")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 8
The multidisciplinary health care team in the management of stenosis in Crohn's disease
Authors Gasparetto M, Angriman I, Guariso G
Received 2 January 2015
Accepted for publication 12 February 2015
Published 31 March 2015 Volume 2015:8 Pages 167—179
DOI https://doi.org/10.2147/JMDH.S38729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Marco Gasparetto
Views: 3044
Marco Gasparetto,1 Imerio Angriman,2 Graziella Guariso1
1Department of Women and Children's Health, Paediatric Gastroenterology Unit, Padua University Hospital, Padova, Italy; 2Department of Surgery, Gastroenterology and Oncology, Padua University, Padova, Italy
Background: Stricture formation is a common complication of Crohn's disease (CD), occurring in approximately one-third of all patients with this condition. Our aim was to summarize the available epidemiology data on strictures in patients with CD, to outline the principal evidence on diagnostic imaging, and to provide an overview of the current knowledge on treatment strategies, including surgical and endoscopic options. Overall, the unifying theme of this narrative review is the multidisciplinary approach in the clinical management of patients with stricturing CD.
Methods: A Medline search was performed, using “Inflammatory Bowel Disease”, “stricture”, “Crohn's Disease”, “Ulcerative Colitis”, “endoscopic balloon dilatation” and “strictureplasty” as keywords. A selection of clinical cohort studies and systematic reviews were reviewed.
Results: Strictures in CD are described as either inflammatory or fibrotic. They can occur de novo, at sites of bowel anastomosis or in the ileal pouch. CD-related strictures generally show a poor response to medical therapies, and surgical bowel resection or surgical strictureplasty are often required. Over the last three decades, the potential role of endoscopic balloon dilatation has grown in importance, and nowadays this technique is a valid option, complementary to surgery.
Conclusion: Patients with stricturing CD require complex clinical management, which benefits from a multidisciplinary approach: gastroenterologists, pediatricians, radiologists, surgeons, specialist nurses, and dieticians are among the health care providers involved in supporting these patients throughout diagnosis, prevention of complications, and treatment.
Keywords: Crohn’s disease, endoscopic balloon dilatation, multidisciplinary team, stricture, strictureplasty
Introduction
Inflammatory bowel disease (IBD) is a chronic inflammatory condition of the gut, which includes conditions such as Crohn’s disease (CD), ulcerative colitis (UC), and IBD-unclassified. Endoscopy and histological examination of the gastrointestinal biopsies represents the gold standard for the diagnosis of IBD. It allows us to assess the extent of IBD, to estimate the success of treatments, to monitor the disease course, and to treat some of its complications.1,2 The Vienna Classification first described three distinct groups of CD behavior: inflammatory, stricturing, and penetrating. An association between disease location and behavior is demonstrated, and stricturing disease mostly involves the terminal ileum and the ileocolonic locations.3
Stricture formation is a common complication of CD, occurring in approximately one-third of all patients with this condition.4 Such complication is the result of chronic inflammation within the intestinal walls and the continuous healing response, which can lead to a progressive narrowing of the lumen and an increased pressure gradient around the stricture.5 CD-related strictures are defined as a persistent luminal narrowing, which can remain clinically silent or manifest with prestenotic dilatation and obstructive symptoms, such as abdominal bloating, distention, and pain.5,6 Strictures in CD are described as either inflammatory or fibrotic. They can occur de novo, at sites of bowel anastomosis or in the ileal pouch.5
Fibrosis is the result of complex interactions among inflammatory mediators including growth factors (ie, transforming growth factor β, insulin-like growth factor, platelet-derived growth factor, and basic fibroblast growth factor) and cytokines (ie, interleukin [IL]-13 and IL-17), which are all involved in driving changes in tissue architecture and function. This can ultimately impact the structure and function of the small intestine and colon and can result in clinical symptoms.7
In the last two decades, the medical therapy for CD has improved remarkably, and the introduction of biologics has dramatically changed the therapeutic approach in both adults and children. However, CD strictures generally show a poor response to medical therapies, and surgical bowel resection or surgical strictureplasty are often required.8,9 Over the last three decades, the role of endoscopic balloon dilation in this clinical setting has increased vastly. Nowadays, it represents a valid complementary option.4
Epidemiology
At the time of diagnosis, intestinal strictures may occur in about 5%–10% of patients with CD.6,7 Up to one-third of the patients will develop intestinal strictures within 10 years of disease activity (mainly at the terminal ileum, ileocolonic, and colonic level).8,9
Though inflammatory strictures have the option of other medical treatments, 60%–70% of these patients will nevertheless require surgery at follow-up.10 Moreover, a high rate of post-surgical relapses is observed: 40% at 4 years after bowel resection, and 50% at 10 –15 years after ileocecal resection. Strictureplasty has also been associated with a risk of stricture relapse in 34% of the cases at 7.5 years. This implies that up to one-third of CD patients will undergo more than one surgery in their life course.11 Patients with early onset of disease have an increased risk of surgical relapse and a need of repeated resections, which may result in a short bowel syndrome.6
Factors that affect stricture formation can be broadly categorized into clinical presentation parameters, serologic markers, and genetic susceptibility.4 Parameters that have been proved to correlate with stricturing CD behavior and worse disease outcome include smoking, lower educational level, and younger age at diagnosis.12 As outlined by the data from the TREAT™ registry (the Crohn’s therapy, resource, evaluation, and assessment tool), other factors that are associated with stricture formation include CD severity at the time of disease onset, CD duration, ileal disease, and use of corticosteroids.11
The role of serologic markers in predicting disease course in IBD is currently not completely defined, though generally perinuclear anti-neutrophil cytoplasmic antibody (pANCA) positivity is thought to correlate with a more benign, “UC-like” clinical presentation, while ASCA antibody (anti-Saccharomyces cerevisiae antibody), OmpC (Escherichia coli outer membrane porin C), Pseudomonas fluorescens-associated sequence I2 (bacterial sequence I2) and Cbir1 (flagellin) correlate with more complicated CD.13
Nucleotide-binding oligomerization domain 2(NOD2)/caspase recruitment domain-containing 15 (CARD15) remains the most established genetic predictor of complicated CD, though it is not currently able to predict which patients should be targeted for more aggressive early intervention.14 The three major polymorphisms reported with CD are Arg702Trp (SNP8), Gly908Arg (SNP12), and Leu1007insC (SNP13), and they have been associated with ileal disease, stenosis, and need for surgery.4,14 Apart from NOD2, other genetic markers for CD confirmed in multiple populations include ATG16L1 (autophagy-related 16-like1 gene) and IL-23R (IL-23 receptor gene).4
Diagnostic techniques: the role of radiologists and endoscopists
Symptomatic CD patients often undergo diagnostic imaging studies for assessment of disease activity or complications including bowel strictures and obstructions.15 It is vital to differentiate between inflammatory versus fibrous-predominant strictures, as the optimal therapy will consequently differ.16
Intestinal ultrasound
Intestinal ultrasound (US) represents a useful option to evaluate aspects including wall thickness, transmural complications, color Doppler grade, quantitative analysis of the contrast enhancement, and the presence and severity of strictures. Ripollés et al investigated the accuracy of several US parameters for evaluation of mural inflammation in CD, referring to the related histopathology findings.16 They report a good correlation between the sonographic and pathology scores, for both inflammatory and fibrostenosing strictures. According to this study, US can be a useful tool for distinguishing inflammatory from fibrostenotic lesions in CD.16
Magnetic resonance enterography and computed tomography
Computed tomography (CT) and magnetic resonance enterography (MRE) are now widely used in patients with CD, both for diagnosis and monitoring.17 These techniques have almost completely replaced traditional barium small bowel follow-through studies.7 MRE provides information regarding disease activity, chronicity, and stricture formation without using ionizing radiation.15 A retrospective study by Ha et al (Table 1) showed that MRE provides an effective alternative to CT for evaluating and directing care in CD patients, particularly those presenting with obstructive symptoms.15 Positive findings of CD including active inflammation, stricturing, and penetrating disease were more frequent in patients with obstructive symptoms, in respect to other indications (P=0.001).15
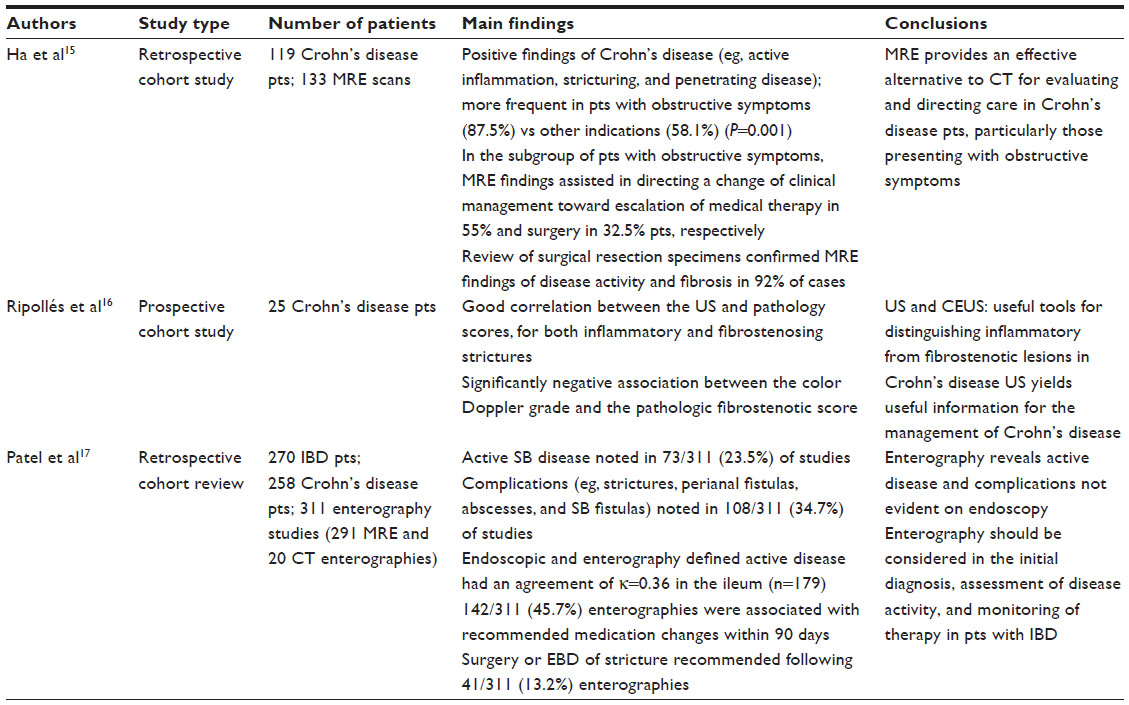 | Table 1 Diagnostic techniques for stenosing Crohn’s disease. Synopsis of main papers cited in this review |
Other supporting data are provided in a retrospective study by Patel et al (Table 1), who sought to assess the use of MRE for management of IBD in a single medical center.17 The authors validated the potential of enterography in revealing active disease and its complications, which are not evident on endoscopy (including strictures, perianal fistulas, and abscesses). They concluded that MRE should be considered in the initial diagnosis, assessment of disease activity, and monitoring of therapy in patients with IBD.17
Small bowel endoscopy
The role of small bowel endoscopy (SBE) for diagnosis and assessment in pediatric patients with suspected or established CD was investigated in a prospective cohort study conducted by Di Nardo et al.18 On the basis of the success rate and of the absence of complications, the authors concluded that SBE is a useful and safe endoscopic procedure for evaluating the small bowel in pediatric patients with CD. In fact, not only does it have the potential to provide a definite diagnosis of CD when this is uncertain, but it is also an effective option in the management of small-bowel strictures, thus allowing clinicians to avoid surgery.18
Medical availabilities: the role of gastroenterologists and pediatricians
While potent anti-inflammatory medications have reduced the symptoms of CD, more than 60% of patients eventually require surgery due to the development of fibrosis.19 Even after the introduction of biologics, the population-based rate of surgery for CD has not decreased. This might be due to late initiation of these therapies, after the fibrosis cascade is unstoppable. To date, no specific intestinal antifibrotic therapy exists.7 Despite the lack of data in literature, azathioprine has been shown to reverse the inflammatory changes at the anastomotic site and to maintain remission in patients with CD.20
The role of biological therapy in case of CD strictures remains controversial.21–24 Because of reports of complete obstruction after treatment with infliximab in patients with or without initial stricture, its use was contraindicated in stenotic forms of CD by some authors.21–24 Theoretically, the rapid tissue healing induced by infliximab administration may result in marked architectural changes in the intestinal wall, which can lead to wall stricturing.25 However, strictures do not occur without inflammation, and chronic inflammation per se may lead to strictures. In fact, a long-term inflammatory process sustained by increased cytokine production results in an excess of fibrotic response. On the other hand, substantial thickening of the mesenchymal layers is observed during mucosal repair. According to the latest evidence, the control of chronic inflammation to prevent fibrosis and stenosis seems more important than the risk of fibrosis induced by treatment, thus justifying infliximab infusions.23,24,26
Govani et al reviewed the evidence that suggests early aggressive therapy is beneficial, especially in patients diagnosed before the age of 40 years, and with ileal or perianal disease. Patients with symptomatic strictures may benefit from early surgery (before penetrating complications) followed by initiation of biologics. With increased early use of biologics and better control of inflammation, a global reduction in intestinal fibrosis and related complications arising from CD should be expected.19
The role of surgeons
CD is usually managed medically, without surgery, while surgery is mostly indicated for complications that do not respond to other medical management. Within 13 years of the disease onset, an estimated 74% of cases require surgery. Also, in the subsequent 10-year follow-up period, the rate of relapse is about 30%–50%.27 Chronic fibrosis and scarring that do not respond to conservative management necessitate surgery, and 25% of patients with CD undergo surgery for intestinal obstruction.27 CD patients with ileocolonic disease do worse with medical therapy (P=0.026) and may require surgery sooner than patients with ileal disease (P=0.023).28 A removal/resection is required in case a longer segment of intestine is involved or when multiple strictures that preclude a simple strictureplasty are present.27 As an alternative to intestinal resection, fibrotic strictures can be treated with strictureplasty.29 Although the latter has the advantage of preserving bowel length, it is still associated with a significant operative recurrence rate of 34% during a median follow-up period of 7.5 years.10
There are 15 distinct strictureplasty methods described, though the two most commonly employed for CD are the Heineke–Mikulicz and the Finney methods. In particular, jejuno–ileal disease offers the widest choice for types of strictureplasty, and generally a Heineke–Mikulicz procedure is used for a shorter disease extent (<5–10 cm), whereas the Finney or Jaboulay procedures are used for longer segment strictures. Modified procedures include Judd, Moskel, Walske, Neumayer, and isoperistaltic strictureplasties.30,31 According to a 2007 meta-analysis that analyzed 1,112 patients with a total of 3,259 strictureplasties, this approach has a complication rate of 4% (including leak, fistula, and abscess) and a recurrence rate of 28% by 5 years (Table 2).32
A colectomy can be required when significant or large segments of the colon are involved. An anastomosis between the ileum and the rectum can be performed when the rectum is free of disease.27 A segmental colectomy represents a possible option when a short segment is involved, and the patient has not presented with a significant number of complications or recurrences.33 A proctocolectomy is needed when the rectum is involved, and an ileostomy is usually performed in conjunction.27 Ileo-anal pouch anastomosis is a surgical procedure done between the ileum and anus after proctocolectomy. This procedure is usually not an option for CD, as the terminal ileum, which is used to form the pouch, is likely to relapse.27
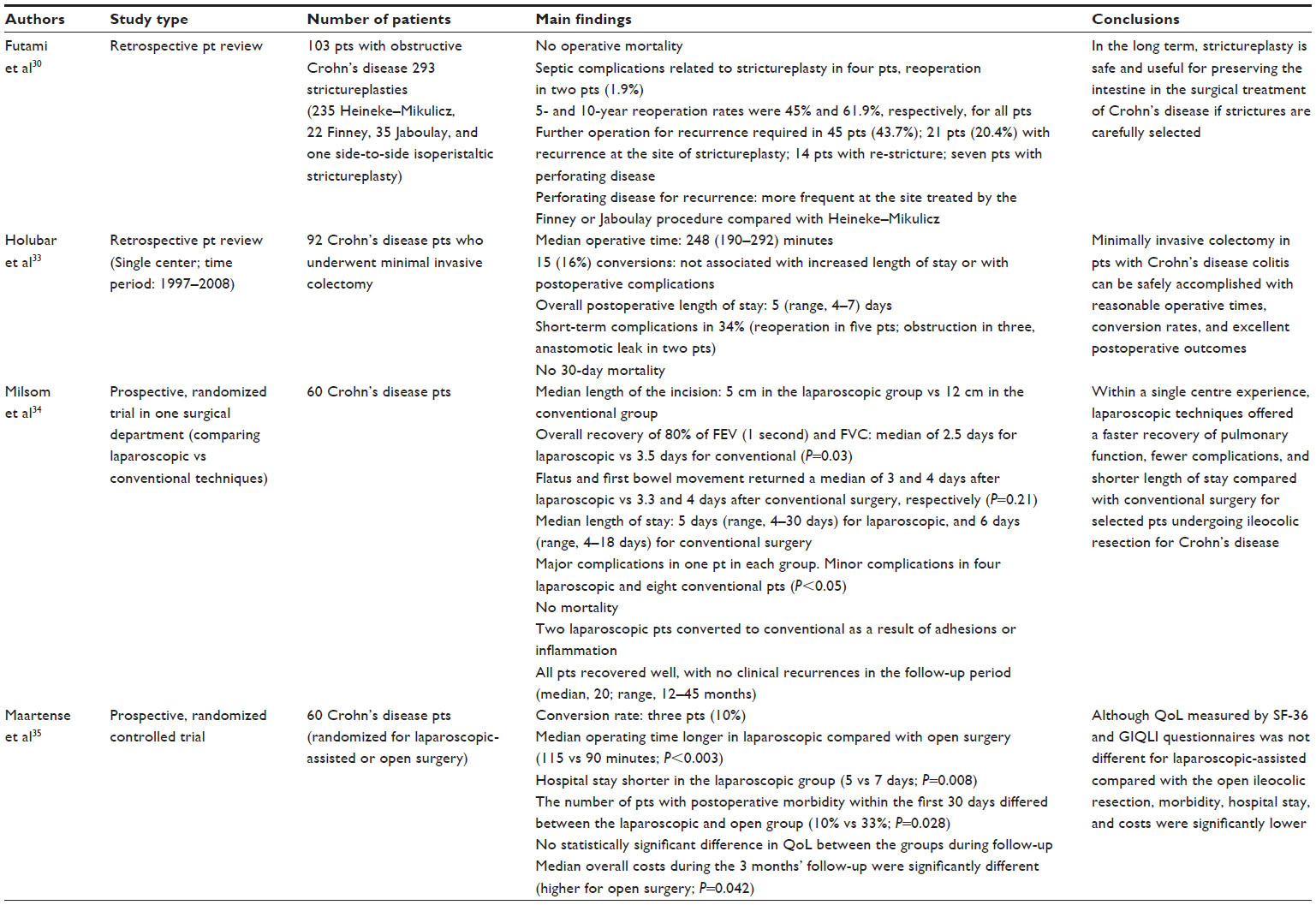 | Table 2 Surgical treatments for stenosing Crohn’s disease. Synopsis of the main papers cited in this review |
The surgical management of CD has advanced considerably over the past two decades. Surgeons are more specialized, and minimally invasive techniques have been introduced from which young patients with CD benefit in particular. Moreover, thanks to improved indications to surgery, such options still represent, at present, a valuable alternative to long-term medical treatments in selected patients. A number of studies have compared short-term outcomes associated with laparoscopic and with open approaches for ileocolic resections in patients with non-penetrating primary CD, though only two of these studies are randomized controlled trials (RCT).19,20 These findings clearly favored the laparoscopic approach over its open counterpart in terms of postoperative morbidity and length of hospital stay, despite the higher costs for the longer operative time. No increase in morbidity or mortality rates was observed.34,35
Although surgical treatment is effective for CD strictures, there is invariably a high risk of recurrence of CD. Medications used in the treatment of CD, such as immunosuppressants, render the patients more prone to complications and post-surgical procedures.27 Symptomatic recurrence is usually seen in approximately 30% of patients at 3 years, with considerably increasing incidence in 10 years. In 20 years, surgery for recurrence is estimated at 70%. Anastomosis sites are the most common locations of recurrence. In the immediate postoperative period, thickening of the loops may be reactive. Obstruction of the bowel due to disease recurrence or the presence of extensive adhesions requires surgical correction.27 Repeated surgery can result in complications related to short bowel syndrome, requirement for total parenteral nutrition, and related complications. Younger patients tend to run an aggressive course with a shorter duration to reoperation.2
The role of operative endoscopy
The advent of endoscopy in the management of complicated CD strictures has changed the approach to the management of anastomotic and small bowel strictures in these patients. Balloon enteroscopy now allows the assessment of areas not deemed possible in the past for dilations.36 Endoscopic balloon dilation (EBD) is a minimally invasive technique that can reduce or delay the need for surgery in patients with CD-related strictures.6,37
There have been several studies aimed at reporting the clinical efficacy, technical feasibility and short and long term results of EBD.6,36,37 Almost all studies have used resolution of symptoms and/or surgery-free period as outcomes. Most studies included had less than 60 patients.36,37
According to current knowledge, EBD in CD strictures appears to be a safe technique (technical success rate of 70%–95%, defined as achieving an endoscopically passable residual stricture) with a low complication rate (0%–10%). Usually, more than one dilatation session is required for every stricture. Complications such as hemorrhages are rare, while perforations are reported mostly in studies in which 25 mm balloons are used. Up to 47% of CD patients show a long-term global benefit, ie, a surgery-free period at 3-year follow-up.38,39 Moreover, with the new generation of double or single endoscopic balloon enteroscopy, this procedure can be performed at almost any level of the gastrointestinal tract, which allows for conserving the bowel length.37,40 The only factor that was proved to significantly affect dilatation efficacy and surgery-free follow-up was the stricture length. In contrast, naïve vs post-surgical, steroid injection, and active vs inactive CD were all deemed to be non-significant.36
Up to now, EBD has been shown to be equally effective in adult and pediatric CD patients. The endoscopic management of CD strictures is of particular importance in children, considering the long life expectancy of these patients together with the major consequences of developing a short bowel syndrome, if repeated surgical resections are performed. Moreover, many clinical concerns are related to malnutrition and subsequent failure to thrive in children with obstructive condition or post-large bowel resections.6,41 EBD could also be taken into consideration as an adjunct to surgery, given that it has been shown to add at least 50% efficacy to the initial surgery by prolonging the surgery-free period.36
It is difficult, at present, to define the relapse risk after EBD, as the published studies are based on very different follow-up periods. According to a prospective long-term study by Stienecker et al, stricture relapses were observed in 46% of patients after a mean of 32 months. Endoscopic re-dilatation was successful in 64% of the patients with relapsing strictures, and the long-term success rate was 80%. On the basis of these long-term results, the authors concluded that EBD, repeated if necessary, is comparable to surgical treatment, whereas the relapse rate after a single balloon dilatation is probably higher than after surgical intervention (Table 2).37
De Angelis et al evaluated short- and long-term efficacy of EBD in a cohort of consecutive patients with symptomatic CD-related strictures (Table 2).6 Both naïve and post-operative strictures of any length or diameter, with or without associated fistula, were included. During the follow-up time, the technical success of EBD was 100%, there were no procedure-related complications, and surgery was avoided in 92.6% of the patients. Two patients, both presenting with ileocecal strictures associated with fistula, failed to respond to treatment and underwent surgical stricture resection. No difference was observed between the EBD success rate for naïve and postoperative CD related strictures (P>0.05). The authors of that study concluded that EBD appears to be a safe and effective procedure in the therapeutic management of CD-related strictures of any origin and dimension in order to prevent surgery.6
A study performed by Chen and Shen showed that the efficacy and safety of EBD in the treatment of strictures is comparable for CD and non-CD related strictures (Table 3).42 Three larger studies have recently been performed to assess the efficacy of EBD for Crohn’s strictures.4,38,43,44 All the studies used a Boston Scientific through the scope balloon, 12–25 mm in diameter, and conscious sedation. Mueller et al (Table 3) investigated 55 patients, mostly with de novo strictures (69%) and reported an initial success rate of 95%.43 Moreover, 76% of patients never required repeat treatment during the follow-up period. They also reported a statistically significant correlation between the need for surgery and stricture length (P=0.006), with average stricture requiring surgery being 7.5 cm vs 2.5 cm for the strictures amenable to endoscopic therapy. One patient was perforated.43
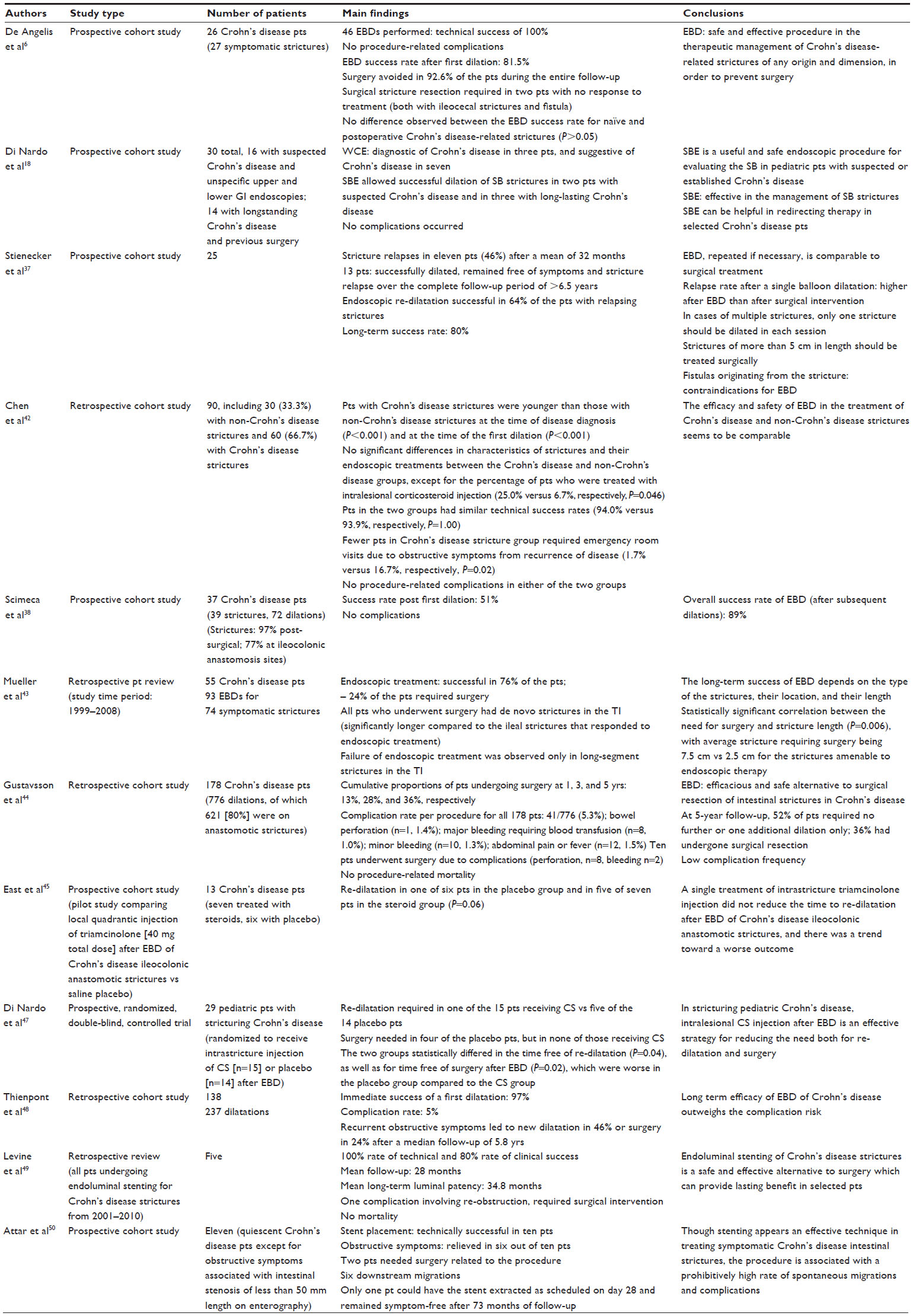 | Table 3 Endoscopic techniques for diagnosis and treatment of stricturing Crohn’s disease, and synopsis of the main studies cited in this review |
Scimeca et al (Table 3) followed 37 CD patients prospectively (39 strictures, 72 dilations) at a single centre. The strictures were mostly post-surgical (97%), with 77% being at ileocolonic anastomosis sites. The success rate post-first dilation was 51%, and the overall success rate (after subsequent dilations) was 89%. No complications were reported.38 The Gustavsson et al retrospective study (Table 3) included a total of 178 patients, most of whom had either ileal or ileocolonic disease, and approximately 40% had stricturing disease at presentation (anastomotic or de novo). At 5 years, 52% of patients had at most one additional dilation, and 36% had a surgical resection.44
Recently, a combined medical and endoscopic therapy has been shown to be effective in the treatment of CD-related strictures. EBD should therefore be considered, together with the medical therapy, as an option to bridge the patient to surgery in better performance conditions (eg, nutrition, inflammatory status), shifting from emergency to elective surgery.6 In cases of multiple strictures, based on their clinical experience, Stienecker et al suggested that only one stricture should be dilated in each session. Strictures of more than 5 cm in length should instead be treated surgically. Fistulas originating from the stricture were considered contraindications for EBD (Table 3).37
The use of intralesional injection of medications in stricturing CD
Given the high rate of stricture recurrence after dilatation, intralesional injection of medications has also been studied.45–47 Nowadays, it is still unknown whether additional medical treatment can influence the recurrence rate.36 Raedler et al treated 30 patients after successful dilatation of ileocecal strictures with azathioprine and budenoside or with placebo. After both 6 and 12 months, the patients in the placebo group presented with a statistically significant greater number of symptoms due to strictures, and needed surgical interventions more frequently.46 A pediatric study of 29 patients also reported a significant trend in patients, who did not receive intralesional steroids, toward re-dilatation and surgery.47
However, another study that investigated single treatment of intrastricture triamcinolone injection did not prove any reduction in the time to re-dilatation after EBD of CD ileocolonic anastomotic strictures (Table 3).45 Moreover, Thienpont et al observed no significant effect of active disease at the time of dilation or systemic medical therapy afterwards, on re-dilation or surgery (Table 3).48 The effect of intralesional injection of infliximab has been studied in a small number of patients and consensus is lacking. Thus, there is no clear evidence at this time to support the role of intralesional injection of medications following dilation.
The use of extractible metallic stents in stricturing CD
The use of extractible metallic stents has also been considered as a possible alternative to EBD, in order to lower the number of recurrences. Levine et al (Table 3) undertook a retrospective review of all patients undergoing endoluminal stenting for CD strictures.49 Five patients underwent this procedure with a 100% rate of technical and an 80% rate of clinical success. There was one complication involving re-obstruction, which required surgical intervention; there were no mortalities. The authors concluded that stenting of CD strictures is a safe and effective alternative to surgery, which can provide lasting benefit in selected patients.49
A prospective pilot study conducted by Attar et al (Table 3) aimed at investigating the feasibility and clinical effectiveness of the use of extractible stents in the treatment of CD intestinal strictures.50 Eleven patients were prospectively included and were treated with transitory stent placement, which was technically successful in ten patients. Obstructive symptoms were relieved in six out of ten patients. Two patients needed surgery related to the procedure, and six downstream migrations were observed.50 The authors concluded that although stenting appears an effective technique in treating symptomatic CD intestinal strictures, the procedure is associated with a prohibitively high rate of spontaneous migrations and complications.50 Other recent studies that have used self-expanding metallic and biodegradable stents, and report a high incidence of migration.2,49,50 Nevertheless, clinical success has ranged from 45%–80%. The majority of stents in these studies were placed in postsurgical strictures.2 Overall, metal stents have been reported as an effective alternative to surgery for the palliation of patients with colorectal neoplastic obstruction.2 However, at present, the role of endoluminal stenting in benign obstruction, especially for CD, is still controversial, with limited data and widely disparate outcomes.49,50
Practical guidelines for the management of strictures in CD
The European Panel on the Appropriateness of CD Therapy (EPACT II)51 have developed appropriateness criteria for the management of CD strictures. Moreover, a flow chart on this topic is also outlined in a recent review by Rieder et al.7 In summary, when clinical symptoms of intestinal obstruction appear in patients with CD, a radiologic assessment of bowel obstruction and an evaluation for active intestinal inflammation are prompted. When intestinal strictures are documented, anti-inflammatory treatments are recommended if signs of active disease are present; if this is not the case, a fibrotic stricture should be presumed, and its location, number, angulation, and diameter of the narrowed tract (> or <4 cm) need to be assessed. Once the diagnostic assessment is completed, options including surgical resection, strictureplasty, or endoscopic dilatation have to be evaluated.7,51
Indications for strictureplasty include: presence of multiple strictures over extensive length of bowel, previous significant small bowel resection (>100 cm), short bowel syndrome, strictures without phlegmon or septic fistula, duodenal strictures, and anastomotic strictures. Contraindications include: associated abscess or phlegmon, perforation with diffuse peritonitis, suspicion of carcinoma in the stricture, or poor nutritional status. Strictureplasty can be performed safely in active disease.7,51
Oncological strictures
Patients with IBD and dysplasia have pathologic characteristics and risks that differ from those of patients with sporadic carcinomas. Therefore, surgical interventions need to be more aggressive in this group of patients than in sporadic cases.52 Only 1%–2% of all general colorectal cancer (CRC) cases per year are diagnosed as CRC arising in IBD. However, as 15% of all IBD deaths are associated with CRC, cancer screening is particularly required in this group. It has to be considered that cancers in patients with UC and CD often present not as mass lesions, but as dysplasia, strictures, or diffuse dysplasia. The risk for CRC development is lower before 8–10 years after symptom onset (3%). The rates of CRC in CD (associated with a 5- to 20-fold increase in risk, in comparison with the general population) seem to mirror those of UC.53,54
Cancer in CD is more likely to be right-sided and associated with ileal and right-sided colonic location.52,54 Colonic strictures are more common in CD (5%–17% of patients) than in UC (5% of patients). Thanks to the medical treatments currently available, which allow more patients to achieve remission, the rate of stricture occurrence seems to be improving nowadays.52,54 Colonic strictures should be considered malignant until proven otherwise.52 A study by Gumaste et al found that 29% of strictures in UC patients were malignant, whereas this malignancy rate was encountered in only 6.8% of CD colorectal strictures.55
Strictureplasty is not indicated as primary management of colonic strictures in IBD. Strictures found at prior anastomotic sites in CD may be carefully dilated to allow endoscopic evaluation of recurrence or surgical complications from the original resection.52,56 Dysplasia and carcinoma at colonic strictures cannot always be detected preoperatively. Ideally, a stricture should be traversed, adequately examined, and biopsied. Nevertheless, a risk of sampling error can still occur.52,56 Oncology resection is indicated any time malignancy cannot be excluded.52,56
While in UC proctocolectomy represents the only option to get to a definitive diagnosis or to rule out a carcinoma and to treat possible multifocal malignancy, in CD colorectal stricture, a segmental oncologic resection may be appropriate in a patient with limited segmental disease.52
In summary, identification and treatment of dysplasia and CRC in IBD is a challenging task for clinicians.52 As sporadic adenomas and inflammatory-related dysplasia in patients with IBD are associated with a different type of risk for the patient, the treatment strategy should therefore be modulated accordingly. Surgical interventions should be based on disease location, finding of dysplasia, and patient morbidities. Although the gold standard for oncologic resection remains total proctocolectomy, many appropriate options exist that are aimed at intestinal continuity.52
Perianal strictures
Perianal CD (PCD) comprises fistulizing lesions (fistulas and abscesses) and non-fistulizing lesions (fissures, ulcers, and strictures). While fistulizing PCD has been thoroughly described and analyzed by guidelines and literature, respectively, data on non-fistulizing PCD remain scarce. Anorectal strictures in CD are either associated with fistulizing PCD or are a long-term consequence of the inflammatory process.57
According to the Cardiff-Hughes classification, strictures are graded on a scale ranging from 0–2 (0= not present, 1= reversible stricture, and 2= irreversible stricture), and location-wise, they are distinguished as anal or lower rectum strictures. Although strictures S1 are mainly inflammatory, and strictures S2 tend to be fibrotic, in most cases both inflammatory and fibrotic compounds occur in association.58
In order to assess the natural history and long-term outcomes of anorectal strictures, Brochard et al57 reviewed all outcomes of patients with non-fistulizing PCD followed in a single unit, as well as subsequent therapeutic management. Out of a total of 102 CD patients, 59% achieved anorectal stricture healing after a median follow-up period of 2.8 years. An unfavorable course (defined as persistent stricture S2, or persistent stoma, or proctectomy at the end of follow-up) was seen in 32% of patients at the end of follow-up, and two patients developed anal adenocarcinoma. A multiple regression analysis showed that female gender, disease duration of CD of less than 10 years, and anal fistula at stricture diagnosis were significantly associated with anorectal stricture healing. Moreover, gender and introduction or optimization of tumor necrosis factor alpha (TNFα) antagonist treatment were associated with a decreased risk of unfavorable course. Conversely, the luminal B2 phenotype at CD diagnosis was the only factor associated with unfavorable course. The authors concluded that anorectal strictures related to severe perianal CD should not be considered as a non-reversible and complicated condition. In fact, in the era of biologics, this study shows a healing rate of anorectal stricture for more than 50% of patients after a 3-year follow-up period. Nevertheless, the need for stoma or proctectomy was required in approximately 25% of patients, which suggests that the presence of anorectal stricture still remains a marker of disease severity.57
Dietary management: the role of dieticians
Given that CD is a debilitating chronic inflammatory condition of the bowel, it is of fundamental importance to promote an appropriate use of diet and nutritional therapy as part of the disease management. The British Dietetic Association has developed evidence-based guidelines on the dietary management of CD in adults, aimed at reducing variation in clinical practice. These guidelines include dietary management of stricturing disease.59 The guidelines state that after a course of enteral nutrition for induction of remission, food re-introduction diets may be useful to help maintain disease remission. Dietary fiber is contraindicated in the presence of strictures because of the risk of mechanical obstruction.59
Conclusion
Stricture formation is a common complication of CD, occurring in approximately one-third of all patients with this condition. CD fibrotic strictures generally show poor response to medical therapies, and surgical bowel resection or surgical strictureplasty are often required.
Endoscopic dilatation represents a valuable treatment of small and large bowel strictures, with an acceptable rate of complications. EBD and surgery should not be seen as mutually exclusive alternatives for treating CD strictures; rather, EBD may be a complementary low-risk procedure that should be considered in both adult and pediatric patients in order to reach a symptom-free condition.
At present, given the complexity in reaching such a condition, the management of patients with stricturing CD requires a multidisciplinary approach. Gastroenterologists, pediatricians, radiologists, surgeons, specialist nurses, and dieticians are among the health care providers involved in supporting these patients throughout diagnosis, prevention of complications, and treatment.
Acknowledgments
The authors would like to acknowledge Megan Roberts for providing writing assistance with this manuscript. The authors would like to thank Alice Ranzato for editing the video abstract of this review.
Disclosure
The authors report no conflicts of interest in this work.
References
Carter D, Eliakim R. Current role of endoscopy in inflammatory bowel disease diagnosis and management. Curr Opin Gastroenterol. 2014;30(4):370–377. | |
Modha K, Navaneethan U. Advanced therapeutic endoscopist and inflammatory bowel disease: dawn of a new role. World J Gastroenterol. 2014;20(13):3485–3494. | |
Gasche C, Scholmerich J, Brjnskov J, et al. A simple classification of Crohn’s disease: report of the Working Party for the World Congresses of Gastroenterology, Vienna 1998. Inflamm Bowel Dis. 2000;6:8–15. | |
Vrabie R, Irwin GL, Friedel D. Endoscopic management of inflammatory bowel disease strictures. World J Gastrointest Endosc. 2012;4(11):500–505. | |
Van Assche G, Geboes K, Rutgeerts P. Medical therapy for Crohn’s disease strictures. Inflamm Bowel Dis. 2004;10:55–60. | |
De Angelis N, Carra MC, Borrelli O, et al. Short- and long-term efficacy of endoscopic balloon dilation in Crohn’s disease strictures. World J Gastroenterol. 2013;19(17):2660–2667. | |
Rieder F, Zimmermann EM, Remzi FH, Sandborn WJ. Crohn’s disease complicated by strictures: a systematic review. Gut. 2013;62: 1072–1084. | |
Travis SP, Stange EF, Lémann M, et al; European Crohn’s and Colitis Organisation. European evidence based consensus on the diagnosis and management of Crohn’s disease: current management. Gut. 2006;55(Suppl 1):i16–i35. | |
Louis E, Collard A, Oger AF, et al. Behaviour of Crohn’s disease according to the Vienna classification: changing pattern over the course of the disease. Gut. 2001;49:777–782. | |
Bernell O, Lapidus A, Hellers G. Risk factors for surgery and postoperative recurrence in Crohn’s disease. Ann Surg. 2000;231:38–45. | |
Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99:956–963. | |
Cosnes J, Bourrier A, Nion-Larmurier I, Sokol H, Beaugerie L, Seksik P. Factors affecting outcomes in Crohn’s disease over 15 years. Gut. 2012;61:1140–1145. | |
Vasiliauskas EA, Kam LY, Karp LC, Gaiennie J, Yang H, Targan SR. Marker antibody expression stratifies Crohn’ s disease into immunologically homogeneous subgroups with distinct clinical characteristics. Gut. 2000;47:487–496. | |
Adler J, Rangwalla SC, Dwamena BA, Higgins PD. The prognostic power of the NOD2 genotype for complicated Crohn’s disease: a meta-analysis. Am J Gastroenterol. 2011;106:699–712. | |
Ha CY, Kumar N, Raptis CA, Narra VR, Ciorba MA. Magnetic resonance enterography: safe and effective imaging for stricturing Crohn’s disease. Dig Dis Sci. 2011;56(10):2906–2913. | |
Ripollés T, Raussell N, Paredes JM, Grau E, Martinez MJ, Vizuete J. Effectiveness of contrast-enhanced ultrasound for characterisation of intestinal inflammation in Crohn’s disease: a comparison with surgical histopathology analysis. J Crohns Colitis. 2013;7(2):120–128. | |
Patel NS, Pola S, Muralimohan R, et al. Outcomes of computed tomography and magnetic resonance enterography in clinical practice of inflammatory bowel disease. Dig Dis Sci. 2014;59(4):838–849. | |
Di Nardo G, Oliva S, Aloi M, et al. Usefulness of single-balloon enteroscopy in pediatric Crohn’s disease. Gastrointest Endosc. 2012;75(1):80–86. | |
Govani SM, Stidham RW, Higgins PD. How early to take arms against a sea of troubles? The case for aggressive early therapy in Crohn’s disease to prevent fibrotic intestinal strictures. J Crohns and Colitis. 2013;7(11):923–927. | |
D’Haens G, Geboes K, Ponette E, Penninckx F, Rutgeerts P. Healing of severe recurrent ileitis with azathioprine therapy in patients with Crohn’s disease. Gastroenterology. 1997;112:1475–1481. | |
Pallotta N, Barberani F, Hassan NA, Guagnozzi D, Vincoli G, Corazziari E. Effect of infliximab on small bowel stenoses in patients with Crohn’s disease. World J Gastroenterol. 2008;14(12):1885–1890. | |
Bouguen G, Trouilloud I, Siproudhis L, et al. Long-term outcome of non-fistulizing (ulcers, stricture) perianal Crohn’s disease in patients treated with infliximab. Aliment Pharmacol Ther. 2009;30(7):749–756. | |
Cosnes J, Nion-Larmurier I, Beaugerie L, Afchain P, Tiret E, Gendre JP. Impact of the increasing use of immunosuppressants in Crohn’s disease on the need for intestinal surgery. Gut. 2005;54:237–241. | |
Vasilopoulos S, Kugathasan S, Saeian K, et al. Intestinal strictures complicating initially successful infliximab treatment for luminal Crohn’s disease. Am J Gastroenterol. 2000;95:2503. | |
Louis E, Boverie J, Dewit O, Baert F, De Vos M, D’Haens G; Belgian IBD Research Group. Treatment of small bowel subocclusive Crohn’s disease with infliximab: an open pilot study. Acta Gastroenterol Belg. 2007;70:15–19. | |
Gasparetto M, Corradin S, Vallortigara F, Cananzi M, Guariso G. Infliximab and pediatric stricturing Crohn’s disease: a possible alternative to surgery? Experience of seven cases. Acta Gastroenterol Belg. 2012;75(1):58–60. | |
Kolar B, Speranza J, Bhatt S, Dogra V. Crohn’s disease: multimodality imaging of surgical indications, operative procedures, and complications. J Clin Imaging Sci. 2011;1:37. | |
Samimi R, Flasar MH, Kavic S, Tracy K, Cross RK. Outcome of medical treatment of stricturing and penetrating Crohn’s disease: a retrospective study. Inflamm Bowel Dis. 2010;16:1187–1194. | |
Romeo E, Jasonni V, Caldaro T, et al. Strictureplasty and intestinal resection: different options in complicated pediatric-onset Crohn disease. J Pediatr Surg. 2012;47(5):944–948. | |
Futami K, Arima S. Role of strictureplasty in surgical treatment of Crohn’s disease. J Gastroenterol. 2005;40(Suppl 16):35–39. | |
Roy P, Kumar D. Strictureplasty. Br J Surg. 2004;91(11):1428–1414. | |
Yamamoto T, Fazio VW, Tekkis PP. Safety and efficacy of strictureplasty for Crohn’s disease: a systematic review and meta-analysis. Dis Colon Rectum. 2007;50:1968–1986. | |
Holubar SD, Dozois EJ, Privitera A, Pemberton JH, Cima RR, Larson DW. Minimally invasive colectomy for Chron’s colitis: a single institution experience. Inflamm Bowel Dis. 2010;16(11):1940–1946. | |
Milsom JW, Hammerhofer KA, Böhm B, Marcello P, Elson P, Fazio VW. Prospective, randomized trial comparing laparoscopic vs conventional surgery for refractory ileocolic Crohn’s disease. Dis Colon Rectum. 2001;44:1–9. | |
Maartense S, Dunker MS, Slors JF, et al. Laparoscopic-assisted versus open ileocolic resection for Chron’s disease: a randomized trial. Ann Surg. 2006;243:143–153. | |
Hassan C, Zullo A, De Francesco V, et al. Systematic review: Endoscopic dilatation in Crohn’s disease. Aliment Pharmacol Ther. 2007;26:1457–1464. | |
Stienecker K, Gleichmann D, Neumayer U, Glaser HJ, Tonus C. Long-term results of endoscopic balloon dilatation of lower gastrointestinal tract strictures in Crohn’s disease: a prospective study. World J Gastroenterol. 2009;15(21):2623–2627. | |
Scimeca D, Mocciaro F, Cottone M, et al. Efficacy and safety of endoscopic balloon dilation of symptomatic intestinal Crohn’s disease strictures. Dig Liver Dis. 2011;43:121–125. | |
Thomas-Gibson S, Brooker JC, Hayward CM, Shah SG, Williams CB, Saunders BP. Colonoscopic balloon dilation of Crohn’s strictures: a review of long-term outcomes. Eur J Gastroenterol Hepatol. 2003;15: 485–488. | |
Couckuyt H, Gevers AM, Coremans G, Hiele M, Rutgeerts P. Efficacy and safety of hydrostatic balloon dilatation of ileocolonic Crohn’s strictures: a prospective longterm analysis. Gut. 1995;36:577–580. | |
Krupnick AS, Morris JB. The long-term results of resection and multiple resections in Crohn’s disease. Semin Gastrointest Dis. 2000;11:41–51. | |
Chen M, Shen B. Comparable short- and long-term outcomes of colonoscopic balloon dilation of Crohn’s Disease and benign non-Crohn’s Disease strictures. Inflamm Bowel Dis. 2014;20(10):1739–1746. | |
Mueller T, Rieder B, Bechtner G, Pfeiffer A. The response of Crohn’s strictures to endoscopic balloon dilation. Aliment Pharmacol Ther. 2010;31:634–639. | |
Gustavsson A, Magnuson A, Blomberg B, Andersson M, Halfvarson J, Tysk C. Endoscopic dilation is an efficacious and safe treatment of intestinal strictures in Crohn’s disease. Aliment Pharmacol Ther. 2012;36:151–158. | |
East JE, Brooker JC, Rutter MD, Saunders BP. A pilot study of intrastricture steroid versus placebo injection after balloon dilatation of Crohn’s strictures. Clin Gastroenterol Hepatol. 2007;5:1065–1069. | |
Raedler A, Peters J, Schreiber S. Treatment with azathioprine and budenoside prevents recurrence of ileocolonic stenosis after endoscopic dilatation in Crohn’s disease. Gastroenterology. 1997;112:A1067. | |
Di Nardo G, Oliva S, Passariello M, et al. Intralesional steroid injection after endoscopic balloon dilation in pediatric Crohn’s disease with stricture: a prospective, randomized, double-blind, controlled trial. Gastrointest Endosc. 2010;72:1201–1208. | |
Thienpont C, D’Hoore A, Vermeire S, et al. Long-term outcome of endoscopic dilatation in patients with Crohn’s disease is not affected by disease activity or medical therapy. Gut. 2010;59:320–324. | |
Levine RA, Wasvary H, Kadro O. Endoprosthetic management of refractory ileocolonic anastomotic strictures after resection for Crohn’s disease: report of nine-year follow-up and review of the literature. Inflamm Bowel Dis. 2012;18(3):506–512. | |
Attar A, Maunoury V, Vahedi K, et al; GETAID. Safety and efficacy of extractible self-expandable metal stents in the treatment of Crohn’s disease intestinal strictures: a prospective pilot study. Inflamm Bowel Dis. 2012;18(10):1849–1854. | |
Felley C, Vader JP, Juillerat P, et al; EPACT II Study Group. Appropriate therapy for fistulizing and fibrostenotic Crohn’s disease: results of a multidisciplinary expert panel–EPACT II. J Crohns Colitis. 2009;3:250–256. | |
Coviello LC, Stein SL. Surgical management of nonpolypoid colorectal lesions and strictures in colonic inflammatory bowel disease. Gastrointest Endosc Clin N Am. 2014;24(3):447–454. | |
Lennard-Jones JE, Melville DM, Morson BC, Ritchie JK, Williams CB. Precancer and cancer in extensive ulcerative colitis: findings among 401 patients over 22 years. Gut. 1990;31:800–806. | |
Choi PM, Zelig MP. Similarity of colorectal cancer in Crohn’s disease and ulcerative colitis: implications for carcinogenesis and prevention. Gut. 1994;35:950–954. | |
Gumaste V, Sachar DB, Grenstein AJ. Benign and malignant colorectal strictures in ulcerative colitis. Gut. 1992;33(7):938–941. | |
Lashner BA, Turner BC, Bostwick DG, Frank PH, Hanauer SB. Dysplasia and cancer complicating strictures in ulcerative colitis. Dig Dis Sci. 1990;35(3):349–352. | |
Brochard C, Siproudhis L, Wallenhorst T, et al. Anorectal stricture in 102 patients with Crohn’s disease: natural history in the era of biologics. Aliment Pharmacol Ther. 2014;40(7):796–803. | |
Hughes LE. Clinical classification of perianal Crohn’s disease. Dis Colon Rectum. 1992;35:928–932. | |
Lee J, Allen R, Ashley S, et al; Gastroenterology Specialist Group of the British Dietetic Association. British Dietetic Association evidence-based guidelines for the dietary management of Crohn’s disease in adults. J Hum Nutr Diet. 2014;27(3):207–218. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.