")
Back to Journals » Clinical Ophthalmology » Volume 10
The outcomes and prognostic factors of vitrectomy in chronic diabetic traction macular detachment
Authors Abu Najma M, Al-Dhibi H, Abboud E, Al Zahrani Y, Alharthi E, Alkharashi A, Ghazi N
Received 18 October 2015
Accepted for publication 10 February 2016
Published 26 August 2016 Volume 2016:10 Pages 1653—1661
DOI https://doi.org/10.2147/OPTH.S98555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Muneera A Abunajma,1 Hassan Al-Dhibi,1 Emad B Abboud,1 Yahya Al Zahrani,1 Essam Alharthi,2 Abdullah Alkharashi,3 Nicola G Ghazi1,4
1Vitreoretinal Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Al Hokama Eye Center, Riyadh, Saudi Arabia; 3Department of Ophthalmology, College of Medicine, King Saud University Riyadh, Saudi Arabia; 4Department of Ophthalmology, University of Virginia, Charlottesville, VA, USA
Purpose: To investigate the outcomes of pars plana vitrectomy (PPV) for chronic diabetic traction macular detachment (CTMD).
Methods: Ninety-six eyes that underwent PPV for CTMD of at least 6 months duration were retrospectively analyzed. Retinal reattachment rate, final vision, and prognostic factors for poor visual outcome were the main outcome measures.
Results: All eyes had long-standing TMD (median 12, range: 6–70 months). The median postoperative follow-up was 15 (range: 3–65) months. Eighty-seven eyes (90.6%) had their retina and macula reattached after one PPV. At final examination, 84 eyes (87.5%) had stable vision or at least one line improvement, and three had no light perception. Seventeen (17.7%) and 41 (43%) eyes had preoperative visual acuity of ≥20/200 and ≥5/200 as compared to 40 (41.6%; P=0.0005) and 64 (66.7%; P=0.0014) eyes at final follow-up, respectively. Age >50 years (Odds ratio [OR] =5.84, 95% confidence interval [CI] =1.53–22.19, P=0.01), preoperative vision <20/400 (OR =7.012, 95% CI =1.82–26.93, P=0.005), and ischemic macula (OR =14.13, 95% CI =3.61–55.33, P<0.001) were significantly associated with final vision <20/400.
Conclusion: PPV for CTMD may be beneficial particularly in patients who are relatively younger and have good baseline vision and no macular ischemia.
Keywords: chronic diabetic traction macular detachment, diabetic retinopathy, diabetic traction macular detachment, pars plana vitrectomy
Introduction
Although diabetic retinopathy used to lead to blindness in many cases,1 most of its complications are currently treatable, particularly with the advent of laser photocoagulation and pars plana vitrectomy (PPV).2,3 With the introduction of PPV by Machmer,4,5 treatment of some of the previously untreatable proliferative complications became possible. The indications for PPV in diabetic retinopathy have evolved over the years. Currently, the most common indications include severe nonclearing vitreous hemorrhage, traction retinal detachment recently involving the macula, combined traction and rhegmatogenous retinal detachment,6–9 dense premacular hemorrhage,10 ghost cell glaucoma,11 macular edema with premacular hyaloid traction,12 and cataract with severe proliferative diabetic retinopathy.13,14 Although the majority of diabetic vitrectomies were performed for nonresolving vitreous hemorrhage in the 1970s,7 traction macular detachment (TMD) became the most common indication, accounting for 40% of diabetic vitrectomies in the late 1980s.15
Vitrectomy is not traditionally performed for extramacular traction detachment since the incidence of progression to involve the macula was reported to be about 15% per year, which is lower than the reported failure rate for surgery.16 However, in the event of progressive traction detachment threatening the macula, early vitrectomy may play a role in preserving vision.17–19 In contrast, vitrectomy for traction detachment is traditionally considered when the macula has been detached for only a relatively short period, usually less than 6 months. The role of vitrectomy is less clear for more chronic diabetic TMD, and surgery has not been traditionally recommended because such chronic detachments are usually associated with a thin and atrophic retina, as well as extensive, thick, and plaque-like, fibrovascular membranes that are typically very adherent to the retina.20 Because of these factors and the associated retinal degeneration, the anatomic and visual outcomes may be limited. Therefore, surgery for such cases is a challenge and requires a careful assessment of the risks and benefits, and a proper case selection is critical to optimize surgical outcomes. However, the literature is relatively scarce regarding chronic diabetic TMD, and the guidelines for surgical intervention are not well explored. Therefore, the approach to such cases has been largely guided by the traditional teaching as already discussed. Since a significant number of cases seen in our practice have long-standing diabetic TMD, our patient population provides a unique opportunity to study the outcome of PPV surgery in such eyes and to identify potential prognostic factors that may guide case selection for surgical intervention.
Methods
After obtaining Institutional Review Board approval from the King Khaled Eye Specialist Hospital, we retrospectively reviewed the records of all patients who underwent PPV for chronic diabetic traction retinal detachment at the King Khalid Eye Specialist Hospital between January 2005 and July 2011. No consent was obtained since this is a retrospective chart review study. Eyes with traction detachment involving the center of the macula for more than 6 months duration were included. Eyes with traction detachment threatening the fovea, combined traction and rhegmatogenous retinal detachment, or a history of other macular pathology, trauma, or advanced glaucoma were excluded. Only eyes that were followed up for at least 3 months were included. For all eyes, data were collected from pre-, intra-, and postoperative evaluations.
The following general variables were recorded for each patient: age, sex, duration of follow-up, type and duration of diabetes, and the presence of hypertension or nephropathy. In addition to details of a complete ophthalmic evaluation, the following preoperative ophthalmic variables were collected: Snellen visual acuity, laterality, previous ocular history and surgeries including previous retinal laser procedures, history of intravitreal bevacizumab injection directly preoperatively, the presence of vitreous hemorrhage or iris neovascularization, the appearance of the macula and macular vessels (ischemic macula with sclerotic macular vessels), the presence of thick fibrovascular tissue, and the approximate duration of macular detachment as represented by the documented time lapse between the diminution of vision from macular involvement and surgery. We attempted to collect data regarding anatomic details of the TMD, such as the shape and height, from preoperative ultrasound and optical coherence tomography images, as well as the perfusion status of the detached macula from fluorescein angiography, but such data were very limited and was not included. Preoperative bevacizumab was used only in eyes with signs of active membranes, vitreous hemorrhage, or iris neovascularization. It was not used in eyes with completely involuted retinopathy. Eyes were operated on within 4–7 days after preoperative injection.
The operative variables that were collected included the details of the macular anatomy, the appearance of the macular vasculature, the length of the procedure, the concomitant performance of pars plana lensectomy, phacoemulsification, or endolaser, the occurrence of iatrogenic retinal breaks, their number, and the use of tamponade (silicone oil or gas). Signs of macular ischemia were subjective and based on the surgeon’s experience but included either complete sclerosis and whitening of the large macular vessels or sclerosis of major tributaries of these vessels to the foveal area.
In addition to postoperative visual acuity along with retinal and macular status, the following postoperative complications were recorded: retinal detachment, corneal decompensation, high intraocular pressure, vitreous hemorrhage, new onset neovascular glaucoma (NVG), progressive cataract, and severe inflammation. In addition, the type, number, and causes of additional ophthalmic procedures were noted.
Univariate analysis was performed with the chi-square and Fisher’s exact test to determine which of the pre-, intra-, and/or postoperative variables collected were associated with a poor visual or anatomic outcome. Subsequently, an entry method multiple logistic regression analysis was used for the following preoperative variables to determine the strongest predictors of a poor visual outcome: preoperative visual acuity, age, the ischemic appearance of the retina, preoperative laser, preoperative intravitreal bevacizumab, and the duration of retinal detachment. Odds ratios (OR) were used to determine the magnitude and direction of associations. For statistical analysis, a poor visual outcome was defined as a visual acuity at final follow-up of less than 20/400.
Results
Ninety-six eyes of 88 patients were included in the study. Sixty-five patients were males (73.8%) and 23 were females (26.2%). The operated eye was the right eye in 32 patients (33.3%) and the left in 48 patients (50%), while eight patients (9%) had bilateral PPV for TMD (Table 1).
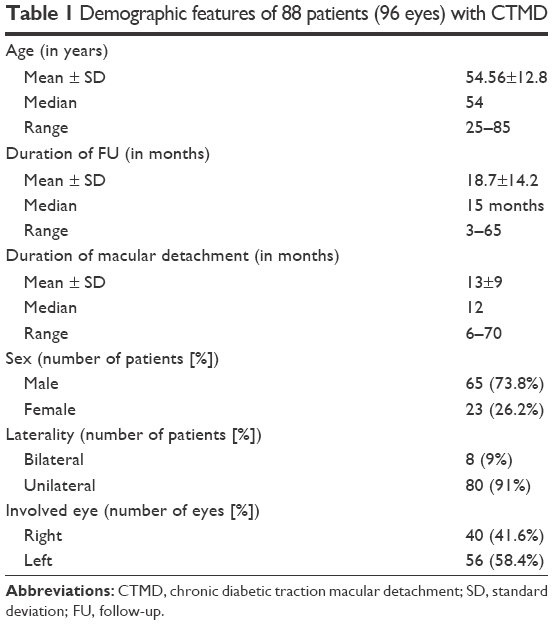 | Table 1 Demographic features of 88 patients (96 eyes) with CTMD |
Eighty-four eyes (87.5%) had stable visual acuity or, at least, one line improvement at final examination, but nine eyes (9%) had worse visual acuity, and three eyes had no light perception (NLP). The preoperative visual acuity was 20/200 or better in 17 eyes (17.7%) and 5/200 or better in 41 eyes (43%). Forty of the 96 eyes (41.6%) achieved a final visual acuity of 20/200 or better (P=0.0005), and 64 of 96 eyes (66.7%) had a final visual acuity of 5/200 or better (P=0.0014; Table 2). The median visual acuity significantly improved from 5/200 (range: light perception to 20/60) to 20/300 (range: NLP to 20/30) after a median follow-up of 15 months (range: 3–65 months, with only four eyes having a follow-up of only 3 months), despite the fact that all eyes had long-standing TMD (median 12 months, range: 6–70 months).
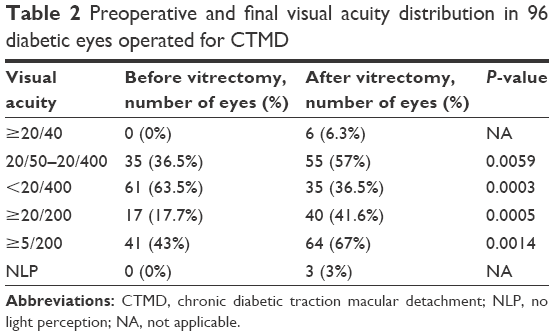 | Table 2 Preoperative and final visual acuity distribution in 96 diabetic eyes operated for CTMD |
Various systemic and perioperative (pre-, intra-, and postoperative) ophthalmic factors were analyzed by univariate analysis to determine whether they influenced the final visual outcome. Three preoperative variables were statistically significantly (P<0.05) associated with greater likelihood of final visual acuity of 20/400 or worse. These factors were 1) age older than 50 years (P=0.024), 2) preoperative visual acuity of <20/400 (P<0.001), and 3) ischemic macula (P<0.001). Of 66 eyes of patients aged >50 years, 29 eyes (43.9%) had a final visual acuity of <20/400, as compared to only six eyes out of 30 patients (20%) aged <50 years. The difference was statistically significant (P=0.024). Thirty-one out of 61 eyes (50.8%) with preoperative visual acuity of <20/400 had visual acuity of less than 20/400 at final follow-up compared to only four out of 35 patients with preoperative visual acuity of ≥20/400 (P<0.001). The macular perfusion status as judged clinically or intraoperatively was found to have a significant influence on the final visual outcome. Thirty of 54 eyes (55.6%) with ischemic macula as judged by the treating physician were found to have final visual acuity of 20/400 or less compared to only four out of 41 eyes (9.8%) with nonischemic macula (P<0.001).
All the other preoperative variables analyzed in this study including type of diabetes, duration of diabetes, existence of prior panretinal laser photocoagulation, use of preoperative intravitreal bevacizumab, iris neovascularization, lens status, presence of vitreous hemorrhage, presence of thick fibrovascular tissue (according to the judgment and description of the treating physician), and the duration of retinal detachment (6–12 months vs >12 months) were not significantly associated with the final visual outcome (Table S1). Interestingly, 27 out of 70 eyes (38.6%) with TMD of 6–12 months duration were found to have a poor visual outcome (<20/400), compared to eight of 26 eyes (30.8%) with duration TMD duration of more than 12 months. This difference was not statistically significant (P=0.63). After adjusting for confounding variables through multiple logistic regression analysis, age >50 years (OR =5.84, 95% CI =1.53–22.19, P=0.01), preoperative visual acuity of <20/400 (OR =7.012, 95% CI =1.82–26.93, P=0.005) and ischemic macula (OR =14.13, 95% CI =3.61–55.33, P<0.001) continued to be the only three factors significantly associated with poor final visual outcome of less than 20/400.
During PPV, 89 eyes (92.7%) received endolaser treatment, 53 eyes (55%) required intraocular tamponade (silicone oil 14 eyes (14.5%) and long-acting gas (C3F8) in 39 eyes (40.5%)), 26 eyes (27%) required cataract extraction surgery (lensectomy 3 (3.1%) eyes and phacoemulsification in 23 eyes (24%)) to clear the media for vitrectomy, and 36 eyes (37.5%) developed iatrogenic breaks. None of these intraoperative variables, including iatrogenic breaks, had a significant association with the final visual outcome.
Eighty-seven eyes (90.6%) had their retina and macula reattached after one vitrectomy (Figure 1). Six eyes had persistent traction retinal detachment; none of them were reoperated on due to poor prognosis associated with severe ischemia or the development of NVG. Two eyes developed rhegmatogenous retinal detachment and were successfully reattached by a second vitrectomy. Only one eye developed combined traction and rhegmatogenous detachment and because of poor prognosis, it was not reoperated on. Persistent subretinal fluid in the absence of retinal breaks or traction was found in three eyes, none of which required any intervention, and the fluid resolved spontaneously. Three eyes were complicated with the formation of epiretinal membranes, two of them needed vitrectomy. Eight eyes developed vitreous hemorrhage, all in the first 4 postoperative weeks, and only one required another vitrectomy for dense nonresolving vitreous hemorrhage. NVG was present in four eyes postoperatively, but only two of these developed this complication after vitrectomy, while the other two had the condition before surgery. One eye developed endophthalmitis and was treated with vitrectomy and intravitreal antibiotics (Table 3). None of the postoperative complications had a significant association with the final visual outcome. However, some of these complications may have occurred too infrequently to show statistical significance. Three eyes ended up with NLP due to retinal detachment and NVG.
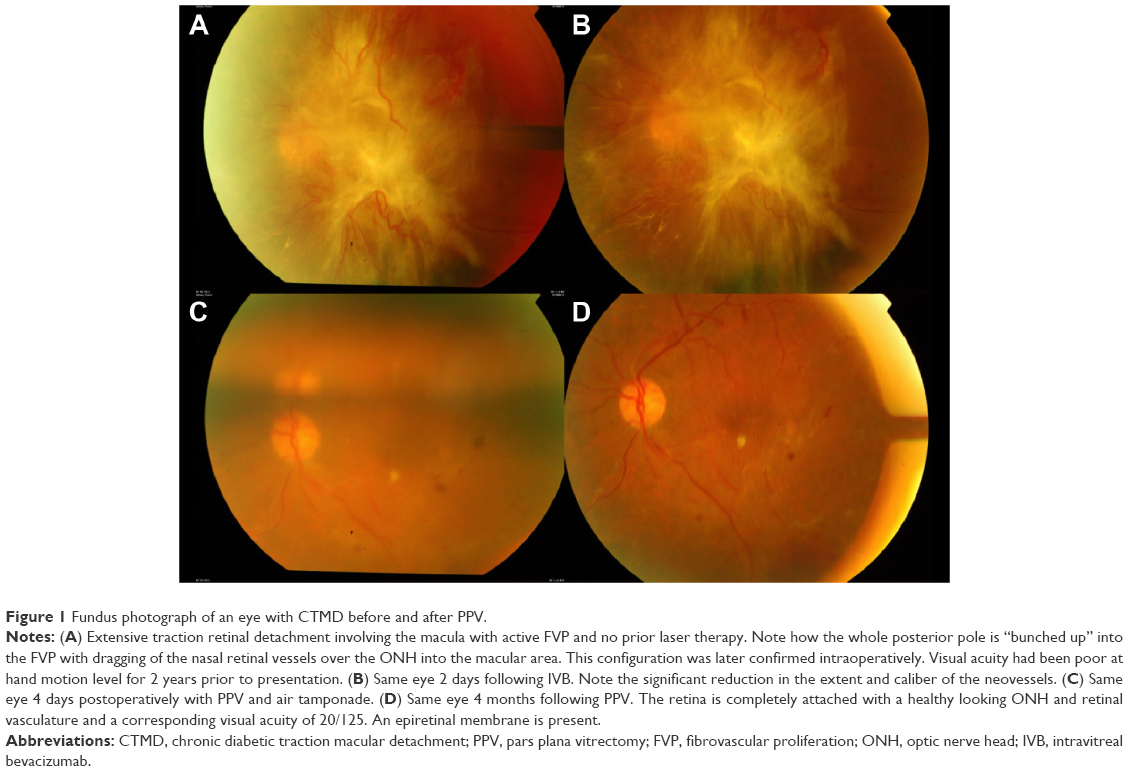 | Figure 1 Fundus photograph of an eye with CTMD before and after PPV. |
 | Table 3 Postoperative complications that developed in 55 eyes (54.3%) |
Discussion
This retrospective study of the outcome of vitrectomy in 96 eyes with TMD of more than 6 months duration showed positive results, with 87.5% of those eyes having stable final visual acuity or gaining, at least, one line compared to their preoperative acuity. In addition, 66.7% and 41.6% of the eyes had a final visual acuity of ≥5/200 and ≥20/200 compared to 43% and 17.7% at baseline, respectively. This relatively successful visual result was associated with a good anatomical outcome of 90.6% retinal reattachment rate following a single procedure.
Our results are comparable to those reported in the literature despite the fact that our study population was solely composed of eyes with long-standing TMD (median 12 months) as opposed to the previous studies (Table 4). For example, according to previous studies, visual improvement or stabilization after vitrectomy for TMD varied from 57% to 89% of eyes. In addition, 22%–72% of eyes have been reported to achieve a visual acuity of 5/200 or better, with a final anatomic success rate of 64%–93%.21–33 Knowing that the latest report we found dates back to 2003 may partially explain our comparative outcome due to the improvement in surgical techniques and equipment over the past few years, such as the higher cut rates vitrectomy machines, better illumination and viewing systems, as well as the availability of staining material for the visualization of hyaloid, epiretinal membranes, and the layers of vitreous schisis.
 | Table 4 Summary of some studies reporting vitrectomy results for diabetic traction retinal detachment over the past three decades |
In our statistical analysis, and among multiple systemic and pre-, intra-, and postoperative ocular variables, only three preoperative factors were found to be associated with a poor visual outcome, namely, 1) macular ischemia that had the strongest prediction with an OR of 14.13, followed by 2) preoperative visual acuity of <20/400 with an OR of 7.012, and 3) age >50 years with an OR of 5.840.
To our knowledge, the macular perfusion status has not been previously studied as a predictive factor for the visual outcome of vitrectomy in eyes with diabetic TMD. But our finding of a strong association between poor macular perfusion and the poor visual outcome is not surprising, knowing the direct negative effect of ischemia on the inner retinal layers, leading to a defective transmission of the visual signal between the photoreceptors and the optic nerve fibers. Although the foveal and outer retinal oxygenation in the macula may improve, inner macular perfusion is not expected to be altered by macular reattachment after surgery; thus, the poor visual outcome observed in such cases in our study. It is acknowledged that it is hard to assess macular perfusion and ischemia without performing ancillary testing such as fluorescein angiography. However, it is our experience that in such eyes with extensive tractional fibrovascular proliferation with TMD, a meaningful angiogram is almost impossible to perform. Accordingly, most of our information regarding the macular perfusion status was obtained from the surgeon’s pre- or intraoperative assessment of the macular vasculature. Similar to our finding, other authors have reported a correlation between poor preoperative visual acuity and a less successful visual outcome.25,28,32 This is likely because eyes with poor baseline vision may represent a subgroup of eyes with a more advanced and chronic disease with increased severity, complexity and chronicity of detachment, and a subsequent higher risk of intra- and postoperative complications. However, our study could not confirm this hypothesis since these variables were not associated with a poor visual outcome. Alternatively, eyes with poor vision at baseline may have irreversibly affected outer retina and photoreceptors that limit postoperative visual recovery. La Heij et al27 reported that age >50 years is a strong predictor of poor visual outcome, which supports our finding. This can probably be explained by a longer duration of diabetes mellitus, worse microvascular complications in older patients, in addition to a slow repair process in older diabetics.34–36
In contrast to our findings, a review of the literature showed that iris neovascularization, long-standing retinal detachment, lack of preoperative pan retinal photocoagulation (PRP), intraoperative iatrogenic breaks, and lensectomy were associated with a worse visual outcome following vitrectomy.24,27,30,37–39 Several studies documented that the lack of preoperative PRP and the presence of preoperative iris neovascularization was associated with poorer visual prognosis due to the development of NVG postoperatively.24,27,30 We were not able to reproduce either of these findings. On one hand, this discrepancy can be explained by the small number of eyes with preoperative iris neovascularization in our study. On the other hand, most of the reported studies date back to the era when endolaser and/or anti-vascular endothelial growth factor (VEGF) agents were not available, thus not allowing the surgeons to control the active proliferative state of the disease promptly either preoperatively by anti-VEGF agents and/or intraoperatively by endolaser. We hypothesize that since all our cases received endolaser and/or preoperative bevacizumab, preoperative iris neovascularization and the lack of preoperative PRP did not turn out to be significant variables in determining the final visual outcome.
Interestingly, the use of preoperative bevacizumab was not a significant factor for the final visual outcome. It appears that although the use of preoperative bevacizumab has been reported to facilitate surgical maneuvers during vitrectomy and to reduce intra- and postoperative bleeding and complications,37,38,40,41 the final visual outcome in chronic TMD does not appear to be dependent on the use of preoperative bevacizumab. This may be attributed to the significant effects of baseline acuity and degree of anatomical alterations related to the disease, such as macular ischemia, factors that preoperative bevacizumab use may not be able to alter.
In contrast to the findings of the previous studies,24,27 eyes with longer duration of TMD did not appear to have a worse final visual outcome. This could be attributed to the different study population included in our study. All our patients had macular detachment for more than 6 months duration (median 12 months). However, even when we compared the outcomes between eyes with 6–12 months duration of macular detachment to those with longer duration macular detachment, no significant differences regarding the final visual or anatomical outcomes were noted. This suggests that once the macula has been detached for more than 6 months, subsequent changes have minimal or no effect on the outcome.
Both lensectomy and the creation of iatrogenic retinal break during vitrectomy were also previously associated with an increased risk of poor postoperative visual results.25,32 Our study does not support these findings. The reasons for the discrepancy may be multifactorial. For example, the negative effect of lensectomy has been thought to be due to the elimination of the barrier between the vitreous cavity and the anterior segment allowing for angiogenic factors to circulate to the anterior segment and lead to postoperative NVG.24,27 Cataracts dense enough to preclude optimal view to the fundus were extracted by phacoemulsification and not lensectomy in almost all (88.5%) cases in our study. Unlike lensectomy, the posterior capsule is not violated during phacoemulsification, thus maintaining a partial barrier between the vitreous and anterior segment, which in turn is thought to decrease the risk of iris neovascularization and NVG development postoperatively.24,27 In addition, the development of endolaser for immediate intraoperative retinal ablative therapy as well as anti-VEGF agents for preoperative use may have allowed for a reduced incidence of such postoperative complications even in eyes that had cataract extraction.
Similarly, the development of better surgical adjuvants such as triamcinolone to identify residual vitreous and traction in the area of iatrogenic breaks, Tano scrapers and newer generation microsurgical forceps such as end-gripping forceps for removal of thin residual traction, as well as endolaser to seal breaks immediately intraoperatively, seem to have a beneficial effect in decreasing the incidence of retinal detachment following surgery, subsequently minimizing the potential negative effects of iatrogenic breaks on the final visual outcome. The beneficial effects of the aforementioned surgical adjuvants may be even more evident in our study, especially since we had a higher rate of iatrogenic breaks (37.5% of eyes) compared to the literature.25,31 Although this may be related to the more complex and chronic detachments included in our study, with subsequently thicker membranes and thinner atrophic and cystic retinas predisposing to tears during dissection, this did not appear to influence the final visual and anatomical outcomes.
Conclusion
In conclusion, despite the limitations of this retrospective study including the lack of fluorescein angiography, optical coherence tomography, and ultrasonography data as well as information regarding the general health status of most of our patients, the findings indicate that vitrectomy for eyes with chronic TMD may be beneficial, particularly in patients who are younger and have a relatively good baseline visual acuity and a nonischemic macula. Although the duration of macular detachment is a significant negative predictive factor for the final visual outcome, the traditional teaching recommending PPV for TMD recently (<6 months) involving the macula and suggesting avoiding PPV for cases in which the macula has been detached for more than 6 months because of poor surgical outcomes may not be totally accurate. Our study shows that the majority of such eyes do relatively well with surgery and retain ambulatory vision. These findings suggest that the traditional teaching should be modified. Our promising results as compared to the previous reports may be at least in part explained by the most recent developments in surgical techniques and intraoperative maneuvers.
Disclosure
No financial or conflicting relationship exists for any author. The authors report no conflicts of interests in this work.
References
Duke-Elder S, Dobree JH. Diabetes mellitus. In: Duke-Elder D, editor. System of Ophthalmology. London, UK: Kimpton; 1967;408–448. | ||
Aiello LM, Beetham WP, Balodimos MC, Koncz L. Ruby-laser photocoagulation of early diabetic neovascular retinopathy: preliminary report of a long-term controlled study. Trans Am Ophthalmol Soc. 1969;67:39–67. | ||
Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. Ophthalmology. 1981;88:583–600. | ||
Machmer R. Reminiscences after 25 years of pars plana vitrectomy. Am J Ophthalmol. 1995;119:505–510. | ||
Machmer R, Buettner H, Norton RWD, Parel JM. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75:813–820. | ||
Aaberg TM. Results of 100 consecutive vitrectomy procedures. In: McPherson A, editor. New and Controversial Aspects of Vitreoretinal Surgery. St Louis, MO: CV Mosby; 1977;245–249. | ||
Aaberg TM. Vitrectomy for diabetic retinopathy. In: Freeman HM, Hirose T, Schepens CL, editors. Vitreous Surgery and Advances in Fundus Diagnosis and Treatment. New York, NY: Appleton-Century-Crofts; 1977;297–313. | ||
Eifriq D, Lockhart DL, Breglund RD, Knobloch WH. Pars plana vitrectomy. Ophthalmol Surg. 1978;9:76–88. | ||
Kloti R. Indications for vitrectomy and results in 115 cases. In: Mc Pherson A, editor. Controversial Aspects of Vitreoretinal Surgery. St Louis, MO: CV Mosby; 1977;237–244. | ||
Thompson JT, de Bustros S, Michels RG, et al. Results of vitrectomy for proliferative diabetic retinopathy. Ophthalmology. 1986;93:1571–1574. | ||
Rinkoff JS, de Juan E Jr, McCuen BW 2nd. Silicone oil for retinal detachment with advanced proliferative vitreoretinopathy following failed vitrectomy for proliferative diabetic retinopathy. Am J Ophthalmol. 1986;101:181–186. | ||
Lewis H, Abrams GW, Blumenkranz MS, Campo RV. Vitrectomy for diabetic macular traction and edema associated with posterior hyaloidal traction. Ophthalmology. 1992;99:753–759. | ||
Benson WE, Brown GC, Tasman W, McNamara JA. Extracapsular cataract extraction, posterior chamber lens insertion and pars plana vitrectomy in one operation. Ophthalmology. 1990;97:819–921. | ||
Blanckenship GW, Flynn HW Jr, Kokame GT. Posterior chamber intraocular lens insertion during pars plana lensectomy and vitrectomy for complications of proliferative diabetic retinopathy. Am J Ophthalmol. 1989;108:1–5. | ||
Aaberg TM, Abrams GW. Changing indications and techniques for vitrectomy in the management of complications of diabetic retinopathy. Ophthalmology. 1987;94:775–779. | ||
Charles S, Flinn CE. The natural history of diabetic extramacular traction retinal detachment. Arch Ophthalmol. 1981;99:66–68. | ||
Early vitrectomy for severe proliferative diabetic retinopathy in eyes with useful vision. Results of a randomized trial – Diabetic Retinopathy Vitrectomy Study Report 3. The Diabetic Retinopathy Vitrectomy Study Research Group. Ophthalmology. 1988;95:1307–1320. | ||
Early vitrectomy for severe proliferative diabetic retinopathy in eyes with useful vision. Clinical application of results of a randomized trial – Diabetic Retinopathy Vitrectomy Study Report 4. The Diabetic Retinopathy Vitrectomy Study Research Group. Ophthalmology. 1988;95:1321–1334. | ||
Packer AJ. Vitrectomy for progressive macular traction associated with proliferative diabetic retinopathy. Arch Ophthalmol. 1987;105:1679–1683. | ||
Eliott D, Lee MS, Abrams GW. Proliferative diabetic retinopathy: principles and techniques of surgical treatment. In: Ryan SJ, editor. Retina. Philadelphia, PA: Elsevier Health Sciences; 2006:2413–2449. | ||
Aaberg TM. Clinical results in vitrectomy for diabetic traction retinal detachment. Am J Ophthalmol. 1979;88:246–253. | ||
Aaberg TM. Pars plana vitrectomy for diabetic traction retinal detachment. Ophthalmology. 1981;88:639–642. | ||
Blankenship GW. Preoperative prognostic factors in diabetic pars plana vitrectomy. Ophthalmology. 1982;89:1246–1249. | ||
Castellarin A, Grigorian R, Bahgat N, Del Priore L, Zabrin MA. Vitrectomy with silicone oil infusion in severe diabetic retinopathy. Br J Ophthalmol. 2003;87:318–321. | ||
Clifford MR, Ronald GM, Cheryl AM, Rice TA. Pars plana vitrectomy for complicated retinal detachments. Ophthalmology. 1983;90:1323–1327. | ||
Hutton W, Bernstein I, Fuller D. Diabetic traction retinal detachment: factors influencing final visual acuity. Ophthalmology. 1980;87:1071–1077. | ||
La Heij EC, Tecim S, Kessels AG, Liem AT, Japing WJ, Hendrikse F. Clinical variables and their relation to visual outcome after vitrectomy in eyes with diabetic retinal traction detachment. Graefes Arch clin Exp Ophthalmol. 2004;242:210–217. | ||
Meier P, Wiedemann P. Vitrectomy for traction macular detachment in diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 1997;235:569–574. | ||
Miller SA, Butler JB, Myers FL, Bresnick GH. Pars Plana Vitrectomy: treatment for tractional macula detachment secondary to proliferative diabetic retinopathy. Arch Ophthalmol.1980;98:659–664. | ||
Rice TA, Michels RG, Rice EF. Vitrectomy for diabetic traction retinal detachment involving the macula. Am J Ophthalmol. 1983;95:22–23. | ||
Steinmetz RL, Grizzard S, Hammer ME. Vitrectomy for diabetic traction retinal detachment using the multiport illumination system. Ophthalmology. 2002;109:2303–2307. | ||
Thompson JT, de Bustros S, Michels RG, Rice TA. Results and prognostic factors in vitrectomy for diabetic traction retinal detachment of the macula. Arch Ophthalmol. 1987;105:497–502. | ||
Tolentino PI, Freeman HM, Tolintino FL. Closed vitrectomy in the management of diabetic traction retinal detachment. Ophthalmology. 1980;87:1078–1089. | ||
Mandavilli BS, Santos JH, Van Houten B: Mitochondrial DNA repair and aging. Mutat Res. 2002;509:127–151. | ||
Straton IM, Adler Al, Neil HA, et al. Association of glycemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 2000;321:405–412. | ||
The diabetes control and complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group: retinopathy and nephropathy in patients with type 1 diabetes 4 years after a trial of intensive therapy. N Engl J Med. 2000;342:381–389. | ||
Avery RL, Pearlman J, Pieramici DJ, et al. Intravitreal bevacizumab (Avastin) in the treatment of proliferative diabetic retinopathy. Ophthalmology. 2006;113(10):1695.e1–e15. | ||
Chen E, Park CH. Use of intravitreal bevacizumab as a preoperative adjunct for tractional retinal detachment repair in severe proliferative diabetic retinopathy. Retina. 2006;26:699–700. | ||
Smith JM, Steel DH. Anti-vascular endothelial growth factor for prevention of postoperative vitreous cavity hemorrhage after vitrectomy for proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2011;5:CD008214. | ||
Singh H, Grand MG. Treatment of blood induced glaucoma by pars plana vitrectomy. Retina. 1981;1:255–257. | ||
Zhao LQ, Zhu H, Zhao PQ, Hu YQ. A systematic review and meta-analysis of clinical outcomes of vitrectomy with or without intravitreal bevacizumab pretreatment for severe diabetic retinopathy. Br J Ophthalmol. 2011;95:1216–1222. | ||
Williams DF, Williams GA, Hartz A, Mieler WF, Abrams GW, Aebreg TM. Results of vitrectomy for diabetic traction retinal detachments using the en bloc excision technique. Ophthalmology. 1989;96:752–758. | ||
Abrams GW, Williams GA. “En block” excision of diabetic membranes. Am J Ophthalmol. 1987;103:302–308. | ||
Rice TA, Michels RG. Vitrectomy for diabetic rhegmatogenous retinal detachment. Am J Ophthalmol. 1983;95:34–44. |
Supplementary material
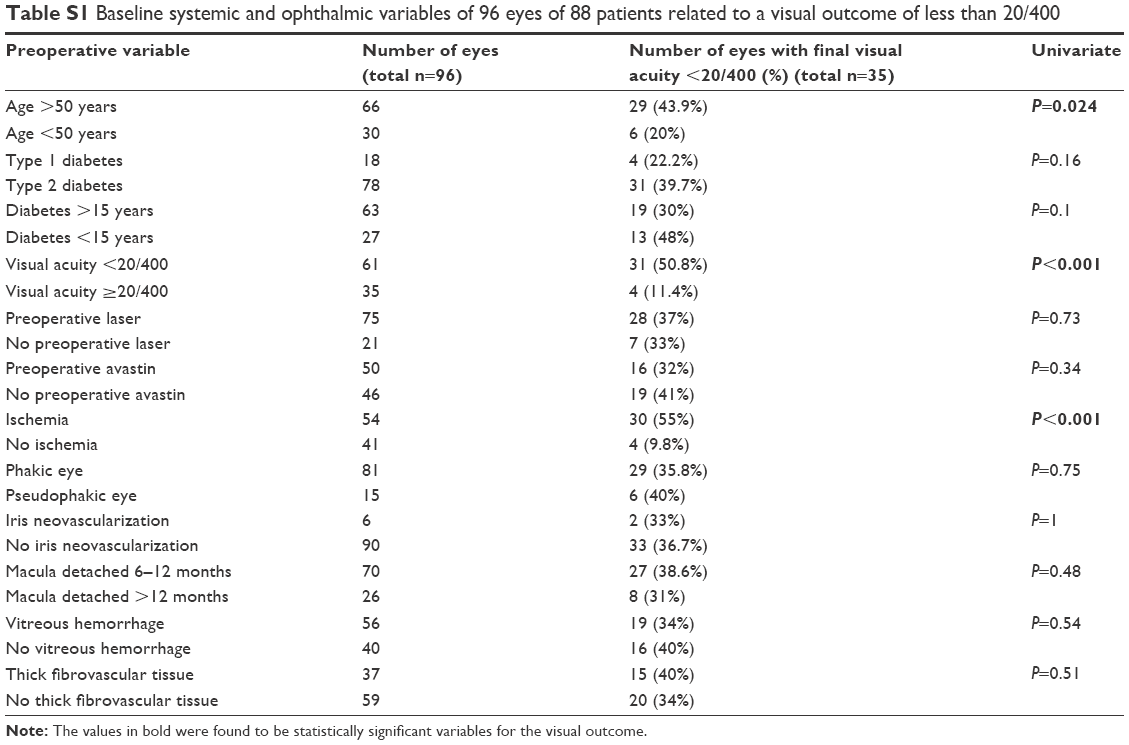 | Table S1 Baseline systemic and ophthalmic variables of 96 eyes of 88 patients related to a visual outcome of less than 20/400 |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.