")
Back to Journals » Cancer Management and Research » Volume 12
The Pathogenesis and Prevention of Port-Site Metastasis in Gynecologic Oncology
Received 6 July 2020
Accepted for publication 1 September 2020
Published 6 October 2020 Volume 2020:12 Pages 9655—9663
DOI https://doi.org/10.2147/CMAR.S270881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Qianqian Gao, Ling Guo, Bo Wang
Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Bo Wang
Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, 107 Wenhuaxi Road, Jinan, Shandong 250012, People’s Republic of China
Email [email protected]
Abstract: Port-site metastasis (PSM) is a specific and challenging complication of laparoscopic gynecologic oncologic procedures. Research has demonstrated that PSM is associated with significant morbidity and poor outcome. The exact pathogenesis of PSM in gynecologic patients is not clear. Several preventive measures of PSM have been addressed in the relevant literature, and novel approaches to prevent this uncommon complication keep emerging. In this review, we summarized the potential mechanisms of PSM and discuss the controversies and merits of proposed preventive measures of PSM in gynecologic oncology. We undertook a literature search using the Medline database to identify studies on the pathogenesis and prevention of laparoscopic PSM. Hypotheses of PSM pathogeneses center on the immune response, pneumoperitoneum, wound contamination, and surgical method. Cogent evidence of effective prevention of PSM after laparoscopic surgery is lacking. Traditional preventive actions such as irrigation and tumor manipulation should be taken individually. Insufflation of hyperthermic CO2 and humidified CO2 leads to a better outcome in patients with a malignant tumor who undergo a laparoscopic procedure compared with normal CO2 pneumoperitoneum. Port-site resection shows no advantage in survival and results in more wound events. PSM prevention plays a crucial part in the overall care of patients with gynecologic malignancies who undergo laparoscopic procedures.
Keywords: laparoscopy, port-site metastasis, risk factor, prognosis, prevention
Introduction
Minimally invasive surgery has become increasingly acceptable to gynecologic oncologists thanks to its few surgical complications, rapid recovery, and good cosmetic results. Laparoscopy has been used widely for the staging and treatment of gynecologic tumors, and has elicited similar surgical results to those of open surgery, but with lower surgical morbidity.
Gallotta undertook a case–control study to compare the oncologic outcome of laparoscopy and laparotomy in early-stage ovarian cancer. They discovered that the oncologic outcome of laparoscopy was equivalent to that of conventional open surgery, and that laparoscopy had advantages over laparotomy in terms of duration of the surgical procedure, blood loss, and duration of hospital stay.1 Besides, the feasibility and safety of laparoscopic secondary cytoreductive surgery in patients with recurrent ovarian cancer were demonstrated by the same research team in another retrospective study.2
Robot-assisted laparoscopy has overcome some difficulties associated with conventional laparoscopy since its approval by the US Food and Drug Administration. Robot-assisted laparoscopy has altered the landscape of minimally invasive gynecologic surgery.3–5 Expanded use of laparoscopic methods for different types of cancer has met with greater awareness of their potential complications.
One of the most important complications is port-site metastasis (PSM).6,7 PSM is defined as tumor-cell implantation at the site of trocar insertion after laparoscopic resection of a malignant tumor.5,8,9 PSM has been reported to occur at 1%–2% of all laparoscopic procedures in gynecologic surgery.3,10 Isolated port-site metastasis (iPSM; also known as “solitary port-site metastasis”) denotes tumor recurrence at trocar sites without evidence of concomitant metastasis.11,12 Conversely, PSM with simultaneous metastasis in other locations (“non-isolated PSM”) is usually regarded as a part of systemic recurrence.5 It has not been demonstrated that all patients with PSM carry a worse prognosis, but some studies have suggested that the PSM associated with multilocal recurrence has an adverse impact upon survival.13,14 Management of PSM with multiple metastases follows the general principles of treating a systematic recurrence, but iPSM treatment is controversial.12 The small number of reported cases has limited the conclusions that can be drawn regarding iPSM management. Surgical excision alone, surgical excision and adjuvant chemoradiotherapy, or radiotherapy alone for iPSM management have been reported, but the outcomes have been heterogeneous.5,15 Given the small study cohorts and heterogeneous outcomes of management, guidelines for iPSM treatment have been lacking. The validity of preventive actions to reduce PSM prevalence has not been demonstrated.16 New concepts and methods for PSM prevention have appeared in recent years.17
We reviewed the hypotheses of PSM pathogeneses in gynecologic oncology. In this way, we wished to summarize the progress in PSM prevention and to select the potential preventive options for patients with gynecologic malignancies.
Materials and Methods
A literature search was undertaken using the Medline database using the following terms: “laparoscopy,” “port-site metastasis,” “gynecology,” and “prevention.” Articles outlining the prevalence, potential etiologies, and modes of prevention of PSM were selected. Abstracts, Letters to the Editor, and Comments were excluded. The reference lists of the initial articles were reviewed manually to obtain additional relevant references.
Prevalence
The first report describing a case of PSM development after laparoscopy for ovarian cancer was by Döbrönte in 1978.18 Numerous studies regarding this rare complication have been presented, and PSM has been debated for decades.
The overall prevalence of PSM after minimally invasive surgery for gynecologic cancers has been estimated to be 0.4%–2.3% (Table 1).4,10,15,19–22 This prevalence is comparable to the prevalence of wound implantation after open surgery.6,13 iPSM is even rarer, with an estimated prevalence at 0.2%–0.5%.4,19 Barraez reported a low prevalence of PSM (0.9%) in 438 patients who underwent robotic-assisted staging of endometrial cancer, and iPSM was identified in two patients (0.45%).4 Zivanovic documented PSM in 20 of 1694 (1.18%) women who underwent laparoscopic procedures for an intra-abdominal malignancy.21 PSM after robotic surgery for gynecologic malignancies has been reported to occur in 0.9%–1.9% of cases.4,10,19,20 Ndofor and collaborators reported that the PSM prevalence after robotic surgery for gynecologic malignancies was 1.1% (2/181).20
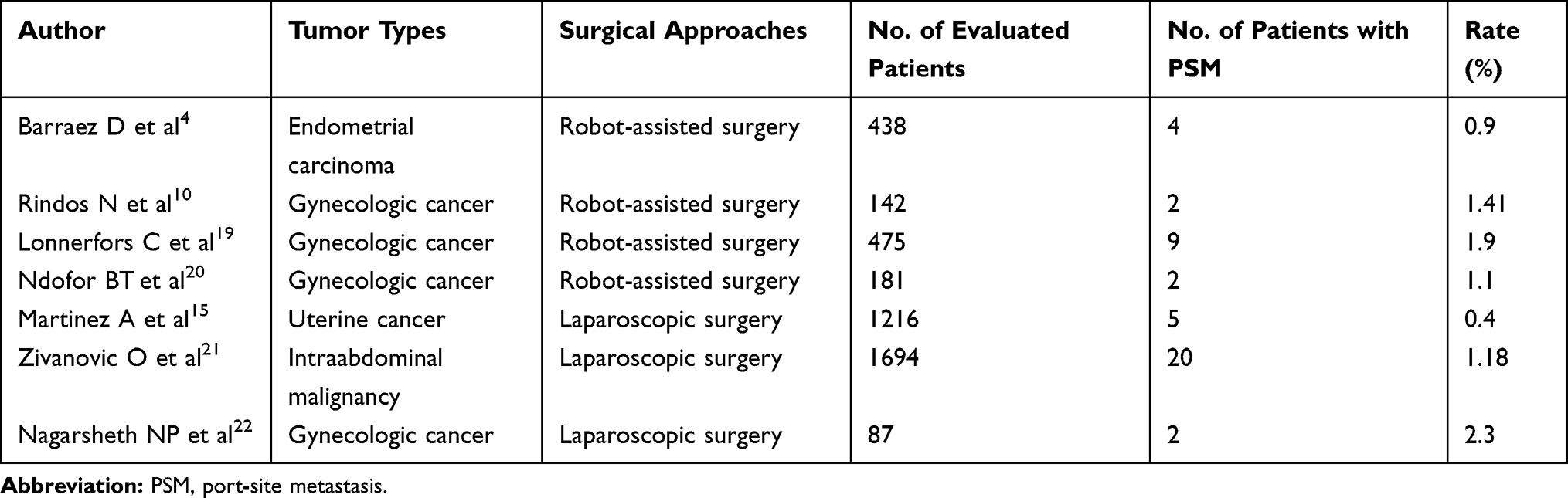 |
Table 1 The Prevalence of PSM in Published Studies |
Data have shown that cervical cancer and endometrial cancer carry a lower risk of PSM development than that for ovarian cancer. In a study by Martínez, laparoscopic procedures were undertaken in 1216 patients with uterine cancer (921 patients with cervical cancer and 295 with endometrial cancer). The PSM prevalence in patients with cervical cancer and in those with endometrial cancer was 0.43% and 0.33%, respectively.15 PSM prevalence after diagnostic laparoscopy for ovarian cancer has been reported to vary from 16% to 47%.23,24 Ataseven evaluated a cohort of patients with epithelial ovarian cancer who underwent port-site resection during primary debulking surgery immediately after diagnostic laparoscopy. Histopathology revealed PSM in 100 of 214 patients (46.7%).25 The high prevalence of PSM in ovarian cancer may be due to the its invasiveness and the delayed diagnosis of advanced disease. Despite the extremely high prevalence of histopathology-diagnosed PSM in patients with ovarian cancer, the prevalence of clinically diagnosed PSM after laparoscopic procedures for ovarian cancer is lower. Vergote and collaborators evaluated 173 patients with advanced ovarian cancer who underwent diagnostic open laparoscopy. Seventy-one patients underwent complete excision of port sites at the time of debulking surgery. The PSM prevalence was 5% (8/171) by the clinical diagnosis and 31% (22/71) by the histopathology diagnosis, respectively.23
Pathogenesis
Establishing identifiable risk factors for PSM development is challenging. The main hypotheses are the immune response, pneumoperitoneum, wound contamination, and surgical method.
Immune Response
Data concerning the role of the immune response in PSM development have demonstrated that systemic immunity seems to be better preserved after a laparoscopic procedure than after open surgery. Also, postoperative immunologic functions return more rapidly after laparoscopy compared with that for an open approach, which may be conducive to implantation of liberated tumor cells.6,26 The impact of surgical trauma on immune surveillance in tumor resistance was demonstrated by Sylla.27 Surgical trauma induced activation of inflammatory cells. This inflammatory response could deplete immune resources and aggravate tumor-related alterations to the immune system. Traumatic handling of tumor tissue during a surgical procedure can result in subsequent release of liberated tumor cells. Synchronously, a shift in the balance of growth factors/inhibitory factors caused by surgical trauma supports the growth and establishment of liberated tumor cells.
Carbon Dioxide (CO2) Pneumoperitoneum
Insufflation of CO2 alters the parameters of the peritoneal microenvironment significantly. Ost demonstrated that CO2 pneumoperitoneum inhibited secretion of tumor necrosis factor-α from peritoneal macrophages transiently, which could contribute to PSM of transitional-cell carcinoma.6,28 Some investigations showed that tumor growth can be stimulated by intra-abdominal pressure. Experiments in vitro showed a nonlinear impact of CO2 insufflation pressures on the viability and proliferation of tumor cell lines.29,30 Asthana demonstrated a “U-shaped”, dose–response effect of pneumoperitoneum pressure on the viability of transitional carcinoma cells and Madin–Darby canine kidney cells.29 They described decreased viability in all cell lines upon exposure to 5 mmHg and 10 mmHg compared with that obtained with control and 0 mmHg, whereas no effects were observed in cells exposed to 15 mmHg of CO2 pneumoperitoneum. Zheng supplied additional information on the effect of CO2 pneumoperitoneum on the proliferation and migration of cells using a gastrointestinal stromal tumor line (GIST-T1). Longer time exposure (3 h) decreased the proliferative capabilities of GIST-T1 cells, whereas a lower pressure (8 mmHg) could increase it. Significant promotion of cell migration was observed upon a longer exposure time or higher pneumoperitoneum pressure (15 mmHg).30 CO2 insufflation during laparoscopy causes an immediate reduction of the pH of the peritoneum, resulting in an appreciable change in the peritoneal acid–base balance and reduced release of cytokines and free oxygen radicals. Simultaneously, severe hypoxia caused by CO2 pneumoperitoneum increases expression of hypoxia inducible factor-1α and −2α. These physiologic changes are considered to create a favorable condition for the adhesion and growth of cells.30,31 Sedimentation of tumor cells at port sites due to continuous air leakage along the trocars during laparoscopic procedures may be another mechanism in PSM development, which is referred to as the “chimney effect”.32 At the time of laparoscopy, the abdominal cavity becomes a closed, high-pressure container with a continuous flow of gas that exits through trocar wounds. Specimen manipulation may lead to exfoliation of tumor cells. Turbulent airflow may transport exfoliated tumor cells to port sites owing to microleakage through trocars.32,33 Nevertheless, investigators have been unable to provide ample evidence to support this hypothesis, and it is doubtful that aerosolization of tumor cells will result in tumor recurrence at trocar sites.34,35
Wound Contamination
Direct contamination of trocar sites has been postulated to be the cause of PSM. That is, malignant cells are implanted directly in port sites during violent retrieval of unprotected tissue or by contaminated instruments.6,32,36,37 Several animal experiments have revealed that the most common ports of tumor-cell deposition were extraction wounds. Paolucci discovered that 55% of PSM occurred at extraction ports.38 Another common site of PSM is the operating port, where there are frequent exchanges of contaminated instruments, which predisposes to implantation of tumor cells. Besides, more tumor cells were found to deposit at operating ports than at assistants’ ports in a study by Allardyce and collaborators.39,40
Surgical Method
It has been proposed that tumor manipulation during laparoscopy is an essential factor influencing the liberation, implantation, and growth of tumor cells. The surgeon’s experience, including surgical skills and intraoperative manipulation of tumors, may have a significant impact upon surgical outcomes.6,32 Schneider undertook an in vivo study to investigate the influence of surgical quality on PSM prevalence. Preventive measures (trocar fixation, instrument disinfection, peritoneal closure) were applied in the preventive group, whereas standardized surgical mistakes were made in control group. PSM prevalence after laparoscopy was 13.8% in the preventive group and 63.8% in the control group, respectively.41 Polat undertook laparoscopic colectomy on a mouse model to investigate the effect of different approaches of resection and manipulation on contamination at trocar sites. In three main groups of rats, the cecum was resected extracorporeally or intracorporeally, or not resected at all. Each main group was divided further into two subgroups according to atraumatic manipulation or traumatic manipulation. They observed that rats who underwent intracorporeal resection with traumatic manipulation developed suffered contamination at most port sites.42 Lack of surgical experience or a shallow learning curve were also reported to be associated with increased PSM.43,44
Other Factors
Several risk factors have been presumed to participate in PSM development. Tumor aggressiveness (tumor stage, histology grade) seems to be a contributory factor in PSM development.6,19 Ataseven reviewed all the data of patients with primary epithelial ovarian, peritoneal, or fallopian-tube cancer who underwent diagnostic laparoscopy. In their multivariate analysis, they revealed that patients with advanced tumor stage, lymph-node metastasis, and massive ascites were more likely to develop PSM.25 From an anatomy viewpoint, it is unlikely that trocar implantation causes hematogenous or lymphatic metastases.34 However, some researchers have postulated that tumor recurrence at port sites is an outcome of hematogenous spread, and shown circulating tumor cells and PSM to be accompanied by disseminated diseases.32,45
Prognostic Impact
The prognostic impact of PSM on survival has been evaluated in several studies. In a retrospective study by Ataseven, the association of PSM and overall survival (OS) in patients with epithelial ovarian cancer undergoing laparoscopy before subsequent primary debulking surgery was evaluated. In the univariate analysis, Eastern Cooperative Oncology Group performance status (ECOG PS) <0, high tumor stage, positive lymph-node status, ascites volume >500 mL, high-grade serous histology, malignant pleural effusion, postoperative residual disease >0 mm, and PSM-positivity were associated significantly with shortened OS. However, in the multivariant analysis, only high tumor stage, malignant pleural effusion, and residual disease >0 mm remained independent risk factors for shortened OS.25 Those data were consistent with the analyses of Heitz, who revealed that ECOG PS >0, FIGO classification of IV, and tumor residuals >1 mm had a detrimental impact on OS in ovarian-cancer patients after laparoscopy, and neither laparoscopy nor PSM had a significant impact on survival.24 The association of PSM and worse OS has been observed in several studies. Bogani revealed that patients with non-iPSM after surgical treatment for endometrial cancer had a significantly worse OS than patients with iPSM. However, patients with non-iPSM were more likely to have advanced-stage disease, which reflected the poor outcome of patients with peritoneal, lymphatic, or hematogenous recurrences.13 Nunez showed that PSM was associated with worse OS compared with that in patients with peritoneal carcinomatosis without PSM. Meanwhile, PSM patients in their series had a higher mean Peritoneal Cancer Index score (>20 denotes extensive disease) and lymph-node metastasis, which were also the risk factors of worse OS, thereby suggesting that PSM was associated with extensive and more aggressive disease.14 Those studies supporting the deleterious impact of PSM on OS suggested that the adverse impact of PSM on OS reflected the impact of aggressive malignant disease on OS. Pearlstone elucidated that PSM associated with distant metastasis probably has little effect on the prognosis because the overall outcome is poor.46 Potential risk factors associated with OS for female patients with malignant disease who develop PSMs were evaluated by Zivanovic. In their cohort, breast-cancer patients without intra-abdominal disease were excluded because none of these patients developed PSM. The interval between laparoscopy and PSM detection was identified as the only meaningful predictor of survival. They found that patients with a shorter interval (<7 months) had a shorter OS (median, 12 months) than patients who developed PSM 7 months after the laparoscopic procedure (median, 37 months).21
Prevention
Surgeons have been trying to find appropriate methods for PSM prevention. Several measures have been proposed to reduce PSM prevalence on the basis of small series in humans or animals.
Patient Selection
PSM prevalence has been shown to be related to tumor aggressiveness (higher tumor stage, high-grade histology or large volume of ascites).4,12,19,25 Hence, undertaking laparoscopy in patients with advanced disease, high-risk histology, or ascites is not recommended.32,36 In their multivariate analysis, Ataseven and collaborators identified that advanced tumor stage, positive lymph-node status, and large-volume ascites were risk factors for PSM in patients with epithelial ovarian cancer undergoing diagnostic laparoscopy.25 Their findings support the concept that patients with advanced disease are not ideal candidates for minimally invasive procedures.
Surgical Method
Despite the incompletely understood mechanism for PSM development and lack of robust evidence of effective prevention of PSM, several surgical modifications have been proposed to reduce PSM prevalence. Modified surgical methods to minimize the number of port-site implants include:32,36,47–50 (i) appropriate placement of trocars with minimal trauma to tissue; (ii) anchor trocars in place to prevent inadvertent dislodgement and sudden desufflation; (iii) minimal manipulation of the tumor, resection of the tumor with adequate margins, and avoidance of tumor rupture; (iv) minimal requirement of repeated withdrawal and reinsertion of a trocar, and rinsing instrument tips in povidone iodine; (v) use of protective bags for tissue retrieval; (vi) removing intra-abdominal fluid before trocar removal; (vii) placement of drainage tube before abdomen deflation; (viii) avoiding CO2 leaks and sudden desufflation; (ix) intraperitoneal application of tumoricidal agents; (x) closure of all abdominal layers (including the peritoneum). Some of the suggestions stated above are unproven but should be followed meticulously.
Irrigation
Some investigators have suggested that intraperitoneal irrigation with agents can eradicate liberated tumor cells. Several agents have been used to reduce the PSM risk, including tumor-static agents, antiadhesion agents, povidone-iodine solution, and taurolidine.33,36 Braumann demonstrated a reduction of trocar-based tumor-cell recurrence when taurolidine was applied intraperitoneally.51 Intra-abdominal application of heparin has been proposed as a potent preventive strategy for PSM because heparin is one of the main substances involved in adherence of tumor cells.32,33 Neuhaus investigated the effect of heparin (i.p.) on tumor-cell implantation following laparoscopy. In their study, tumor-cell implantation and PSM were reduced upon intraperitoneal administration of heparin.52 Some investigators found that instillation of chemotherapeutic agents directly into the peritoneal cavity reduced cancer spread to the resection site and peritoneal surfaces. When injecting chemotherapeutic agents (eg, doxorubicin, cyclophosphamide, methotrexate), an optimal chemotherapy regimen and appropriate dose may be crucial. In another experimental study by Neuhaus, a significant decrease in tumor-cell implantation and PSM was observed in the methotrexate group.53 Eshraghi developed a rat model to assess the feasibility of port-site irrigation before wound closure to minimize tumor-cell implantation at trocars. Four treatment groups were analyzed by irrigating each port site with sterile water, physiologic (0.9%) saline, heparin, or 5-fluorouracil (5-FU), respectively. The 5-FU group showed a significant decrease in metastasis when compared with that in the control group (30% vs 81%).54 Importantly, one must balance the irritative side-effects of tissue exposure to these caustic agents with the benefits of preventing tumor-cell implantation.33
Pneumoperitoneum Modification
Pneumoperitoneum has a crucial role in the development of peritoneal dissemination and PSM after oncologic laparoscopy. The insufflated CO2 can cause diffuse damage to the entire peritoneum, and promote peritoneal dissemination of the spilled tumor cells.6,32 Controversies exist regarding the impact of helium pneumoperitoneum or gasless laparoscopy on PSM development. Gupta and collaborators demonstrated less PSM in laparoscopy with helium insufflation or gasless laparoscopy.55 However, in the animal studies of Ludemann and Agostini and colleagues, advantages were not demonstrated for insufflation with helium gas or gasless laparoscopy.56,57 However, a promising approach, hyperthermic CO2 insufflation and humidified CO2 insufflation, has shown efficacy in preventing peritoneal dissemination and PSM.17 During a conventional laparoscopy, the peritoneum is exposed to the cold, dry ambient air of the operating theatre (20°C, 0%– 5% relative humidity), which causes serious peritoneal damage.17,58 Peng investigated the effect of hyperthermic CO2 insufflation and humidified CO2 insufflation on the development of peritoneal dissemination.59 In their study, mice were divided into two groups and subjected to hyperthermic CO2 insufflation (43°C, >95% humidity, HT-CO2 group) or standard normothermic CO2 insufflation (21°C, <1% relative humidity, NTCO2 group) for 3 h. Peritoneal dissemination was evaluated quantitatively, and port sites and ascites were observed. There were significantly fewer peritoneal nodules in the HT-CO2 group than those in the NT-CO2 group, and the mean weight of metastases in the HT-CO2 group was lower than that in the NT-CO2 group. PSM was not detected in the HT-CO2 group, whereas three of 24 mice (12.5%) in the NT-CO2 group developed PSM. Slight damage to the peritoneum was examined by histology, and adhesions did not form after HT-CO2 treatment.59 Besides, intraperitoneal hyperthermic chemoperfusion was found to eradicate liberated tumor cells and micrometastases, thereby preventing peritoneal dissemination of tumor cells. The therapeutic effects of hyperthermic CO2 pneumoperitoneum and intraperitoneal irrigation of chemotherapy could be integrated. Zhao explored the effect of hyperthermic CO2 pneumoperitoneum in combination with 5-FU on the proliferation and invasion of colon cancer cells. They found inhibition of cell proliferation, transwell cell number, and transplantation tumor weight in the hyperthermic CO2 (43°C) group, 5-FU group, and hyperthermic CO2 + 5-FU group, but the most significant changes were observed in the group with hyperthermic CO2 insufflation in combination with 5-FU.60
Port-Site Resection
Given the high prevalence of PSM detected in patients who undergo port-site resection following laparoscopy, excision of port sites seems to be an option to avoid PSM. However, suspicions regarding the benefit of port-site resection persist. Lago evaluated the impact of port-site resection after laparoscopy on the oncologic outcome of advanced ovarian cancer. They found that port-site resection carried no advantage upon survival but resulted in a higher prevalence of wound complications.61 Maker also raised the question about the necessity of port-site resection. In their study on patients with incidental gallbladder carcinoma, port-site resection was not associated with improved OS or disease recurrence, and was not recommended in patients without macroscopic PSM.62 Excision of a port site may negate the principle of minimally invasive surgery (primarily the advantages of a small wound). Moreover, the safe margin of excision is not known.32 Based on the undesired results stated above, some investigators propose whether it’s time to abandon port-site resection.
Adjuvant Therapy
The hypothesis that early subsequent adjuvant therapy after laparoscopy can reduce PSM prevalence has been promoted by some researchers. However, in a retrospective study by Lonnerfors, all patients who developed PSM had received adjuvant therapy for a median time of 33 (range, 8–46) days postoperatively.19
Conclusions
PSM is an uncommon complication of laparoscopy in gynecologic oncology. PSM is associated with wound events and a poor prognosis. The hypotheses of PSM pathogenesis mainly involves the immune response, pneumoperitoneum, wound contamination, and surgical method. Ways to prevent PSM have been updated constantly but are controversial. Strict adherence to oncologic principles is the foundation of good surgical outcomes. Modified surgical methods should be adopted meticulously. Hyperthermic CO2 insufflation and humidified CO2 insufflation can serve as promising adjuvant treatment for preventing PSM development. Port-site resection is not recommended to prevent PSM in patients without macroscopic PSM. However, well-conducted, large, multi-institutional randomized trials are needed to verify the efficacy of preventive measures.
Abbreviations
PSM, port-site metastasis; iPSM, isolated port-site metastasis; OS, overall survival; 5-FU, 5-fluorouracil; ECOG PS, Eastern Cooperative Oncology Group performance status.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to this journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gallotta V, Petrillo M, Conte C. Laparoscopic Versus Laparotomic Surgical Staging for Early-Stage Ovarian Cancer: A Case-Control Study. J Minim Invasive Gynecol. 2016;23(5):769–774. doi:10.1016/j.jmig.2016.03.006
2. Gallotta V, Conte C, Giudice MT, et al. Secondary Laparoscopic Cytoreduction in Recurrent Ovarian Cancer: A Large, Single-Institution Experience. J Minim Invasive Gynecol. 2018;25(4):644–650. doi:10.1016/j.jmig.2017.10.024
3. Seror J, Bats AS, Bensaid C, Douay-Hauser N, Ngo C, Lecuru F. Risk of port-site metastases in pelvic cancers after robotic surgery. Eur j Surg Oncol. 2015;41(4):599–603. doi:10.1016/j.ejso.2015.01.003
4. Barraez D, Godoy H, McElrath T, Kredentser D, Timmins P. Low incidence of port-site metastasis after robotic assisted surgery for endometrial cancer staging: descriptive analysis. J Robot Surg. 2015;9(1):91–95. doi:10.1007/s11701-014-0491-y
5. Grant JD, Garg AK, Gopal R, et al. Isolated port-site metastases after minimally invasive hysterectomy for endometrial cancer: outcomes of patients treated with radiotherapy. Int j Gynecol. 2015;25(5):869–874. doi:10.1097/IGC.0000000000000424
6. Manvelyan V, Khemarangsan V, Huang K-G, Adlan A-S, Lee C-L. Port-site metastasis in laparoscopic gynecological oncology surgery: an overview. Gynecol Minimally Invasive Therapy. 2016;5(1):1–6. doi:10.1016/j.gmit.2015.06.009
7. Worley MJ, Slomovitz BM, Ramirez PT. Complications of laparoscopy in benign and oncologic gynecological surgery. Rev Obstet Gynecol. 2009;2(3):169–175.
8. Deshmukh U, McAdow M, Black J, Hui P, Azodi M. Isolated port site recurrence of node-negative clinical stage IB1 cervical adenocarcinoma. Gynecol Oncol Rep. 2017;20:54–57. doi:10.1016/j.gore.2017.03.001
9. Abu-Rustum NR, Rhee EH, Chi DS, Sonoda Y, Gemignani M, Barakat RR. Subcutaneous tumor implantation after laparoscopic procedures in women with malignant disease. Obstet Gynecol. 2004;103(3):480–487. doi:10.1097/01.AOG.0000114974.40512.c9
10. Rindos N, Curry CL, Tabbarah R, Wright V. Port-site metastases after robotic surgery for gynecologic malignancy. JSLS. 2014;18(1):66–70. doi:10.4293/108680813X13693422519271
11. Agarwala V, Ramaswamy A, Dsouza S, et al. Resection of Isolated Port Site Metastasis in Gall Bladder Cancers-Careful Selection and Perioperative Systemic Therapy May Improve Outcomes. Indian J Surg Oncol. 2018;9(3):427–431. doi:10.1007/s13193-018-0809-8
12. Baptiste CD,Buckley de Meritens A, Jones NL, et al. Port Site Metastases: A Survey of the Society of Gynecologic Oncology and Commentary on the Clinical Workup and Management of Port Site Metastases. J Minim Invasive Gynecol. 2017;24(4):592–598. doi:10.1016/j.jmig.2017.01.011
13. Bogani G, Dowdy SC, Cliby WA, et al. Incisional Recurrences After Endometrial Cancer Surgery. Anticancer Res. 2015;35(11):6097–6104.
14. Nunez MF, Sardi A, Jimenez W, et al. Port-site metastases is an independent prognostic factor in patients with peritoneal carcinomatosis. Ann Surg Oncol. 2015;22(4):1267–1273. doi:10.1245/s10434-014-4136-1
15. Martinez A, Querleu D, Leblanc E, Narducci F, Ferron G. Low incidence of port-site metastases after laparoscopic staging of uterine cancer. Gynecol Oncol. 2010;118(2):145–150. doi:10.1016/j.ygyno.2010.03.011
16. Huang KG, Wang CJ, Chang TC, et al. Management of port-site metastasis after laparoscopic surgery for ovarian cancer. Am J Obstet Gynecol. 2003;189(1):16–21. doi:10.1067/mob.2003.330
17. Cheong JY, Keshava A, Witting P, Young CJ. Effects of Intraoperative Insufflation With Warmed, Humidified CO2 during Abdominal Surgery: A Review. Ann Coloproctol. 2018;34(3):125–137. doi:10.3393/ac.2017.09.26
18. Dobronte Z, Wittmann T, Karacsony G. Rapid development of malignant metastases in the abdominal wall after laparoscopy. Endoscopy. 1978;10(2):127–130. doi:10.1055/s-0028-1098280
19. Lonnerfors C, Bossmar T, Persson J. Port-site metastases following robot-assisted laparoscopic surgery for gynecological malignancies. Acta Obstet Gynecol Scand. 2013;92(12):1361–1368. doi:10.1111/aogs.12245
20. Ndofor BT, Soliman PT, Schmeler KM, Nick AM, Frumovitz M, Ramirez PT. Rate of port-site metastasis is uncommon in patients undergoing robotic surgery for gynecological malignancies. Int j Gynecol. 2011;21(5):936–940.
21. Zivanovic O, Sonoda Y, Diaz JP, et al. The rate of port-site metastases after 2251 laparoscopic procedures in women with underlying malignant disease. Gynecol Oncol. 2008;111(3):431–437. doi:10.1016/j.ygyno.2008.08.024
22. Nagarsheth NP, Rahaman J, Cohen CJ, Gretz H, Nezhat F. The incidence of port-site metastases in gynecologic cancers. JSLS. 2004;8(2):133–139.
23. Vergote I, Marquette S, Amant F, Berteloot P, Neven P. Port-site metastases after open laparoscopy: a study in 173 patients with advanced ovarian carcinoma. Int j Gynecol. 2005;15(5):776–779. doi:10.1111/j.1525-1438.2005.00135.x
24. Heitz F, Ognjenovic D, Harter P, et al. Abdominal wall metastases in patients with ovarian cancer after laparoscopic surgery: incidence, risk factors, and complications. Int j Gynecol. 2010;20(1):41–46. doi:10.1111/IGC.0b013e3181c443ba
25. Ataseven B, Grimm C, Harter P, et al. Prognostic Impact of Port-Site Metastasis After Diagnostic Laparoscopy for Epithelial Ovarian Cancer. Ann Surg Oncol. 2016;23(Suppl 5):834–840. doi:10.1245/s10434-016-5415-9
26. Holub Z. Impact of laparoscopic surgery on immune function. Clin Exp Obstet Gynecol. 2002;29(2):77–81.
27. Sylla P, Kirman I, Whelan RL. Immunological advantages of advanced laparoscopy. Sur Clin North Am. 2005;85(1):1–18. doi:10.1016/j.suc.2004.09.005
28. Ost MC, Tan BJ, Lee BR. Urological laparoscopy: basic physiological considerations and immunological consequences. J Urol. 2005;174(4 Pt 1):1183–1188. doi:10.1097/01.ju.0000173102.16381.08
29. Asthana R, Oblak ML, Singh A, Mutsaers AJ. In vitro evaluation of a simulated pneumoperitoneum environment using carbon dioxide on canine transitional cell carcinoma. Veterinary Surg. 2018;47(3):412–420. doi:10.1111/vsu.12778
30. Zheng L, Zhou D, Lu L, Liu Z, Fang L. Effects of CO2 pneumoperitoneum on proliferation, apoptosis, and migration of gastrointestinal stromal tumor cells. Surg Endosc. 2019;33(10):3384–3395. doi:10.1007/s00464-018-06633-6
31. Molinas CR, Campo R, Elkelani OA, Binda MM, Carmeliet P, Koninckx PR. Role of hypoxia inducible factors 1α and 2α in basal adhesion formation and in carbon dioxide pneumoperitoneum-enhanced adhesion formation after laparoscopic surgery in transgenic mice. Fertil Steril. 2003;80:795–802. doi:10.1016/S0015-0282(03)00779-9
32. Ramirez PT, Wolf JK, Levenback C. Laparoscopic port-site metastases: etiology and prevention. Gynecol Oncol. 2003;91(1):179–189. doi:10.1016/S0090-8258(03)00507-9
33. Lee BR, Tan BJ, Smith AD. Laparoscopic port site metastases: incidence, risk factors, and potential preventive measures. Urology. 2005;65(4):639–644. doi:10.1016/j.urology.2004.09.067
34. Sellers GJ, Whelan RL, Allendorf JD, et al. An in vitro model fails to demonstrate aerosolization of tumor cells. Surg Endosc. 1998;12(5):436–439. doi:10.1007/s004649900698
35. Mathew G, Watson DI, Ellis T, De Young N, Rofe AM, Jamieson GG. The effect of laparoscopy on the movement of tumor cells and metastasis to surgical wounds. Surg Endosc. 1997;11(12):1163–1166. doi:10.1007/s004649900561
36. Curet MJ. Port site metastases. Am J Surg. 2004;187(6):705–712. doi:10.1016/j.amjsurg.2003.10.015
37. Targarona EM, Martínez J, Nadal A, et al. Cancer dissemination during laparoscopic surgery: tubes, gas, and cells. World J Surg. 1998;22(1):55–60. doi:10.1007/s002689900349
38. Paolucci V, Schaeff B, Schneider M, Gutt C. Tumor seeding following laparoscopy: international survey. World J Surg. 1999;23(10):989–995. doi:10.1007/s002689900613
39. Allardyce R, Morreau P, Bagshaw P. Tumor cell distribution following laparoscopic colectomy in a porcine model. Dis Colon Rectum. 1996;39(10 Suppl):S47–S52. doi:10.1007/BF02053805
40. Allardyce RA, Morreau P, Bagshaw PF. Operative factors affecting tumor cell distribution following laparoscopic colectomy in a porcine model. Dis Colon Rectum. 1997;40(8):939–945. doi:10.1007/BF02051202
41. Schneider C, Jung A, Reymond MA, et al. Efficacy of surgical measures in preventing port-site recurrences in a porcine model. Surg Endosc. 2001;15(2):121–125. doi:10.1007/s004640010069
42. Polat AK, Yapici O, Malazgirt Z, Basoglu T. Effect of types of resection and manipulation on trocar site contamination after laparoscopic colectomy: an experimental study in rats with intraluminal radiotracer application. Surg Endosc. 2008;22(5):1396–1401. doi:10.1007/s00464-007-9457-8
43. Lee SW, Gleason NR, Bessler M, Whelan RL. Port site tumor recurrence rates in a murine model of laparoscopic splenectomy decreased with increased experience. Surg Endosc. 2000;14(9):805–811. doi:10.1007/s004640000231
44. Zmora O, Weiss EG. Trocar Site Recurrence in Laparoscopic Surgery for Colorectal Cancer. Surg Oncol Clin N Am. 2001;10(3):625–638. doi:10.1016/S1055-3207(18)30054-1
45. Chaturvedi S, Bansal V, Kapoor R, Mandhani A. Is port site metastasis a result of systemic involvement? Indian j Urol. 2012;28(2):169–173. doi:10.4103/0970-1591.98458
46. Pearlstone DB, Mansfield PF, Curley SA, Kumparatana M, Cook P, Feig BW. Laparoscopy in 533 patients with abdominal malignancy. Surgery. 1999;125(1):67–72. doi:10.1016/S0039-6060(99)70290-4
47. Sugarbaker PH. Port site recurrence, an unintended consequence of laparoscopic resection of ovarian cancer. A case report. Int J Surg Case Rep. 2019;62:5–8. doi:10.1016/j.ijscr.2019.07.024
48. Coskun AK, Coskun ZY. Prevention from port-site metastasis. Arch Gynecol Obstet. 2015;292(2):239–240. doi:10.1007/s00404-015-3734-x
49. Agostini A, Robin F, Jais JP, et al. Peritoneal closure reduces port site metastases: results of an experiment in a rat ovarian cancer model. Surg Endosc. 2002;16(2):289–291. doi:10.1007/s00464-001-9063-0
50. Franklin ME, Rosenthal D, Abrego-Medina D, et al. Prospective comparison of open vs. laparoscopic colon surgery for carcinoma. Five-year results. Dis Colon Rectum. 1996;39(10 Suppl):S35–S46. doi:10.1007/BF02053804
51. Braumann C, Ordemann J, Wildbrett P, Jacobi CA. Influence of intraperitoneal and systemic application of taurolidine and taurolidine/heparin during laparoscopy on intraperitoneal and subcutaneous tumour growth in rats. Clin Exp Metastasis. 2000;18(7):547–552. doi:10.1023/A:1011988923523
52. Neuhaus SJ, Ellis T, Jamieson GG, Watson DI. Experimental study of the effect of intraperitoneal heparin on tumour implantation following laparoscopy. Br J Surg. 1999;86(3):400–404. doi:10.1046/j.1365-2168.1999.01031.x
53. Neuhaus SJ, Watson DI, Ellis T, Rofe AM, Jamieson GG. Influence of cytotoxic agents on intraperitoneal tumor implantation after laparoscopy. Dis Colon Rectum. 1999;42(1):10–15. doi:10.1007/BF02235176
54. Eshraghi N, Swanstrom LL, Bax T, et al. Topical treatments of laparoscopic port sites can decrease the incidence of incision metastasis. Surg Endosc. 1999;13(11):1121–1124. doi:10.1007/s004649901186
55. Gupta A, Watson DI, Ellis T, Jamieson GG. Tumour implantation following laparoscopy using different insufflation gases. ANZ J Surg. 2002;72(4):254–257. doi:10.1046/j.1445-2197.2002.02385.x
56. Ludemann W, Smith E, Smith E, Ellis T, Jamieson GG. Jamieson. Tumor implantation during laparoscopy using different insufflation gases - an experimental study using cultured cancer cells. Minimally Invasive Therapy Allied Tech. 2003;12(6):310–314. doi:10.1080/13645700310017868
57. Agostini A, Robin F, Aggerbeck M, Jaïs JP, Blanc B, Lécuru F. Influence of peritoneal factors on port-site metastases in a xenograft ovarian cancer model. BJOG. 2001;108(8):809–812.
58. Peng Y, Zheng M, Ye Q, Chen X, Yu B, Liu B. Heated and humidified CO2 prevents hypothermia, peritoneal injury, and intra-abdominal adhesions during prolonged laparoscopic insufflations. J Surg Res. 2009;151(1):40–47. doi:10.1016/j.jss.2008.03.039
59. Peng Y, Yang H, Ye Q, Zhou H, Zheng M, Shi Y. Inhibition of peritoneal dissemination of colon cancer by hyperthermic CO2 insufflation: A novel approach to prevent intraperitoneal tumor spread. PLoS One. 2017;12(2):e0172097. doi:10.1371/journal.pone.0172097
60. Zhao J, Lv Y, Cai Y, et al. Hyperthermic carbon dioxide pneumoperitoneum reinforces the inhibition of 5-FU on the proliferation and invasion of colon cancer. Oncol Rep. 2017;37(1):492–500. doi:10.3892/or.2016.5229
61. Lago V, Gimenez L, Matute L, et al. Port site resection after laparoscopy in advance ovarian cancer surgery: time to abandon? Surg Oncol. 2019;29:1–6. doi:10.1016/j.suronc.2019.01.007
62. Maker AV, Butte JM, Oxenberg J, et al. Is port site resection necessary in the surgical management of gallbladder cancer? Ann Surg Oncol. 2012;19(2):409–417. doi:10.1245/s10434-011-1850-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.