")
Back to Journals » Infection and Drug Resistance » Volume 14
The Occurrence of rtA194T Mutant After Long-Term Lamivudine Monotherapy Remains Sensitive to Tenofovir Disoproxil Fumarate: A Case Report
Authors Li J, Zhang D, Zhang X
Received 3 December 2020
Accepted for publication 3 March 2021
Published 15 March 2021 Volume 2021:14 Pages 1013—1017
DOI https://doi.org/10.2147/IDR.S295060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Jing Li,1 Donghua Zhang,1 Xinxin Zhang1,2
1Department of Infectious Diseases, Research Laboratory of Clinical Virology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Sino-French Research Centre for Life Sciences and Genomics, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Xinxin Zhang
Department of Infectious Diseases, Research Laboratory of Clinical Virology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, No. 197 Ruijin Second Road, Shanghai, 200025, People’s Republic of China
Tel +86 21-64370045 ext 681088
Email [email protected]
Abstract: Tenofovir disoproxil fumarate (TDF) is recommended as first-line agents in chronic hepatitis B (CHB) patients for its high antiviral effects and high barrier to resistance. It is controversial whether the rtA194T mutation truly confers resistance against TDF. We present here a 62-year-old CHB patient who occurred rtL180M, rtM204V and rtA194T mutants after lamivudine (LAM) monotherapy for 9 years. TDF was introduced in replacement of LAM and led to Hepatitis B Virus (HBV) DNA undetectable in 1 month, maintained in the follow up of 52 weeks. These observations suggest that rtA194T mutation emerges under LAM monotherapy and remains sensitive to TDF.
Keywords: hepatitis B, tenofovir disoproxil fumarate, resistance, rtA194T mutant, case report
Introduction
Chronic Hepatitis B (CHB) is a major problem for global public health. Antiviral treatment improves liver histology and reduces risks of liver-related fibrosis, hepatocellular carcinoma (HCC), and mortality.1 Currently, tenofovir disoproxil fumarate (TDF) is recommended as first-line nucleos(t)ide analogue (NA) treatment in patients with CHB for its high antiviral effects and high genetic barriers to drug resistance.2 Additionally, TDF is effective in patients harboring lamivudine (LAM)-resistant mutations.3 Although TDF-resistance can be found in anti-HIV treatment,4,5 TDF resistance was not detected in CHB patients after long-term TDF treatment.6 The rtA194T Hepatitis B Virus (HBV) polymerase mutation was firstly identified, along with LAM resistance-associated mutations (rtL180M and rtM204V), in two HIV/HBV-coinfected patients treated with long-term TDF and LAM therapy. Meanwhile, phenotypic analyses revealed that constructs harboring rtA194T together with rtL180M and rtM204V displayed a 10-fold reduction in TDF susceptibility.7 In addition, Samad Amini-Bavil-Olyaee demonstrated that clones harboring rtA194T showed partial resistance (a fivefold to sevenfold increase in the EC50) to TDF in vitro, irrespective of additional mutations.8 However, Delaney WE had not found a clear association between rtA194T and viral load by using transfected-HepG2 cell culture.9 It appears that the potential impact of rtA194T mutation on TDF susceptibility remains unclear and therefore deserves further study. Here, we report a case of a CHB patient who developed rtM204V, rtL180M and rtA194T mutations in association with viral breakthrough on LAM monotherapy and was rescued by TDF.
Case Presentation
A 62-year-old man was diagnosed with HBV-related HCC in June 2010 and then received LAM antiviral treatment followed by surgery. At the time of diagnosis, HBV DNA level was almost 10,000 copies/mL by self-reports, the patient was hepatitis B surface antigen (HBsAg) positive, hepatitis B e antigen (HBeAg) negative, anti-HBe positive, and without co-infection by hepatitis C virus (HCV) or human immunodeficiency virus (HIV). Two months later (August 2010), the detectable level of HBV DNA was <1000 copies/mL (Roche Diagnostics, Mannheim, Germany, detection threshold, 1000 copies/mL), HBsAg was 454.12 IU/mL (Roche Diagnostics GmBH, Mannheim, Germany), serum alanine aminotransferase (ALT) was 24 IU/L (normal level: 10–64 IU/L), aspartate aminotransferase (AST) was 24 IU/L (normal level: 8–40 IU/L), total bilirubin (TBil) was 22.3μmol/L (normal level: 4.7–24μmol/L), direct bilirubin was 4.0 μmol/L (normal level: 0–6.8μmol/L), indirect bilirubin (IBil) was 18.3μmol/L, AFP was 13.05 ng/mL (normal level: <8.04 ng/mL). No HBV resistance mutations were detected using direct sequencing of the reverse transcriptase region of HBV polymerase gene. Ultrasonography (US) of liver showed that this patient had fatter liver and gallbladder stone. During follow-up of 8 years, the detectable level of HBV DNA was <500 IU/mL (Shanghai KEHUA Bio-engineering Co., LTD; detection threshold, 500IU/mL), ALT and AST were normal and IBil mildly elevated (35.4μmol/L). In November 2019, the HBV load rebounded to 4920 IU/mL (Roche COBAS TaqMan HBV test, Roche Diagnostics, Mannheim, Germany, detection threshold, 20 IU/mL), HBsAg was 20.40 IU/mL, quantification of anti-HBc (qAnti-HBc) was 3323.12 IU/mL, ALT and AST were normal, IBil was 23.4 μmol/L, estimated glomerular filtration rate (eGFR) was 94.1, complete blood count was normal, AFP was 2.46 ng/mL. Subsequently, TDF was introduced in replacement of LAM. Further genotypic drug resistance testing found the emergence of rtL180M, rtM204V and rtA194T mutations (confirmed by a second sequencing). US showed that this patient had fatter liver and gallbladder stone. Transient elastography (FibroScan) revealed that controlled attenuation parameter (CAP) was 252dB/m and liver stiffness measurement (LSM) was 8.8 kPa. After 1 month (December 2019), HBV DNA was undetectable (Roche COBAS TaqMan HBV test, Roche Diagnostics, Mannheim, Germany, detection threshold, 20 IU/mL) and HBsAg was 18.27 IU/mL, qAnti-HBc was 2801.62 IU/mL. Sequencing of uridine diphosphate glucuronosyl transferase 1A1 (UGT1A1) revealed that the patient was a heterozygous individual with a TA insertion in TATA box of promoter region as A(TA)6/(TA)7TAA. In April 2020, HBV DNA was undetectable (Roche COBAS TaqMan HBV test), HBsAg was 21.37 IU/mL, qAnti-HBc was 1640.44 IU/mL, and ALT was 33 IU/L, AST was 27 IU/L, IBil was 28.7 μmol/L, eGFR was 93.6, complete blood count was normal, AFP was 2.38 ng/mL. In June 2020, HBV DNA was also undetectable (Roche COBAS TaqMan HBV test), HBsAg was 21.30 IU/mL, qAnti-HBc was 1808.99 IU/mL, and ALT and AST were normal, IBil was 45.2 μmol/L. In December 2020, HBV DNA remained undetectable (Roche COBAS TaqMan HBV test), HBsAg was 20.96 IU/mL, and ALT was 24 IU/L, IBil was 38.2 μmol/L. The evolution of viral load and HBV genotypic patterns were presented in Figure 1, and the unified unit of HBV DNA was IU/mL (1 IU/mL=5.6 copies/mL).10
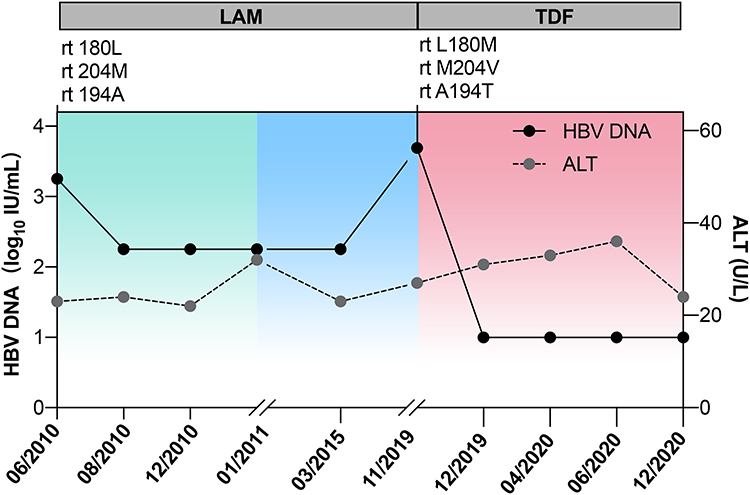 |
Figure 1 Evolution of HBV DNA (log10 IU/mL), ALT levels (IU/mL), HBV genotypic patterns, and antiviral regimen for the patient. Abbreviations: LAM, lamivudine; TDF, tenofovir disoproxil fumarate; rt, reverse transcriptase; L180M, from leucine to methionine at amino-acid 180; M204V, from methionine to valine at amino-acid 204; A194T, from aspartate to tyrosine at amino-acid 194. |
Discussion
Whether the rtA194T mutation conferring resistance against TDF is still controversial and more clinical evidences are needed to reveal the true relevance of the rtA194T mutation. In this case, we report the occurrence of rtA194T mutant during the long-term LAM monotherapy in a CHB patient who remains sensitive to TDF.
Prolonged LAM therapy is associated with the emergence of LAM-resistant mutations, from 24% in 1 year to 70% in 5 years.11,12 Three mutations associated with LAM resistance have been mostly described: rtM204V/I in C domain, rtV173L and rtL180M in B domain.13 In the present case, no drug-resistant HBV variants were detected at the initiation of antiviral treatment in this patient. However, HBV load rebounded to 4920 IU/mL from <500 IU/mL at the ninth years of LAM monotherapy. Subsequently, TDF was introduced as rescue therapy to replace LAM. The HBV load decreased to undetectable level in 1 month and maintained in follow-up of 52 weeks, which suggested that the patient was sensitive to TDF. Interestingly, genotypic drug resistance testing showed that rtA194T mutation was present in this patient, along with rtL180M and rtM204V mutations. It is coincided with an in vitro study that the rtA194T mutation did not confer to TDF as a single mutation or in a LAM-resistant viral background, using a HepG2 cell system.9 But these results do not agree with the previous study that a clear association between rtA194T and viral load rebound reported by Sheldon.7 The discrepancy might be explained by differences among clinical data in patients. HBV rtA194T mutant emerged prior TDF treatment in this case, whereas Sheldon reported that rtA194T mutation occurred under the treatment with TDF for 11.2±6.7 months in two HIV/HBV-coinfected patients. Also, the HIV infection may influence the association between rtA194T mutation and TDF resistance. In addition, only one patient had a transient viral increase and the other one had continuous viral decrease after the occurrence of rtA194T mutant under TDF treatment in his study.
Furthermore, previous studies reported that rtA194T mutant can be observed in treatment-naïve patients.14–16 Nevertheless, HBV DNA could be detected in a patient again at 3 month after TDF treatment, which can be explained by short follow-up and nonoptimal compliance in this study.14 Apart from rtL180M, rtM204V and rtA194T mutations, rtM187V and rtV207L were also detected. RtV207L has been previously reported in LAM-resistance patients,17 but clinical implication needs to be further investigated. Notedly, close virological monitoring is necessary, because CHB patients with HBeAg negative may be at particular risk to rtA194T mutations on account of precore (PC) and basic core promoter (BCP) substitutions enhancing the reduced replicative capacity of rtA194T mutants.8 PC mutations occur frequently among patients infected with genotype D HBV and BCP mutations are more prevalent in genotype A and C.18,19 However, G1896A or A1762T/G1764A mutations were not found in this patient with genotype C HBV by DNA sequencing, while A1727T, C1730G and C1799G mutations were found in BCP region, which were reported to be associated significantly with cirrhosis.20
The patient was diagnosed as Gilbert syndrome based on mild prolonged indirect hyperbilirubinemia and A(TA)7TAA genotype.21 Individuals with Gilbert syndrome may be susceptible to these drugs that require glucuronidation for metabolism, such as menthol, estradiol benzoate, ethinyl estradiol, lamotrigine, tolbutamide, rifamycin SV, acetaminophen, nonsteroidal inflammatory drugs, statins and gemfibrozil,22 human immunodeficiency virus (HIV) protease inhibitors.23 Indinavir and atazanavir (HIV protease inhibitors) can induce hyperbilirubinemia by inhibiting UGT1A1.24 Hyperbilirubinemia associated with the use of nucleoside/nucleotide reverse transcriptase inhibitors is uncommon.25 TDF as one of nucleotide reverse transcriptase inhibitors, to our knowledge, no previous study has shown that TDF has notable toxicity to patient with Gilbert syndrome. And in our study, the TBil level of patient did not increase obviously after receiving TDF treatment. However, both chronic liver disease and Gilbert syndrome may potentiate the hyperbilirubinemia. Therefore, the regular clinical and laboratory follow-up is essential.
In conclusion, our case reported that the emergence of rtA194T mutants within the HBV polymerase after LAM treatment is sensitive to TDF rescue therapy. The potential impact of this mutation on TDF susceptibility deserves to be elucidated by long-term observation of large cohorts.
Ethics and Consent Statement
Written informed consent was obtained from the patient for the publication of this case report and the study was approved by the institutional review board of Ruijin Hospital in accordance with the Declaration of Helsinki.
Acknowledgement
This work was supported by National Key Grant 2017ZX10202202.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ganem D, Prince AM. Hepatitis B virus infection–natural history and clinical consequences. N Engl J Med. 2004;350(11):1118–1129. doi:10.1056/NEJMra031087
2. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560–1599.
3. Fung S, Kwan P, Fabri M, et al. Randomized comparison of tenofovir disoproxil fumarate vs emtricitabine and tenofovir disoproxil fumarate in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology. 2014;146(4):980–988. doi:10.1053/j.gastro.2013.12.028
4. Kabbara WK, Ramadan WH. Emtricitabine/rilpivirine/tenofovir disoproxil fumarate for the treatment of HIV-1 infection in adults. J Infect Public Health. 2015;8(5):409–417. doi:10.1016/j.jiph.2015.04.020
5. Behrens G, Rijnders B, Nelson M, et al. Rilpivirine versus efavirenz with emtricitabine/tenofovir disoproxil fumarate in treatment-naïve HIV-1-infected patients with HIV-1 RNA ≤100,000 copies/mL: week 96 pooled ECHO/THRIVE subanalysis. AIDS Patient Care STDS. 2014;28(4):168–175. doi:10.1089/apc.2013.0310
6. Liu Y, Corsa AC, Buti M, et al. No detectable resistance to tenofovir disoproxil fumarate in HBeAg+ and HBeAg- patients with chronic hepatitis B after 8 years of treatment. J Viral Hepat. 2017;24(1):68–74. doi:10.1111/jvh.12613
7. Sheldon J, Camino N, Rodés B, et al. Selection of hepatitis B virus polymerase mutations in HIV-coinfected patients treated with tenofovir. Antivir Ther (Lond). 2005;10:727–734.
8. Amini-Bavil-Olyaee S, Herbers U, Sheldon J, Luedde T, Trautwein C, Tacke F. The rtA194T polymerase mutation impacts viral replication and susceptibility to tenofovir in hepatitis B e antigen-positive and hepatitis B e antigen-negative hepatitis B virus strains. Hepatology. 2009;49(4):1158–1165. doi:10.1002/hep.22790
9. Delaney WE, Ray AS, Yang H, et al. Intracellular metabolism and in vitro activity of tenofovir against hepatitis B virus. Antimicrob Agents Chemother. 2006;50(7):2471–2477. doi:10.1128/AAC.00138-06
10. Liaw YF, Leung N, Kao JH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2(3):263–283. doi:10.1007/s12072-008-9080-3
11. Liaw YF, Leung NW, Chang TT, et al. Effects of extended lamivudine therapy in Asian patients with chronic hepatitis B. Asia Hepatitis Lamivudine Study Group. Gastroenterology. 2000;119(1):172–180. doi:10.1053/gast.2000.8559
12. Dienstag JL, Goldin RD, Heathcote EJ, et al. Histological outcome during long-term lamivudine therapy. Gastroenterology. 2003;124(1):105–117. doi:10.1053/gast.2003.50013
13. Zoulim F, Locarnini S. Optimal management of chronic hepatitis B patients with treatment failure and antiviral drug resistance. Liver Int. 2013;33(Suppl 1):116–124. doi:10.1111/liv.12069
14. Dupouey J, Gerolami R, Solas C, Colson P. Hepatitis B virus variant with the a194t substitution within reverse transcriptase before and under adefovir and tenofovir therapy. Clin Res Hepatol Gastroenterol. 2012;36(2):e26–e28. doi:10.1016/j.clinre.2012.01.003
15. Dos Santos M, Pacheco SR, Stocker A, et al. Mutations associated with drug resistance and prevalence of vaccine escape mutations in patients with chronic hepatitis B infection. J Med Virol. 2017;89(10):1811–1816. doi:10.1002/jmv.24853
16. Pastor R, Habersetzer F, Fafi-Kremer S, et al. Hepatitis B virus mutations potentially conferring adefovir/tenofovir resistance in treatment-naive patients. World J Gastroenterol. 2009;15(6):753–755. doi:10.3748/wjg.15.753
17. Alvarado-Esquivel C, de la Ascensión Carrera-gracia M, Conde-González CJ, et al. Genotypic resistance to lamivudine among hepatitis B virus isolates in Mexico. J Antimicrob Chemother. 2006;57(2):221–223. doi:10.1093/jac/dki457
18. Chu CJ, Keeffe EB, Han SH, et al. Hepatitis B virus genotypes in the United States: results of a nationwide study. Gastroenterology. 2003;125(2):444–451. doi:10.1016/S0016-5085(03)00895-3
19. Chu CJ, Keeffe EB, Han SH, et al. Prevalence of HBV precore/core promoter variants in the United States. Hepatology. 2003;38(3):619–628. doi:10.1053/jhep.2003.50352
20. Yin J, Xie J, Liu S, et al. Association between the various mutations in viral core promoter region to different stages of hepatitis B, ranging of asymptomatic carrier state to hepatocellular carcinoma. Am J Gastroenterol. 2011;106(1):81–92. doi:10.1038/ajg.2010.399
21. Erlinger S, Arias IM, Dhumeaux D. Inherited disorders of bilirubin transport and conjugation: new insights into molecular mechanisms and consequences. Gastroenterology. 2014;146(7):1625–1638. doi:10.1053/j.gastro.2014.03.047
22. Strassburg CP. Hyperbilirubinemia syndromes (Gilbert-Meulengracht, Crigler-Najjar, Dubin-Johnson, and Rotor syndrome). Best Pract Res Clin Gastroenterol. 2010;24(5):555–571. doi:10.1016/j.bpg.2010.07.007
23. Thoguluva Chandrasekar V, John S. Gilbert Syndrome. StatPearls; 2021.
24. Rotger M, Taffe P, Bleiber G, et al. Gilbert syndrome and the development of antiretroviral therapy-associated hyperbilirubinemia. J Infect Dis. 2005;192(8):1381–1386. doi:10.1086/466531
25. Korenblat KM, Berk PD. Hyperbilirubinemia in the setting of antiviral therapy. Clin Gastroenterol Hepatol. 2005;3(4):303–310. doi:10.1016/S1542-3565(05)00083-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.