")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
The obstacles to diabetes self-management education and support from healthcare professionals’ perspectives: a nationwide survey
Authors Preechasuk L , Sriussadaporn P, Likitmaskul S
Received 25 November 2018
Accepted for publication 8 March 2019
Published 16 May 2019 Volume 2019:12 Pages 717—727
DOI https://doi.org/10.2147/DMSO.S195916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Steven F. Abcouwer
Lukana Preechasuk,1 Pornsri Sriussadaporn,1 Supawadee Likitmaskul1,2
1Siriraj Diabetes Center of Excellence, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Division of Endocrinology and Metabolism, Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Purpose: This study identified the obstacles to diabetes self-management education and support (DSMES) from healthcare professionals’ perspectives in Thailand.
Patients and methods: A cross-sectional survey was conducted at 613 hospitals throughout Thailand from December 2016 to March 2017. A self-completion questionnaire on the characteristics of, and obstacles to, diabetes education was sent to administrators, doctors, and diabetes educators (DEs). The views of DEs at public and private hospitals on the characteristics of diabetes education were compared. The obstructing factors reported by administrators, doctors, and DEs were also analyzed.
Results: The overall response was 76.6%; the response rates of DEs, doctors, and administrators were 85.6%, 58.9%, and 46.5%, respectively. Although the respondents reported that 75% of patients received diabetes education, only 30% of the DEs believed it was successful. An individual-patient education approach was used by 95.1% of public and 81.4% of private hospitals. The median durations of the individual education sessions were 15 (IQR 10, 28) and 30 (IQR 15, 30) minutes for public and private hospitals, respectively. The DE workload at public hospitals was 3 times heavier than at private hospitals (60 [IQR 30, 140] vs 20 [IQR 10, 33] patients per week; p<0.001). Obstacles to diabetes education were a lack of time due to other duties, a lack of skills in assisting patients with behavior change, inadequate DE numbers, patient disinterest in diabetes education, and patient reluctance to change unhealthy behaviors.
Conclusions: High workloads, unclear DE roles, and a lack of DE skills to support patients with behavior change are the primary obstacles to diabetes education.
Keywords: diabetes education, diabetes self-management education, obstacle
Introduction
The 5th Thai National Health Examination Survey reported an increased prevalence of diabetes in people aged ≥15 years, with a rise from 6.9% in 2009 to 8.9% in 2014.1 Data from the Medical Research Network of the Consortium of the Thai Medical Schools (MedResNet) indicated that there was a low level of glycemic control in Thailand, with only 36.3% of patients with type 2 diabetes having an HbA1c below 7% in 2015. Effective diabetes management support from health care providers and appropriate diabetes self-management by patients are fundamental to achieving diabetes goals. Diabetes self-management education (DSME) is the process of facilitating the development of the knowledge, skills, and abilities necessary for diabetes self-care, whereas diabetes self-management support (DSMS) refers to the activities that assist patients with diabetes to implement and sustain the behaviors needed to manage diabetes on an ongoing basis.2 Diabetes self-management education and support (DSMES) improves HbA1c,3 increases diabetes-complication screening,4 improves quality of life,2 and is cost-effective in the long term.5 It has been recommended that all patients with diabetes receive DSMES, and that adequate resources are made available in local communities to support DSMES services.2 In many developed countries, DSMES is usually provided by certified diabetes educators (CDEs);6–8 by contrast, there were no CDEs in Thailand either before or during the present survey. The majority of health professionals providing diabetes education to patients in Thailand attended short-course training in diabetes care for a few days at university hospitals, the Thai Association of Diabetes Educators, or the Diabetes Association of Thailand. Moreover, the costs of DSMES services in Thailand are not reimbursed by either the government or private organizations. All of these factors represent key differences between the approach to diabetes education in Thailand and other countries. Therefore, this study aimed to describe the characteristics of diabetes education and identify the perceptions of Thai health professionals regarding the obstacles to diabetes education.
Materials and methods
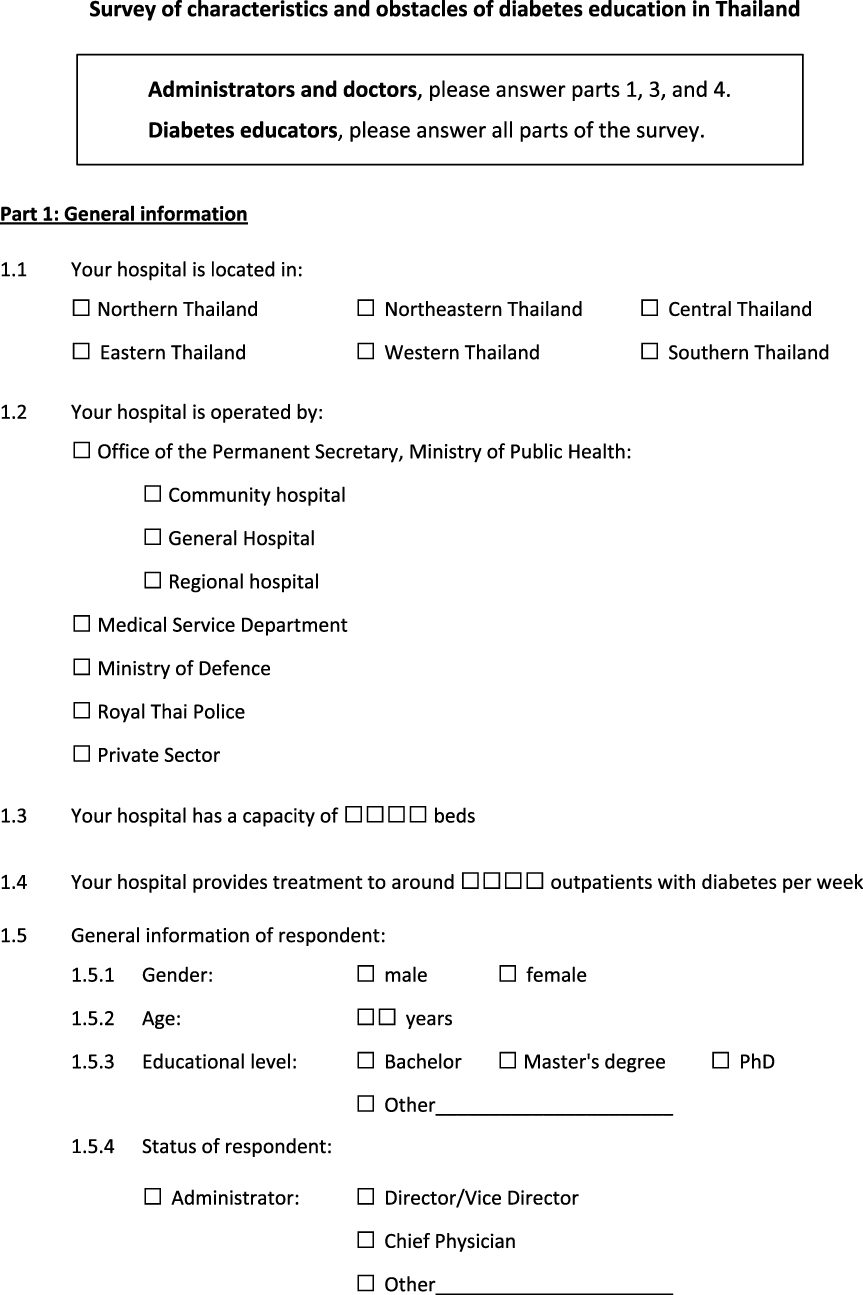
Questionnaire
A self-completion questionnaire (Supplementary 1) was created by an adult endocrinologist, a pediatric endocrinologist, and an experienced nurse working at Siriraj Diabetes Center of Excellence, Faculty of Medicine Siriraj Hospital. It comprised 7 questions on the characteristics of diabetes education, 4 on the workload associated with diabetes education, and a list of commonly perceived obstacles to diabetes education. This study listed the obstacles to diabetes education that had been identified in the national standards for DSMES in the USA9 and by a previous study;10 however, those obstacles were first modified to suit the diabetes education situation in Thailand. The questionnaire was validated by 4 lecturers from the Division of Endocrinology and Metabolism, Department of Medicine and Division of Endocrinology and Metabolism, Department of Pediatrics, Faculty of Medicine Siriraj Hospital, Mahidol University, and 1 lecturer from the Department of Medical Nursing, Faculty of Nursing, Mahidol University. Two of the four validators also worked as administrators, and three were expert in diabetes education for adult and pediatric patients. Using the averaging calculation method, the scale-level content validity index was 0.99.11
Study design and data collection
A cross-sectional survey was conducted at 613 hospitals (508 public and 105 private) across Thailand from December 2016 to March 2017. It was conducted in every region in Thailand (68 in the north, 195 in the northeast, 169 in the central region, 35 in the west, 44 in the east, and 102 in the south) and at different-sized hospitals (277 public and 18 private hospitals with <60 beds; 141 public and 42 private hospitals with 60–119 beds; and 90 public and 45 private hospitals with ≥120 beds). Participant information sheets and self-completion questionnaires were sent to 3 groups: administrators, diabetes clinic doctors, and health professionals responsible for providing diabetes education (this third group is termed “diabetes educators” [DEs] in this paper). The survey collected data from all participants on the perceived obstacles to diabetes education, but data from only the DEs on the characteristics of diabetes education. Introductory letters were also sent to the administrators to inform them of the study’s purpose and to request their permission to conduct it at their institution. Reminder postcards were sent to the 3 groups of health professionals one month after the questionnaire had been sent. The questionnaires were remailed to hospitals that had not replied to the first approach within 3 months.
Sample size calculation and statistical analysis
The sample size was calculated using the Taro Yamane formula;12 it was based on a population size (N) of 1,300 hospitals (the estimated number of hospitals in Thailand) and a margin of error of 0.05. The requisite sample size was calculated to be at least 306 hospitals. However, given that the response rate to mail surveys of medical professionals has been established to be around 50%,13 the information sheets and questionnaires were dispatched to 613 hospitals.
The statistical analyses were performed using IBM SPSS Statistics for Windows, version 18.0 (IBM Corp., Armonk, NY, USA). Continuous data were reported as means (SD) or medians (IQR), and categorical data as numbers or percentages. The continuous data were analyzed using the independent t-test, Mann–Whitney U test, one-way analysis of variance (ANOVA), or Kruskal–Wallis test, as appropriate, and the categorical data were evaluated with the Chi-squared test. A p-value of <0.05 was considered statistically significant.
Human research ethics
The Institutional Review Board of the Faculty of Medicine Siriraj Hospital, approved this study and waived the need for written informed consent, given the questionnaire-based nature of the study.
Results
Response rate
The overall response was 76.6% (470 hospitals). The response from the public hospitals was 81.5% (414 hospitals) and from the private hospitals was 53.3% (56 hospitals). The response rates from <60-bed, 60–120-bed, and ≥120-bed hospitals were 72.2% (213 hospitals), 75.9% (139 hospitals) and 87.4% (118 hospitals), respectively. The response rates of the administrators, doctors, and DEs were 46.5%, 58.9%, and 85.6%, respectively. The primary occupations of the DEs responding to the questionnaire were outpatient department nurse (85.2%), nutritionist (9.6%), health educator (3.1%), inpatient nurse (1.8%), pharmacist (0.2%), and other (0.1%). Sixty-seven percent of the respondents were female, and the mean ± SD age of the respondents was 41±9.9 years. In some hospitals, there was more than one answer from the same group of respondents. The authors analyzed all data from all of the respondents.
DE-reported characteristics of diabetes education in public and private hospitals
The DEs at both the public and private hospitals reported that nearly 75% of patients with diabetes received diabetes education, but that the larger hospitals tended to have a lower percentage of patients receiving diabetes education (Table 1). Diabetes education was provided to patients with newly diagnosed diabetes, uncontrolled diabetes, diabetes complications, and other individual problems. Of the hospital types, the private hospitals tended to have a lower glycemic control threshold for the provision of diabetes education, and they tended to prefer individual to group diabetes education classes. Although the diabetes education sessions provided by the public hospitals were shorter in duration, the public hospitals conducted more sessions per year than the private hospitals. Interestingly, only 30% of the DEs at the public and private hospitals reported that the diabetes education was successful. In contrast, the large majority (nearly 70%) stated that the results of the diabetes education programs were either uncertain or no evaluations were performed. However, because the success of diabetes education was assessed by DEs from each hospital, the assessment process and definitions of diabetes educational outcomes might have differed between respondents.
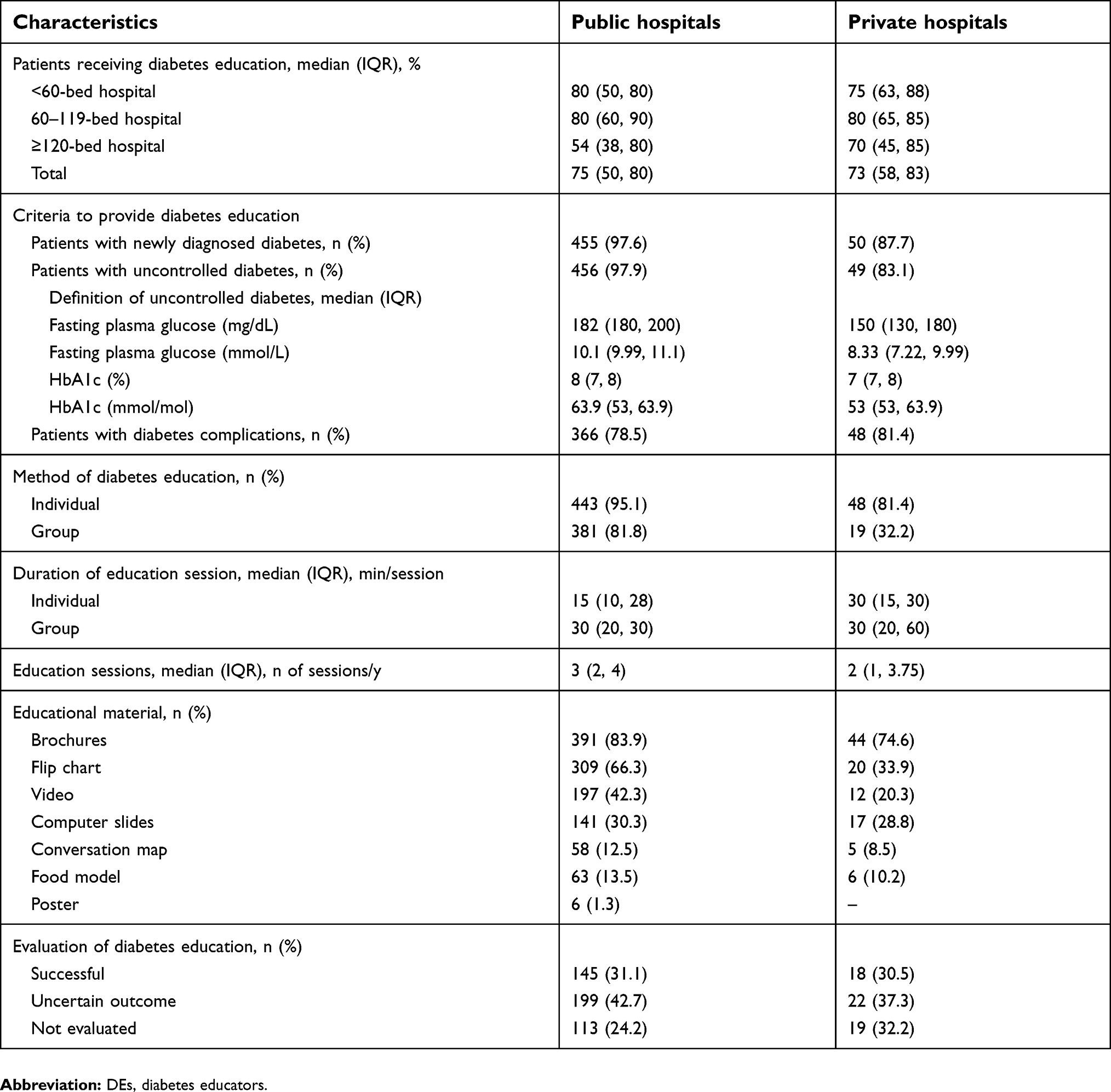 | Table 1 Characteristics of diabetes education programs in public and private hospitals, as reported by DEs |
Workload of diabetes care and diabetes education
Ninety-three percent of the hospitals reported that they had DEs. Their occupations were wide-ranging: outpatient department nurses (at 89.7% of the hospitals), nutritionists (at 61%), pharmacists (at 54.3%), doctors (at 44.4%), inpatient nurses (at 34.1%), physical therapists (at 16.6%), health educators (at 15%), Thai traditional-medicine staff (at 7.2%), and dentists (at 3%). Although the public hospitals reported having more patients with diabetes than private hospitals, the number of DEs did not differ between the types of hospital. The DEs in the public hospitals provided diabetes education to a greater median number of patients per week than the DEs in private hospitals (60 [IQR 30, 140] vs 20 [IQR 10, 33]; p<0.001), as shown in Figure 1. As the response rate of the DEs located at <60-bed private hospitals was very low (n=2), a statistical analysis was not performed for that subgroup.
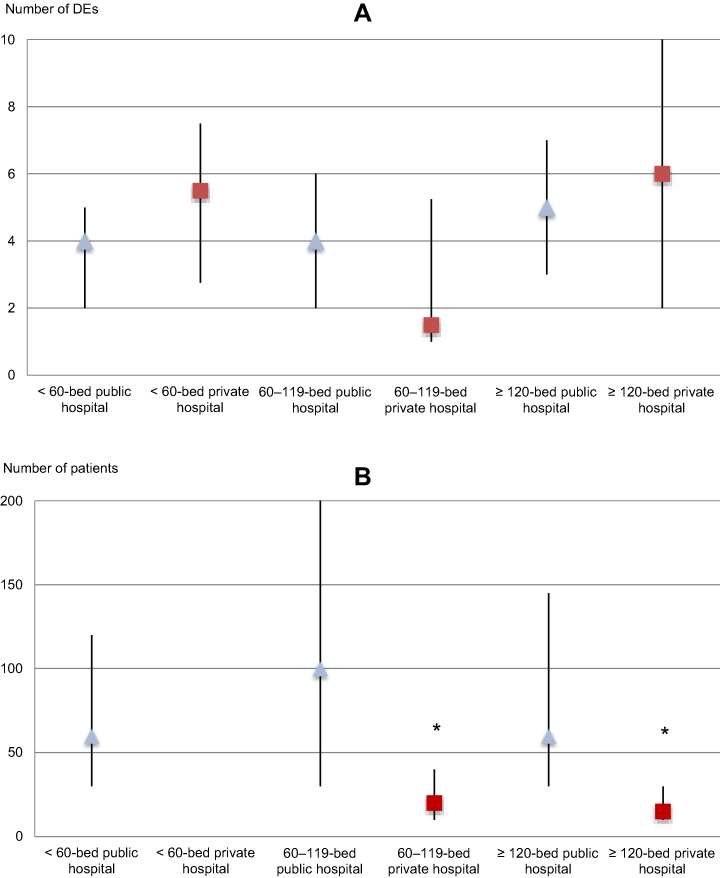 | Figure 1 Number and workload of DEs at different-sized, public and private hospitals, as reported by DEs. (A) median (IQR) number of DEs per hospital; (B) median (IQR) number of patients receiving diabetes education per week per DE, * p-value <0.05, compared between public and private hospitals. Abbreviation: DEs, diabetes educators. |
Self-reported factors perceived as obstacles to diabetes education
The three most commonly perceived obstacles to diabetes education reported by staff at both public and private hospitals were: (1) a reluctance by patients to change their unhealthy behaviors, (2) a lack of time for DEs to deliver diabetes education due to other duties, and (3) patient disinterest in diabetes education. In the case of public hospitals, DEs reported higher percentages for nearly all of the queried obstructing factors than the administrators and doctors (Figure 2). A number of additional problems were reported by DEs at public hospitals, such as a lack of dietitians, communication problems with ethnic minorities, communication problems with older people, and a lack of evaluation after diabetes education programs.
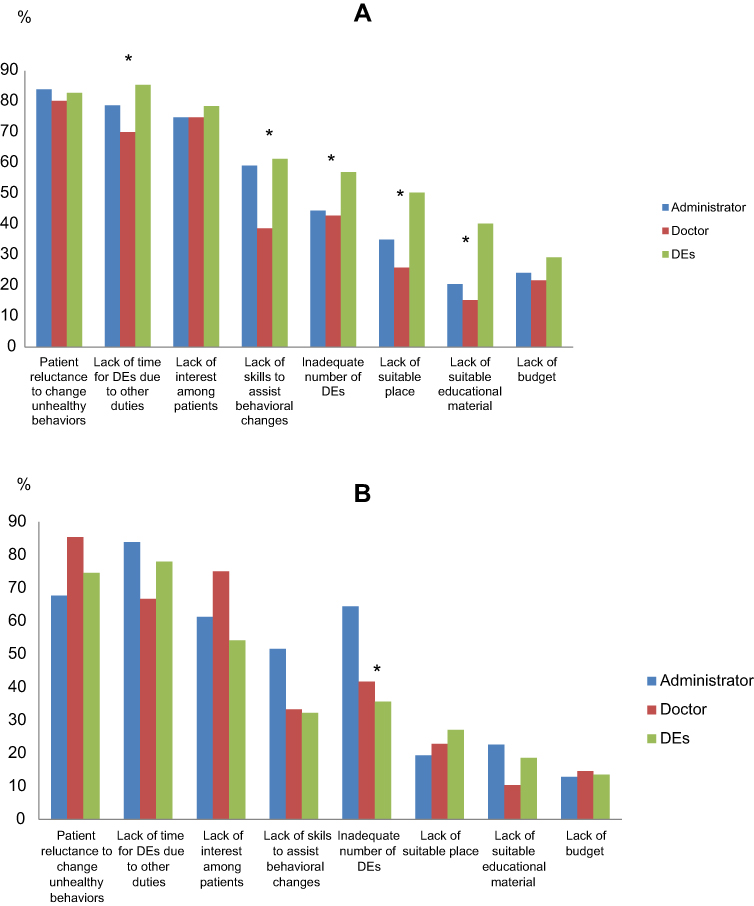 | Figure 2 Perceptions of obstacles to diabetes education, by respondent group. (A) public hospitals; (B) private hospitals. *p-value <0.05, compared between three groups of respondents. Abbreviation: DEs, diabetes educators. |
Demand for diabetes educators
A need for more DEs was reported by 74.3% of the participating public hospitals and 62.3% of the private hospitals. The median number of additional DEs required by the public and private hospitals was 2 (IQR 2, 4) positions per hospital.
Discussion
This is the first nationwide survey of diabetes education in Thailand. The overall response was 76.6%. In total, around 75% of patients were reported to receive diabetes education. This proportion was higher than the corresponding figures that have been presented by other studies. For instance, in a self-report survey from the USA,14 physicians estimated that 37% of their patients received DSME in their service, while data drawn from Medicare and private-insurance reimbursements in the USA indicated that only 5%–6.8% of patients with newly diagnosed diabetes used a diabetes self-management training service.15,16 Unfortunately, there were no data on the number of patients receiving diabetes education through the health care system in Thailand. The major, government-provided, health insurance scheme in Thailand, the Universal Coverage Scheme, records process indicators and outcome indicators related to diabetes care; unfortunately, it only records the percentage of patients receiving foot care education.17 Although our survey reported a high percentage of patients receiving diabetes education, 70% of DEs were uncertain about the educational outcomes. The lack of formal evaluation systems after the conduct of diabetes education programs is one of the diabetes-education weaknesses in Thailand.
Either individual or group approaches to DSMES is effective.3 Individual diabetes education is the approach predominantly utilized by public and private hospitals in Thailand. The public hospitals had a higher proportion of group education programs, a higher glycemic threshold for the provision of DSMES programs, and a shorter duration for individual programs than the private hospitals. The 2017 Diabetes Educator and the DSME National Practice Survey in the USA established that the majority of DEs (55%) saw ≤5 patients with diabetes per day, while 34% of DEs saw 6–10 patients with diabetes daily.18 In contrast, our study demonstrated that public hospital DEs in Thailand saw a median of 60 (IQR 30, 140) patients with diabetes weekly. Assuming that Thai public hospital DEs work a 5-day week, 22% of them advised ≤5 patients per day, 24.6% advised 6–10 patients daily, while 53.5% advised >10 patients each working day. The higher workload of public hospital DEs might be one of the factors related to the low level of glycemic control achievement in Thailand.
Some of the reported perceived obstacles appear to relate to the absence of CDEs in Thailand. Because there is no official CDE training program and no formal position of “diabetes educator” in the Thai health care system, health professionals engaging in the duties of a DE are also obliged to work in their primary disciplines (such as nursing, clinical nutrition, and pharmacology). As a result, the most consequential obstacle to diabetes education that was reported was a lack of time to undertake diabetes education by the DEs due to their need to carry out their primary duties. In addition, DEs require a comprehensive knowledge of diabetes, effective teaching and learning skills, and a sound understanding of various psychosocial and behavior approaches.19 Interestingly, 60% of the public hospital DEs in the present study stated that their perceived lack of skills in assisting patients with behavior changes was an obstacle to diabetes education. Although the sustainability of behavior changes depends on many factors (such as self-efficacy, family support, social policy, and hierarchy of needs), developing behavior change skills is one of the strategies that can be employed by DEs to facilitate diabetes self-care by patients. Therefore, formally establishing the position of DE in the health care system, promoting DE as a career choice, and creating specific DE programs for health professionals may remove the identified obstacles.
Furthermore, healthcare professionals perceived some obstacles from patients in that they were often unwilling to change their unhealthy behaviors and/or showed a lack of interest in diabetes education. However, this study did not survey patients with diabetes. Therefore, we do not know whether the patients were really not interested in diabetes education or whether they had other reasons for not following the advice of the DEs. In a previous study, the reasons cited by people with diabetes for not attending DSME programs were an aversion to group classes, a lack of interest, transportation difficulties, and an inconvenient schedule.10 Furthermore, the current study demonstrated that administrators and doctors tended to report a lower percentage of obstacles than DEs. Because administrators and doctors have a major role in determining hospital policies, an underestimation of the obstacles to diabetes education might result in less support by way of human, financial and facility resources.
This study has some limitations. Firstly, it did not specify the type of diabetes. However, because the prevalence of type 1 diabetes in Thailand is very low, the authors believe that the results represent the characteristics and obstacles of diabetes education for patients with type 2 diabetes.20 In addition, while the study included the common obstacles to diabetes education listed in the literature, it did not specifically cover all existing obstacles in the Thai health care system (such as communication problems with ethnic minorities). Finally, the results of the current study were only based on the responses of health care professionals. In other words, the obstacles to diabetes education from the perspective of patients were not identified.
Conclusions
Both individual and group approaches to education are used in Thailand. Despite the reported percentage of patients receiving diabetes education being high, the large majority of DEs thought the programs were ineffective. For healthcare professionals undertaking the defined roles of DEs, the chief obstacles to diabetes education were reported to be high workloads, unclear roles, and a lack of skills to assist patients to achieve behavior change. Lastly, a compounding factor is that hospital administrators and doctors often perceived a lower prevalence of obstacles than the nominal DEs, which may give rise to negative resource implications.
Acknowledgments
This study was supported by Siriraj Research Development Fund (Managed by Routine to Research: R2R). The authors give special thanks to Clinical Adjunct Professor Anne Belton for advice on the manuscript preparation, and thanks to Nujeejan Bunyapattanapong, Varisara Boonyuang, Bandit Pidokrath, and the Siriraj Diabetes Center staff for the data collection and administrative work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aekplakorn W. The 5th Thai national health examination survey 2014. Nonthaburi Health systems research institute; 2014.
2. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: a joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Diabetes Care. 2015;38(7):1372–1382. doi:10.2337/dc14-1100
3. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: A systematic review of the effect on glycemic control. Patient Educ Couns. 2016;99(6):926–943. doi:10.1016/j.pec.2016.07.004
4. Kent D, D’Eramo Melkus G, Stuart PM, et al. Reducing the risks of diabetes complications through diabetes self-management education and support. Popul Health Manag. 2013;16(2):74–81. doi:10.1089/pop.2012.0020
5. Lian JX, McGhee SM, Chau J, Wong CKH, Lam CLK, Wong WCW. Systematic review on the cost-effectiveness of self-management education programme for type 2 diabetes mellitus. Diabetes Res Clin Pract. 2017;127:21–34. doi:10.1016/j.diabres.2017.02.021
6.
7.
8.
9. Haas L, Maryniuk M, Beck J, et al. National standards for diabetes self-management education and support. Diabetes Care. 2014;37(Suppl 1):S144–S153. doi:10.2337/dc14-S144
10.
11. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/(ISSN)1098-240X
12. Yamane T. Statistics, an Introductory Analysis.
13. Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol. 1997;50(10):1129–1136. doi:10.1016/S0895-4356(97)00126-1
14. Peyrot M, Rubin RR, Funnell MM, Siminerio LM. Access to diabetes self-management education: results of national surveys of patients, educators, and physicians. Diabetes Educ. 2009;35(2):
15. Strawbridge LM, Lloyd JT, Meadow A, Riley GF, Howell BL. Use of medicare’s diabetes self-management training benefit. Health Educ Behav. 2015;42(4):530–538. doi:10.1177/1090198114566271
16. Li R, Shrestha SS, Lipman R, Burrows NR, Kolb LE, Rutledge S. Diabetes self-management education and training among privately insured persons with newly diagnosed diabetes—United States, 2011–2012. MMWR Morb Mortal Wkly Rep. 2014;63(46):1045–1049.
17.
18. Rinker J, Dickinson JK, Litchman ML, et al. The 2017 diabetes educator and the diabetes self-management education national practice survey. Diabetes Educ. 2018:44(3):1–9.
19.
20.
Supplementary materials
 | Figure S1 (Continued). |
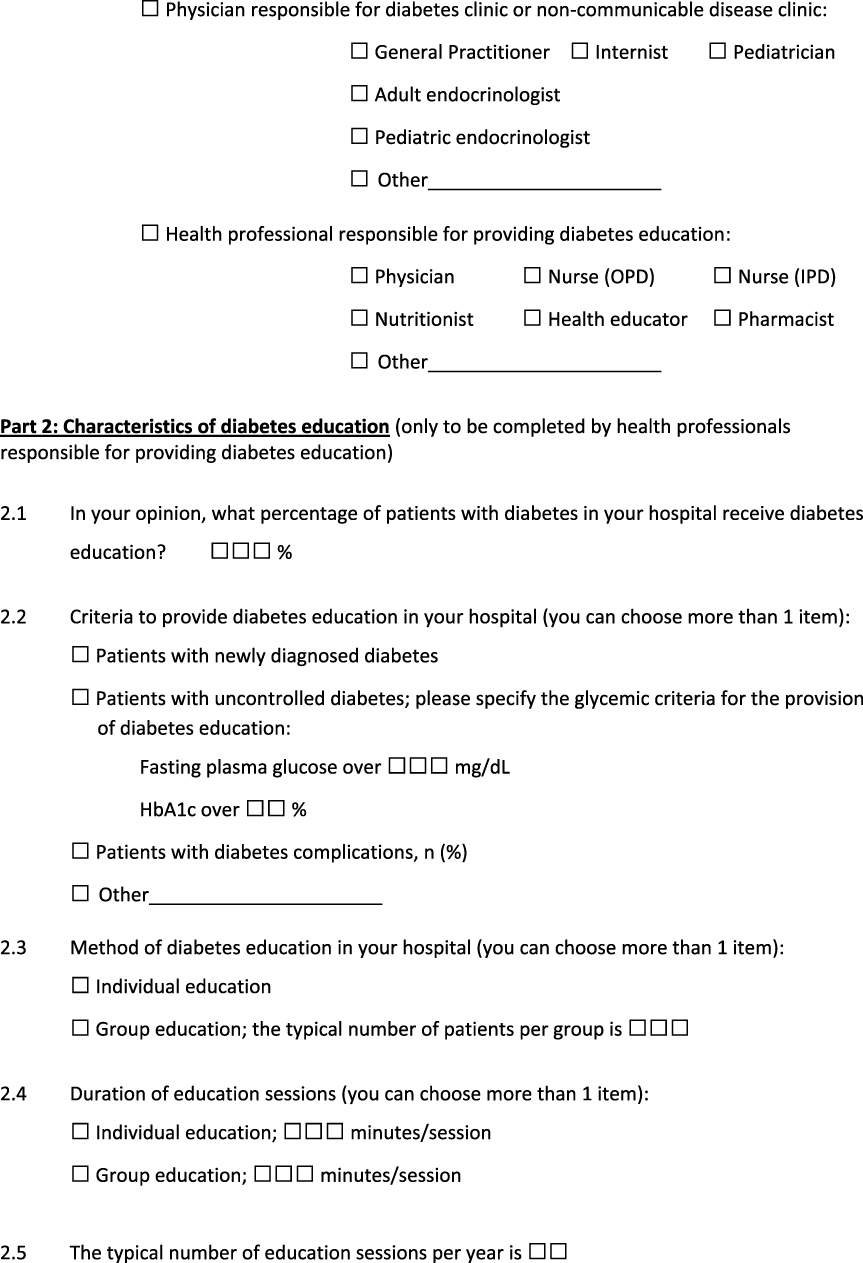 | Figure S1 (Continued). |
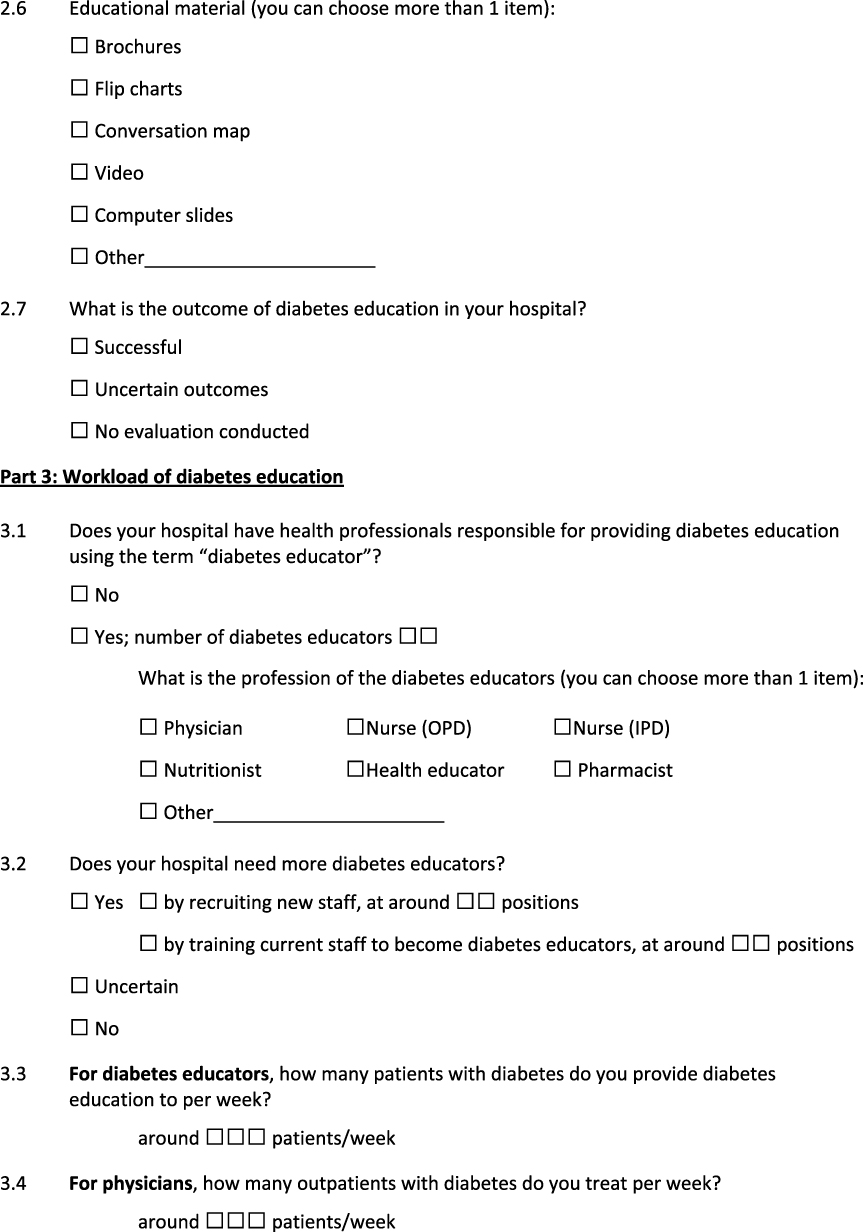 | Figure S1 (Continued). |
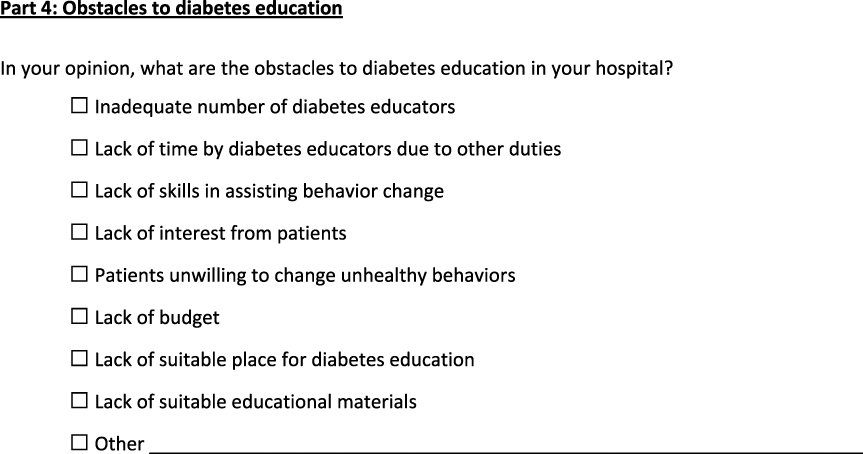 | Figure S1 Survey of characteristics and obstacles of diabetes education in Thailand. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.