")
Back to Journals » International Journal of General Medicine » Volume 14
The Perceptions and Views of Rural Residents Towards COVID-19 Recovered Patients in China: A Descriptive Qualitative Study
Authors Chen D, Song F, Cui N , Tang L, Zhang H, Shao J, Qiu R , Wang D, Wang X , Ye Z
Received 24 November 2020
Accepted for publication 12 February 2021
Published 2 March 2021 Volume 2021:14 Pages 709—720
DOI https://doi.org/10.2147/IJGM.S293368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Dandan Chen,1 Feng Song,2 Nianqi Cui,3 Leiwen Tang,1 Hui Zhang,4 Jing Shao,1 Ruolin Qiu,1 Dan Wang,1 Xiyi Wang,1 Zhihong Ye1
1Zhejiang University School of Medicine, Affiliated Sir Run Run Shaw Hospital, Hangzhou, Zhejiang, People’s Republic of China; 2Yunnan College of Business Management, Medical Faculty, Kunming, Yunnan, People’s Republic of China; 3The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 4Guizhou Provincial People’s Hospital, Department of Cardiology, Guiyang, Guizhou, People’s Republic of China
Correspondence: Zhihong Ye
Affiliated Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, 3 East Qingchun Road, Hangzhou, Zhejiang, 310016, People’s Republic of China
Tel +86 136 0661 2119
Email [email protected]
Introduction: With the effective treatments of novel coronavirus disease 2019 (COVID-19), thousands of patients have recovered from COVID-19 globally. The public perceptions and views are vital to facilitate recovered COVID-19 patients reintegrate into society. In China, the rural population accounts for nearly 70% of the total population. Therefore, we chose to evaluate perceptions and views of rural residents towards COVID-19 recovered patients in China.
Methods: Fifteen participants were sampled from a village with the severe COVID-19 epidemic in Zibo city, Shandong Province. The fifteen participants who lived in the village with COVID-19 recovered patients were included. They were over 18 years of age and were voluntary to participant in the study. A descriptive qualitative design using semi-structured telephone interviews was undertaken. Thematic analysis was undertaken.
Results: Five main themes emerged from the data: (1) Perceived personal characteristics of COVID-19 recovered patients; (2) Perceived difficulties faced by COVID-19 recovered patients; (3) Perceptions on the social relationship with COVID-19 recovered patients; (4) Views on COVID-19 recovered patients going to public venues; (5) Views on helping COVID-19 recovered patients. Each theme was supported by several subthemes.
Conclusion: Our study showed that discrimination and reduced social intimacy exist among rural residents. To improve their views or the situation, relevant departments could lead health educational programs and encourage supportive social connections. Through these strategic messaging, rural residents are expected to recognize that COVID-19 recovered patients need more social support, rather than discrimination and resistance, which helps recovered patients better return to society.
Keywords: rural residents, perceptions, views, COVID-19 recovered patients, China
Introduction
While novel coronavirus disease 2019 (COVID-19) patients have skyrocketed in the world, thousands of patients have recovered from COVID-19 globally with the effective treatments of COVID-19. In China, a total of 78,509 COVID-19 patients were discharged as of July 3, 2020.1 When patients recovered and expected to return to normal life, many of them had long-term physical symptoms such as residual respiratory symptoms, and experienced psychosocial difficulties such as employment and financial problems,2,3 which contributed to suicidal behavior.4 Besides, Wu et al,3 reported that approximately 10% of COVID-19 recovered patients were anxious and depressed, because of respiratory residual symptoms after discharge, fear of recurrence, and infection to others. Therefore, COVID-19 recovered patients suffered from enormous physiological and psychological health issues.
COVID-19 was found to be a distinct clade from the betacoronaviruses related to human severe acute respiratory syndrome (SARS).5 A previous study showed that SARS survivors were stigmatized by the general public.6 Furthermore, SARS survivors had considerable difficulties in resuming their normal life due to general people’s discrimination.7 Therefore, public attitudes play a vital role in prompting SARS survivors to reintegrate into society. Similarly, public attitudes may have significant impacts on COVID-19 recovered patients. Given that, it was also imperative to know the public attitudes towards COVID-19 recovered patients.
To our knowledge, most studies investigated the knowledge, attitudes, and practices of residents or the public towards COVID-19.8–10 However, no relevant research on the public attitudes towards COVID-19 recovered patients has been reported in the current epidemic situation of COVID-19. In China, the rural population accounts for nearly 70% of the total population.11 Because of uneven levels of education and limited access to news, many rural residents negatively responded to the epidemic.12 Therefore, the perceptions and views of rural residents towards COVID-19 recovered patients deserve our special attention and penetrating research. In this context, this study took rural residents in a village in Shandong Province as the research objects to evaluate their perceptions and views towards recovered patients from COVID-19 in China. It was through exploring how rural residents viewed COVID-19 recovered patients that we would understand how to change residents’ behaviors13 and providing public health agencies with a reference in determining the knowledge required to underpin the necessary educational programs.14 Above these initiatives will contribute to the reintegration of individuals into society.
Methods
We employed a qualitative, descriptive study design. When research is aimed at discovering and describing a process, a phenomenon, opinions or views of the participants, a qualitative descriptive design is suitable for this study.15,16 A qualitative descriptive study design can provide comprehensive information on events.17 Moreover, qualitative descriptive studies used the principles of naturalistic enquiry, or investigated a phenomenon in its natural state as much as possible.17,18 Therefore, a descriptive qualitative method was employed to explore the perceptions and views of rural residents towards COVID-19 recovered patients. The study was performed according to the Standards for Reporting Qualitative Research (SRQR) (Supplementary file 1).1,19 1 The thematic analysis was used to elicit perceptions and views of rural residents towards COVID-19 recovered patients.
Setting, Sampling and Participants
The study was conducted in a village, Zibo city, Shandong Province, China. The village has a population of about 4000 and covers an area of about 2 square kilometers. Most of the people in this village are Han nationality and over 50 years old. The 10 individuals in the village had been diagnosed with COVID-19, and one of whom had died and the remaining 9 individuals recovered from COVID-19. Because the residents of the village live close and have access to news reports about COVID-19, it is not difficult for them to know who were COVID-19 recovered patients.
Given the above situation, we distributed a recruitment advertisement to these residents via WeChat, which is the most frequently used social media platform in China. A total of 52 individuals responded to the recruitment advertisement. A purposive sampling procedure20 was used to recruit participants of different gender, age, education level, and income among the responded individuals, to obtain rich information. Those residents, who were over 18 years of age, knew who had been treated for COVID-19 and were voluntary to participant in the study, were included. Those residents, who had severe diseases, or were COVID-19 recovered patients or were unable to communicate effectively, were excluded. The reason they could not be included was that their participation would affect the quality of the interview. The participation was confidential and other residents did not know who participated in the study.
Research Team and Reflexivity
A total of ten researchers participated in the present study. Most of them were Ph.D. candidates in health education and chronic disease management in qualitative research. All members of our research team have participated in qualitative research workshops several times, which has improved the understanding of descriptive qualitative research designs. Before the interviews started, the researchers and participants had established a close relationship, which was conducive to performing the study.
Data Collection
Electronic informed consent was obtained before starting the interview with participants. The semi-structured one-on-one in-depth interviews were conducted from February 20, 2020 to April 2, 2020. The method is conducive to a deep understanding of the inner world of the subjects.21 Due to the COVID-19 epidemic, the village was imposed a comprehensive quarantine. Therefore, all participants chose to be interviewed by telephone at home. All interviews were audio-recorded and ranged from 18~60 minutes. The first author (CDD), who was a Ph.D. candidate in nursing, interviewed the participants. The interview environments were quiet, and interruptions were minimized. When the researcher interviewed participants, no one else was present. The expert panel (YZH, CDD, SF and TLW) created an interview guideline (Supplementary file 2). The questions were open-ended. With the permission of the participants, the interviews were digitally recorded using a handheld recorder. The researchers (CNQ, ZH, QRL, and WD) transcribed verbatim audio materials in Chinese, and the first authors (CDD) and the second (SF) encoded within 24 hours. Data collection and analysis were conducted simultaneously, which helped researchers identify thematic saturation. Thematic saturation occurred with the 12th villager. To confirm thematic saturation, 3 additional villagers were interviewed. However, these additional interviews did not bring out new themes. The interview concluded when data saturation was achieved.22
Data Analysis
Inductive thematic analysis methods were used to identify codes, concepts, and patterns, analyze and synthesis material to form themes from the data.18,23 This technique was chosen because it offered a flexible method to gain a rich and detailed account of data.24 The themes and subthemes were derived from the data rather than from existing theoretical or conceptual frameworks.25 CDD and SF immersed in the transcripts and independently read and reread the transcripts and interview notes to get familiar with them. We developed broad codes from these transcripts and refined and synthesized these codes to produce the themes and subthemes. The risk of researcher bias was reduced by the multi-coding approach.26 Discussions with the co-researchers (QRL, ZH, WD and TLW) continued until a consensus was reached on the final themes and subthemes.23 We ensured the trustworthiness of the present study by enhancing its credibility, transferability, dependability and confirmability.27 We addressed the credibility of the entire transcripts by checking all transcripts for accuracy by two researchers (CDD and ZH). Two independent qualitative researchers (YZH and CNQ) verified the findings of the interview data analysis to augment the data consistent. Further, we repeated and clarified information with participants after the interview. The dependability of this study was upheld by descriptions of the participants’ characteristics, contexts and verbatim quotes, which would enable the readers to make judgments about the transferability of the results. The transcripts were cross-checked by the people who were not participated in the transcription process to ensure dependability and confirmability (SJ, and WXY).
Ethical Consideration
The study received ethics approval from Yunnan College of Business Management (2020062). We received the electronic informed consents from all participants before the interviews began. The participants were informed about the confidentiality of their data, and all the interview materials were securely stored. Participants could choose to refuse to answer any question and withdraw at any time without repercussion. Our study complied with the Declaration of Helsinki. The participants provided informed consent for the publishing of anonymized responses.
Results
Demographic Profile
Demographics are presented in Table 1. Fifteen participants were interviewed, and the participant selection process is showed in Figure 1. Participants varied in terms of age, gender, marital status, religion, educational levels and personal monthly income. There were four males and eleven females, and the age ranged from 22 years to 68 years. Eleven people married and only one had religious beliefs. Thirteen people were under undergraduate degree and the personal monthly income level of 0~1000 accounted for the largest proportion of participants.
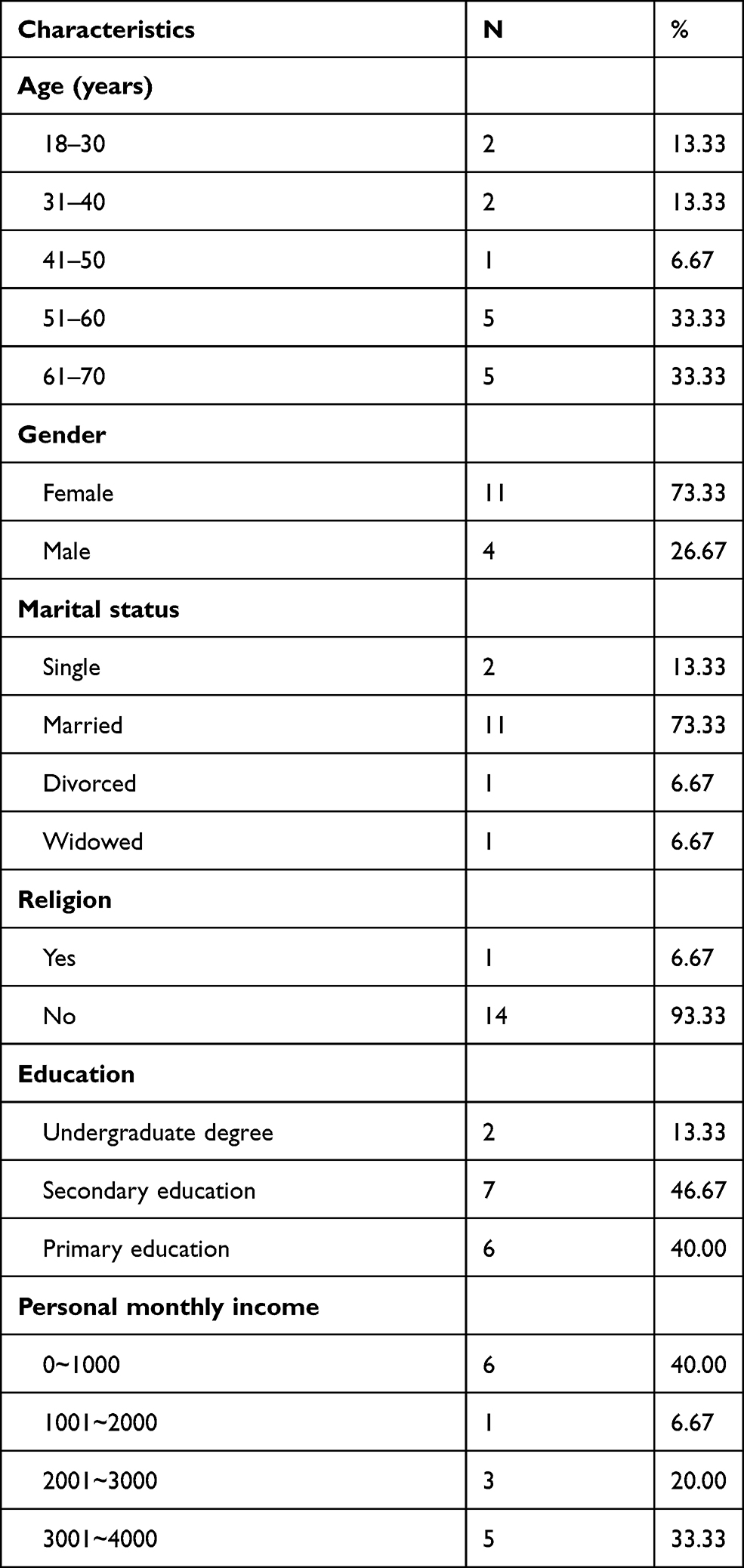 |
Table 1 Characteristics of the Study Population (N=15) |
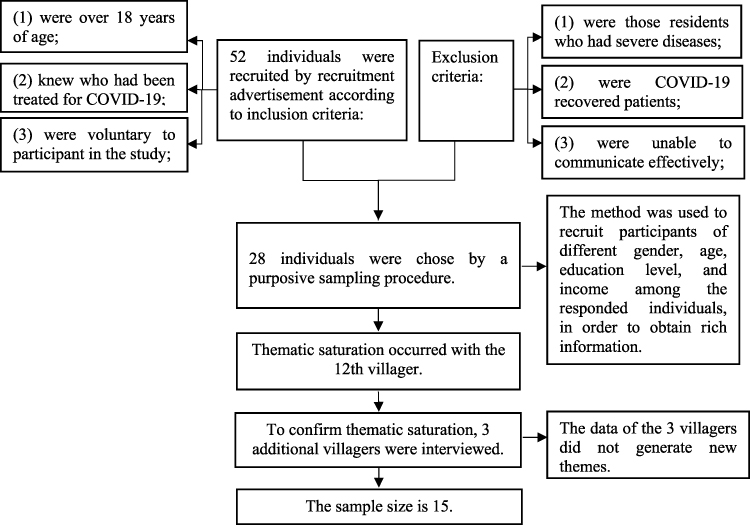 |
Figure 1 Flow chart of participant selection process. |
Qualitative Findings
Five themes emerged from the interview narratives: (1) Perceived personal characteristics of COVID-19 recovered patients; (2) Perceived difficulties faced by COVID-19 recovered patients; (3) Perceptions on the social relationship with COVID-19 recovered patients; (4) Views on COVID-19 recovered patients going to public venues; (5) Views on helping COVID-19 recovered patients. Additionally, interview data were given to illustrate these themes emerging during the analysis. (Table 2).
 |
 |
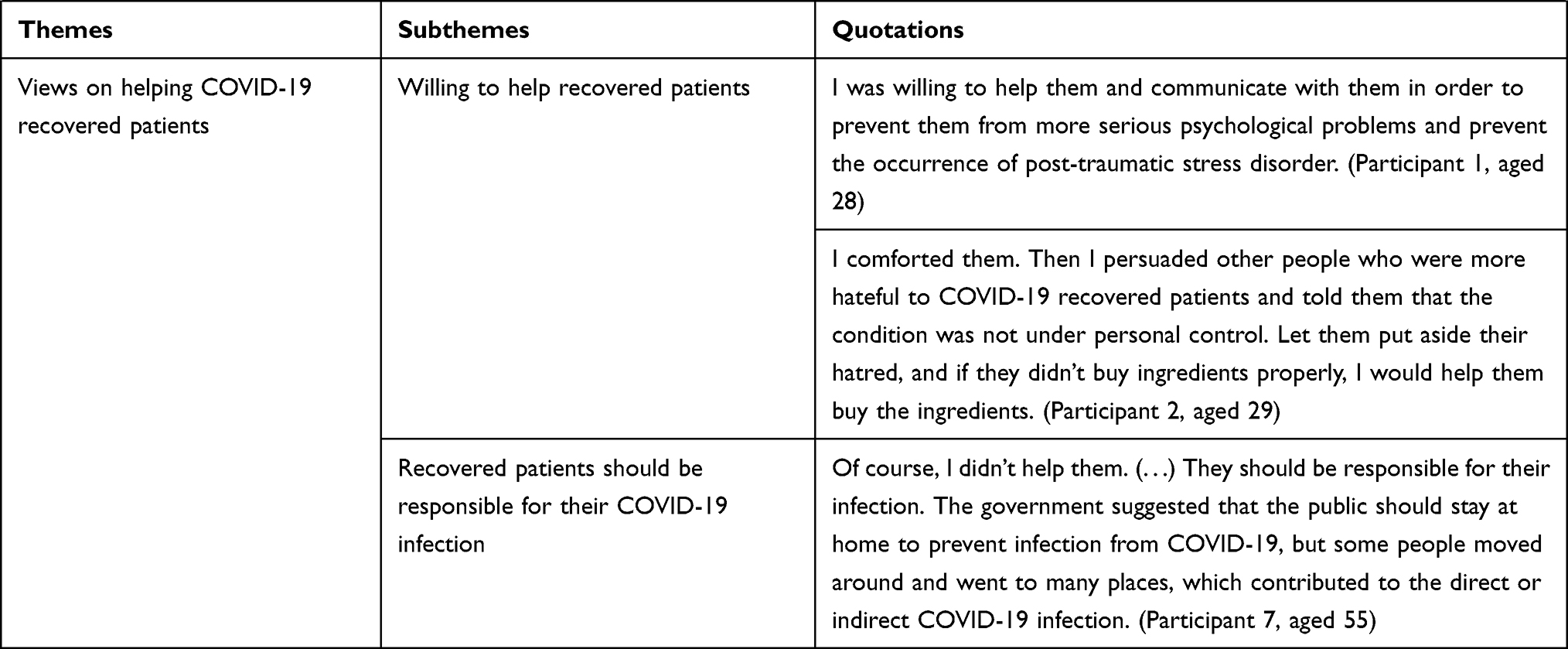 |
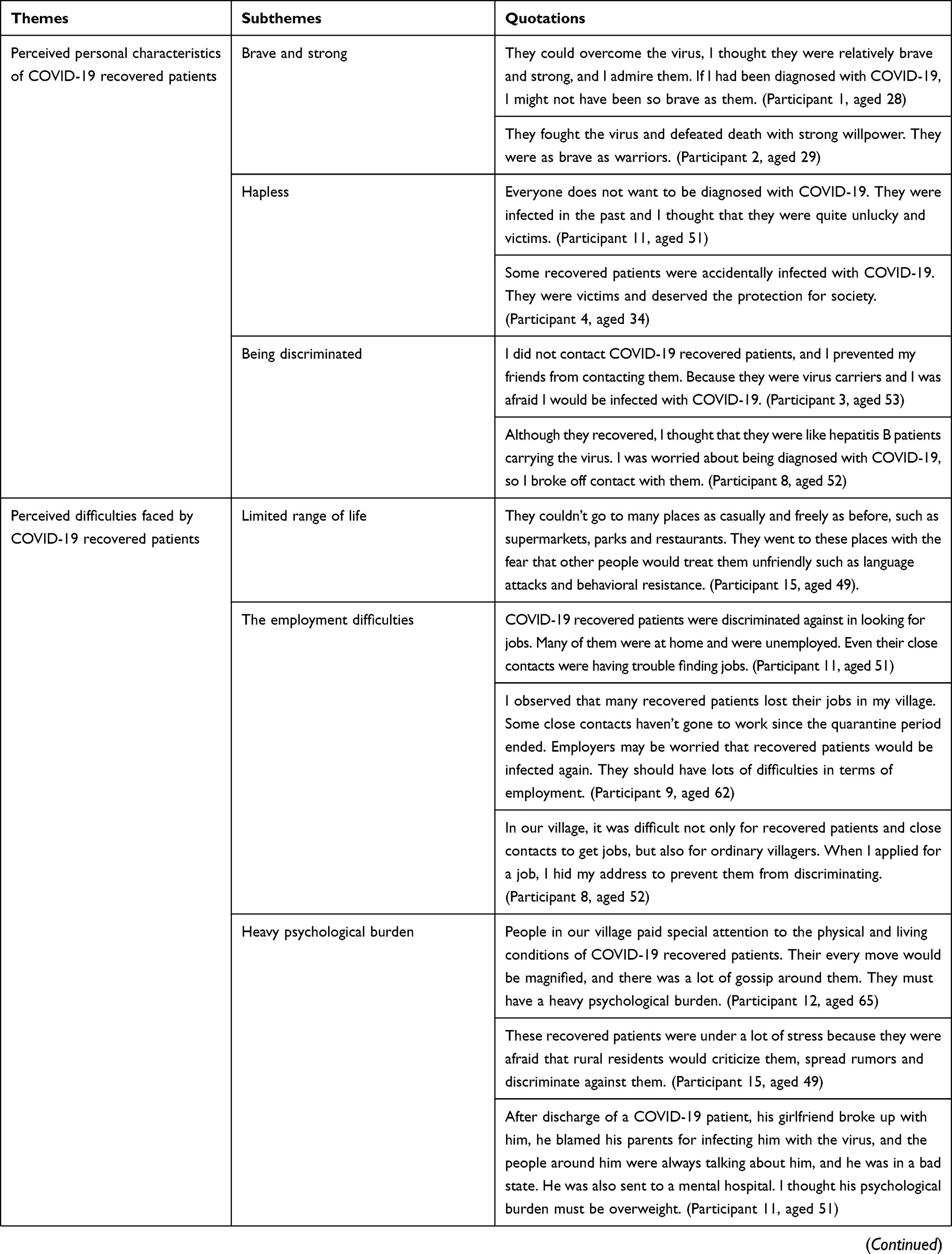
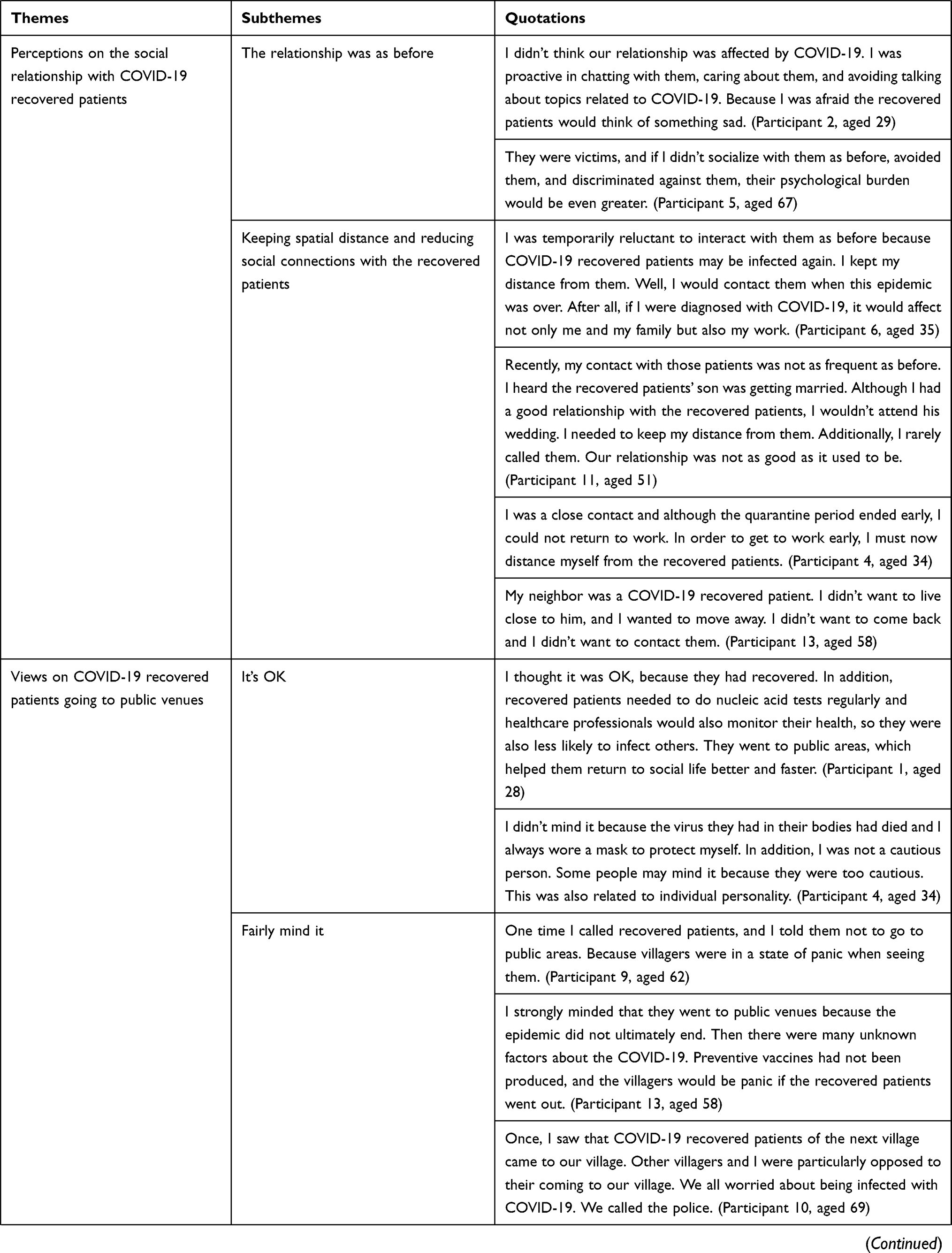
Table 2 Themes, Subthemes and Quotations of Perceptions and Views of Rural Residents Towards COVID-19 Recovered Patients |
Theme 1: Perceived Personal Characteristics of COVID-19 Recovered Patients
Brave and Strong
Two participants gave positive descriptions of COVID-19 recovered patients. They thought that COVID-19 recovered patients were brave in the fight against the COVID-19 and defeated the virus with strong willpower, and they behaved like warriors. There was a quotation showed:
They could overcome the virus, I thought they were relatively brave and strong, and I admire them. If I had been diagnosed with COVID-19, I might not have been so brave as them. (Participant 1, aged 28)
Hapless
Several interviewed participants described COVID-19 recovered patients as victims and thought that they were hapless. Due to their carelessness in life or work, they failed to take adequate protective measures, leading to being infected with COVID-19, which affected their physical and mental health. They deserve the protection and attention of society. As the evidence showed:
Everyone does not want to be diagnosed with COVID-19. They were infected in the past and I thought that they were quite unlucky and victims. (Participant 11, aged 51)
Being Discriminated
The majority of the participants described COVID-19 recovered patients as virus carriers. Some rural residents either treated recovered patients with indifferent faces or stayed away from them because they feared contacting COVID-19. Even a participant prevented his friends from contacting the recovered patients. Furthermore, a rural resident refused to touch any of the belongings of COVID-19 recovered patients. These behaviors of rural residents reflected that they may discriminate against COVID-19 recovered patients to some extent. For instance:
I did not contact COVID-19 recovered patients, and I prevented my friends from contacting them. Because they were virus carriers and I was afraid I would be infected with COVID-19. (Participant 3, aged 53)
Theme 2: Perceived Difficulties Faced by COVID-19 Recovered Patients
Limited Range of Life
The villagers thought that the life range of COVID-19 recovered patients was not as free as it had been before. They had concerns before going anywhere. They were particularly worried that others were unkind to themselves, which led to heavy psychological pressure on them and affected their normal life. The sentence was:
They couldn’t go to many places as casually and freely as before, such as supermarkets, parks and restaurants. They went to these places with the fear that other people would treat them unfriendly such as language attacks and behavioral resistance. (Participant 15, aged 49).
The Employment Difficulties
Some villagers believed that COVID-19 recovered patients would have difficulty in applying for jobs. Employers may be worried that recovered patients would be infected again. Thus, recovered patients may be discriminated against. Moreover, some close contacts said that they had not returned to work. Even ordinary people had difficulty finding jobs. Apparently, there was a lot of pressure on the employment of COVID-19 recovered patients. The quotation was:
I observed that many recovered patients lost their jobs in my village. Some close contacts haven’t gone to work since the quarantine period ended. Employers may be worried that recovered patients would be infected again. They should have lots of difficulties in terms of employment. (Participant 9, aged 62)
Heavy Psychological Burden
This third subtheme reported that rural residents thought that COVID-19 recovered patients were under great psychological pressure. The excessive attention, discrimination, criticism and rumors from others could increase recovered patients’ psychological burden. Moreover, the negative impacts of the COVID-19 diagnosis were also stress sources for recovered patients. Some patients experienced family breakdown, were blamed by their employers, and their loved ones have been quarantined due to COVID-19 infections. As a participant said:
These recovered patients were under a lot of stress because they were afraid that rural residents would criticize them, spread rumors and discriminate against them. (Participant 15, aged 49)
Theme 3: Perceptions on the Social Relationship with COVID-19 Recovered Patients
The Relationship Was as Before
This subtheme clearly illustrated that some participants would interact with COVID-19 recovered patients as before with both wearing masks. Their relationship was not affected by COVID-19. These participants stated that they would not actively mention the topic of COVID-19, so as not to trigger the memories of the recovered patients. One participant described that COVID-19 recovered patients were unlucky and victims. If people did not communicate with them as before, their psychological pressure would be even greater. Evidence showed:
They were victims, and if I didn’t socialize with them as before, avoided them, and discriminated against them, their psychological burden would be even greater. (Participant 5, aged 67)
Keeping Spatial Distance and Reducing Social Connections with the Recovered Patients
This second subtheme emphasized that most of the participants would reduce social connections with COVID-19 recovered patients and keep away from them. The main reason was that participants were worried about being infected with COVID-19 and the bad outcomes of the infection. For instance:
I was temporarily reluctant to interact with them as before because COVID-19 recovered patients may be infected again. I kept my distance from them. Well, I would contact them when this epidemic was over. After all, if I were diagnosed with COVID-19, it would affect not only me and my family but also my work. (Participant 6, aged 35)
Theme 4: Views on COVID-19 Recovered Patients Going to Public Venues
It’s OK
A small number of participants did not mind the recovered patients moving in public venues. Because COVID-19 patients had recovered, and healthcare professionals continued to monitor the health of recovered patients. If recovered patients have symptoms related to COVID-19, the health care provider will take prompt measures to deal with them. At the same time, villagers always wore masks to protect themselves. As a result, recovered patients were less likely to infect others. Furthermore, the views also depended on people’ personality. If they were cautious, they mind it. And the participant said:
I didn’t mind it because the virus they had in their bodies had died and I always wore a mask to protect myself. In addition, I was not a cautious person. Some people may mind it because they were too cautious. This was also related to individual personality. (Participant 4, aged 34)
Fairly Mind It
This subtheme reported that the majority of participants believed that the COVID-19 outbreak was not completely over. They had too much uncertainty about COVID-19. If COVID-19 recovered patients moved to public areas, the public would feel panic and fear about contacting COVID-19 infection. For example:
One time I called recovered patients, and I told them not to go to public areas. Because villagers were in a state of panic when seeing them. (Participant 9, aged 62)
Theme 5: Views on Helping COVID-19 Recovered Patients
Willing to Help Recovered Patients
Two participants reported that they were willing to help COVID-19 recovered patients. These main performances were that they would also persuade others not to hate the recovered patients and were willing to help the recovered patients to do something. For example:
I was willing to help them and communicate with them in order to prevent them from more serious psychological problems and prevent the occurrence of post-traumatic stress disorder. (Participant 1, aged 28)
Recovered Patients Should Be Responsible for Their COVID-19 Infection
Some participants were unwilling to help the COVID-19 recovered patients. The reason behind the view may be that the participants did not obey the government’s quarantine orders and should be responsible for their actions. For instance:
Of course, I didn’t help them. (…) They should be responsible for their infection. The government suggested that the public should stay at home to prevent infection from COVID-19, but some people moved around and went to many places, which contributed to the direct or indirect COVID-19 infection. (Participant 7, aged 55)
Discussion
To the best of our knowledge, this is the first study to explore the perceptions and views of rural residents towards patients recovered from COVID-19. Our study found that some participants hold positive attitudes towards them. However, most participants seemed to choose to keep social contact with recovered patients and showed their discrimination and resistance to some extent. By taking perceptions and views into consideration of rural residents, decision-makers may develop targeted strategies to improve their awareness and behaviors and create a supportive social environment for the recovered patients to return to normal life and work.
With the effective treatments of COVID-19 in China, the number of cured patients increased significantly.28 Some participants in this study thought that cured individuals were brave and unfortunate. Based on their perceptions, we could infer that some rural residents were full of admiration and sympathy for COVID-19 recovered patients. However, over half of villagers described COVID-19 recovered patients as virus carriers and they were worried about being infected by the virus in the bodies of recovered patients. As reported, the nucleic acid test results of discharged patients returned positive during their follow-up visits in many places in China. The studies by Yuan et al,29 Zhang et al,30 and Li et al,28 reported that discharged COVID‐19 Chinese patients had later positive nucleic acid test results and showed high viral load for nucleic acid. If patients with high viral load were contagious, they might be potential and mobile infectious sources.31 Additionally, Lan et al,32 suggested that at least a proportion of recovered patients still may be virus carriers. Therefore, it is understandable that villagers have this perception. However, not all recovered individuals are virus carriers. Labeling all of them as virus carriers may reflect discrimination of villagers to some extent. Some studies found that the insufficient or inaccurate knowledge of Human Immunodeficiency Virus (HIV)/Acquired Immune Deficiency Syndrome (AIDS) may contribute to stigma toward people living with HIV/AIDS.33,34 Thus, relevant departments should aim to raise their scientific awareness of COVID-19 by conducting extensive health education, disseminating precise information related to COVID-19 and providing counseling to reduce their discrimination and exclusion. In order to enhance the dissemination of health education-related knowledge and information, it is recommended to use modern media technologies, including television, the Internet, mobile phones, etc.
In the present study, participants gave an objective account of the difficulties faced by the recovered patients after discharge. We understood the difficulties faced by recovered patients from the perspective of rural residents, which help policymakers develop strategies to promote patients reintegrate into society. When questioned on their understanding of the problems faced by COVID-19 recovered patients, participants’ responses were categorized as belonging to employment difficulties, heavy psychological burden, and limited living scope. The present study was in line with Tansey et al’ study,35 which evaluated 117 SARS survivors from Toronto, 17% of these survivors had not returned to work and 51% required over 660 visits to psychiatry or psychology practitioners at 1 year after hospital discharge. In our study, the reason behind the employment difficulties may be that some COVID-19 recovered patients were discriminated against by their employers. Government departments should take measures to strictly prevent discrimination in employment so that recovered patients could enjoy fair employment rights. Regarding the heavy psychological burden on recovered patients, Huang and Zhao,36 identified a significantly higher prevalence of mental health burden in the Chinese public during the COVID-19 outbreak. Therefore, we have reasons to speculate that the psychological burden of recovered patients would be heavier. Our finding was consistent with Cheng et al’ study,37 which showed that the psychological distress of SARS survivors at 1-month recovery was real and significant. Moreover, SARS survivors still had elevated stress levels and elevated worrying levels of psychological distress one year after the outbreak.38 In the present study, discrimination, criticism and rumors from others were the causes of the psychological burden of recovered patients. Therefore, healthcare professionals should provide regular psychological counseling and follow-up for recover patients.
In terms of the perceived relationships with COVID-19 recovered patients, most participants chose to distance themselves from the recovered patients. We could understand that villagers kept spatial space with the recovered patients in order to protect themselves. However, in our study, while the participants kept spatial space with recovered patients, social closeness with them was gradually declining. Some villagers even decided to cut off contact with the recovered patients. This avoidance shown by the rural residents has created a non-supportive environment for the recovered patient’s social reintegration. Moreover, reduced social contact with recovered patients could have deleterious psychosocial effects among COVID-19 healers. The study by Cheng et al,39 showed that better social support to SARS survivors could have beneficial effects on distress and quality of life. Abel et al,40 suggested that public health should respond to the threat of COVID-19 by promoting social closeness. Therefore, it is necessary to encourage friendly and supportive interpersonal behaviors when spatial space is kept.
Our research also found that most of the participants minded recovered patients going to public areas with the perception that they may be re-infected and transmit the COVID-19 virus to others. Given the facts, recovered patients should be less likely to go to places where people gather and take precautions. For villagers, if recovered patients use personal protective equipment to go to public areas, they should be given tolerance and understanding, instead of resisting them. Additionally, most participants were reluctant to help participants. The reason behind the phenomenon may be attributed to the that villagers hold recovered patients responsible for their actions, and therefore the bad results should be borne by themselves. Only two participants showed the willingness to help COVID-19 recovered patients, who had higher education levels compared to others. Therefore, people with higher education levels could have a more tolerant attitude towards COVID-19 recovered patients.
We can understand the cognition and behavior of most villagers, but we are concerned about the discrimination of villagers and the decrease in social closeness. To reduce the discrimination and increase the social closeness of the rural residents, a joint effort of multiple departments is necessary. For medical departments, they should publish precise information to the public on the physical conditions of COVID-19 recovered patients, whether they are still contagious and whether they have sequelae, and so on, to dispel public doubts. For government departments, they should appease the psychological pressure of the healers, formulate employment-related protection measures, and then strictly prevent employment discrimination, so that recovered patients can enjoy fair employment rights. The village committees where COVID-19 recovered patients are located should provide health education programs related to COVID-19 to the villagers by modern media technologies, enhance their scientific understanding of COVID-19 knowledge, and alleviate their resistance and discrimination; and encourage social connection between villagers and recovered patients. Through multi-sectoral cooperation, the rural residents may effectively reduce the discrimination against COVID-19 healers.
Limitations
There were several limitations in our study. Firstly, all the participants were from Shandong Province, in China. Although data saturation had been reached, the applicability of this study to other settings was a limitation. Future research could explore the attitudes of people in different districts. Moreover, our study only explored the perceptions and views of rural residents, and future studies can compare their differences between rural residents and urban residents. Finally, the interview duration of the three participants was short (20, 18 and 22 minutes), which could imply that the details provided by the participants were limited. Therefore, we should be cautious when interpreting the results.
Conclusion
The perceptions and views of rural residents towards COVID-19 recovered patients were important in judging recovered patients’ return to social life aspect. Our study underlines the need for related departments to reduce rural residents’ discrimination and resistance towards COVID-19 recovered patients and increase social closeness between rural residents and recovered patients. Relevant departments can lead educational programs by mass media and issue regulations that should be tailored based on villagers’ views and perceptions. Additionally, it is practical to develop interventions that address identifiable and modifiable cognitive for rural residents. Our findings may assist government advisors and healthcare professionals in providing targeted interventions for rural residents in the face of the COVID-19 recovered patients in China and the different parts of the world.
Disclosure
The authors declare that there is no conflicts of interest.
References
1. China, N.H.C.O. The latest situation of the COVID-19 epidemic situation as of 24:00 on July 3; 2020.
2. Sher L. Are COVID-19 survivors at increased risk for suicide? Acta Neuropsychiatrica. 2020;32(5):1–4. doi:10.1017/neu.2020.21
3. Wu C, Hu X, Song J, et al. Mental health status and related influencing factors of COVID-19 survivors in Wuhan, China. Clin Transl Med. 2020;10:3. doi:10.1002/ctm2.52
4. Sher L. Resilience as a focus of suicide research and prevention. Acta Psychiatr Scand. 2019;140:2. doi:10.1111/acps.13059
5. Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
6. Mak WW, Mo PKH, Cheung RYM, et al. Comparative stigma of HIV/AIDS, SARS, and tuberculosis in Hong Kong. Soc Sci Med. 2006;63(7):1912–1922. doi:10.1016/j.socscimed.2006.04.016
7. Lau JT, Yang X, Wong E, et al. Prevalence and factors associated with social avoidance of recovered SARS patients in the Hong Kong general population. Health Educ Res. 2006;21(5):662–673. doi:10.1093/her/cyl064
8. Azlan AA, Hamzah MR, Sern TJ, et al. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
9. Hezima A, Aljafari A, Aljafari A, et al. Knowledge, attitudes, and practices of Sudanese residents towards COVID-19. East Mediterr Health J. 2020;26(6):646–651. doi:10.26719/emhj.20.076
10. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the Novel Coronavirus Disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
11. Xu J, Chen P. The rural children’s loneliness and depression in Henan, China: the mediation effect of self-concept. Soc Psychiatry Psychiatr Epidemiol. 2019;54(9):1101–1109. doi:10.1007/s00127-018-1636-5
12. Rong Huan DRCX. Study on the rural residents’ knowledge, attitude and practice on COVID-19 and their coping styles. J Chengdu Med Coll. 2020;(2):1–7.
13. Kamate SK, Agrawal A, Chaudhary H, et al. Public knowledge, attitude and behavioural changes in an Indian population during the Influenza A (H1N1) outbreak. J Infect Dev Ctries. 2009;4(1):7–14. doi:10.3855/jidc.501
14. Ahayalimudin N, Ismail A, Saiboon IM. Disaster management: a study on knowledge, attitude and practice of emergency nurse and community health nurse. Bmc Public Health. 2012;12(2):1. doi:10.1186/1471-2458-12-S2-A3
15. Caelli K, Ray L, Mill J. ‘Clear as Mud’: toward greater clarity in generic qualitative research. Int J Qual Methods. 2003;2:2. doi:10.1177/160940690300200201
16. Neergaard MA, Olesen F, Andersen RS, et al. Qualitative description - the poor cousin of health research? BMC Med Res Methodol. 2009;9:52. doi:10.1186/1471-2288-9-52
17. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33(1):77–84. doi:10.1002/nur.20362
18. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15(3):398–405. doi:10.1111/nhs.12048
19. O’Brien BC, Harris IB, Beckman TJ, et al. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
20. Patton MQ. Qualitative Research and Evaluation Methods.
21. Zhou Y. Qualitative Research in Nursing: Theory and Cases. China: Zhejiang University Press; 2017:98.
22. Green J, Thorogood N. Qualitative Methods for Health Research.
23. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
24. Nicolson P, Anderson P. The psychosocial impact of spasticityrelated problems for people with multiple sclerosis: a focus group study. J Health Psychol. 2001;6(5):551–567. doi:10.1177/135910530100600508
25. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods. 2006;5(1):1–11. doi:10.1177/160940690600500107
26. Whitley R, Crawford M. Qualitative research in psychiatry. Can J Psychiatry. 2005;50(2):108–114. doi:10.1177/070674370505000206
27. Guba EG, Lincoln YS. Paradigmatic controversies, contradictions, and emerging confluences. In: Denzin NK, Lincoln YS, editors. The SAGE Handbook of Qualitative Research.
28. Li Y, Hu Y, Yu Y, et al. Positive result of Sars-Cov-2 in faeces and sputum from discharged patients with COVID-19 in Yiwu, China. J Med Virol. 2020.
29. Yuan J, Kou S, Liang Y, et al. PCR assays turned positive in 25 discharged COVID-19 patients. Clin Infect Dis. 2020;71:2230–2232. doi:10.1093/cid/ciaa398
30. Zhang JF, Yan K, Ye -H-H, et al. SARS-CoV-2 turned positive in a discharged patient with COVID-19 arouses concern regarding the present standards for discharge. Int J Infect Dis. 2020;97:212–214. doi:10.1016/j.ijid.2020.03.007
31. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (2019-nCoV) infection is suspected Interim guidance. World Health Organization: Geneva; 2020. Available from: https://apps.who.int/iris/handle/10665/330854.
32. Lan L, Xu D, Ye G, et al. Positive RT-PCR test results in patients recovered from COVID-19. JAMA. 2020;323(15):1502–1503. doi:10.1001/jama.2020.2783
33. Alemi Q, Stempel C. Association between HIV knowledge and stigmatizing attitudes towards people living with HIV in Afghanistan: findings from the 2015 Afghanistan demographic and health survey. Int Health. 2019;11(6):440–446. doi:10.1093/inthealth/ihz013
34. Letshwenyo-Maruatona SB, Madisa M, Boitshwarelo T, et al. Association between HIV/AIDS knowledge and stigma towards people living with HIV/AIDS in Botswana. Afr J AIDS Res. 2019;18(1):58–64. doi:10.2989/16085906.2018.1552879
35. Tansey CM, Louie M, Loeb M, et al. One-year outcomes and health care utilization in survivors of severe acute respiratory syndrome. Arch Intern Med. 2007;167(12):1312–1320. doi:10.1001/archinte.167.12.1312
36. Huang Y, Zhao N. Mental health burden for the public affected by the COVID-19 outbreak in China: who will be the high-risk group? Psychol Health Med. 2020;1–12.
37. Cheng SK, Wong CW, Tsang J, et al. Psychological distress and negative appraisals in survivors of severe acute respiratory syndrome (SARS). Psychol Med. 2004;34(7):1187–1195. doi:10.1017/S0033291704002272
38. Lee AM, Wong JG, McAlonan GM, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. 2007;52(4):233–240. doi:10.1177/070674370705200405
39. Cheng SK, Sheng B, Lau KK, et al. Adjustment outcomes in Chinese patients following one-month recovery from severe acute respiratory syndrome in Hong Kong. J Nerv Ment Dis. 2004;192(12):868–871. doi:10.1097/01.nmd.0000147169.03998.dc
40. Abel T, McQueen D. The COVID-19 pandemic calls for spatial distancing and social closeness: not for social distancing! Int J Public Health. 2020;65(3):231. doi:10.1007/s00038-020-01366-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.