")
Back to Journals » International Journal of Women's Health » Volume 12
The Persian Version of Menopause Rating Scale (MRS): A Psychometric Study
Authors Allahverdipour H , Asghari Jafarabadi M , Burri A, Javadivala Z
Received 4 April 2020
Accepted for publication 11 June 2020
Published 25 June 2020 Volume 2020:12 Pages 505—512
DOI https://doi.org/10.2147/IJWH.S249466
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Hamid Allahverdipour,1 Mohammad Asghari Jafarabadi,2,3 Andrea Burri,4 Zeinab Javadivala5
1Research Center of Psychiatry and Behavioral Sciences, Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz, Iran; 2Road Traffic Injury Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 3Department of Statistics and Epidemiology, Tabriz University of Medical Sciences, Tabriz, Iran; 4Institute for Sex Counselling and Sexual Sciences (ISCSS), Zurich, Switzerland; 5Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Zeinab Javadivala
Department of Health Education and Promotion, Tabriz University of Medical Sciences, Tabriz 14711, Iran
+98-411-3344731
Email [email protected]
Objective: Menopause-related symptoms can strongly affect health-related quality of life (HRQOL) in most peri-menopausal women. The aim of the present study was to explore the psychometric properties of a culturally adapted and translated Persian version of the Menopause Rating Scale (MRS).
Study Design: The study was conducted on a random sample of 270 middle-aged women (age range 40– 60 yrs) selected from 25 urban health service centers across Tabriz, Iran. Content validity was evaluated by a panel of 11 experts. Construct validity was assessed by exploratory factor analyses with Varimax rotation and principal axis factoring extraction method and by confirmatory factor analyses. Internal consistency and test–retest reliability were assessed with Cronbach’s alpha and intra-class correlation coefficient (ICC), respectively. In addition, the feasibility of the measure was judged based on ceiling and floor effects.
Results: Content validity of the measure was good with a mean content validity index (CVI) and mean content validity ratio (CVR) of 0.88 and 0.94, respectively. Exploratory factor analyses identified three factors accounting for 47.69% of the variance. Confirmatory factor analyses found the original three-factor model to have the best fit to the data. Cronbach’s alpha coefficient (0.85) and the test–retest reliability score (0.91) indicated good internal consistency.
Conclusion: The Persian version of the MRS demonstrated excellent reliability and validity. It can therefore be used in both clinical and research settings to assess menopause-related symptoms and associated quality of life.
Keywords: Menopause Rating Scale, psychometric, menopause, Persian
Introduction
Menopause is a natural stage of biological changes in every woman’s life.1 Because of increasing life expectancy, women are expected to spend more than three decades of their lives after menopause.2 By 2050, about one-fifth of the global female population will be post-menopausal. Today, based on Population and Housing Censuses conducted in 2016 it is estimated that about 8.5 million 40–64-year-old women are living in Iran.3 By 2020 it is expected that worldwide more than 50 million women will be older than 51 years – which constitutes the average age of menopause.4
It is well documented that the majority of women suffer from menopause-related symptoms which can have adverse effects on health-related quality of life (HRQOL) at a physical, psychological, and urogenital level.5 According to a study conducted by Javadivala et al, hot flashes, mood swings, vaginal dryness, and sleep problems are the most common symptoms associated with menopause in Iranian women.2 The intensity of menopause-related complaints can further range from mild to severe in more than 80% of the women.1,2 Considering a systematic review performed in 2014, prevalence of menopausal symptoms in African women was at the highest level which indicates different expression of symptoms and intensity of symptoms in the diverse cultures by women. Consistently, women from South America complained about discomfort associated with muscle pain and joint aches (84%), occurrence of depressive (82%) and sexual dysfunctions (80%) while among European women, sleep hot flashes (97%) and muscle pain and joint aches (95%) were reported more than other symptoms of menopause.6
Various instruments exist that allow the assessment of menopause-related symptoms and their severity.1 One such instrument is the Menopause Rating Scale (MRS) which was developed in the early 1990s in response to the lack of standardized scales to measure the severity of menopausal symptoms and their impact on women’s HRQoL.7 The MRS is a simple self-report questionnaire used to assess the frequency and severity of peri- and post-menopausal symptoms in women.7–9 Its English version has shown excellent psychometric properties and ever since has been translated and validated into more than 27 languages.7–13 Adopting MRS into Persian language would allow identification and assessment of menopause-related symptoms in the Persian-speaking population and compare the prevalence and severity of the symptoms with the figures assessed in other countries. It may further allow the measurement of pre- and post-treatment (eg, hormonal supplement) changes in symptom manifestation and severity. Therefore, the aim of the present study was to translate the English version of the MRS into Persian language and to explore the psychometric properties of this translated and culturally adapted version.
Methods
Participants
This study was conducted in Tabriz City, Iran, between September and October 2017. It has been suggested that 5 or more participants per item provide sufficient statistical power to conduct factor analysis.14,15 Thus, considering 10 samples per item, for an 11-item instrument, a total of 110 participants are required. Considering a design effect of 1.5 (to cover the cluster random sampling design effect) and an attrition rate of 80%, finally 300 middle-aged women were recruited from 25 urban health service centers in Tabriz city which represents an adequate sample size. In each center, a proportion to the population size meeting the eligibility criteria were randomly selected using random numbers table. Since the population under coverage of each center were approximately equal, twelve women were chosen from each health center. The inclusion criteria were being between 40 and 60 years old, being peri- or post-menopausal according to the Stages of Reproductive Aging Workshop (STRAW) criteria, and willingness to participate in the study. Exclusion criteria were having a past history of or currently being treated for any type of cancer, being treated for a psychiatric condition, and/or receiving hormone replacement therapy. According to STRAW, perimenopause is characterized by a woman having regular menstrual cycles with interval changes of 7 days or more and/or two or more skipped menstrual cycles and at least one inter-menstrual interval of 60 days or more. Post-menopause is defined as the stage reached when 12 months have passed since the final menstruation.
Once potential participants meeting the inclusion criteria had been selected, three trained researchers attended the participants’ homes, and performed home-based interviews to collect demographic information and fill in the Persian version of MRS. Eventually 270 women agreed to participate in the present study (90% of the women that had been approached by the principal investigator). The test–retest was conducted with a 2-week interval in a same population (n=68) and the intra-class correlation coefficient was computed along with its 95% confidence interval. Informed consent was obtained from all study participants before collecting the information. The study was approved by the Ethical Committee, Tabriz University of Medical Sciences, Tabriz, Iran (code number = # TBZMED. 1394.735).
MRS
The MRS is an 11-item, self-report questionnaire that captures three subdomains: (a) somatic symptoms: hot flashes, heart discomfort/palpitation, sleeping problems and muscle and joint problems; (b) psychological symptoms: depressive mood, irritability, anxiety and physical and mental exhaustion; (c) urogenital symptoms: sexual problems, bladder problems and dryness of the vagina. Responses are scored from “0” (no symptom) to “4” (very severe symptom expression).7 The total scores for each of the subdomains can be computed by adding up each item of the respective subscale.
Design and Item Generation
A forward-backward translation procedure was chosen to translate the questionnaire into Persian language.16 In the first step, the English questionnaire was translated into Persian independently by two bilingual translators. Following this, the Persian version was back-translated into English by a health education expert and a reproductive health/gynecology science specialist – both fluent in both languages. Both backward translators were unfamiliar (ie, blinded) with the English version of the MRS. After forward and backward translation, all translators created a final, consolidated version.
This preliminary final version was then evaluated and revised by an expert panel consisting of four health education scholars, two psychologists, and five midwives with clinical experience in dealing with menopause and related issues. The panel members were asked to review and assess the items and to evaluate the relevance and appropriateness of the items for the research target group. The panel was also responsible for the evaluation of the response formats of the translated scale. The resulting version of the translated MRS was then tested in a small sample of Persian-speaking women (n=30) who were asked to provide feedback on this MRS version. Based on the responses, a final consolidated Persian version of the MRS was obtained.
Content Validity
For the assessment of the content validity of the MRS two indicators – the content validity index (CVI) and the content validity ratio (CVR) – were calculated by a panel of 10 experts who were not part of the previous expert panel responsible for the questionnaire translation.17 The content validity index assesses the relevance, simplicity, and clarity of each item in relation to the construct assessed by the instrument. The experts further assessed the relevance of the items using a 4-point rating scale: a) not relevant; b) slightly relevant; c) relevant; and d) completely relevant. A CVI of ≥ 0.79 was considered satisfactory for each statement. The content validity ratio assesses the necessity of each item. For evaluating the necessity of each item to be included in the questionnaire we used a question with a 3-point response rating scale (“necessary”, “useful but unnecessary”, “and unnecessary”).15–17
Face Validity
The same expert panel also conducted the qualitative assessment of each questionnaire item in terms of ambiguity, relevance, and difficulty. They assessed the face validity of the items and scored the importance of each item based on a 5-point rating scale. For face validity, an impact score (frequency× importance) was calculated. The score indicates the proportion of the expert panel who considers the item to be important or quite important. Those items associated with an impact score ≥ 1.5 (which corresponds to a mean frequency of 50% and a mean importance of 1.5 on the 5-point Likert scale) were considered appropriate.18
Reliability
Analysis techniques to assess reliability included the examination of Cronbach’s alpha for internal consistency and test-retest to evaluate the stability of the questionnaire using intraclass correlation coefficients (ICCs) after a two-week interval.
Statistical Analyses
The statistical package for social sciences (SPSS) (v. 17 for Windows) and AMOS (v. 17; SPSS Inc., Chicago, IL, USA) were used to perform all statistical analyses. Normality of the data distribution was confirmed by conducting one-sample Kolmogorov–Smirnov tests. A P-value less than 0.05 was considered significant unless stated otherwise. The range of measurement was examined by computing ceiling (the maximum possible score) and floor (the minimum possible score) effects. Ceiling and floor effects are considered to be present if more than 13% of participants report the lowest or highest possible total score.19
Exploratory factor analysis (EFA) was used for structure detection.13 The purpose of structure detection is to examine the underlying (or latent) relationships between the variables. Exploratory factor analysis was carried out by principal axis factoring (PAF) extraction method with varimax rotation and kaiser normalization. The scree plot procedure was used for deciding on the number of factors to be extracted. KMO (Kaiser-Meyer- Olkin) measure of sampling adequacy, Bartlett’s test of sphericity, and total variance explained were used for the evaluation of model fit. High values of KMO (> 0.7) generally indicate a good fit. Bartlett’s test of sphericity was conducted to test the hypothesis that a correlation matrix is an identity matrix, indicating that variables are unrelated and therefore unsuitable for structure detection. Values < 0.05 of the significance probability indicate a satisfactory factor analysis. Items with factor loadings of > 0.3 were included in the final model. Confirmatory factor analysis (CFA) was conducted to assess how well the EFA extracted model fits the observed data. For this, the absolute model fit was evaluated using the Chi-Square statistic, comparative fit index (CFI), Tucker–Lewis index (TLI), and root-mean-square error of approximation (RMSEA). The model was considered to be acceptable if normed chis-square (Chi2/df) was in the range of 1–5, CFI was more than 0.8, TLI was greater than 0.9, and RMSEA was < 0.05 or between 0.05 and 0.08.20
Results
Participants
The mean age of participants was 50 years (SD=5.1), ranging from 40 to 60 years. The mean age of menopause was 47.2 years (SD=5.4). About 126 (46%) women were postmenopausal and 144 (54%) were peri-menopausal (Table 1).
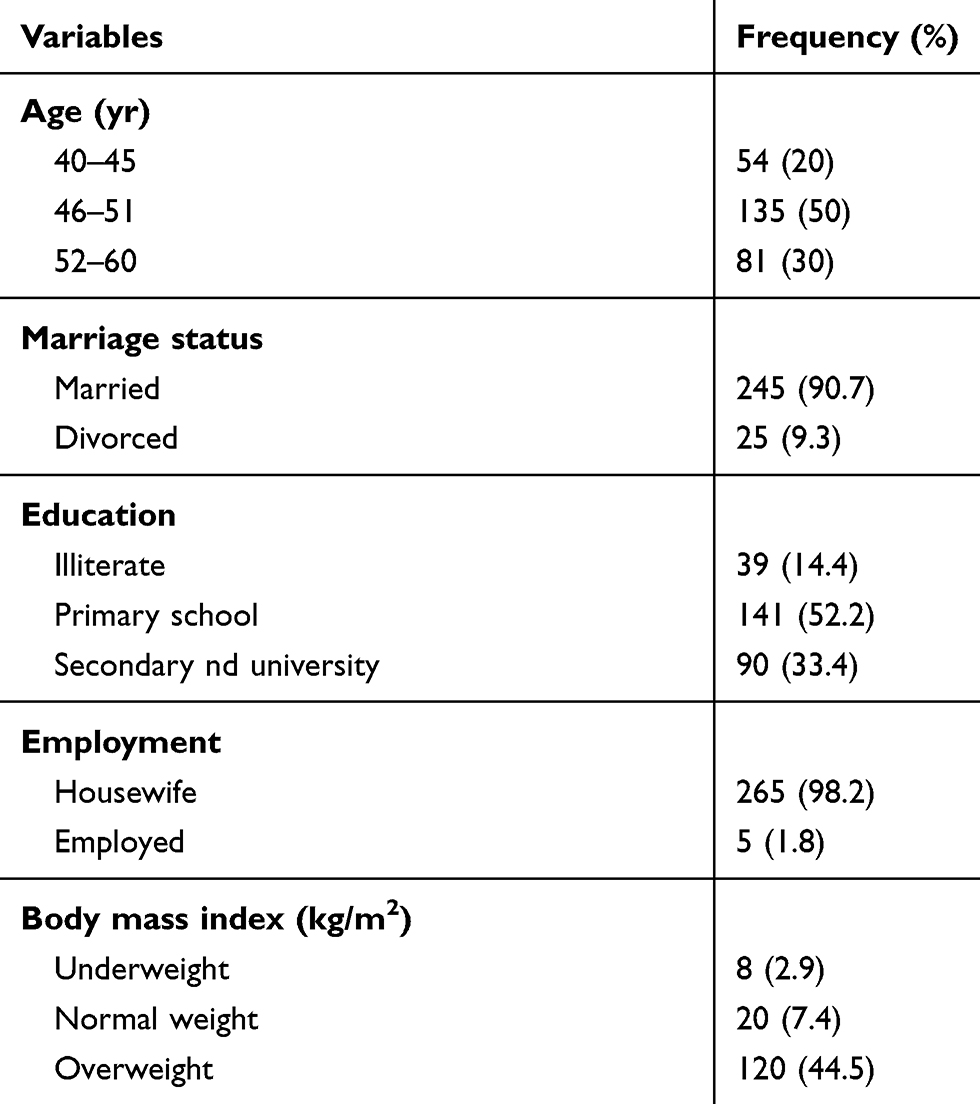 |
Table 1 Demographic Characteristics |
Feasibility
No floor or ceiling effects could be detected for the total score of the Persian version of the MRS scale (Range: 0–44, frequency (%): 17 (6.2%) – 2 (0.7%)), supporting the feasibility of the instrument.
Content Validity
The impact score for face validity was greater than 1.5 for all items of the MRS and both the CVI and CVR ranged between 0.80 and 1.00. Consequently, no items were deleted (Table 2). Furthermore, the expert panel confirmed the clarity and relevance of the wording and phrasing of the translated MRS items.
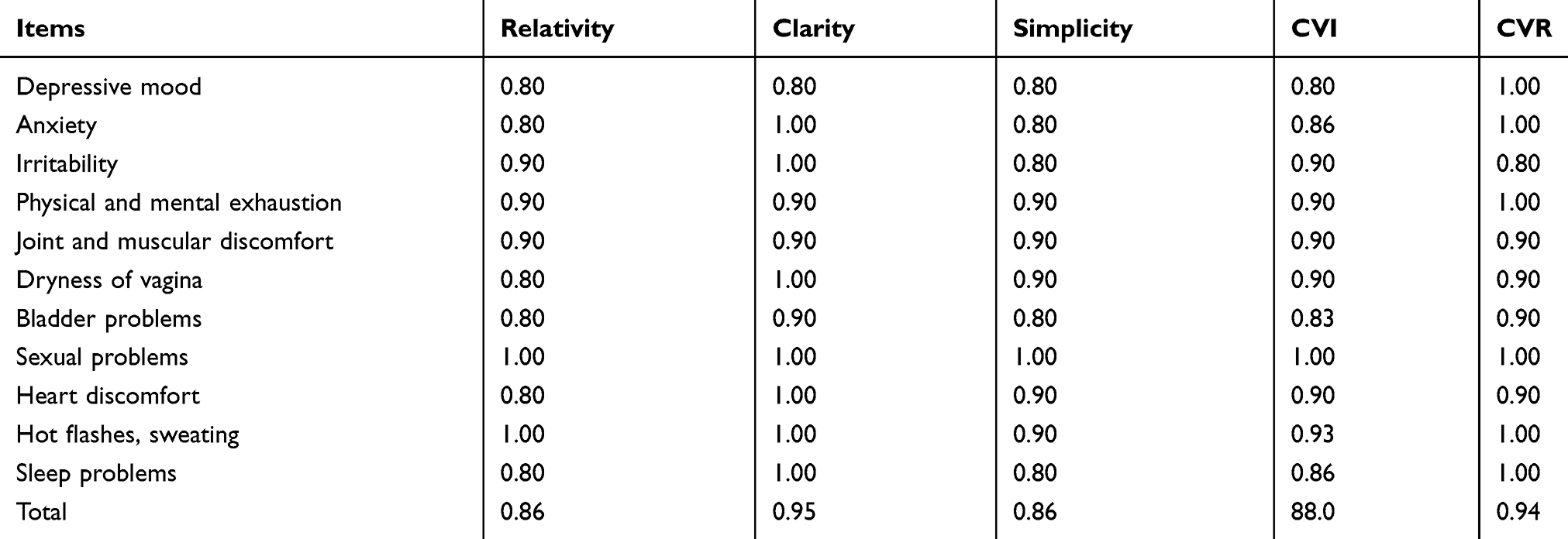 |
Table 2 The Scores of Relevancy, Clarity, Simplicity, CVI and CVR for MRS |
Factor Structure
KMO measure of sampling adequacy as well as the Bartlett’s test of sphericity was 0.89 for the constructs (approx. Chi-square = 858.03, df = 55, p<0.001). After principal axis factor analysis with Varimax rotation, three factors with eigenvalues greater than 1 could be extracted, which altogether accounted for 47.69% of the total variance (Table 3). However, joint and muscular discomfort has changed its factorial belonging from somatic (Rotated factor pattern coefficients: −0.365) to urogenital (Rotated factor pattern coefficients: 0.617). We found the measured model to have a good fit to the data in the assumed model according to the calculated fit indices (Chi2: 52.58; DF: 41; normed Chi2=Chi2/DF: 1.28; GFI: 0.97; AGFI: 0.94; CFI: 0.99; NFI: 0.95; TLI: 0.98; RMSEA: 0.03 (0.0–0.06)) (Figure 1). In addition, significant correlations between the psychological domain with the urogenital domain (r=0.65, p<0.001), the psychological domain with the somatic domain (r= 0.77; p < 0.001) and the somatic domain with the urogenital domain could be found (r= 0.70, p < 0.001). (Joint and muscular discomfort) has changed its factorial belonging (from somatic to urogenital)
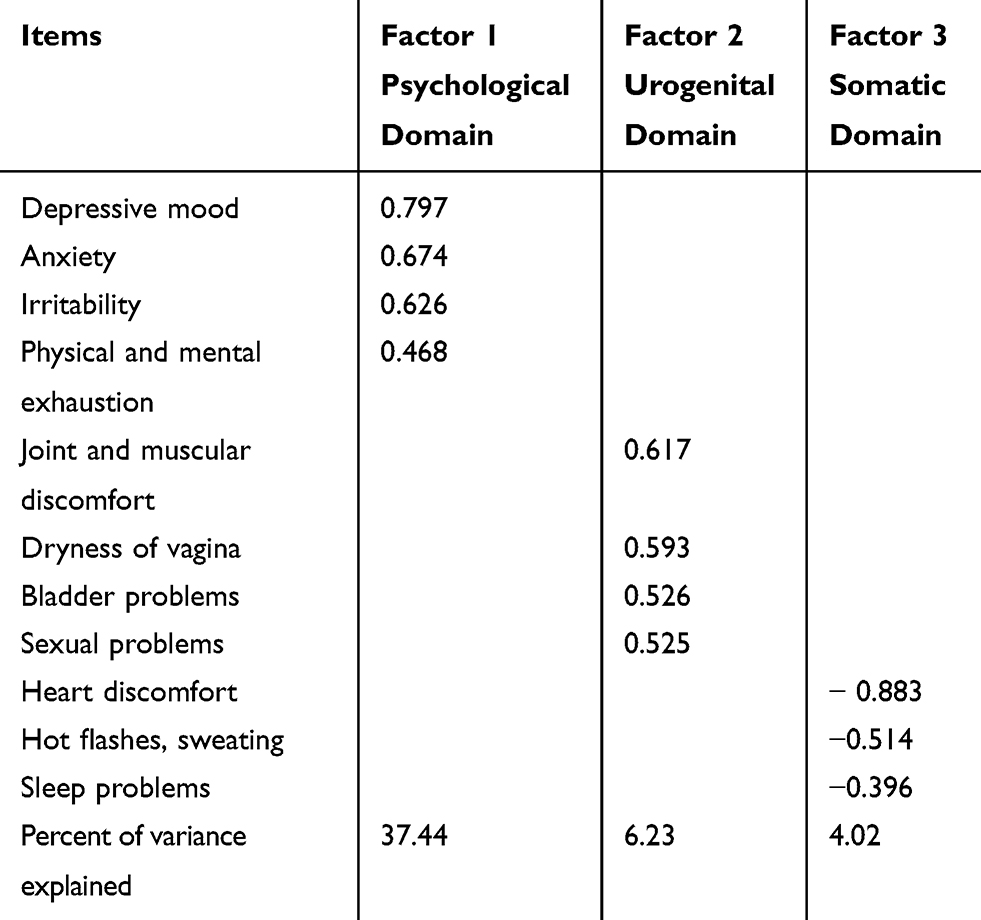 |
Table 3 Rotated Factor Pattern Coefficients for Variable Solutions (11 Items) of the Factors |
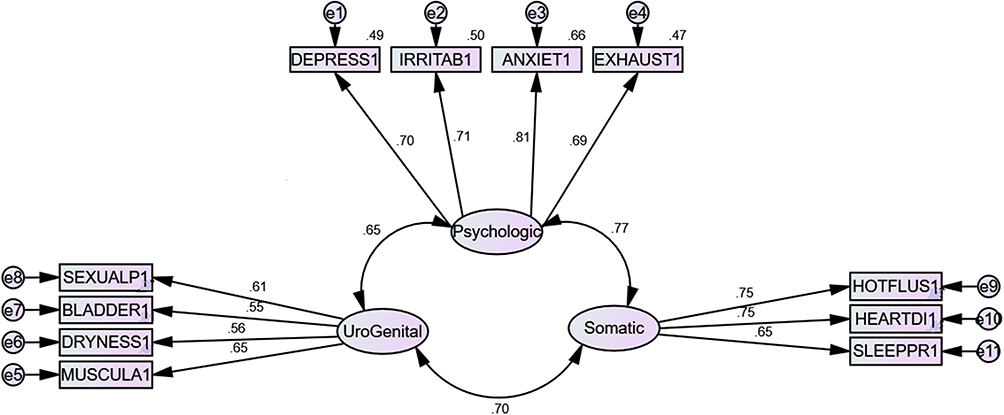 |
Figure 1 CFA-based relations between the items and the factors and between the factors. All the relations between the factors and the items and between the factors were statistically significant (all p<0.05). |
Internal Consistency and Reliability
Cronbach’s alpha was 0.85, indicating good internal consistency of the MRS and its domains (Table 4). According to the ICC listed in Table 4, the MRS also showed good test-retest reliability.
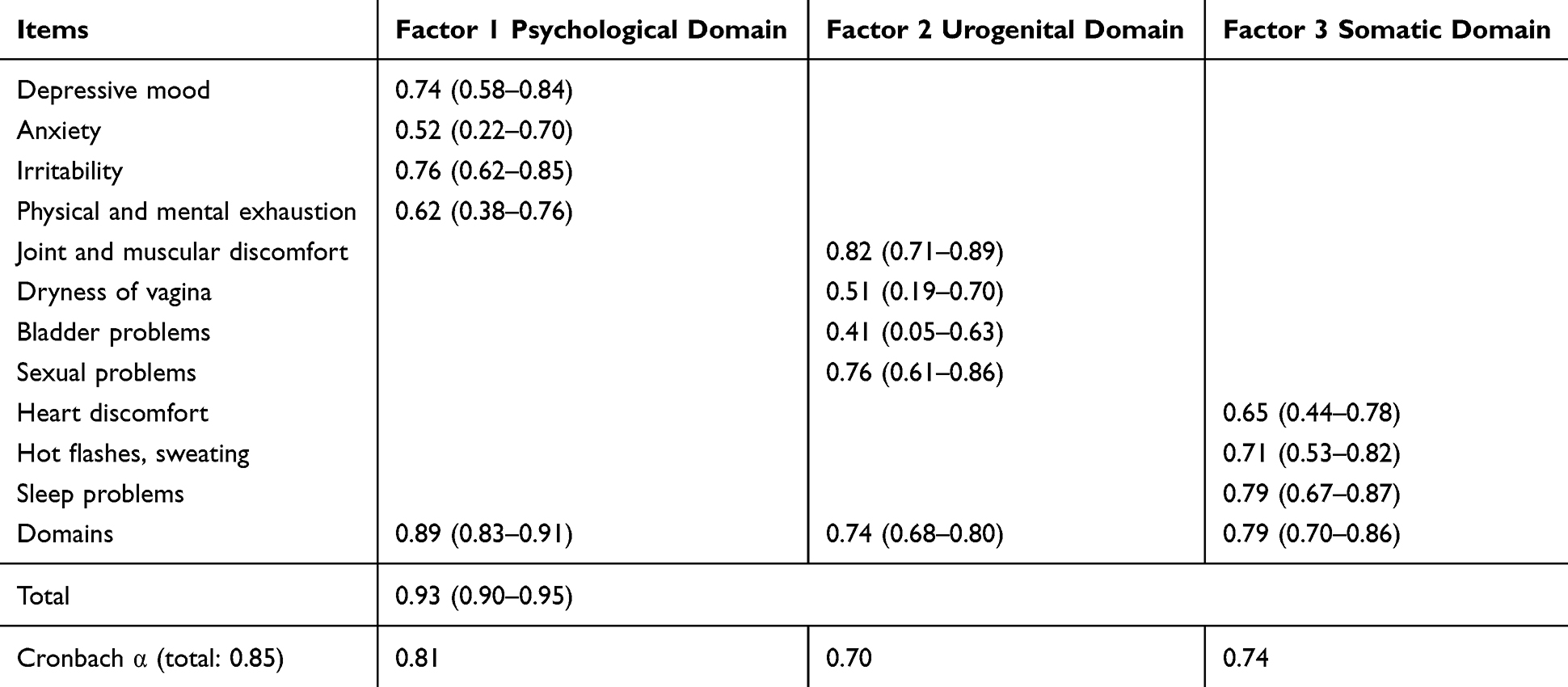 |
Table 4 Item-Level Intraclass Correlation Coefficients and Cronbach’s Alpha for MRS |
Discussion
The main purpose of the present study was to evaluate the psychometric properties of the translated and culturally adapted version of the MRS for the assessment of menopause-related symptoms in Persian-speaking women. Overall, our findings show the Persian version of the scale to have good validity and high reliability. The translated questionnaire version further showed good feasibility and content validity, reflected in the fact that menopausal Iranian women did not find any question unnerving or inconvenient. The sample further confirmed the clarity and relevance of the wording and phrasing of the MRS items within the context of the Iranian culture.
The good reliability found for the total score of Persian version of the MRS (Cronbach’s alpha = 0.85) is in agreement with findings from other countries/cultures (range between 0.6 and 0.9) such as Nepal (0.77), Czech (0.87) and Serbia (0.88).8–10 Moreover, for all MRS domains good internal consistencies, with Cronbach’s alpha coefficients above 0.7 could be detected. The highest coefficient was found for the psychological domain (0.81) and the lowest for the urogenital domain (0.70). Again, this is similar to the validation results of the Chinese, Serbia and US MRS versions where Cronbach’s alpha coefficients for the psychological domain were consistently above 0.80 and lower for the urogenital domain.7,10,11 In addition, we found a high test–retest reliability score (0.91) which is also in line with the previously reported stability of the scale and its subscales, with scores ranging from 0.8 to 0.96 (ref). Again, the highest ICC was found for the psychological (0.84) and the lowest for urogenital domain (0.74).
We detected a very clear three-factor structure, altogether accounting for 47.69% of the total variance. This is somewhat in accordance with the results of the factor analyses conducted in the validation study of the English questionnaire which also found three dimensions explaining 58.8% of the total variance. Similar results were obtained for other translated and culturally adapted questionnaire versions.7 In the present study, the effects of the psychological and urogenital factors were very strong, together explaining more than 44% of the total variance.
Apart from the difference in prevalence of menopausal symptoms across countries and cultures, the list and expression of complaints/symptoms seem to vary as well based on women’s perception.7 Our findings showed that the items pertaining to the subdomain of “joint and muscular discomfort/ pain“ loaded on the “urogenital domain”, while in the previous validation studies these items loaded on the somatic domain. We assume that there might be a robust correlation between the perception of ”joint and muscular discomfort/pain” and urogenital (dryness of vagina, bladder problems, and sexual problems) symptoms among Iranian women. Indeed, have previous studies such as the one by Areskoug-Josefsson (2009) found a relationship between muscular discomfort/ pain and sexual problem.21 In addition, other findings have revealed that joint and muscular discomfort/ pain increase sexual problem among men and women,22 and in the study among Iranian menopausal women, participants explicitly reported the existence of bodily pain alongside adverse effects on sexual desire and a decrease in their sexual motivation.5 Also according to previous validation studies conducted in the USA, Spain, Mexico and Brazil, there seems to be a slight overlap between the three MRS domains.7
Limitations
Although the generalizability of our results is given due to the random selection of the data collection settings, cultural diversity of the Persian-language populations in Iran as well as conducting the study exclusively in urban areas may have affected the generalization of the results. Hence, the applicability of the validated scale in other Persian-language communities of different ethnicities and/or living in rural areas may be restricted and needs to be addressed in future studies. Future research should consider using a more heterogeneous sample of Persian-speaking female populations. We further did not consider any co-morbidities which may have affected the perception of menopausal symptoms in the participants. Although our sample were both peri and post-menopausal women, we did not find any significant differences in the frequency of post-menopausal and peri-menopausal symptoms. Therefore, the accuracy and applicability of the scale were not tested individually in peri-menopausal and post-menopausal women. Moreover, we were unable to establish convergent and divergent validity by comparing the MRS to other generic HRQOL and depression scales due to the unavailability of the data.
Conclusions
We found the culturally adapted and translated Persian version of the MRS to have good content validity and high reliability. The scale can therefore be applied in a clinical and/or research setting to assess menopause-related symptoms in Persian-speaking women.
Abbreviations
MRS, Menopause Rating Scale; HRQOL, Health-related quality of life; EFA, exploratory factor analyses; CFA, confirmatory factor analyses; ICC, intra-class correlation coefficient; CVI, content validity index; CVR, content validity ratio; KMO, Kaiser-Meyer-Olkin; TLI, Tucker–Lewis index; RMSEA, root-mean-square error of approximation.
Data Sharing Statement
At present, data are not freely available (however available on request) for the reason that we are still writing up papers for publication as well as a new project building on this dataset.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The ethics committee at Tabriz University of Medical Sciences (Ethics Code: A/131) approved this protocol. Informed written consent was obtained from all the participants before the interviews.
Consent for Publication
Informed written consent was obtained from all the participants before the interviews.
Acknowledgments
The researchers appreciate the health-care centers and the women who participated in the study.
Author Contributions
All authors read and approved the final manuscript. All authors made contributions to conception and design, acquisition of data, or analysis and interpretation of data; All authors analyzed and wrote the manuscript and revised it critically for important intellectual content and edited the manuscript. Finally, all authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Javadivala Z, Merghati-Khoei E, Asghari-Jafarabadi M, et al. Efficacy of pharmacological and non-pharmacological interventions on low sexual interest/arousal of peri- and post-menopausal women: a meta-analysis. Sex Relation Ther. 2018. doi:10.1080/14681994.2018.1446515
2. Javadivala Z, Kousha A, Allahverdipour H, Asghari Jafarabadi M, Tallebian H. Modeling the relationship between physical activity and quality of life in menopausal-aged women: a cross-sectional study. J Res Health Sci. 2013;13(2):168–175.
3. Moghasemi SP, Ozgoli GP, Ahmadi FP, Simbar MP. Sexual experience of Iranian women in their middle life: a qualitative approach. Int J Community Based Nurs Midwifery. 2018;6(1):47–55.
4. Keefe DL, Wright KP. Chapter 2 – Reproductive Physiology, in General Gynecology. Sokol AI, Sokol ER, Editors. Philadelphia: Mosby; 2007:21–41.
5. Javadivala Z, Merghati-Khoei E, Underwood C, Mirghafourvand M, Allahverdipour H. Sexual motivations during the menopausal transition among Iranian women: a qualitative inquiry. BMC Women’s Health. 2018;18(1):191. doi:10.1186/s12905-018-0684-z
6. Makara-Studzińśka MT, Kryś-Noszczyk KM, Jakiel G. Epidemiology of the symptoms of menopause - an intercontinental review. Przeglad Menopauzalny = Menopause Rev. 2014;13(3):203–211. doi:10.5114/pm.2014.43827
7. Heinemann K, Ruebig A, Potthoff P, Schneider HP, Strelow F, Heinemann LA. The Menopause rating scale (MRS) scale: a methodological review. Health Qual Life Outcomes. 2004;2(1):45. doi:10.1186/1477-7525-2-45
8. Moravcová M, Mareš J, Ježek S. Menopause rating scale–validation Czech version specific instrument for assessing health-related quality of life in postmenopausal women. Ošetrovatelství a Porodní Asistence. 2014;5(1):36–45.
9. Baral G. Menopause rating scale: validation and applicability in Nepalese Women. J Nepal Health Res Counc. 2019;17(42):9–14. doi:10.33314/jnhrc.1770
10. Gazibara T, Dotlic J, Kovacevic N, et al. Validation of the menopause rating scale in Serbian language. Arch Gynecol Obstet. 2015;292(6):1379–1386. doi:10.1007/s00404-015-3743-9
11. Wang XY, Yang HY, Nie GN, et al. [Study on the reliability and validity of the Chinese Menopause Rating Scale (CMRS)]. Zhonghua Liu Xing Bing Xue Za Zhi= Zhonghua Liuxingbingxue Zazhi. 2008;29(9):882–886. Chinese.
12. Monterrosa-Castro A, Jose Paternina-Caicedo A, Herazo-Acevedo E, Celina Oviedo-Acevedo H, Campo-Arias A. Validity and reliability of menopause rating scale in Colombia Indigenous population. Duazary. 2017;14(1):8–15. doi:10.21676/2389783X.1737
13. Mazhar SB, Rasheed S; Menopause Rating Scale (MRS). A simple tool for assessment of climacteric symptoms in Pakistani women. Ann Pak Inst Med Sci. 2009;5(3):158–161. doi:10.5114/pm.2014.43827
14. Hauser GA, Huber IC, Keller PJ, Lauritzen C, Schneider HP. [Evaluation of climacteric symptoms (Menopause Rating Scale)]. Zentralbl Gynakol. 1994;116(1):16–23. German.
15. Coaley K. An Introduction to Psychological Assessment and Psychometrics. SAGE Publications; 2014.
16. Waltz FC, Strickland OL, Lenz ER. Measurement in Nursing and Health Research: Fourth Edition. Springer Publishing Company; 2010:19–21.
17. Polit DF, Beck CT, Owen SV. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res Nurs Health. 2007;30(4):459–467. doi:10.1002/nur.20199
18. Newton P, Shaw S. Validity in Educational and Psychological Assessment. SAGE Publications; 2014.
19. Jette DU, Warren RL, Wirtalla C. Functional independence domains in patients receiving rehabilitation in skilled nursing facilities: evaluation of psychometric properties. Arch Phys Med Rehabil. 2005;86(6):1089–1094. doi:10.1016/j.apmr.2004.11.018
20. Dianat I, Ghanbari Z, AsghariJafarabadi M. Psychometric properties of the Persian language version of the system usability scale. Health Promot Perspect. 2014;4(1):82–89. doi:10.5681/hpp.2014.011
21. Areskoug-Josefsson K, Oberg U. A literature review of the sexual health of women with rheumatoid arthritis. Musculoskeletal Care. 2009;7(4):219–226. doi:10.1002/msc.152
22. Yazmalar L, Sarıyıldız M, Batmaz İ. Adalimumab tedavisi alan romatoid artritli hastada seksüel disfonksiyon. Dicle Tip Dergisi. 2015;42(2). doi:10.5798/diclemedj.0921.2015.02.0570
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.