")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 11
The noradrenaline metabolite MHPG is a candidate biomarker between the depressive, remission, and manic states in bipolar disorder I: two long-term naturalistic case reports
Authors Kurita M, Nishino S, Numata Y, Okubo Y , Sato T
Received 18 September 2014
Accepted for publication 2 December 2014
Published 11 February 2015 Volume 2015:11 Pages 353—358
DOI https://doi.org/10.2147/NDT.S74550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Masatake Kurita,1–3 Satoshi Nishino,1,2 Yukio Numata,1 Yoshiro Okubo,3 Tadahiro Sato1
1Sato Hospital, Koutokukai, Nanyo, Yamagata, Japan; 2Department of Cellular Signaling, Graduate School of Pharmaceutical Sciences, Tohoku University, Sendai, Miyagi, Japan; 3Department of Psychiatry and Behavioral Science, Graduate School of Medicine, Nippon Medical School, Bunkyo-ku, Tokyo, Japan
Background: Treatment of the depressive and manic states in bipolar disorder I (BDI) is a challenge for psychiatrists. Despite the recognized importance of the switch phenomenon, the precise mechanisms underlying this process are yet to be shown. We conducted a naturalistic study in two BDI patients to determine whether biological markers (monoamine metabolites and brain-derived neurotrophic factor [BDNF]) are associated with the switch between depressive and manic states.
Case presentation and methods: Blood sampling and mood assessments were performed at 2-week intervals over a period of 2 (Case 1, n=72) and 6 (Case 2, n=183) years. Plasma concentrations of 3-methoxy-4-hydroxyphenylglycol (MHPG) and homovanillic acid (HVA) were analyzed by high-performance liquid chromatography with electrochemical detection. Plasma BDNF was assayed by sandwich ELISA (enzyme-linked immunosorbent assay).
Results: MHPG had the highest standardized coefficient (β) in the multiple regression analysis. We found a significant positive correlation between Young Mania Rating Scale scores and plasma MHPG levels (Case 1: р=0.429; Case 2: р=0.488), and a significant negative correlation between Montgomery–Asberg Depression Rating Scale scores and MHPG levels (Case 1: р=-0.542; Case 2: р=-0.465). Conversely, no significant correlation was found between the level of BDNF and the presence of a manic or depressive state, and although HVA had a slightly stronger correlation than MHPG, the levels of neither of these were found to significantly correlate with the symptoms.
Conclusion: These data suggest that peripheral MHPG levels (which is related to noradrenaline levels in the brain) could be used as a biomarker of mood states in BDI. The noradrenaline level in the brain is likely to reflect the clinical characteristics of the switch process in BDI, and has prognostic significance for the treatment of both manic and depressive states.
Keywords: brain-derived neurotrophic factor (BDNF), monoamine, dopamine, homovanilic acid (HVA), depression, pathophysiology, mood disorder
Introduction
Bipolar disorder I (BDI) is an episodic illness characterized by recurrent manic, mixed, and depressive episodes, with an estimated global lifetime prevalence of 1%–5%.1 The illness is associated with high levels of mortality and morbidity2 and functional impairment,3 and high rates of suicide.4 Despite the phenomenon of switching from depression to mania or from mania to depression being a core aspect of the clinical presentation of BDI, the neurobiology of the switching process is still poorly understood. Recently, we reported that 3-methoxy-4-hydroxyphenylglycol (MHPG), more so than homovanillic acid (HVA) or brain-derived neurotrophic factor (BDNF), is a biomarker for the switch from the manic to the remission state in BDI.5 However, the usefulness of MHPG levels as a biomarker for the switch from depression to remission or from depression to mania in BDI is not yet clear. Most antidepressants have been associated with an increased risk for treatment-emergent affective switch. Consequently, antidepressants targeting the serotonergic, noradrenergic, dopaminergic, BDNF, and other systems may affect the switching process in BDI.6 In fact, MHPG and HVA levels are higher in bipolar manic patients than in both bipolar depressed and control patients.7 Furthermore, a meta-analysis showed that BDNF levels are decreased in both bipolar mania and bipolar depression when compared with those in both control groups.8 Thus, the association of BDI with peripheral biomarkers is not uniform. There is currently no biomarker that could serve as an objective index for evaluating the severity or switch progression of BDI. Moreover, the long-term clinical consequences of the switch process are still poorly understood. The main purpose of this study was to determine whether plasma levels of catecholamine metabolites and BDNF are correlated with mood states or severity of manic or depressive symptoms. Our report describes the first long-term, naturalistic, retrospective case study examining MHPG (a noradrenaline metabolite that is associated with noradrenaline levels in the brain), HVA (a dopamine metabolite that is associated with dopamine levels in the brain), and BDNF levels in both the depressed and manic states of BDI.
Patients and methods
The subjects included two Japanese BDI patients admitted to in- or outpatient clinics at Sato Hospital, Koutokukai: a 50-year-old man (Case 1) and a 44-year-old woman (Case 2). The patients received standard psychiatric treatment, mainly mood stabilizers.
Case 1 had 20 incidences of hospitalization and release between X−9 and X+4 years (X is the study start year). His highest level of education is university. He has been divorced twice and went into voluntary bankruptcy because of debts due to excessive spending and gambling while in the manic state.
Case 2 had 14 incidences of hospitalization and release between X−2 and X+5 years (X is the study start year). Her highest level of education is university. She has been divorced once.
The severity of depressive and manic states were assessed every 2 weeks by independent experienced raters. The raters were objective and were not concerned with treatment outcome. The Montgomery–Asberg Depression Rating Scale (MADRS) was used to measure depression, and the Young Mania Rating Scale (YMRS) to measure mania.
Blood was withdrawn by venipuncture from each subject, between 10 am and 5 pm on the assessment day, into a blood collection tube containing EDTA (ethylenediaminetetraacetic acid) as an anticoagulant. The tubes were immediately cooled to 4°C and then centrifuged at 2,000× g for 20 minutes. The plasma was kept frozen at -80°C until assayed.
Plasma MHPG and HVA levels were analyzed by high-performance liquid chromatography with electrochemical detection (HPLC-ECD)9,10 using both the internal standard (5-hydroxyindolecarboxylic acid) method and standard addition methods. Plasma BDNF levels were analyzed by sandwich ELISA (enzyme-linked immunosorbent assay) according to methods described previously.11
Written informed consent was obtained from all patients participating in the study. The study protocols were approved by the Ethics Committee of Sato Hospital, Koutokukai, and the Ethics Committee of Graduate School of Pharmaceutical Sciences, Tohoku University. This study was performed according to the ethical standards of the Declaration of Helsinki.
The Spearman’s rank correlation coefficient (ρ) was calculated to investigate the relationship between the plasma levels of MHPG, HVA, and BDNF and the rating scales of MADRS and YMRS for each individual patient. Standardized coefficient beta (β) was calculated for the factors (biomarkers) that appeared to be linked to the symptoms (MADRS and YMRS), using the multiple regression analysis. Thus, multivariate analysis was applied to the rating scales as the independent variables and the biomarkers as the dependent variables, to determine an influence factor that influences the dependent variable. Data are shown as mean ± standard deviation (mean ± SD). Statistical significance was defined as P<0.05. Effective correlation coefficient was defined as |ρ|>0.25. Normality testing was performed using the Shapiro–Wilk test. Analyses were performed using the SPSS software (IBM, Tokyo, Japan) version 19.0 for Macintosh.
Results
Case 1
A description of the mood states of the patient (determined by rating MADRS and YMRS) throughout the 2 years and 4 months that he participated in the study is shown in Figure 1A. For most of the study period the patient was prescribed mood stabilizers by psychiatrists. For Case 1 a total of 72 data points were obtained, and all data points were analyzed. The mean scores of the YMRS and the MADRS over the study period were 8.3±12.0 and 11.8±15.5 points, respectively. The mean plasma MHPG, HVA, and BDNF levels over the study period were 8.0±2.3 ng/mL, 10.4±4.0 ng/mL, and 6,704±3,164 pg/mL, respectively. We investigated the relationship between the plasma levels of MHPG, HVA, and BDNF and the rating scales of MADRS and YMRS. The homoscedasticity of all variables was rejected by the Shapiro–Wilk test (P<0.05). Therefore, these data were analyzed by a nonparametric test.
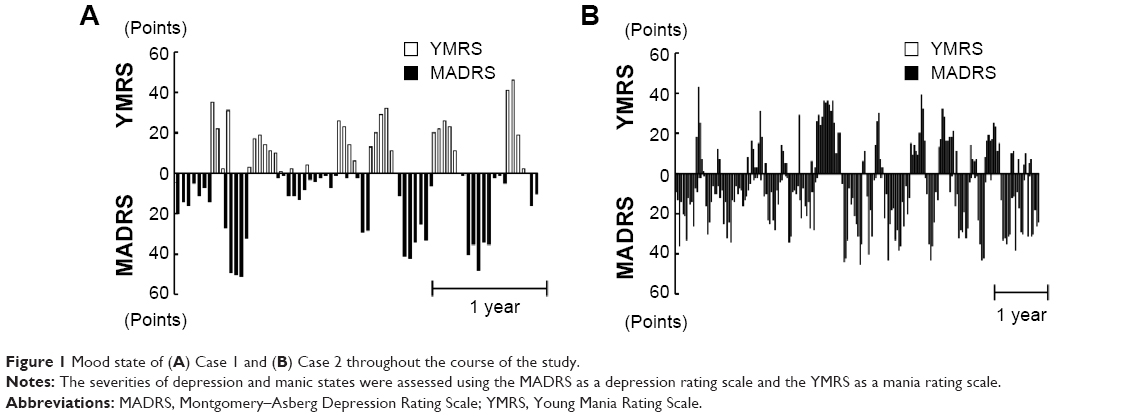 | Figure 1 Mood state of (A) Case 1 and (B) Case 2 throughout the course of the study. |
We found a significant positive correlation between YMRS scores and plasma MHPG levels (ρ=0.429, P<0.001). We also found a significant negative correlation between MADRS scores and plasma MHPG (ρ=-0.542, P<0.001) and HVA (ρ=-0.429, P<0.001) levels (Figure 2A). In contrast, no significant correlation was found between YMRS scores and the plasma HVA level. Furthermore, no significant correlation was found between the plasma BDNF levels and the mood state (both YMRS and MADRS scores). In the multiple regression analysis, the standardized coefficient beta (β) for YMRS was 0.437 (MHPG). The standardized coefficient beta (β) for MADRS was -0.466 (MHPG). In this analysis, other factors were not shown to be significantly different.
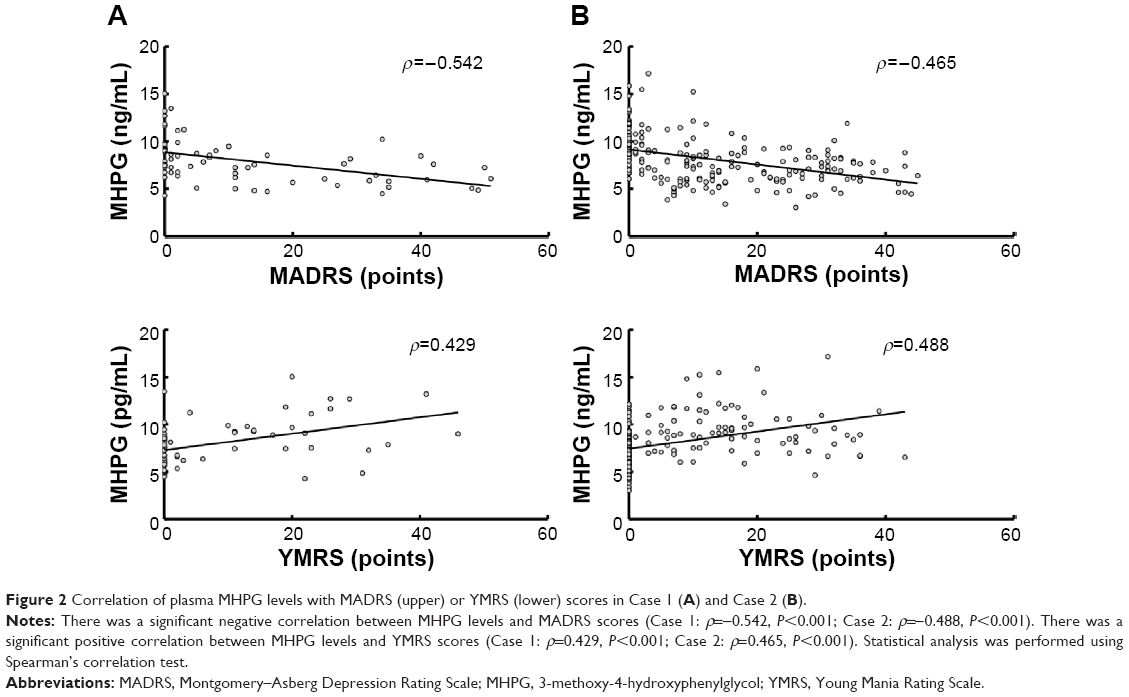 | Figure 2 Correlation of plasma MHPG levels with MADRS (upper) or YMRS (lower) scores in Case 1 (A) and Case 2 (B). |
Case 2
A description of the mood states of the patient (determined by rating MADRS and YMRS) throughout the 5 years and 11 months that she participated in the study is shown in Figure 1B. For most of the study period the patient was prescribed mood stabilizers by psychiatrists. For Case 2 a total of 183 data points were obtained, and all data points were analyzed. The mean scores of the YMRS and the MADRS over the study period were 7.1±10.8 and 12.8±12.9 points, respectively. The mean plasma MHPG, HVA, and BDNF levels over the study period were 8.1±2.7 ng/mL, 11.9±4.0 ng/mL, and 7,781±3,743 pg/mL, respectively. We investigated the relationship between the plasma levels of MHPG, HVA, and BDNF and the rating scales of MADRS and YMRS. The homoscedasticity of all variables was rejected by the Shapiro–Wilk test (P<0.05). Therefore, these data were analyzed by a nonparametric test.
We found a significant positive correlation between YMRS scores and plasma MHPG (ρ=0.488, P<0.001) and HVA (ρ=0.319, P<0.001) levels. We also found a significant negative correlation between MADRS scores and plasma MHPG (ρ=-0.465, P<0.001) and HVA (ρ=-0.381, P<0.001) levels (Figure 2A). In contrast, no significant correlation was found between the plasma BDNF level and the mood state (both YMRS and MADRS scores). The standardized coefficient beta (β) for YMRS was 0.266 (MHPG), 0.235 (BDNF), and 0.233 (HVA). The standardized coefficient beta (β) for MADRS was -0.292 (MHPG), -0.270 (HVA), and -0.136 (BDNF).
Discussion
Antipsychotics have good efficacy in controlling manic symptoms in BDI patients.12 However, these can induce depression or extrapyramidal symptoms in bipolar manic patients.13–15 Hence, antipsychotics are a temporary treatment in severe manic cases, and clinicians know that there is an increased risk of depression or extrapyramidal symptoms if high doses of antipsychotics are continued to be prescribed. Conversely, although antidepressants have good efficacy in controlling depressive symptoms in BDI,16 most antidepressants have been associated with increased risk for treatment-emergent mania/hypomania.17 A study by Altshuler et al has detected an increased likelihood of switching in BDI patients treated with antidepressants.18 For these reasons, antidepressant monotherapy is not recommended for patients with bipolar depression.19
Many reports suggest that regulating monoaminergic transmission or the BDNF system might increase individual susceptibility for BDI switching. However, the association between BDI and peripheral biomarkers is not uniform and clear.
This is the first report in which two cases of BDI have been continuously evaluated for plasma MHPG, HVA, and BDNF levels in a long-term retrospective study. Plasma MHPG and HVA levels showed a weak correlation with symptoms of BDI switching. These results are supported by previous findings that the switch to mania is associated with increased functional brain noradrenaline and dopamine.6,20 Interestingly, in both cases, we found a significant positive correlation between YMRS scores and plasma MHPG levels, and a significant negative correlation between MADRS scores and plasma MHPG levels (more so than for HVA or BDNF). That is, plasma MHPG acted as a peripheral biomarker, consistently indicating the switch of symptoms from manic to depressive state in both BDI cases. MHPG is the major noradrenaline metabolite in the brain.21 Although HVA was significantly correlated with YMRS score in Case 2, no significant correlation was found between YMRS score and HVA levels in Case 1. Multiple regression analysis also showed that MHPG level was the most effective predictor of mood state in both cases. The results of the present study suggest that changes in the noradrenergic system are more likely to induce switching in BDI than are changes in the dopaminergic and BDNF systems.
Given the role of noradrenaline in treatment-emergent affective switch, we suggest that noradrenaline reuptake changes and dysfunction of noradrenaline autoreceptors may be involved in switching in BDI. Some antidepressants are noradrenaline reuptake inhibitors, which inhibit the action of the noradrenaline transporter.
Manic states may involve enhanced presynaptic noradrenaline release or suppressed presynaptic noradrenaline reuptake. Conversely, depressive states may involve diminished presynaptic noradrenaline release or increased presynaptic noradrenaline reuptake. Interestingly, two naturalistic studies found a significantly lower rate of treatment-emergent affective switch when patients were treated with selective serotonin reuptake inhibitors, compared with tricyclic antidepressants.22,23
The levels of biomarkers were markedly different from individual to individual.5 Therefore, it is important that the biomarker level of an individual patient is known, because it may change over time. Also, the difference in correction coefficient between Cases 1 and 2 may be due to the difference in effect size. More large-scale design follow-up studies are needed to understand the pathologic state for the treatment of BDI.
Conclusion
In summary, the results show that plasma levels of MHPG may reflect the pathophysiology of BDI from manic to depressive states better than do the plasma HVA or BDNF levels. These data suggest that peripheral MHPG (which is associated with noradrenaline levels in the brain) could be used as a biomarker of both the manic and depressive states for BDI. The MHPG level is likely to reflect the clinical characteristics of the switch process in BDI, and has prognostic significance for the treatment of manic and depressive states.
Trial registration
This study is registered in the UMIN Clinical Trials Registry (UMIN-CTR): Analysis of genome and blood components for elucidation and treatment of mood disorders (https://upload.umin.ac.jp/cgi-open-bin/ctr/ctr.cgi?function=brows&action=brows&recptno=R000007415&type=summary&language=E; UMIN000006264).
Acknowledgments
We thank the study participants, without whom this study would not have been accomplished, as well as the following psychiatrists of Sato Hospital and Wakamiya Hospital, Koutokukai, for their participation in this study: Kazuo Kenmi, MD, PhD; Asao Hasegawa, MD; Masaaki Mitomo, MD; Tomotaka Suzuki, MD; Yukihiro Takeuchi, MD, PhD; Hiroshi Yamamoto, MD; Maiko Kato, MD; Kenji Takeyoshi, MD; and Kohei Koizumi, MD.
Disclosure
This study was supported by funding from Sato Hospital, Koutokukai. The study did not receive funding from any pharmaceutical corporations. The authors declare no biomedical financial interests or potential conflicts of interest. The authors report no other conflicts of interest in this work.
References
Kastrup MC, Ramos AB. Global mental health. Dan Med Bull. 2007;54(1):42–43. | ||
Rush AJ. Toward an understanding of bipolar disorder and its origin. J Clin Psychiatry. 2003;64(Suppl 6):4–8. Discussion 28. | ||
Rosa AR, Franco C, Martinez-Aran A, et al. Functional impairment in patients with remitted bipolar disorder. Psychother Psychosom. 2008;77(6):390–392. | ||
American Psychiatric Association. Practice guideline for the treatment of patients with bipolar disorder (revision). Am J Psychiatry. 2002;159(Suppl 4):1–50. | ||
Kurita M, Nishino S, Numata Y, et al. The noradrenaline metabolite MHPG is a candidate biomarker from the manic to the remission state in bipolar disorder I: a clinical naturalistic study. PLoS One. 2014;9(6):e100634. | ||
Salvadore G, Quiroz JA, Machado-Vieira R, et al. The neurobiology of the switch process in bipolar disorder: a review. J Clin Psychiatry. 2010;71(11):1488–1501. | ||
Yoshimura R, Nakano Y, Hori H, et al. Effect of risperidone on plasma catecholamine metabolites and brain-derived neurotrophic factor in patients with bipolar disorders. Hum Psychopharmacol. 2006;21(7):433–438. | ||
Fernandes BS, Gama CS, Cereser KM, et al. Brain-derived neurotrophic factor as a state-marker of mood episodes in bipolar disorders: a systematic review and meta-regression analysis. J Psychiatr Res. 2011;45(8):995–1004. | ||
Yeung PK, Buckley SJ, Pedder SC, et al. Determination of 3,4-dihydroxyphenylacetic acid and 5-hydroxyindoleacetic acid in human plasma by a simple and rapid high-performance liquid chromatography assay. J Pharm Sci. 1996;85(4):451–453. | ||
Yoshimura R, Nakamura J, Shinkai K, et al. An open study of risperidone liquid in the acute phase of schizophrenia. Hum Psychopharmacol. 2005;20(4):243–248. | ||
Kurita M, Nishino S, Kato M, et al. Plasma brain-derived neurotrophic factor levels predict the clinical outcome of depression treatment in a naturalistic study. PLoS One. 2012;7(6):e39212. | ||
Yildiz A, Vieta E, Leucht S, et al. Efficacy of antimanic treatments: meta-analysis of randomized, controlled trials. Neuropsychopharmacology. 2011;36(2):375–389. | ||
Tohen M, Sanger TM, McElroy SL, et al. Olanzapine versus placebo in the treatment of acute mania. Olanzapine HGEH Study Group. Am J Psychiatry. 1999;156(5):702–709. | ||
Kukopulos A, Reginaldi D, Laddomada P, et al. Course of the manic-depressive cycle and changes caused by treatment. Pharmakopsychiatr Neuropsychopharmakol. 1980;13(4):156–167. | ||
White E, Cheung P, Silverstone T. Depot antipsychotics in bipolar affective disorder. Int Clin Psychopharmacol. 1993;8(2):119–122. | ||
Gijsman HJ, Geddes JR, Rendell JM, et al. Antidepressants for bipolar depression: a systematic review of randomized, controlled trials. Am J Psychiatry. 2004;161(9):1537–1547. | ||
Truman CJ, Goldberg JF, Ghaemi SN, et al. Self-reported history of manic/hypomanic switch associated with antidepressant use: data from the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD). J Clin Psychiatry. 2007;68(10):1472–1479. | ||
Altshuler LL, Suppes T, Black DO, et al. Lower switch rate in depressed patients with bipolar II than bipolar I disorder treated adjunctively with second-generation antidepressants. Am J Psychiatry. 2006;163(2):313–315. | ||
Yatham LN, Kennedy SH, Schaffer A, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) collaborative update of CANMAT guidelines for the management of patients with bipolar disorder: update 2009. Bipolar Disord. 2009;11(3):225–255. | ||
Murphy DL, Brodie HK, Goodwin FK, et al. Regular induction of hypomania by L-dopa in “bipolar” manic-depressive patients. Nature. 1971;229(5280):135–136. | ||
Schanberg SM, Breese GR, Schildkraut KK, et al. 3-methoxy-4-hydroxyphenylglycol sulfate in brain and cerebrospinal fluid. Biochem Pharmacol. 1968;17(9):2006–2008. | ||
Boerlin HL, Gitlin MJ, Zoellner LA, et al. Bipolar depression and antidepressant-induced mania: a naturalistic study. J Clin Psychiatry. 1998;59(7):374–379. | ||
Bottlender R, Rudolf D, Strauss A, et al. Mood-stabilisers reduce the risk of developing antidepressant-induced maniform states in acute treatment of bipolar I depressed patients. J Affect Disord. 2001;63(1–3):79–83. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.