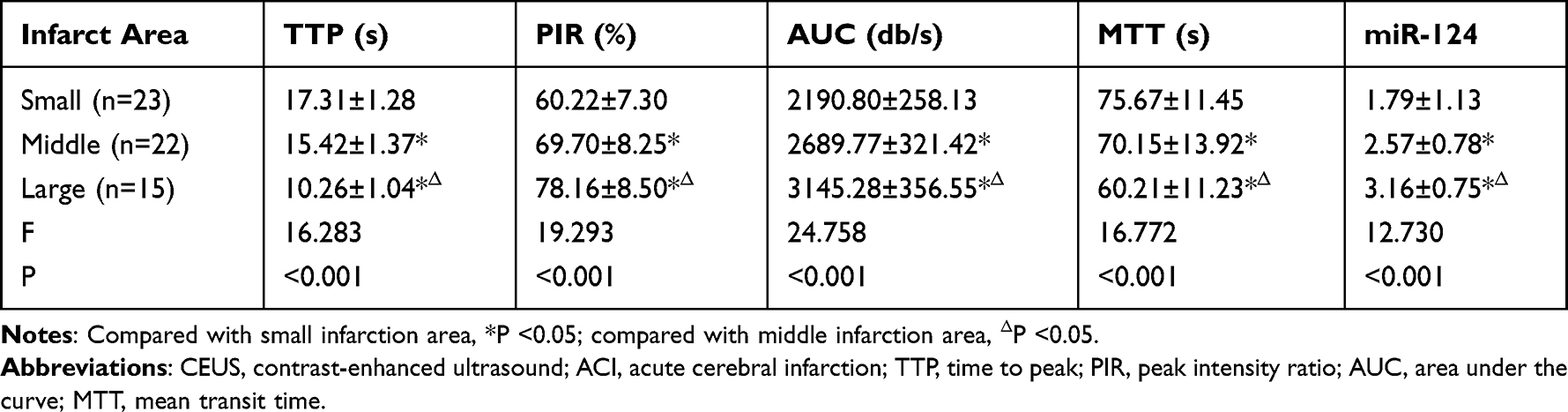 |
Table 2 Comparison of CEUS Parameters and Serum miR-124 Levels in ACI Patients with Different Infarct Areas |
The Predictive Value of CEUS Parameters Combined with Serum miR-124 Level in ACI Patients
When the optimal cut-off values of CEUS parameters TTP, PIR, and MTT were 15.82, 70.38, and 71.29, respectively, they had a sensitivity of 80.00% (48/60), 83.33% (50/60), and 86.67% (52/60) and the specificity of 83.33% (50/60), 86.67% (52/60), and 91.67% (55/60), respectively in predicting ACI. The sensitivity and specificity of serum miR-124 levels for the prediction of ACI were 71.67% (43/60) and 90.00% (54/60), respectively, with a cut-off value of 1.52. Importantly, CEUS parameters combined with serum miR-124 level detection had a sensitivity of 86.67% (52/60) and a specificity of 93.33% (56/60) (Table 3).
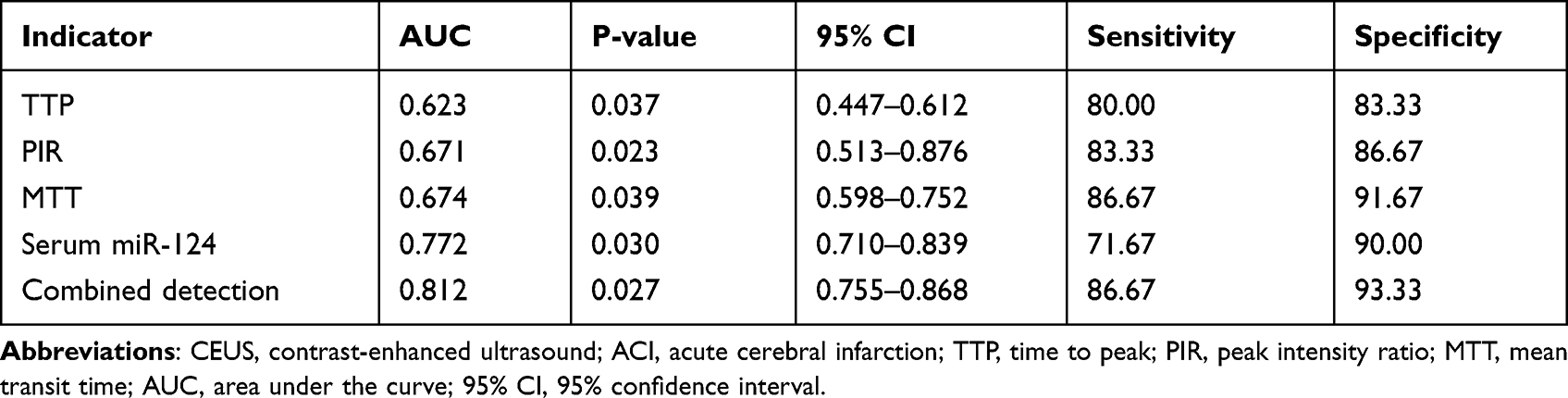 |
Table 3 The Predictive Value of CEUS Parameters and Serum miR-124 Level in ACI |
Comparison of the Intraplaque Contrast Enhancement Between ACI and Control Groups
To compare the plaque stability between ACI patients and controls, intraplaque contrast enhancement was assessed by CEUS. The intraplaque contrast enhancement was classified as grades 0–3 as the previously described. Compared with the control group, the ACI group showed a higher proportion of grade 2 and grade 3 (P <0.001). Thirteen patients in the ACI group exhibited low grades, ten of whom had stenotic carotid plaques (Table 4).
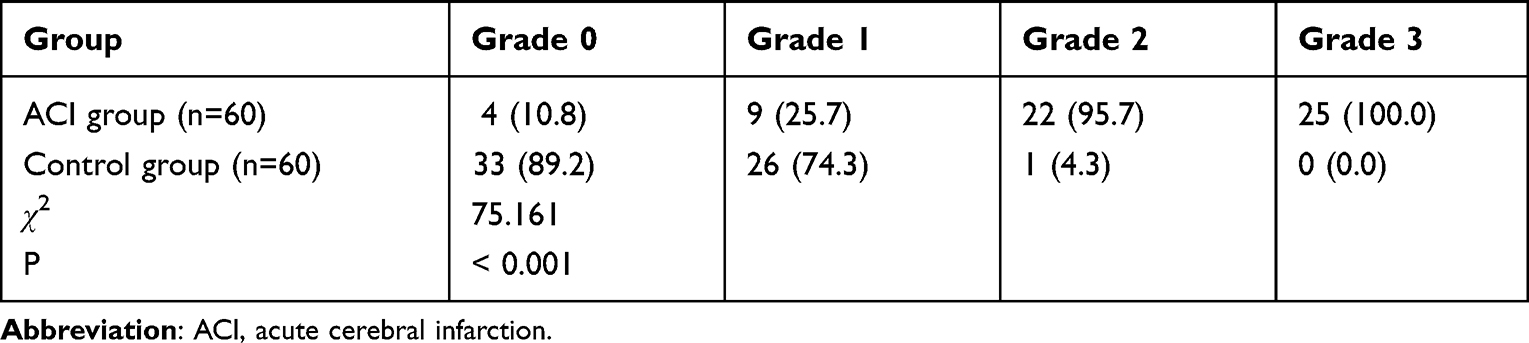 |
Table 4 Comparison of the Intraplaque Contrast Enhancement Between ACI and Control Groups (n, %) |
Association of CEUS Parameters and Serum miR-124 Level with the Intraplaque Contrast Enhancement
Pearson correlation analysis showed that there were negative associations of CEUS parameters TTP and MTT with the enhancement degree of CEUS in carotid atherosclerotic plaques (r=−0.482, −0.557). Whereas, PIR, AUC, and serum miR-124 levels were positively related to the intraplaque contrast enhancement (r=0.544, 0.601, 0.528), suggesting that CEUS parameters and serum miR-124 levels may assist in evaluating the stability of carotid atherosclerotic plaques.
Discussion
ACI is a common disease with high morbidity and mortality.19 Atherosclerotic plaque rupture is the leading cause of ACI.20 It has been reported that neovascularization is an essential factor in promoting the formation and development of vulnerable atherosclerotic plaques.21 In addition, neovascularization is a consistent feature of vulnerable plaques in cerebrovascular diseases.22 These studies exhibited that neovascularization might play a vital role in the occurrence of plaque rupture, thereby promoting ACI.
Due to its advantages of convenient examination and non-invasiveness, ultrasonography has become the most important auxiliary method in clinical practice and the first choice for the screening and assessment of carotid atherosclerosis.23 Nevertheless, the presence of new blood vessels in atherosclerotic plaques is difficult to be accurately detected by ordinary ultrasound.24 CEUS is a kind of imaging technique in which the contrast agent containing microbubbles is injected into the patient’s vein, which helps to observe the changes of the lesion signal through the scattering intensity and sound impedance, and then analyze the character of the lesion.25 When used for the detection of atherosclerosis, it can enhance the blood flow signal, reflect the change of plaque, improve the imaging of intraplaque neovascularization, and carry out parameter analysis.26 The quantitative CEUS parameters reflect the blood perfusion and perfusion patterns of atherosclerotic plaques from different sides.16 We compared the CEUS parameters in different groups and found that the TTP and MTT in the ACI group were significantly lower than those in the control group, but the PIR and AUC were remarkably higher. This suggested that the carotid atherosclerotic plaques of ACI patients might have more neovascularization and vulnerability.
Inflammation, as another crucial factor of vulnerable plaque, had an intimate relationship with atherosclerosis.4,27 Therefore, serum inflammatory markers are very powerful for assessing the prognosis of ACI patients. Extracellular vesicles (EVs) containing miRNAs represent an essential role in cell signaling events both during the acute phase of stroke and in the long-term post-stroke recovery. The EVs can be detected in the periphery, making them useful in deciphering the mechanisms underlying other brain disorders such as Parkinson’s disease and Alzheimer’s disease.28 In addition, these small EVs regulated a set of miRNAs linked to angiogenesis, which have therapeutic efficacy in ischemic stroke recovery.29 MiR-124 is involved in synapse morphology, neurotransmission, inflammation, autophagy, and mitochondrial function.30 It has been evidenced that the aberrant expression of miR-124 was linked to various neurological disorders including stroke.31 Further, miR-124 has been shown to participate in myocardial remodeling in a number of cardiovascular diseases.32 Accumulating evidence exhibited that miR-124 is abnormally expressed in peripheral blood and brain vascular endothelial cells following cerebral ischemia.33 In this study, the relative miR-124 expression was increased in ACI patients. The authors speculated that the elevated level of miR-124 might be associated with ischemic hypoxia or subsequent inflammatory cascade after ACI. Expectedly, there were differences in miR-124 levels among groups with different infarct areas. The relative expression level of miR-124 in ACI patients with middle and large infarct areas was significantly higher than that of those with small infarcts, and the miR-124 level in patients with large infarct areas was significantly higher than that of those with middle infarcts. The serum level of miR-124 elevated with the increase of infarct area, which may be due to ACI-induced inflammation in blood vessels and nerves. Thus, it is reasonable to infer that the miR-124 level might be a critical biomarker of ACI and could reflect the severity of ACI.
Furthermore, we explored the predictive value of the CEUS parameters combined with the miR-124 expression level in ACI. The results showed that the sensitivity was 71.67% and specificity was 90.00% of serum miR-124 levels in predicting ACI with a cut-off value of 1.52, and the combined detection performed well in predicting ACI with an AUC of 0.812. Since carotid atherosclerotic plaques have the same pathological changes as ACI, some patients developed ACI due to plaque shedding.34 Meanwhile, patients with ACI should be alert to the risk of secondary infarction caused by plaque shedding. Thus, further understanding of the stability of atherosclerotic plaques is needed in patients with ACI. In this study, the plaque grades were mainly grades 2 and 3 in patients with ACI; while the pure atherosclerotic patients were mainly at grades 0 and grade 1, indicating that the plaque stability in ACI patients was poor. Pearson correlation analysis showed that the intraplaque contrast enhancement was negatively related to TTP and MTT, but had a positive correlation with PIR, AUC, and serum miR-124 levels, suggesting that CEUS parameters and serum miR-124 levels were closely associated with instability of the plaque.
However, further research with a larger sample size is required to validate our results. Second, only the thickest plaque was analyzed in patients with more than one separate plaque, which might not be the one causing symptoms. Then, the authors did not collect the serum miR-124 levels at several time points. Finally, the study did not take into account some important risk factors related to lifestyle, obesity, and aging, which will be studied in the future.
In conclusion, grades 2 and 3 intraplaque contrast enhancement and serum miR-124 level of 1.52 had high sensitivity and specificity to predict ACI. Additionally, the combination of CEUS parameters with serum miR-124 level improved the efficacy of predicting ACI.
Data Sharing Statement
The dataset used and/or analyzed during the current study is available from the corresponding author on reasonable request.
Ethics Approval
This study was approved by the ethics committee of Affiliated People’s Hospital of Ningbo University and informed consent was obtained from all the patients. Our study complies with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest to declare.
References
1. Liu G, Liang Y, Xu M, et al. Protective mechanism of Erigeron breviscapus injection on blood-brain barrier injury induced by cerebral ischemia in rats. Sci Rep. 2021;11(1):18451. doi:10.1038/s41598-021-97908-x
2. Nasb M, Li Z, Say A, Dayoub L, Chen H. Comparison of the effects of modified constraint-induced movement therapy and intensive conventional therapy with a botulinum-a toxin injection on upper limb motor function recovery in patients with stroke. Libyan J Med. 2019;14(1):1609304. doi:10.1080/19932820.2019.1609304
3. Xia J, Yin A, Li Z, Liu X, Peng X, Xie N. Quantitative analysis of lipid-rich necrotic core in carotid atherosclerotic plaques by in vivo magnetic resonance imaging and clinical outcomes. Med Sci Monit. 2017;23:2745–2750. doi:10.12659/MSM.901864
4. Pelisek J, Eckstein HH, Zernecke A. Pathophysiological mechanisms of carotid plaque vulnerability: impact on ischemic stroke. Arch Immunol Ther Exp. 2012;60(6):431–442. doi:10.1007/s00005-012-0192-z
5. Mamlouk MD, Tsai FY, Drachman D, Stradling D, Hasso AN. Cerebral thromboembolism: value of susceptibility-weighted imaging in the initial diagnosis of acute infarction. Neuroradiol J. 2012;25(1):45–56. doi:10.1177/197140091202500107
6. Zhang W, Cheng J, Zhang Y, Wang K, Jin H. Analysis of CT and MRI combined examination for the diagnosis of acute cerebral infarction. J Coll Physicians Surg Pak. 2019;29(9):898–899. doi:10.29271/jcpsp.2019.09.898
7. Giles JT, Rist PM, Liao KP, et al. Testing the effects of disease-modifying antirheumatic drugs on vascular inflammation in rheumatoid arthritis: rationale and design of the TARGET trial. ACR Open Rheumatol. 2021;3(6):371–380. doi:10.1002/acr2.11256
8. Sedding DG, Boyle EC, Demandt JAF, et al. Vasa vasorum angiogenesis: key player in the initiation and progression of atherosclerosis and potential target for the treatment of cardiovascular disease. Front Immunol. 2018;9:706. doi:10.3389/fimmu.2018.00706
9. Akkus Z, Hoogi A, Renaud G, et al. New quantification methods for carotid intra-plaque neovascularization using contrast-enhanced ultrasound. Ultrasound Med Biol. 2014;40(1):25–36. doi:10.1016/j.ultrasmedbio.2013.09.010
10. Schmidt C, Fischer T, Ruckert RI, et al. Identification of neovascularization by contrast-enhanced ultrasound to detect unstable carotid stenosis. PLoS One. 2017;12(4):e0175331. doi:10.1371/journal.pone.0175331
11. Li Z, Xu X, Ren L, et al. Prospective study about the relationship between CEUS of carotid intraplaque neovascularization and ischemic stroke in TIA patients. Front Pharmacol. 2019;10:672. doi:10.3389/fphar.2019.00672
12. Camps-Renom P, Prats-Sanchez L, Casoni F, et al. Plaque neovascularization detected with contrast-enhanced ultrasound predicts ischaemic stroke recurrence in patients with carotid atherosclerosis. Eur J Neurol. 2020;27(5):809–816. doi:10.1111/ene.14157
13. Sanuki R, Yamamura T. Tumor suppressive effects of miR-124 and its function in neuronal development. Int J Mol Sci. 2021;22:11. doi:10.3390/ijms22115919
14. Forero DA, van der Ven K, Callaerts P, Del-Favero J. miRNA genes and the brain: implications for psychiatric disorders. Hum Mutat. 2010;31(11):1195–1204. doi:10.1002/humu.21344
15. Sun Y, Luo ZM, Guo XM, Su DF, Liu X. An updated role of microRNA-124 in central nervous system disorders: a review. Front Cell Neurosci. 2015;9:193. doi:10.3389/fncel.2015.00193
16. Xu R, Yin X, Xu W, Jin L, Lu M, Wang Y. Assessment of carotid plaque neovascularization by contrast-enhanced ultrasound and high sensitivity C-reactive protein test in patients with acute cerebral infarction: a comparative study. Neurol Sci. 2016;37(7):1107–1112. doi:10.1007/s10072-016-2557-2
17. Liu X. Changes and significance of serum CXCL-16, GDF-15, PLA-2 levels in patients with cerebral infarction. Am J Transl Res. 2021;13(5):5617–5622.
18. Motoyama R, Saito K, Tonomura S, et al. Utility of complementary magnetic resonance plaque imaging and contrast-enhanced ultrasound to detect carotid vulnerable plaques. J Am Heart Assoc. 2019;8(8):e011302. doi:10.1161/JAHA.118.011302
19. Zhang Y, Zhang QQ, Fu C, et al. Clinical efficacy of tirofiban combined with a Solitaire stent in treating acute ischemic stroke. Braz J Med Biol Res. 2019;52(10):e8396. doi:10.1590/1414-431x20198396
20. Luo X, Li W, Bai Y, Du L, Wu R, Li Z. Relation between carotid vulnerable plaques and peripheral leukocyte: a case-control study of comparison utilizing multi-parametric contrast-enhanced ultrasound. BMC Med Imaging. 2019;19(1):74. doi:10.1186/s12880-019-0374-9
21. Chen F, Eriksson P, Kimura T, Herzfeld I, Valen G. Apoptosis and angiogenesis are induced in the unstable coronary atherosclerotic plaque. Coron Artery Dis. 2005;16(3):191–197. doi:10.1097/00019501-200505000-00009
22. Staub D, Patel MB, Tibrewala A, et al. Vasa vasorum and plaque neovascularization on contrast-enhanced carotid ultrasound imaging correlates with cardiovascular disease and past cardiovascular events. Stroke. 2010;41(1):41–47. doi:10.1161/STROKEAHA.109.560342
23. Katakami N, Matsuoka TA, Shimomura I. Clinical utility of carotid ultrasonography: application for the management of patients with diabetes. J Diabetes Investig. 2019;10(4):883–898. doi:10.1111/jdi.13042
24. Zamani M, Skagen K, Scott H, Russell D, Skjelland M. Advanced ultrasound methods in assessment of carotid plaque instability: a prospective multimodal study. BMC Neurol. 2020;20(1):39. doi:10.1186/s12883-020-1620-z
25. Liu YX, Liu Y, Xu JM, Chen Q, Xiong W. Color Doppler ultrasound and contrast-enhanced ultrasound in the diagnosis of lacrimal apparatus tumors. Oncol Lett. 2018;16(2):2215–2220. doi:10.3892/ol.2018.8879
26. Reiber JHC, De Sutter J, Schoenhagen P, Stillman AE, Vande Veire NRL. Cardiovascular imaging 2016 in the International Journal of Cardiovascular Imaging. Int J Cardiovasc Imaging. 2017;33(6):761–770. doi:10.1007/s10554-017-1111-5
27. Jenny NS, Callas PW, Judd SE, et al. Inflammatory cytokines and ischemic stroke risk: the REGARDS cohort. Neurology. 2019;92(20):e2375–e2384. doi:10.1212/WNL.0000000000007416
28. Driga MP, Catalin B, Olaru DG, et al. The need for new biomarkers to assist with stroke prevention and prediction of post-stroke therapy based on plasma-derived extracellular vesicles. Biomedicines. 2021;9(9):1226. doi:10.3390/biomedicines9091226
29. Gregorius J, Wang C, Stambouli O, et al. Small extracellular vesicles obtained from hypoxic mesenchymal stromal cells have unique characteristics that promote cerebral angiogenesis, brain remodeling and neurological recovery after focal cerebral ischemia in mice. Basic Res Cardiol. 2021;116(1):40. doi:10.1007/s00395-021-00881-9
30. Soreq H, Wolf Y. NeurimmiRs: microRNAs in the neuroimmune interface. Trends Mol Med. 2011;17(10):548–555. doi:10.1016/j.molmed.2011.06.009
31. Sun Y, Gui H, Li Q, et al. MicroRNA-124 protects neurons against apoptosis in cerebral ischemic stroke. CNS Neurosci Ther. 2013;19(10):813–819. doi:10.1111/cns.12142
32. Liu L, Zang J, Chen X, et al. Role of miR-124 and miR-141 in the regulation of vascular reactivity and the relationship to RhoA and Rac1 after hemorrhage and hypoxia. Am J Physiol Heart Circ Physiol. 2016;310(2):H206–H216. doi:10.1152/ajpheart.00651.2014
33. Liu X, Feng Z, Du L, et al. The potential role of MicroRNA-124 in cerebral ischemia injury. Int J Mol Sci. 2019;21(1):120. doi:10.3390/ijms21010120
34. Wang G, Cheng X, Zhang X. Use of various CT imaging methods for diagnosis of acute ischemic cerebrovascular disease. Neural Regen Res. 2013;8(7):655–661. doi:10.3969/j.issn.1673-5374.2013.07.010
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.