")
Back to Journals » Infection and Drug Resistance » Volume 13
The Phylogenetic Relatedness of blaNDM-1 Harboring Extended-Spectrum β-Lactamase Producing Uropathogenic Escherichia coli and Klebsiella pneumoniae in the North of Iran
Authors Jamali S, Tavakoly T, Mojtahedi A , Shenagari M
Received 9 September 2019
Accepted for publication 8 February 2020
Published 25 February 2020 Volume 2020:13 Pages 651—657
DOI https://doi.org/10.2147/IDR.S230335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eric Nulens
Samar Jamali, 1 Talayeh Tavakoly, 1 Ali Mojtahedi, 1 Mohammad Shenagari 2
1Department of Microbiology, Rasht Branch, Islamic Azad University, Rasht, Iran; 2Cellular and Molecular Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran
Correspondence: Ali Mojtahedi
Department of Microbiology, School of Medicine, Guilan University Campus, 7th Km of Rasht-Tehran Highway, Rasht, Guilan, Iran
Tel +981333690884
Fax +981333690036
Email [email protected]
Background: Escherichia coli and Klebsiella pneumoniae as an important part of Enterobacterales family are important causes of both community- and hospital-acquired infections. The present study aimed to investigate the prevalence of antibiotics resistance and molecular characteristics of uropathogenic isolates of E. coli and K. pneumoniae in Iranian patients.
Methods: This cross-sectional study performed on 223 Escherichia coli and 68 Klebsiella pneumoniae isolates obtained from hospitalized patients in the north of Iran. The isolates were identified by standard microbiologic tests and confirmed by API 20E strip. Disk diffusion method was applied to determine antibiotic susceptibility pattern. The presence of β-lactamases encoding genes was evaluated by PCR method. Analysis of the mutations and homology among sequences was done by the CLC sequence viewer (Qiagen, Denmark), and phylogenetic trees were constructed by the neighbor-joining method (Bootstrap: 1000 times).
Results: The overall rates of extended-spectrum β-lactamases (ESBLs)-producing E. coli and K. pneumoniae isolates were 37.7% and 32.4%, respectively. The overall presence of blaSHV, blaNDM-1, and blaOXA-1 genes was detected in 16 (5.5%), 12 (4.1%), and 48 (16.4%) of isolates, respectively. The neighbor-joining analysis for E. coli KU985246.1 strain showed that the most related blaNDM-1 sequences were from China, Singapore, UK, Thailand, and Bangladesh. While K. pneumoniae KU985245.1 strains were mostly related to blaNDM-1 sequences form Myanmar, and China.
Conclusion: In summary, the remarkable rate of ESBL-producing uropathogenic Enterobacterales along with the first prevalence of NDM-1 β-lactamases can be a serious concern in our region.
Keywords: uropathogenic, Escherichia coli, Klebsiella pneumoniae, antibiotic resistance, ESBL, NDM-1 β-lactamases
Introduction
Escherichia coli and Klebsiella pneumoniae are Gram negative, facultative anaerobic rods belonging to the family of Enterobacterales which are part of the gastrointestinal tract microbiota.1 These opportunistic pathogens lead to both community- and hospital-acquired infections with a wide range of complications, such as blood stream, respiratory tract, surgical wounds, gastrointestinal, and urinary tract infections.1,2
Beta-lactam (β-lactam) antibiotics are amongst the widely prescribed agents for managing E. coli and K. pneumoniae related infections.3,4 However, recently extended-spectrum beta-lactamases (ESBLs) producing strains have emerged as a critical health issue.3 The hydrolyzing activity of ESBLs which results in the inactivation of penicillins, broad-spectrum cephalosporins, and monobactams.3,4 These enzymes are divided into several main groups, including SHV, TEM, and CTX-M, which are able to inactivate the b-lactams by hydrolyzing the b-lactam ring.3
ESBLs cannot efficiently inactivate cephamycins, beta-lactamase inhibitors, and particularly carbapenems. So, carbapenems act as important therapeutic options against multiple-drug resistant (MDR) strains.5 However, recently the trend of carbapenemase producing Enterobacterales has increased all around the world, as well as in Iran.6–8 According to the Ambler classification of β-lactamases, two main classes of carbapenemases were introduced. One of them is class B Zinc metallo-beta-lactamase (MBL), susceptibleto metallic ion chelator such as EDTA,9 in which New Delhi metallo-β-lactamase (NDM) is the most important enzyme.10 Secondly come oxacillinase (OXA) enzymes or class D β-lactamases, subclassified based on single amino acid substitutions or deletions that are responsible for their effective hydrolyzing activity.10
The β-lactamase production is mostly associated with achievement of resistance determinant genes carried on large plasmids whose dissemination by horizontal gene transfer among different species has become a serious global health problem.11
In regard to the importance of epidemiological data on ESBLs and carbapenems producing strains, we aimed to analyze the molecular characteristics of uropathogenic E. coli and K. pneumoniae and its antibiotics resistance pattern in northern Iran.
Materials and Methods
Study Design and Bacterial Isolates
This cross-sectional study was performed at 5 teaching hospitals in the north of Iran within six months. This study has been designed in accordance with the declaration of Helsinki and also the regional approval obtained by University Ethics Committee (IR.GUMS.REC.1394.641). The presumptive E. coli and K. pneumoniae isolates were isolated from clean-catch urine specimens using standard microbiologic tests and API 20E strips (API-bioMérieux, France).
Antimicrobial Susceptibility Testing
The antibiotic susceptibility of isolates was tested by standard disk diffusion method on Mueller-Hinton agar medium (Merck, Germany) according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.12 The antibiotic disks were ampicillin (10 µg), amoxicillin-clavulanate (20/10 µg), cefepime (30 µg), aztreonam (30 µg), gentamicin (10 µg), nalidixic acid (30 µg), ofloxacin (5 µg), ciprofloxacin (5 µg), cefoxitin (30 µg), cefixime (5 µg), ceftazidime (30 µg), cefotaxime (30 µg), imipenem (10 µg), tetracycline (30 µg), trimethoprim/sulfamethoxazole (25 µg), and nitrofurantoin (300 µg). E. coli ATCC 25922 strain was employed for quality check purpose. Multiple-drug resistant (MDR) isolates were defined non-susceptible (resistant or intermediate) to at least 1 agent in ≥3 antimicrobial categories according to previously mentioned definitions.13 ESBL testing was performed by double-disk synergy test using cefotaxime (30 µg) and ceftazidime (30 µg), alone and in combination with clavulanate (10 µg).12 Escherichia coli ATCC 25922 and K. pneumoniae ATCC 700603 were used as negative and positive control strains, respectively.
Plasmid DNA Extraction and Molecular Assays
Plasmid DNA extraction from the fresh isolates was done using gene JET plasmid miniprep Kit (Fermentas, Lithuania) according to its instructions. PCR was performed to detect blaSHV, blaOXA-1, and blaNDM genes by a Veriti 96-well thermal cycler instrument (Applied Biosystems at Life Technologies, Foster City, CA) as previously described.14–16 Primers were provided by Metabion Co, Germany. The list of used primers is shown in Table 1. PCR was done in a final volume of 20 μL containing Master Mix (Bioneer, South Korea), primers at concentrations of 0.3–0.4 µM, 3μL DNA templates and ddH2O. All controls for PCR were kindly provided by Pasteur Institute, Tehran, Iran. The PCR setup was an initial denaturation step at 94°C for 3 min, followed by 30 cycles of DNA denaturation at 94°C for 30 s, primer annealing for 45 sec Temperatures varied based on the sequences of primers, and primer extension at 72°C for 50 sec, followed by a final extension at 72°C for 5 min. The products were separated by electrophoresis in 1% agarose gels with 1 X TAE (Tris/Acetate/EDTA) buffer, stained with safe stain load dye (CinnaGen Co., Iran), and visualized under ultraviolet illumination.
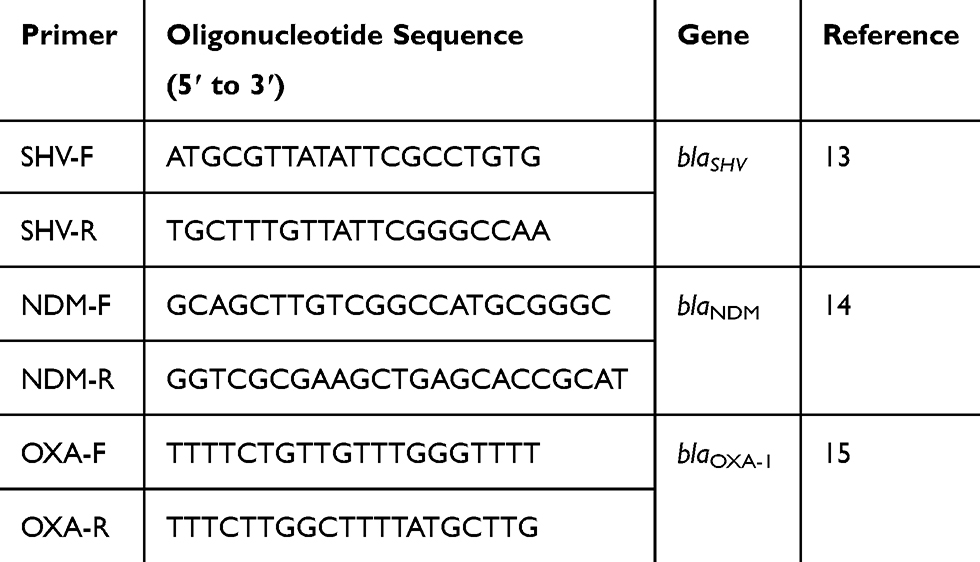 |
Table 1 Primer Sequences Used in the Present Study |
DNA Sequencing
To confirm PCR products, a purified amplicon of tested genes was sent for sequencing by the ABI capillary system (Macrogen Research, Seoul, Korea). Afterwards, sequences were confirmed by comparison with available sequences on NCBI database (http://www.ncbi.nlm. nih.gov/BLAST/). These sequences were submitted in the GenBank nucleotide database under accession numbers: MG797557 (OXA-1, E. coli), KU985247.1 (OXA-1, K. pneumoniae), MG797558 (SHV-1, E. coli), MG797559 (SHV-1, K. pneumoniae), KU985246.1 (NDM-1, E. coli), and KU985245.1 (NDM-1, K. pneumoniae) available at National Center of Biotechnology Information website (http://www.ncbi.nlm.nih.gov). The mutations and homology among sequences were analyzed by the CLC sequence viewer (Qiagen, Denmark), and phylogenetic trees were constructed by the neighbor-joining method (Bootstrap: 1000 times).
Statistical Analysis
The distribution of antibiotic resistance and genes between groups was calculated by Chi-square and Fisher’s exact tests using SPSSTM software, version 21.0 (IBM Corp., USA). A P value of ≤0.05 was considered as statistically significant.
Results
Generally, 291 uropathogenic isolates, consisting of 223 E. coli and 68 K. pneumoniae isolates were included in our study. E. coli isolates were obtained from 169 (75.8%) female and 54 (24.2%) male subjects with a mean age of 35.8 ± 26.3 years. Also, K. pneumoniae isolates were obtained from 38 (55.9%) female and 30 (44.1%) male subjects with a mean age of 28.3 ± 26.7 years. In overall, the age range of included patients was from 1 month to 89 years.
The results revealed that E. coli isolates were mostly non-susceptible to ampicillin (84.8%) followed by nalidixic acid (78.5%) and tetracycline (65.5%) while the highest susceptibility belonged to imipenem (97.8%). Regarding antibiotic susceptibility among K. pneumoniae isolates, the lowest susceptibility rate was held by nalidixic acid (29.4%) followed by nitrofurantoin (47.1%), and the highest susceptibility belonged to imipenem (94.1%). Further analysis revealed that the rate of ESBL-producing E. coli and K. pneumoniae isolates were 37.7% and 32.4%, respectively. ESBLs producers showed significantly higher antibiotic resistance compared to non-ESBLs (Tables 2 and 3). Moreover, the most effective in vitro agent against ESBL-producing in both uropathogenic isolates was imipenem. The distribution of ESBLs isolates according to patients age was 28 (26.4%) among patients less than 18 years, 55 (51.9%) among 19–64 years, and 23 (21.7%) among older than 65 years old.
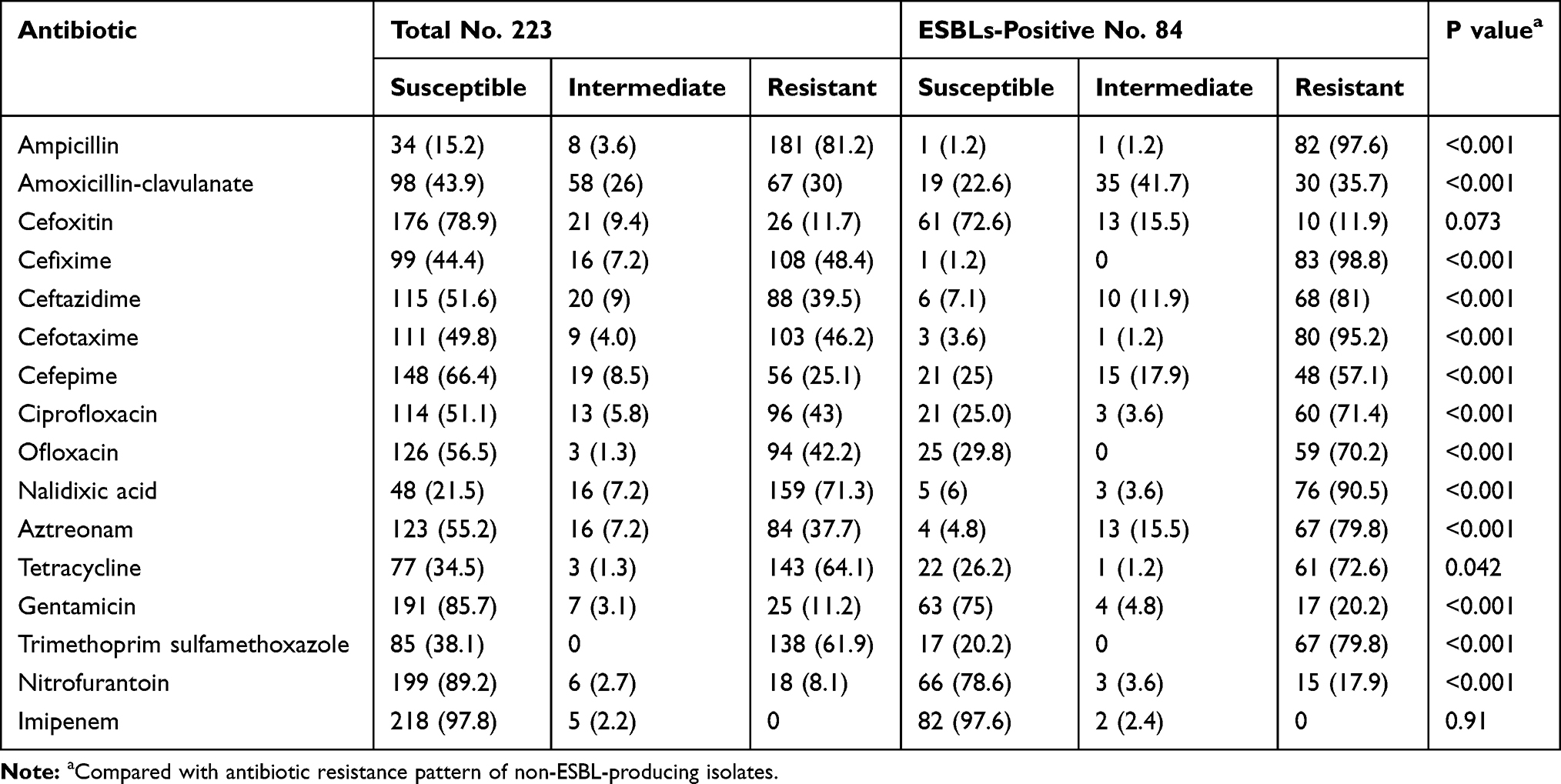 |
Table 2 The Results of Antibiotic Susceptibility Pattern of E. coli Isolates |
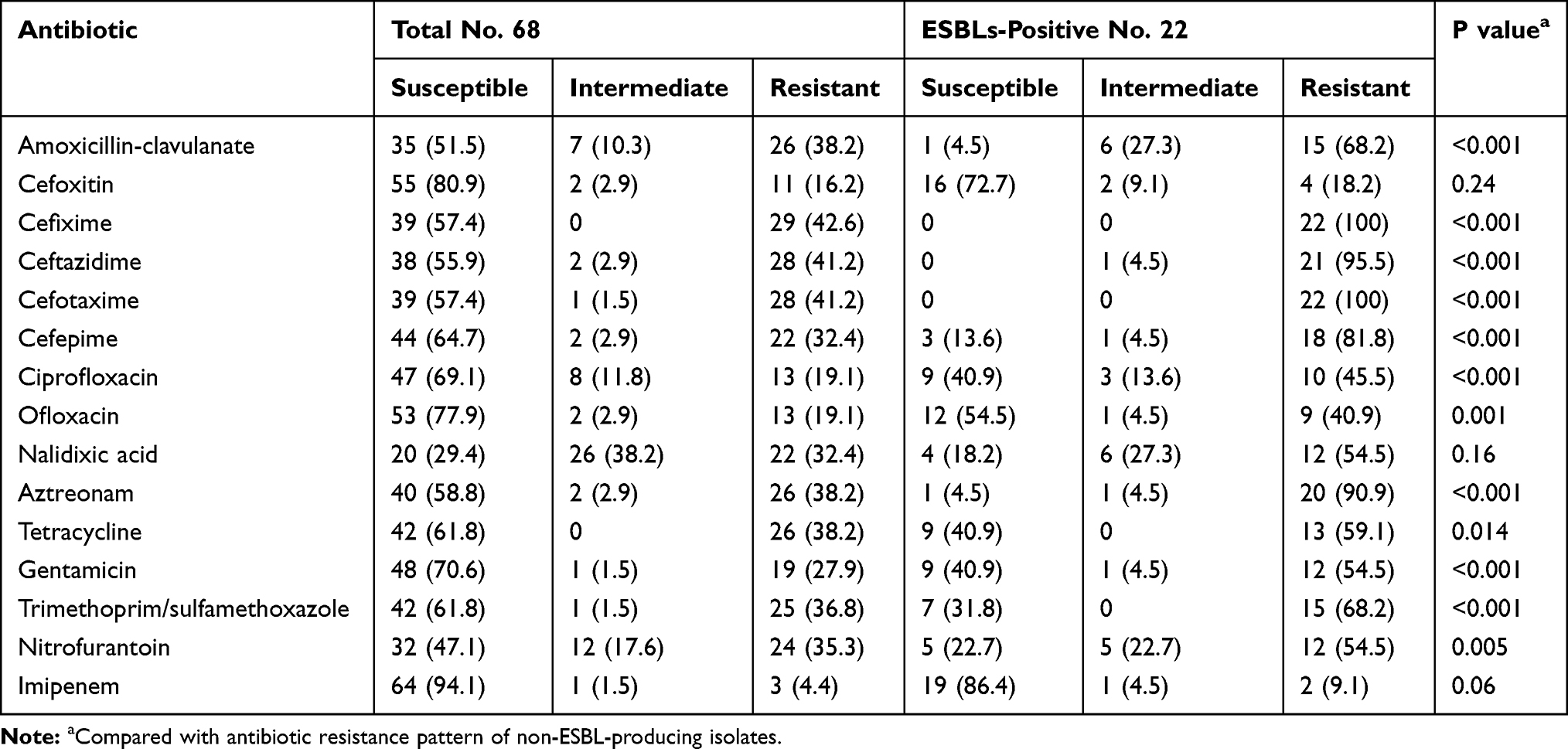 |
Table 3 The Results of Antibiotic Susceptibility Pattern of K. pneumoniae Isolates |
The overall presence of blaSHV, blaNDM-1, and blaOXA-1 genes was detected in 16 (5.5%), 12 (4.1%), and 48 (16.4%) of isolates, respectively. Full results of investigated genes separated by pathogen, MDR, ESBLs, and carbapenem resistance are presented in Table 4. The investigated genes were significantly more prevalent in ESBLs-producing isolates in both uropathogens whereas only the presence of blaNDM-1 gene in K. pneumoniae was significantly associated with carbapenem-resistant isolates.
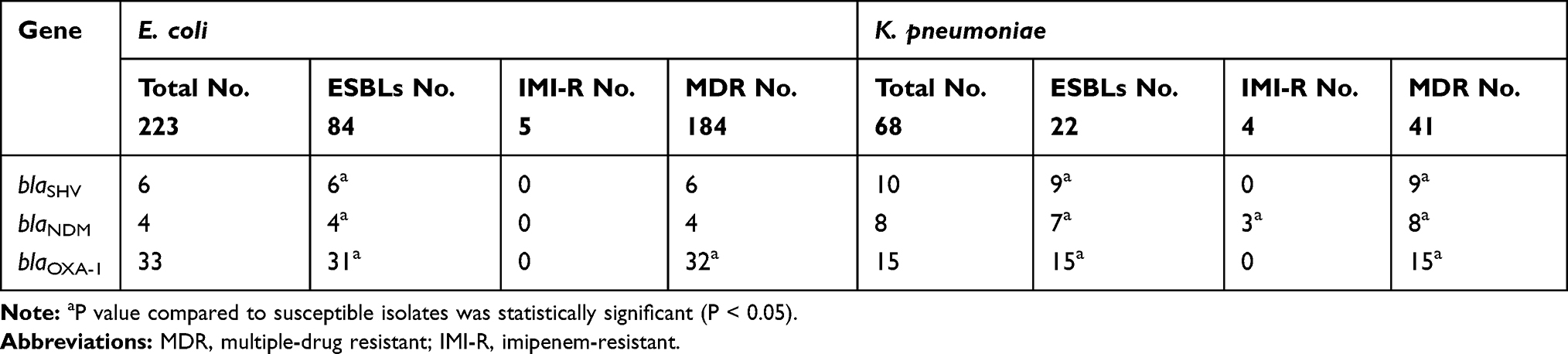 |
Table 4 The Full Results of Investigated Genes Separated by Pathogen, MDR, ESBLs, and Carbapenem Resistance |
The neighbor-joining analysis for E. coli KU985246.1 strain indicated that the most related blaNDM-1 sequences were from China, Singapore, UK, Thailand, and Bangladesh. However, K. pneumoniae KU985245.1 strains were mostly related to blaNDM-1 sequences from Myanmar and China (Figure 1).
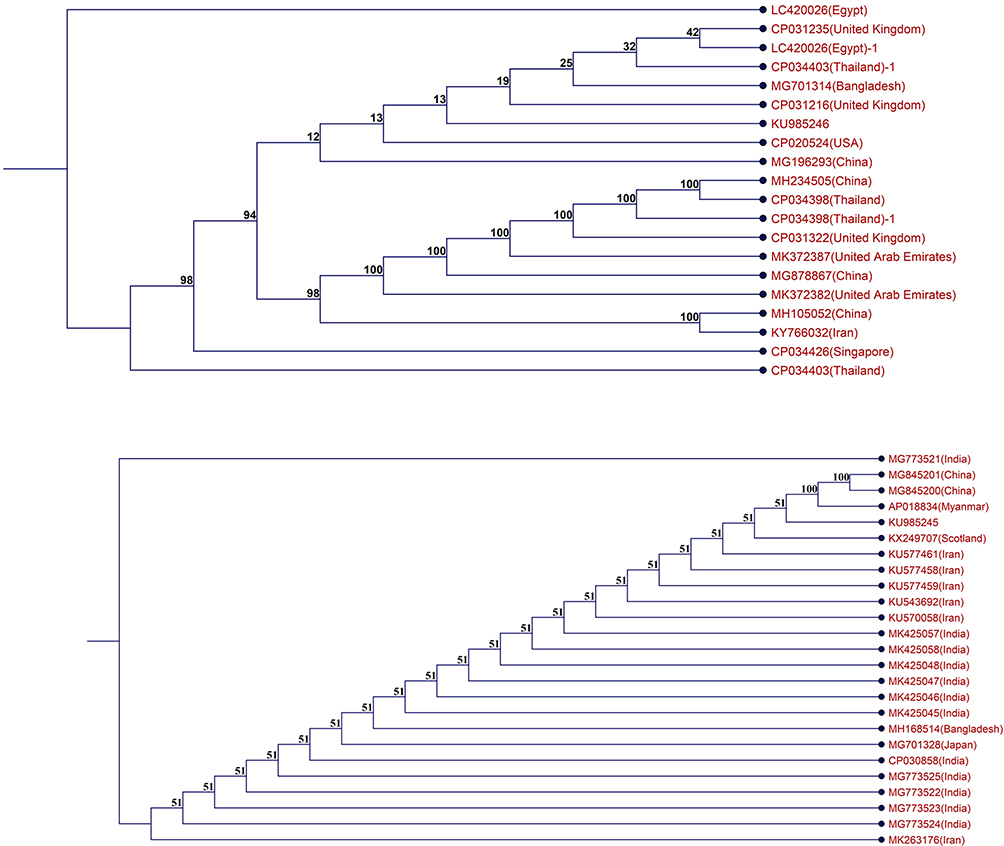 |
Figure 1 The neighbor-joining dendrogram (Boot strap: 1000) of two blaNDM-1 harboring isolates. |
The pervasiveness of MDR isolates was estimated at 82.5% in E. coli and 60.3% in K. pneumoniae while the rate of MDR isolates was significantly higher in ESBLs-producing isolates, as 45.7% of E. coli, and 53.7% of K. pneumoniae isolates were MDR (P < 0.001).
The co-occurrence of β-lactamase genes in E. coli isolates was one blaSHV-1/blaNDM-1, and one blaOXA-1/blaNDM-1 isolates. This pattern in K. pneumoniae isolates was one blaSHV-1/blaNDM-1/blaOXA-1, 3 blaOXA-1/blaNDM-1, and 7 blaSHV-1/blaOXA-1 isolates.
Discussion
The emergence of MDR Enterobacterales, particularly ESBLs-producing strains, is responsible for a large rate of nosocomial outbreaks, related to increased morbidity and mortality.17 Drug-resistant strains of E. coli and K. pneumoniae have acquired resistance to most—and in some cases to all antibiotics that are currently available in the clinic. This problem demands looking for novel antibiotics targeting drug-resistant Gram-negative pathogens. Darobactin is an example of the current efforts that showed a reasonable activity against important drug-resistant pathogens, E. coli and K. pneumoniae, including polymyxin-resistant, ESBLs and carbapenem-resistant isolates with a minimum inhibitory concentration (MIC) of 2 μg mL−1.18 The periodic surveillance for knowing the distribution and mechanisms of antibiotic resistance has an important role in preventing and overcoming the risk of complications attributed to ESBL-producing strains.3
In our study, 36.4% of all isolates were ESBL producers with a high rate of antibiotic resistance. Despite the great discrepancy in the rate of ESBLs-producing Enterobacterales, our finding is consistent with the median values (range 13.4% to 69.2%) reported in different uropathogens and regions of Iran.19–22 The variations in the occurrence of ESBL producers can be in account of different infection control measures, infection types and studied population.
Regarding the emergence of ESBL-producing strains, the main concern is the spread of resistance determinants due to the horizontal gene transfer.3 blaTEM, blaSHV, and blaCTX-M are the most frequent ESBLs encoding genes.23 In the present research, the proportion of blaSHV genotype was low and found in 5.5% (2.7% in E. coli vs 14.7% in K. pneumoniae) of isolates. The prevalence of ESBLs genes among Enterobacterales was varied. Previously, the rates of blaSHV containing Enterobacterales with a focus on uropathogenic isolates were reported 12.2% to 54.8% by Iranian authors.24–29 Meanwhile, several authors have shown the global spared of SHV type β-lactamases in uropathogenic Enterobacterales from China,30 India,31 Saudi Arabia,32 Turkey,33 Ukraine,34 and Morocco.35
In our results, 4.1% of uropathogenic Enterobacterales contained blaNDM-1, which to the best of our knowledge, is the first prevalence of this gene in Guilan province (North of Iran). Previously, the most reported origin of NDM-1 producing bacteria belonged to Asian countries, including China, India, Turkey, Pakistan and our neighboring countries in Persian Gulf region.10 Unfortunately, reports point out the increasing emergence of blaNDM-1 harboring Enterobacterales in different regions of Iran. Concerning the emergence of blaNDM-1 harboring Enterobacterales, there are some reports from the Capital (Tehran),6,36,37 central part (Isfahan),7 and southwest (Shiraz) of Iran.10
In the present study, the most prevailing β-lactamases encoding genes, generally 16.4% of isolates, and 44.4% of ESBLs-producing isolates were blaOXA-1 positive. Previously, Alizadeh et al, in a study conducted in the southwest of Iran (Kerman), showed that 17.2% of uropathogenic isolates were OXA-1 producers.20 Reviewing global reports such as Brazil (60%),38 Portugal (55%),39 Saudi Arabia (54.8%, and 48.3%),32,40 and Bangladesh (47.5%),41 indicate that the occurrence of OXA-1 β-lactamases can be varied based on type and source of isolates and the prevalence of ESBLs in each region.
The present work has some limitations: firstly, the β-lactamase expression was not assessed by real time-PCR, particularly concerning those isolates genetically positive for investigated genes yet phenotypically β-lactam susceptible. Secondly, other β-lactamases encoding genes reported in other Iranian studies should be further investigated. Finally, the availability of clinical features of the patient populations including treatments and outcomes of treatments could provide important information.
In summary, the prevalence of ESBL-producing uropathogenic Enterobacterales containing NDM-1 β-lactamases could be a major concern in our region. Carbapenems are still effective on our MDR isolates, but the co-occurrence of β-lactamases genes suggests restricted infection control policies and the rational prescription and use of antibiotics.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mehrad B, Clark NM, Zhanel GG, Lynch JP
2. Peleg AY, Hooper DC. Hospital-acquired infections due to gram-negative bacteria. N Engl J Med. 2010;362(19):1804–1813. doi:10.1056/NEJMra0904124
3. Shaikh S, Fatima J, Shakil S, Rizvi SM, Kamal MA. Antibiotic resistance and extended spectrum beta-lactamases: types, epidemiology and treatment. Saudi J Biol Sci. 2015;22(1):90–101. doi:10.1016/j.sjbs.2014.08.002
4. Ebrahim-Saraie HS, Nezhad NZ, Heidari H, Motamedifar A, Motamedifar M. Detection of antimicrobial susceptibility and integrons among extended-spectrum β-lactamase producing uropathogenic Escherichia coli isolates in Southwestern Iran. Oman Med J. 2018;33(3):218–223. doi:10.5001/omj.2018.40
5. Drawz SM, Bonomo RA. Three decades of beta-lactamase inhibitors. Clin Microbiol Rev. 2010;23(1):160–201. doi:10.1128/CMR.00037-09
6. Solgi H, Giske CG, Badmasti F, et al. Emergence of carbapenem resistant Escherichia coli isolates producing blaNDM and blaOXA-48-like carried on IncA/C and IncL/M plasmids at two Iranian university hospitals. Infect Genet Evol. 2017;55:318–323. doi:10.1016/j.meegid.2017.10.003
7. Fazeli H, Norouzi-Barough M, Ahadi AM, Shokri D, Solgi H. Detection of New Delhi metallo-beta-lactamase-1 (NDM-1) in carbapenem- resistant Klebsiella pneumoniae isolated from a university hospital in Iran. Hippokratia. 2015;19(3):205–209.
8. Sadeghi MR, Ghotaslou R, Akhi MT, Asgharzadeh M, Hasani A. Molecular characterization of extended-spectrum beta-lactamase, plasmid-mediated AmpC cephalosporinase and carbapenemase genes among Enterobacteriaceae isolates in five medical centres of East and West Azerbaijan, Iran. J Med Microbiol. 2016;65(11):1322–1331. doi:10.1099/jmm.0.000356
9. Moghadam MN, Motamedifar M, Sarvari J, Sedigh E-S, Mousavi SM, Moghadam FN. Emergence of multidrug resistance and metallo-beta-lactamase producing acinetobacter baumannii isolated from patients in Shiraz, Iran. Ann Med Health Sci Res. 2016;6(3):162–167. doi:10.4103/2141-9248.183946
10. Hosseinzadeh Z, Sedigh Ebrahim-Saraie H, Sarvari J, et al. Emerge of blaNDM-1 and blaOXA-48-like harboring carbapenem-resistant Klebsiella pneumoniae isolates from hospitalized patients in southwestern Iran. J Chin Med Assoc. 2017.
11. van Hoek AH, Mevius D, Guerra B, Mullany P, Roberts AP, Aarts HJ. Acquired antibiotic resistance genes: an overview. Front Microbiol. 2011;2:203. doi:10.3389/fmicb.2011.00203
12. Wayne PA. Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute (CLSI); 2016. 26th Informational Supplement.
13. Magiorakos A-P, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
14. Hujer KM, Hujer AM, Hulten EA, et al. Analysis of antibiotic resistance genes in multidrug-resistant Acinetobacter sp. isolates from military and civilian patients treated at the Walter Reed Army Medical Center. Antimicrob Agents Chemother. 2006;50(12):4114–4123. doi:10.1128/AAC.00778-06
15. Doyle D, Peirano G, Lascols C, Lloyd T, Church DL, Pitout JD. Laboratory detection of Enterobacteriaceae that produce carbapenemases. J Clin Microbiol. 2012;50(12):3877–3880. doi:10.1128/JCM.02117-12
16. Sugumar M, Kumar KM, Manoharan A, Anbarasu A, Ramaiah S. Detection of OXA-1 beta-lactamase gene of Klebsiella pneumoniae from blood stream infections (BSI) by conventional PCR and in-silico analysis to understand the mechanism of OXA mediated resistance. PLoS One. 2014;9(3):e91800. doi:10.1371/journal.pone.0091800
17. Giamarellou H. Multidrug resistance in Gram-negative bacteria that produce extended-spectrum beta-lactamases (ESBLs). Clin Microbiol Infect. 2005;11(Suppl 4):1–16. doi:10.1111/j.1469-0691.2005.01160.x
18. Imai Y, Meyer KJ, Iinishi A, et al. A new antibiotic selectively kills Gram-negative pathogens. Nature. 2019;576(7787):459–464. doi:10.1038/s41586-019-1791-1
19. Ghadiri H, Vaez H, Razavi-Azarkhiavi K, et al. Prevalence and antibiotic susceptibility patterns of extended-spectrum ss-lactamase and Metallo-ss-Lactamase-producing uropathogenic Escherichia coli isolates. Lab Med. 2014;45(4):291–296. doi:10.1309/LMHEP4VQHEY2POOK
20. Alizade H, Fallah F, Ghanbarpour R, et al. Genotyping of ESBL producing uropathogenic and diarrheagenic Escherichia coli in southeast of Iran. Infect Disord Drug Targets. 2015;15(2):118–124. doi:10.2174/1871526515666150724113847
21. Shakib P, Ramazanzadeh R, Taherikalani M, Nouri B. Detection of Extended-Spectrum Beta-Lactamases (ESBLs) and antibiotic susceptibility patterns in Klebsiella pneumoniae in Western, Iran. Infect Disord Drug Targets. 2017.
22. Pouladfar G, Basiratnia M, Anvarinejad M, Abbasi P, Amirmoezi F, Zare S. The antibiotic susceptibility patterns of uropathogens among children with urinary tract infection in Shiraz. Medicine (Baltimore). 2017;96(37):e7834. doi:10.1097/MD.0000000000007834
23. Chandramohan L, Revell PA. Prevalence and molecular characterization of extended-spectrum-beta-lactamase-producing Enterobacteriaceae in a pediatric patient population. Antimicrob Agents Chemother. 2012;56(9):4765–4770. doi:10.1128/AAC.00666-12
24. Eftekhar F, Rastegar M, Golalipoor M, Mansoursamaei N. Detection of extended spectrum b-lactamases in urinary isolates of klebsiella pneumoniae in relation to Bla, Bla and Bla gene carriage. Iran J Public Health. 2012;41(3):127–132.
25. Nakhaei Moghaddam M, Forghanifard MM, Moshrefi S. Prevalence and molecular characterization of Plasmid-mediated extended-spectrum beta-lactamase Genes (balaTEM, blaCTX and blASHV) among urinary Escherichia coli clinical isolates in Mashhad, Iran. Iran J Basic Med Sci. 2012;15(3):833–839.
26. Sedighi I, Arabestani MR, Rahimbakhsh A, Karimitabar Z, Alikhani MY. Dissemination of Extended-Spectrum beta-Lactamases and Quinolone Resistance Genes Among Clinical Isolates of Uropathogenic Escherichia coli in children. Jundishapur J Microbiol. 2015;8(7):e19184. doi:10.5812/jjm.19184v2
27. Ranjbar R, Memariani H, Sorouri R. Molecular epidemiology of extended-spectrum beta-lactamase-producing klebsiella pneumoniae strains isolated from children with urinary tract infections. Arch Pediatr Infect Dis. 2017;5(2):e39000.
28. Ghafourian S, Sekawi Z, Neela V, Khosravi A, Rahbar M, Sadeghifard N. Incidence of extended-spectrum beta-lactamase-producing Klebsiella pneumoniae in patients with urinary tract infection. Sao Paulo Med J. 2012;130(1):37–43. doi:10.1590/S1516-31802012000100007
29. Zamani H, Salehzadeh A, Zarrin S. Prevalence of ambler class a extended-spectrum-β-lactamases (ESBLS) among Uropathogenic Escherichia coli strains isolated from Rasht city, Iran. Biosci J. 2017;33(5):1314–1320. doi:10.14393/BJ-v32n1a2016
30. Zhao R, Shi J, Shen Y, et al. Phylogenetic distribution of virulence genes among ESBL-producing uropathogenic Escherichia coli isolated from long-term hospitalized patients. J Clin Diagn Res. 2015;9(7):Dc01–Dc04.
31. Jena J, Debata NK, Sahoo RK, Gaur M, Subudhi E. Molecular characterization of extended spectrum beta-lactamase-producing Enterobacteriaceae strains isolated from a tertiary care hospital. Microb Pathog. 2018;115:112–116. doi:10.1016/j.micpath.2017.12.056
32. Al-Agamy MH, Aljallal A, Radwan HH, Shibl AM. Characterization of carbapenemases, ESBLs, and plasmid-mediated quinolone determinants in carbapenem-insensitive Escherichia coli and Klebsiella pneumoniae in Riyadh hospitals. J Infect Public Health. 2018;11(1):64–68. doi:10.1016/j.jiph.2017.03.010
33. Copur Cicek A, Saral A, Ozad Duzgun A, et al. Nationwide study of Escherichia coli producing extended-spectrum β-lactamases TEM, SHV and CTX-M in Turkey. J Antibiot (Tokyo). 2013;66(11):647–650. doi:10.1038/ja.2013.72
34. Chub OI, Bilchenko AV, Khalin I. Extended spectrum beta-lactamase production in uropathogens isolated from hospitalized patients with chronic pyelonephritis. Open Urol Nephrol J. 2015;8:71–75. doi:10.2174/1874303X01508010071
35. El Bouamri MC, Arsalane L, Zerouali K, Katfy K, El Kamouni Y, Zouhair S. Molecular characterization of extended spectrum β-lactamase-producing Escherichia coli in a university hospital in Morocco, North Africa. Afr J Urol. 2015;21(3):161–166. doi:10.1016/j.afju.2015.02.005
36. Nobari S, Shahcheraghi F, Rahmati Ghezelgeh F, Valizadeh B. Molecular characterization of carbapenem-resistant strains of Klebsiella pneumoniae isolated from Iranian patients: first identification of blaKPC gene in Iran. Microb Drug Resist. 2014;20(4):285–293. doi:10.1089/mdr.2013.0074
37. Shahcheraghi F, Nobari S, Rahmati Ghezelgeh F, et al. First report of New Delhi metallo-beta-lactamase-1-producing Klebsiella pneumoniae in Iran. Microb Drug Resist. 2013;19(1):30–36. doi:10.1089/mdr.2012.0078
38. Flores C, Romão CMCPA, Bianco K, et al. Detection of antimicrobial resistance genes in beta-lactamase- and carbapenemase-producing Klebsiella pneumoniae by patient surveillance cultures at an intensive care unit in Rio de Janeiro, Brazil. J Bras Patol Med Lab. 2016;52:284–292. doi:10.5935/1676-2444.20160049
39. Oliveira C, Amador P, Prudêncio C, Tomaz CT, Tavares-Ratado P, Fernandes R. ESBL and AmpC β-lactamases in clinical strains of Escherichia coli from Serra da Estrela, Portugal. Medicina (Kaunas). 2019;55(6):272. doi:10.3390/medicina55060272
40. Alyamani EJ, Khiyami AM, Booq RY, Majrashi MA, Bahwerth FS, Rechkina E. The occurrence of ESBL-producing Escherichia coli carrying aminoglycoside resistance genes in urinary tract infections in Saudi Arabia. Ann Clin Microbiol Antimicrob. 2017;16(1):1. doi:10.1186/s12941-016-0177-6
41. Lina TT, Khajanchi BK, Azmi IJ, et al. Phenotypic and molecular characterization of extended-spectrum beta-lactamase-producing Escherichia coli in Bangladesh. PLoS One. 2014;9(10):e108735. doi:10.1371/journal.pone.0108735
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.