")
Back to Journals » Psychology Research and Behavior Management » Volume 15
The Management of Sleep Disturbances in Patients with Schizophrenia: A Case Series
Authors Vanek J , Prasko J , Genzor S , Mizera J
Received 20 September 2022
Accepted for publication 28 November 2022
Published 15 December 2022 Volume 2022:15 Pages 3673—3681
DOI https://doi.org/10.2147/PRBM.S388702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Jakub Vanek,1 Jan Prasko,1– 4 Samuel Genzor,5 Jan Mizera5
1Department of Psychiatry, University Hospital Olomouc, Faculty of Medicine, Palacky University in Olomouc, Olomouc, The Czech Republic; 2Department of Psychological Sciences, Faculty of Social Science and Health Care, Constantine the Philosopher University in Nitra, Nitra, The Slovak Republic; 3Department of Psychotherapy, Institute for Postgraduate Training in Health Care, Prague, The Czech Republic; 4Rehabilitation Hospital Beroun, Jessenia Inc, Akeso Holding, Závodí, The Czech Republic; 5Department of Respiratory Medicine, Faculty of Medicine and Dentistry, Palacky University Olomouc and University Hospital Olomouc, Olomouc, The Czech Republic
Correspondence: Jan Prasko, Department of Psychiatry, Faculty of Medicine and Dentistry, University Hospital Olomouc, I. P. Pavlova 6, Olomouc, 77900, The Czech Republic, Email [email protected]
Abstract: Patients with schizophrenia commonly encounter a variety of sleep disorders. Disturbed sleep can be found in 30– 80% of patients, depending on the degree of psychotic symptomatology. Difficulty falling asleep, maintaining, or achieving restful sleep is associated with symptom severity and has been reported as a prodromal symptom of psychotic relapse. Although some sleep disorders improve with antipsychotic treatment, in many cases, even during disease remission, sleep continues to be fragmented, or even different pathophysiological mechanism is causing sleep disruption. Moreover, it may be complicated if the patient needs specific treatment, such as positive airway pressure (PAP) therapy, due to sleep-disordered breathing. The article presents case reports of patients with schizophrenia with sleep disturbances. As presented in our case reports, cognitive behavioral therapy seems effective in treating comorbid insomnia, even in patients with schizophrenia. The second and third case reports emphasise the need for broader clinical considerations, a cross-diagnostic approach, and cooperation in care for patients with severe mental disorders.
Keywords: schizophrenia, sleep, REM sleep, NREM sleep, polysomnography, actigraphy, antipsychotics, hypnotics, cognitive behavioral therapy, symptomatology
Introduction
Disturbed sleep is found in 30–80% of patients with schizophrenia, depending on the degree of psychotic symptomatology.1,2 Patients with psychosis often report difficulty falling asleep or staying asleep, as well as fatigue the next day.3 Sleep disturbances can also appear as a warning sign of an exacerbation of a new episode. Sleep disorders appear during an acute exacerbation of a schizophrenic disorder, but they can persist even in the remission of the disease or belong to the residual symptoms of chronic disease.1 Dissatisfaction with sleep is high in this group of patients.4,5 Although sleep disorders in this group of patients should be a specific therapy target, it is often not even diagnosed. Recent works point out that insomnia can be a trigger or aggravating modulator of delusions and hallucinations and has a significant effect on the deterioration of delusional experience and its emotional impact.6–9 Treatment of insomnia, on the other hand, weakens delusional beliefs.10 A study by Freeman et al (2010) found that in a group of patients with paranoid delusions, 27% suffered clinically severe insomnia, 27% moderate insomnia, 30% mild insomnia, and only 16% slept well.6 At the neurobiological level, the overactivity of dopamine D2 receptors in the striatum appears to be related to positive symptoms of schizophrenia but also increases alertness.11
In studies that used polysomnography (PSG), a reduction in total sleep time, a reduction in slow wave sleep, REM latency and sleep efficiency were found in patients with schizophrenia.2 Moreover, meta-analysis of Chan et al revealed that individuals with longer history of schizophrenia (more than 3 years) have significantly shorter duration of slow wave sleep. Patients without the medication have less abnormities on PSG, but shorter sleep duration and longest sleep-onset latency.12 Similarly, meta-analysis of Biam et al revealed in treatment naïve individuals with schizophrenia reduced total sleep time, lower sleep efficiency, increased REM latency, decreased slow-wave sleep, and increased stage-1 of non-REM.13 Studies using actigraphy have also found that these patients experience changes in circadian rhythms related to sleep disturbances, particularly irregularity and phase advance. Although some sleep disorders improve after antipsychotic treatment, in many cases, especially in remission, sleep remains fragmented, suggesting that the physiological mechanisms of the sleep disorder may remain unchanged by treatment.3 Many sleep parameters, such as the amount of slow-wave sleep and REM latency, are significantly correlated with clinical variables, including disease severity, positive symptoms, negative symptoms, outcome, neurocognitive impairment, and brain structure.2
Palmese et al studied the prevalence of insomnia in schizophrenia and investigated the relationship between sleep, cognitions, quality of life and clinical variables in 175 outpatients with schizophrenia or schizoaffective disorder.14 Participants were assessed for sleep difficulties, sleep patterns, body mass index, a short assessment of cognitive performance, and psychiatric symptoms. In this group, up to 44% of patients met the criteria for clinical insomnia. Another 4% were successfully treated with medication for insomnia. Insomnia was associated with depression and an independent predictor of poor quality of life. It was also associated with a higher frequency of nocturnal overeating, and patients with severe insomnia were significantly more obese. No differences were found in the evaluation of cognitive performance; however, when the group with severe insomnia was evaluated separately, the difference was already present.14 The probable cause of abnormities of sleep and wakefulness in individuals with schizophrenia seems to be impaired function of hypothalamic-pituitary-adrenal axis (glucocorticorticoid secretion rhythm) and disrupted secretion of melatonin.15 This leads to abnormal circadian rhythm regulation and further deteriorates the psychical condition of the patients.16 Moreover, impaired sleep quality is connected also to higher risk of obesity and metabolic syndrome.17 Similarly, Suttajit and Pilakanta in a study of the prevalence of metabolic syndrome in patients with schizophrenia, found that central obesity and metabolic syndrome are often associated with insomnia in these patients, and insomnia is an independent risk factor for metabolic syndrome in addition to depression and psychomotor retardation.18 The increased risk of moderate insomnia in patients with metabolic syndrome may be explained by the fact that this insomnia is often associated with obstructive sleep apnoea.19,20 Interestingly, genetic studies suggest that genotypic differences in insomnia have been found in both schizophrenia and metabolic syndrome.21
Unfortunately, weight gain is the common side effect of antipsychotic therapy. According to Bak et al virtually all antipsychotics increase body weight.22 The adverse effect is more pronounced in treatment-naive patients and usually increases with continuous therapy as obesity is the most significant risk factor of sleep disordered breathing (SDB).22–24 Therefore, it seems logical to expect a higher prevalence of SDB in patients with schizophrenia. However, the data about this problem is limited. Okada et al found clinically relevant obstructive sleep apnoea in 58% of patients with schizophrenia.25 More surprisingly, the presence of objective SDB symptoms were not significantly connected with the diagnosis. The authors assume that polysomnography is needed to confirm the diagnosis, and the indication of the screening method should be considered even in asymptomatic patients.25
Treatment of Sleep Disorders in Patients with Schizophrenia
Antipsychotics are also prescribed for insomnia or sedation in patients who do not suffer from schizophrenia or bipolar disorder. Hermes et al examined the use of second-generation antipsychotics for the treatment of insomnia at the Veterans Affairs Medical Center over 20 months.26 They found that 32.2% of 2613 prescribed antipsychotics were used in a sleep indication, with 12.1% being the only indication. Quetiapine was most often prescribed (47.0% or 73.6%).26 Administration of second-generation antipsychotics in the indication of insomnia did not depend on the diagnosis of schizophrenia or bipolar disorder, nor sociodemographic factors, and was often a newly started treatment.26
Very few consistent studies measure the effects of first-generation antipsychotics on sleep continuity and structure in patients with schizophrenia.1 The situation is better with second-generation antipsychotics. The atypical antipsychotics studied (clozapine, olanzapine, quetiapine, risperidone, ziprasidone, and paliperidone) show a relatively consistent effect on sleep continuity with increases in total sleep time (TST) and sleep efficiency. Individually, they show different effects on other sleep parameters, such as the increase in REM latency observed with olanzapine, quetiapine and ziprasidone and the increase in SWS documented with olanzapine and ziprasidone in healthy subjects.1
Against the background of the conflicting effects of first-generation antipsychotics observed in healthy subjects, it seems possible that highly effective drugs exert their effects on sleep in patients with schizophrenia largely indirectly by suppressing psychotic symptomatology and accompanying stress.1 The effects of second-generation antipsychotics on sleep in healthy subjects and patients with schizophrenia are related to their broader receptor profile and effect on other symptomatology, such as depression, cognitive impairment, etc.1
When dealing with SDB and its most common example, obstructive sleep apnoea, the best conservative treatment remains PAP.27 The therapy is, however, frequently not even considered in patients with schizophrenia. Gilles et al found that this should be changed in their prospective study.28 The psychotic patients had fewer check-ups, but the response to the therapy and adherence level was no different compared with SDB patients without psychiatric comorbidity.28
CBT of Insomnia in Patients with Schizophrenia
CBT is a long time established adjuvant psychotherapeutic treatment in patients with schizophrenia. Myers et al showed in a case series of 15 patients with paranoid delusions who were resistant to previous treatment that CBT treatment eliminated insomnia and reduced the urgency of delusional beliefs.10 Recent studies confirmed its positive impact on persecutory delusions and accompanying worry.29 In another study patients with persistent paranoid delusions and insomnia underwent four sessions of standardised cognitive behavioural therapy for insomnia (CBT-i) under the supervision of psychiatric nurses. Patients were evaluated before treatment, after treatment and at a one-month follow-up. After the intervention, there was a statistically significant reduction in insomnia and paranoid production. The size effect was large, and the changes were maintained even during the monthly catamnesis. Nine patients reduced their insomnia score by at least half, and another five patients by at least 25%. Five patients decreased their persecutory thinking score by at least 50% and eight by at least 25%. There was also a significant decrease in hallucinations, anxiety and depression.30 Moreover, CBT principles also improve CPAP therapy adherence and its overall effect.31,32 In a more recent works a study by Hwang et al showed significant improvement in sleep measured by PSQI in 63 patients with schizophrenia.33 Waters et al in their study divided patients into three categories according to their response to CBT-i and found that total non-responders tended to have more severe psychopathology on average compared to partial and strong responders.34
Case Reports
All case reports are presented with informed consent of the patients and with approval of University Hospital in Olomouc.
Case 1
A 30 year-old woman treated for a long-term schizophrenic disorder attempted suicide via overdose. The patient did not report any developmental problems during her childhood or adolescence, and she was just more distant from her peers because she was more fearful, and the children mocked her. She did quite well in high school, was a good student, and actively did gymnastics. She handled social situations quite well but felt shy and insecure around strangers. After high school, she continued to study at university. In her sophomore year, when she was 21, she became convinced that she was being watched and withdrew from social activities. She shut herself in the house, stopped going to school, and was afraid to go out on the street, where she felt cars with dark windows were chasing her. Her parents brought her to a psychiatric hospital, and she was diagnosed with schizophrenia, a paranoid type. She was treated with atypical antipsychotics (risperidone – 4mg). The medication worked well; she finished college at 26. After graduating from university, she started teaching at an elementary school but was not very good at it because she could not handle children. Then she started working as a clerk in the social sphere. She coped with the work with difficulty because she did not tolerate even minor conflicts in the face of the client’s demands. At that time, her uncle, to whom she was very attached, committed suicide. She began having auditory hallucinations accusing her of being responsible for his death. Although her parents repeatedly told her it was not her fault, she did not believe them. She became pessimistic about the future because her salary was low. She did not see the possibility of moving away from her family because she could not afford to pay the rent on her own in the city she lived in. She began to perceive sleep disturbances such as difficulty falling asleep and maintaining sleep.
The psychiatrist prescribed her levomepromazine 25 mg and zolpidem 10 mg along with risperidone (stable 4 mg). The patient did not admit that she had not taken risperidone for three months. She started taking zolpidem and levomepromazine for insomnia but did not return to risperidone. Sleep was not improving. After two weeks, the patient swallowed 20 tablets of zolpidem and ten tablets of levomepromazine with suicidal intent. Her father found her unconscious and called the emergency services. She regained consciousness quickly and remained drowsy after inpatient care at the intensive care unit. A psychiatric assessment was conducted. It discovered auditory hallucinations and the feeling of being watched by the secret police. The patient admitted to suicidal thoughts and an attempt. She feels that nothing good awaits her in life. She has schizophrenia, and no one cares about her. She is dependent on her parents, and she has no partner. She was transferred to the psychiatric ward. The doctors returned to the original risperidone 4 mg medication and added the antidepressant mirtazapine 15 mg to levomepromazine 25 mg in a night dosage. Within three weeks, the patient calmed down, said that the hallucinations had disappeared, that she was no longer afraid of the secret police, and that her sleep and mood had improved.
She wanted to be released home quickly, so she pretended to be healthy. She started going to work again and tried to be as efficient as possible. However, she was tense with hallucinations and feelings of persecution, and the time she slept quickly shortened. Again, there was a feeling of exhaustion and that life was difficult. She began to think about suicide again, and there was an increase in anxiety and hopelessness. Her father recognised that she was not well and took her to a psychiatrist. There she admitted that she stopped taking risperidone again because she did not believe it would help her. She only took hypnotic drug (zolpidem 10 mg), but it did not help. She also admitted that she no longer felt like living. The doctor expressed understanding and convinced her to start a long-acting injectable antipsychotic (LAI) paliperidone 100 mg every four weeks. The patient continued to take hypnotic drug (zolpidem 10 mg).
The condition improved, the patient went to work, stopped being paranoid, and the hallucinations disappeared. Nevertheless, sleep remained shortened. She often woke up during night. Cognitive behavioural therapy was therefore started in about three months. CBT insomnia consisted of 8 sessions lasting 30 minutes each. The first two educational sessions focused on mapping and strengthening sleep hygiene and creating a suitable environment for sleep. In the next six sessions, the therapist and the patient tried to find other ways to improve sleep. The therapist emphasised the need for a regular rhythm during the day and sleep. Get up and sleep and have breakfast and dinner at the same time each day. The patient also tried to get carbohydrates as a small dinner before bed, stopped watching the watch, warmed up her body with a warm bath before bed, stopped napping after work, and bought black curtains for her room so outside lights would not get into the bedroom. She also tried to get up early to exercise in the morning. Sleep time gradually increased, but by the sixth session, she claimed that she still had trouble falling asleep in the evening and felt very sleepy the next day, even though total sleep time had increased. The doctor realised that higher doses of levomepromazine could paradoxically lead to sedation during the morning of the following day and then worsen the ability to fall asleep in the evening, so they also discontinued both levomepromazine and zolpidem gradually, and the patient remained only on LAI antipsychotics. The patient reported improved sleep even without hypnotic drug in the next session. The improved sleep status is maintained at the next check-up in a week. Then the patient is invited for regular check-ups once a month - The condition is good, the patient works, deny psychotic symptoms, and sleeps well.
Case 2
A 43-year-old male was treated for more than ten years by a psychiatrist due to schizophrenic disorder. He gradually gained weight, estimated at least 30 kilograms, as a side-effect of the medication. The last year had, the subject also depressive symptoms, increased fatigue and was unable to work for more than one year (previously worked as a sell-keeper). For the last six months, he was hospitalised for 30 days in the psychiatry ward for therapy titration. Moreover, his surroundings complained about his loud snoring and sleep apnoeas. The subject had the subjective feeling of excessive daytime sleepiness, but he filled the Epworth sleepiness scale with 6 points. The snoring, history of apnoeas and obesity were reasons for the night sleep testing of the patient. Screening examination by limited respiratory polygraphy revealed hyposaturation (100% of time under 90% of saturation and 79% of time under 85%) and apnoea-hypopnoea index (AHI) 7. The patient, meantime, started a programme of controlled weight reduction by the obesitologist. The medication at the time of admission was: bupropion (300 mg single dose in the morning), quetiapine (100 mg single dose in the evening), pregabalin (450 mg twice a day each 12 hours) (all prescribed by the psychiatrist) and allopurinol (due to hyperuricemia). He was a smoker for over 20 years, with a history of 20 pack-years.
At the time of initial examination, anthropometric parameters were listed in Table 1. The polysomnography (PSG) revealed severe obstructive sleep apnoea syndrome and hypoventilation syndrome (in obesity). The wake time after sleep onset was increased, with numerous arousals after apnoeas. The REM sleep and slow wave sleep were reduced significantly, and another PSG finding was without pathology (Figure 1, Figure 2). Complete parameters of the sleep apnoea syndrome are also listed in Table 1. He had no alcohol or other substance abuse history. Due to severe hyposaturation, arterial blood gasses analysis was also performed to exclude respiratory failure. The results showed only mild hypercapnia (6.58 kPa), consistent with the obesity hypoventilation diagnosis, and the partial oxygen pressure was within the normal range (10.2 kPa).
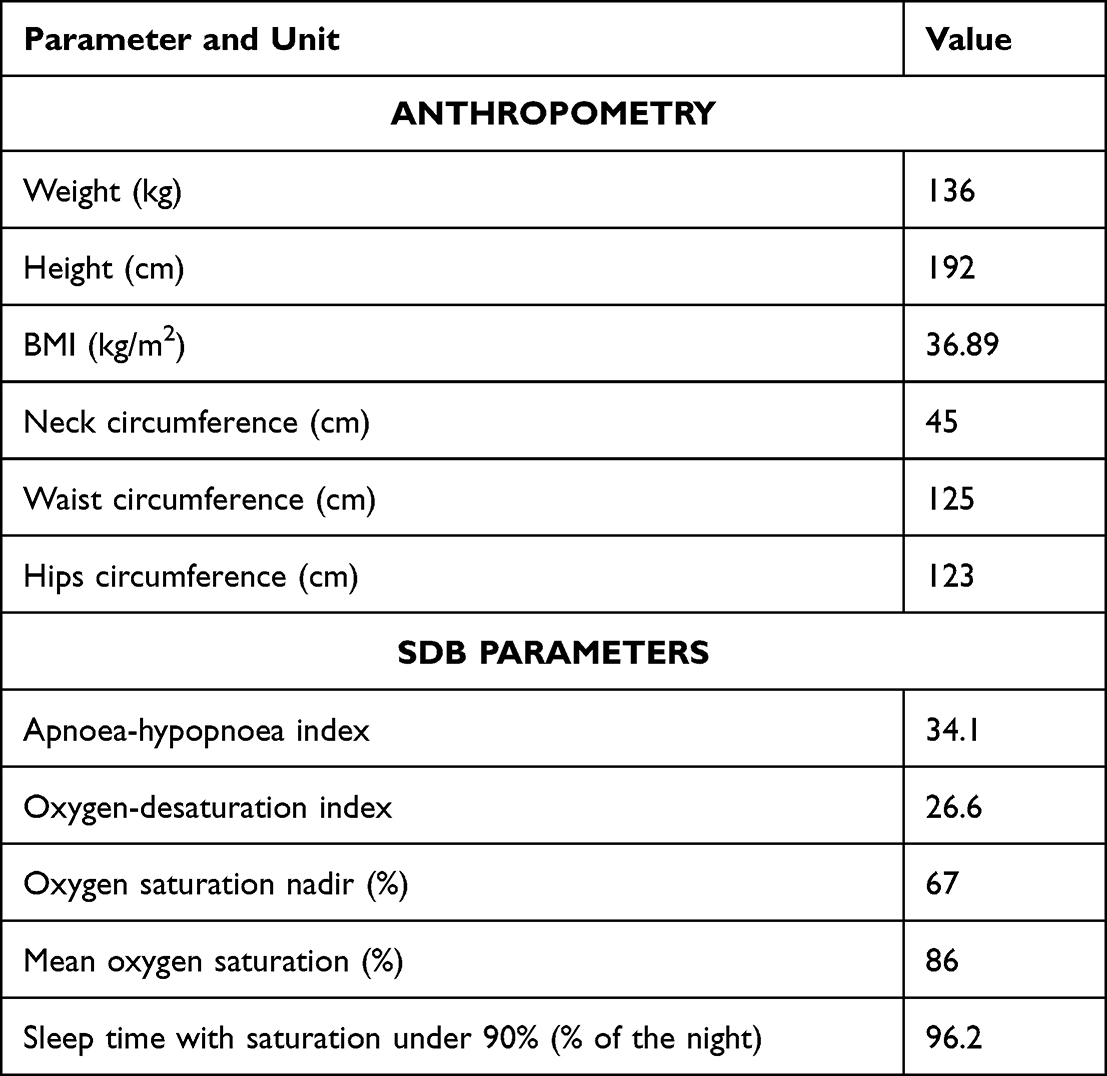 |
Table 1 Anthropometry and SDB Parameters of the Patient |
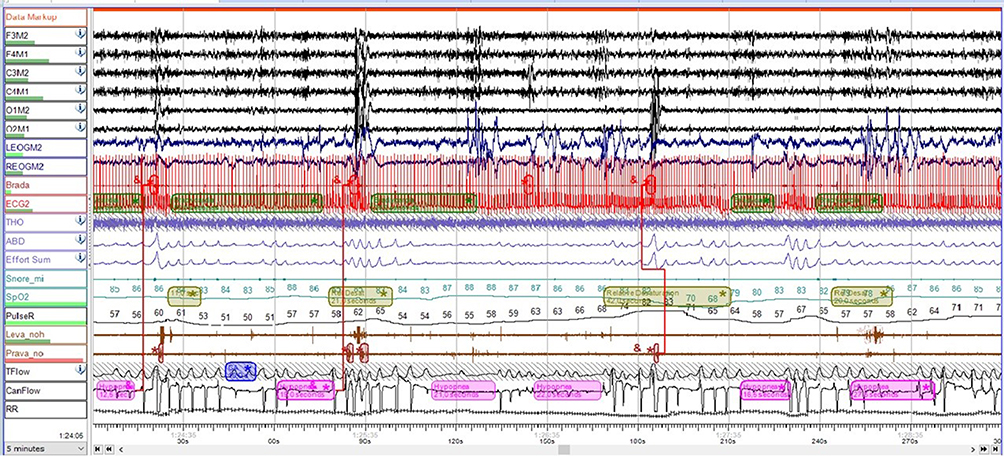 |
Figure 1 Polysomnography of the patient – numerous hypopnoea with consequent drops in the oxygen saturation. |
 |
Figure 2 Sleeps stages and respiratory events of the patient. |
The otorhinolaryngologist examination was normal, without the indication for surgical treatment of SDB and without contraindication to the PAP therapy. Afterwards, the treatment was initiated, and the sleep laboratory technician manually titrated the optimal pressures for the therapy. The initial setting of the machines was: volume-adjusted bi-level positive airway pressure therapy with expiratory pressure of 7 hPa and pressure support of 4–12 hPa. The tidal volume was set at 700 mL, with a breath rate of 16 per minute. The therapy was well tolerated, and the application of the therapy was submitted to the revision physician of the patient’s insurance company. The treatment was approved, and our department contacted the patient to educate him on using and signing equipment rental contracts. On this occasion, the first conflict with the patient arose. The subject felt unsure if he should sign the contracts, as he was worried about possible financial consequences in case of the machine damage.
Moreover, he stated that he was humiliated by the technician. The technician had unilateral facial nerve paresis; according to the patient, she was strangely gazing at him. The technician negated any verbal or another conflict with the patient. The patient disagreed with the contract signature at the time of education and requested more time to consider it. We patiently educated him about the impact of untreated SDB and made a deal with him to decide on the treatment up to one month later. After four weeks, the patient returned, signed the contracts, and started PAP therapy. Shortly after, he stated that the set pressures were too high for him, and he could not sleep with the machine. In addition, he also requested the mask change, as he felt uncomfortable with the mask he was given. He also stated that he is worried about his health. He was asked if the machine could not kill or hurt him. Once again, we educated the patient and deescalated the pressures on the machine – the new setting was bi-level positive airway pressure therapy (BPAP) in spontaneous breathing mode and stable pressures of expiratory pressure of seven hPa and inspiratory pressure of 11 hPa. We also changed the mask type for a different type of nasal mask. He also started with cognitive behavioural therapy (CBT) by the psychologist in our department. On the next check-up (after three months of therapy), he requested the presence of his psychologist at the examination. At this point, total BPAP use was 282 hours, ie average of 3 hours per night. However, the adherence and tolerance gradually improved, and in the last month, the adherence level was better, with average use of 4.5 hours BPAP per night. Residual AHI was 4, which was considered to be an effective treatment. He also stated that he is no longer sleepy and started to work again. The CBT was continued, and the overall life quality of the patient was improved. No admission to the psychiatry ward was needed in the first six months of the BPAP treatment. He attended the weight loss treatment program for one year, and after PAP, therapy began to be more effective in his weight reduction, and he has lost up to 10 kilograms until now.
Case 3
A 46-year-old woman was treated for schizoaffective disorder since she was 18. She was admitted for inpatient care for the eighth time in her life. She was also treated for hypothyroidism and hypertension and had a positive family history of psychotic disorders and dementia. She was living with her husband and had a son of 22 years. She was a non-smoker and was not taking any alcohol or illicit substances. She was working part times job and had a pension due to a psychiatric disorder. During the treatment, she was taking numerous antipsychotics. At the time of admission, she took 15 mg of olanzapine in combination with 150 mg of clomipramine. She was admitted for a depressive episode with psychotic symptoms.
The main clinical symptoms upon admission were depressed mood, anhedonia, abulia, hypoprosexia and micromagnetic delusions. As a side effect of antipsychotic medication, she had a BMI of 42.72 (height 169 cm and weight 122 kg) at the time of admission. In the routine lab scan upon admission, we found a slightly elevated CRP of 8.9 mg/l and borderline glycaemia of 6.5 mmol per litre. She also underwent a CT scan and discovered that she had bilaterally atrophy of the frontal lobes.
During the inpatient care, we switched antidepressants from clomipramine to duloxetine, 120 mg daily. Since the patient was already suffering from metabolic syndrome and had hyperglycaemia in her lab scan, we switched antipsychotics as well to more metabolically neutral aripiprazole, 30 mg per day. Gradually psychotic symptoms regressed, and the patient’s mood improved—however, residual symptoms such as loss of energy, hypobulie and hypoprosexia. Nurses during regular night check-ups also observed severe snoring with breathless pauses inpatient. In the wider diagnostic consideration, we used a screening device for obstructive sleep apnoea syndrome and discovered severe obstructive sleep apnoea syndrome with an Apnoea hypopnoe index of 35, oxygen desaturation index of 22.5 and average time under 90% saturation being 25%.
After the screening, we sent the patient to a standard diagnostic process in a sleep laboratory, and it was confirmed that the patient was suffering from severe obstructive sleep apnoea syndrome, and she was indicted for CPAP treatment. She underwent an otorhinolaryngologist examination with normal findings, without the indication for surgical treatment of the sleep-disordered breathing and without the CPAP therapy. The optimal pressures and volumes for the therapy were titrated for the patient. The therapy was well tolerated. Upon psychiatrist check-up, one month after the start of the CPAP therapy patient significantly improved clinically. Residual shared symptoms between depressive episodes and obstructive sleep apnoea subsided, and the patient was referred to a normal level of energy and volition. As the patient was not in outpatient care of our department, we contacted her again six months after discharge, and she confirmed stable remission of both schizoaffective disorder and obstructive sleep apnoea and even a slight loss of weight of 12kg.
Discussion
The first case showed that even patients with schizophrenia with sleep disorders could benefit from cognitive behavioural therapy. CBT procedures can help prevent polypharmacy, which can adjust the length of sleep but can also lead to sleepiness the next morning and, paradoxically, worsen falling asleep in the evening. Although CBT-i is time-consuming, it requires about 8–10 meetings once a week, it is an effective procedure that can help the overall improvement of the patient.29,33 Improving sleep can then strengthen the stability of recovery and thus act synergistically with the long-acting antipsychotic.1 In addition, CBT strengthens the patient’s confidence that he can improve his quality of life through his behaviour.29
The second case demonstrated that treatment of SDB improves life quality in schizophrenic individuals.32 The PAP therapy setting was more complicated, but the result was favourable. CBT was an adjunct therapy to psychopharmaceuticals and improved PAP compliance. This resulted in an improvement in the overall condition of the subject. He started in the new employment, which shows good compensation for the schizophrenia. No further admissions to the psychiatric ward were needed.
The third case in our series presents the clinical significance of the broader diagnostic process. It is established in contemporary literature that obstructive sleep apnoea shares several symptoms with the depressive disorder spectrum, even when part of other diagnostic units such as schizoaffective disorder in a provided case report.35 Residual depressive symptoms, as a major topic in psychiatry, can be, in certain cases, part of comorbid disorders, especially when the residual symptoms are prominently part of the somatic symptoms of depression (loss of energy, e.g.).36 Contemporary literature suggests actively screening for OSA in psychiatric patients with risk factors.37 Since weight gain is a common side effect in many psychopharmacs, untreated and undiagnosed secondary obstructive sleep apnoea induced by the weight gain during psychiatric treatment is a potentially significant risk factor that might contribute to an already shorter life span of patients with severe mental disorders.35 Moreover, recent literature shows that the weight gain in patients with schizophrenia can lead to a metabolic syndrome that further impair quality of sleep.17
Another factor to consider in patients with schizophrenia is a natural chronotype of each individual patient. Recent literature points to a key role of eveningness chronotype as an intermediate factor between poor sleep quality, metabolic syndrome, and schizophrenia.17
In two cases - cases 2 and 3 - weight reduction was also observed after stabilising the condition and effective PAP therapy. However, PAP therapy alone does not lead to weight loss.38,39 Much more effective is a combination of exercise and rationalisation of the diet with the help of the specialist.39
Main limitation of our case series is a small number of patients that prevent greater generalizability. Other limitation of our case series is the lack of measurement of the effects of CBT and CPAP therapy via standardised scales such as PANSS, and PSQI that could further quantify the effect of interventions.
Conclusion
Disruption of adequate peaceful sleep, which leads to a feeling of rest, can have a negative effect on the severity of the psychopathology of schizophrenic disease. It can be a prodrome of a new attack, a symptom of an acute exacerbation, or a chronic residual symptom. Insomnia impairs the patient’s quality of life and can contribute to the severity of delusions and hallucinations and worsening cognitive deficits. Assessment of insomnia in patients with schizophrenia should become a routine practice and a specific target of pharmacological and non-pharmacological therapy. Sleep disordered breathing is another major problem impacting the patients’ overall condition. With effective treatment of both disorders, we can improve quality of life together with prognosis. Cognitive behavioural therapy is an efficient tool in treating insomnia and may also be used as an adjunct to positive airway pressure therapy. All obese patients should be encouraged to the weight reduction.
We conclude that the health care of the patients with schizophrenia has to be complex and personalised for the patient’s requirements.
A Statement Confirming Consent to Publish
Informed consent was obtained from all patients whose cases are published in the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cohrs S. Sleep disturbances in patients with schizophrenia: impact and effect of antipsychotics. CNS Drugs. 2008;22(11):939–962. doi:10.2165/00023210-200822110-00004
2. Sheaves B, Freeman D, Isham L, et al. Stabilising sleep for patients admitted at acute crisis to a psychiatric hospital (OWLS): an assessor-blind pilot randomised controlled trial. Psychol Med. 2018;48:1694–1704. doi:10.1017/S0033291717003191
3. Afonso P, Viveiros V, Vinhas de Sousa T. Sleep disturbances in schizophrenia. Acta Med Port. 2011;24(Suppl 4):799–806.
4. Harvey A, Murray G, Chandler RA, Soehner A. Sleep disturbance as transdiagnostic consideration of neurobiological mechanisms. Clin Psychol Rev. 2011;31:225–235. doi:10.1016/j.cpr.2010.04.003
5. Wulff K, Gatti S, Wettstein JG, Foster RG. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat Rev Neurosci. 2010;11:589–599. doi:10.1038/nrn2868
6. Freeman D, Brugha T, Meltzer H, Jenkins R, Stahl D, Bebbington P. Persecutory ideation and insomnia: findings from the second British National Survey of Psychiatric Morbidity. J Psychiatr Res. 2010;44:1021–1026. doi:10.1016/j.jpsychires.2010.03.018
7. Freemna D, McManus S, Brugda T, Meltzer H, Jenkins R, Bebbington P. Concomitants of paranoia in the general population. Psychol Med. 2011;41:923–936. doi:10.1017/S0033291710001546
8. Freman D, Stahl D, McManus S, et al. Insomnia, worry, anxiety and depression as predictors of the occurrence and the persistence of persecutory ideation. Soc Psychiatry Psychiatr Epidemiol. 2012;47:1195–1203. doi:10.1007/s00127-011-0433-1
9. Freeman D, Startup H, Myers E, et al. The effects of using cognitive behavioural therapy to improve sleep for patients with delusions and hallucinations (the BEST study): study protocol for a randomised controlled trial. Trials. 2013;14:214. doi:10.1186/1745-6215-14-214
10. Myers E, Startup H, Freeman D. Cognitive behavioral treatment of insomnia in individuals with persistent persecutory delusions. J Behav Ther Exp Psychiatry. 2011;42:330–336. doi:10.1016/j.jbtep.2011.02.004
11. Monti JM, Monti D. Sleep disturbance in schizophrenia. Int Rev Psychiatry. 2005;17:247–253. doi:10.1080/09540260500104516
12. Chan MS, Chung KF, Yung KP, Yeung WF. Sleep in schizophrenia: a systematic review and meta-analysis of polysomnographic findings in case-control studies. Sleep Med Rev. 2017;32:69–84. doi:10.1016/j.smrv.2016.03.001
13. Bian Y, Liang WY, Yue WH, et al. Sleep architecture in drug naive patients with schizophrenia: a meta-analysis. Chinese Ment Heal J. 2017;31:208–214.
14. Palmese LB, DeGeorge PC, Ratliff JC, et al. Insomnia is frequent in schizophrenia and associated with night eating and obesity. Schizophr Res. 2011;133(1–3):238–243. doi:10.1016/j.schres.2011.07.030
15. Kirlioglu SS, Balcioglu YH. Chronobiology revisited in psychiatric disorders: from a translational perspective. Psychiatry Investig. 2020;17(8):725–743. doi:10.30773/pi.2020.0129
16. Kivelä L, Papadopoulos MR, Antypa N. Chronotype and psychiatric disorders. Curr Sleep Med Rep. 2018;4(2):94–103. doi:10.1007/s40675-018-0113-8
17. Balcioglu SSK, Balcioglu YH, Devrim Balaban O. The association between chronotype and sleep quality, and cardiometabolic markers in patients with schizophrenia. Chronobiol Int. 2022;39(1):77–88. doi:10.1080/07420528.2021
18. Suttajit S, Pilakanta S. Prevalence of metabolic syndrome and its association with depression in patients with schizophrenia. Neuropsychiatr Dis Treat. 2013;9:941–946. doi:10.2147/NDT.S47450
19. Perlis ML, Smith LJ, Lyness JM, et al. Insomnia as a risk factor for onset of depression in the elderly. Behav Sleep Med. 2006;4(2):104–113. doi:10.1207/s15402010bsm0402_3
20. Björnsdóttir E, Janson C, Gíslason T, et al. Insomnia in untreated sleep apnea patients compared to controls. J Sleep Res. 2012;21(2):131–138. doi:10.1111/j.1365-2869.2011.00972.x
21. Ban HJ, Kim SC, Seo J, Kang HB, Choi JK. Genetic and metabolic characterisation of insomnia. PLoS One. 2011;6(4):e18455. doi:10.1371/journal.pone.0018455
22. Bak M, Fransen A, Janssen J, van Os J, Drukker M. Almost all antipsychotics result in weight gain: a meta-analysis. PLoS One. 2014;9(4):e94112. doi:10.1371/journal.pone.0094112
23. Lee JH, Cho J. Sleep and obesity. Sleep Med Clin. 2022;17(1):111–116. doi:10.1016/j.jsmc.2021.10.009
24. Rodrigues GD, Fiorelli EM, Furlan L, Montano N, Tobaldini E. Obesity and sleep disturbances: the “chicken or the egg” question. Eur J Intern Med. 2021;92:11–16. doi:10.1016/j.ejim.2021.04.017
25. Okada I, Miyata S, Iwamoto K, Fujishiro H, Noda A, Ozaki N. Prevalence of obstructive sleep apnea as assessed by polysomnography in psychiatric patients with sleep-related problems. Sleep Breath. 2022;26:1983–1991. PMID: 35029795. doi:10.1007/s11325-022-02566-6
26. Hermes ED, Sernyak M, Rosenheck R. Use of second-generation antipsychotic agents for sleep and sedation: a provider survey. Sleep. 2013;36(4):597–600. doi:10.5665/sleep.2554
27. Batool-Anwar S, Goodwin JL, Kushida CA, et al. Impact of continuous positive airway pressure (CPAP) on quality of life in patients with obstructive sleep apnea (OSA). J Sleep Res. 2016;25(6):731–738. doi:10.1111/jsr.12430
28. Giles JJ, Ling I, McArdle N, et al. Obstructive sleep apnea is treatable with continuous positive airway pressure in people with schizophrenia and other psychotic disorders. Schizophr Bull. 2022;48(2):437–446. doi:10.1093/schbul/sbab100
29. Freeman D, Dunn G, Startup H, et al. Effects of cognitive behaviour therapy for worry on persecutory delusions in patients with psychosis (WIT): a parallel, single-blind, randomised controlled trial with a mediation analysis. Lancet Psychiatry. 2015;2(4):305–313. doi:10.1016/S2215-0366(15)00039-5
30. Espie CA, MacMahoon KMA, Kelly H, et al. Randomized clinical effectiveness trial of nurse-administered small-group cognitive behaviour therapy for persistent insomnia in general practice. Sleep. 2006;30:574–584. doi:10.1093/sleep/30.5.574
31. Sánchez AI, Martínez P, Miró E, Bardwell WA, Buela-Casal G. CPAP and behavioral therapies in patients with obstructive sleep apnea: effects on daytime sleepiness, mood, and cognitive function. Sleep Med Rev. 2009;13(3):223–233. doi:10.1016/j.smrv.2008.07.002
32. Richards D, Bartlett DJ, Wong K, Malouff J, Grunstein RR. Increased adherence to CPAP with a group cognitive behavioral treatment intervention: a randomised trial. Sleep. 2007;30(5):635–640. doi:10.1093/sleep/30.5.635
33. Hwang DK, Nam M, Lee YJG. The effect of cognitive behavioral therapy for insomnia in schizophrenia patients with sleep disturbance: a non-randomized, assessor-blind trial. Psychiatry Res. 2019;274:182–188. doi:10.1016/j.psychres.2019.02.002
34. Waters F, Chiu VW, Dragovic M, Ree M. Different patterns of treatment response to Cognitive-Behavioural Therapy for Insomnia (CBT-I) in psychosis. Schizophr Res. 2020;221:57–62. doi:10.1016/j.schres.2020.03.054
35. Vanek J, Prasko J, Genzor S, et al. Obstructive sleep apnea, depression and cognitive impairment. Sleep Med. 2020;72:50–58. doi:10.1016/j.sleep.2020.03.017
36. Paykel ES. Partial remission, residual symptoms, and relapse in depression. Dialogues Clin Neurosci. 2008;10(4):431–437. doi:10.31887/DCNS.2008.10.4/espaykel
37. Braitman DV. Screening for sleep apnea in psychiatry. Am J Psychiatry Resid J. 2018;13(5):5–7. doi:10.1176/appi.ajp-rj.2018.130502
38. Redenius R, Murphy C, O’Neill E, Al-Hamwi M, Zallek SN. Does CPAP lead to change in BMI? J Clin Sleep Med. 2008;4(3):205–209. doi:10.5664/jcsm.27181
39. Drager LF, Brunoni AR, Jenner R, Lorenzi-Filho G, Benseñor IM, Lotufo PA. Effects of CPAP on body weight in patients with obstructive sleep apnoea: a meta-analysis of randomised trials. Thorax. 2015;70(3):258–264. doi:10.1136/thoraxjnl-2014-205361
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.