")
Back to Journals » International Journal of General Medicine » Volume 14
The Magnitude of Failed Induction of Labor and Associated Factors Among Women Delivered at Public Hospitals of Arsi Zone, Southeast Ethiopia, 2020: A Cross-Sectional Study
Received 5 May 2021
Accepted for publication 7 September 2021
Published 23 September 2021 Volume 2021:14 Pages 6021—6033
DOI https://doi.org/10.2147/IJGM.S318441
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mulatu Desta,1,2 Abdissa Duguma2,3
1Arsi University, College of Medical Sciences, Department of Nursing, Bokoji, Ethiopia; 2Wollega University, Institute of Health Sciences, Department of Nursing, Nekemte, Ethiopia; 3Mettu University, College of Medical Sciences, Department of Nursing, Mettu, Ethiopia
Correspondence: Abdissa Duguma
Mettu University, P.O. Box 318, Mettu, Ethiopia
Tel +251 923761502
Email [email protected]
Background: Failed induction of labor is one challenge in all obstetrics care given all over the world, which increases the incidence and percentage of cesarean sections. It is still a major challenge in both developed and developing countries. This study was significant because it identified the magnitude and associated factors of failed induction of labor.
Objective: To assess the magnitude of failed induction of labor and associated factors among women delivered at public hospitals in the Arsi zone, South East Ethiopia.
Methods: We conducted institutional-based cross-sectional study design in public hospitals in the Arsi zone. We used random-sampling methods, and collected the data using a structured questionnaire and checklist and analysed using a statistical package for social science (SPSS) version 25 software, described and presented data using texts, tables, and charts. We took those variables with a p-value of 0.05 as statistically significant determinants of failed induction of labor.
Results: The magnitude of failed induction of labor was 21.3%. AOR =8.788, 95% CI = (2.884– 12.397), maternal residence in urban [AOR=0.356, 95% CI: (0.143– 0.886)], multi para 0.390 times less likely than prime para with odds ratio [AOR=0.390, CI: (0.147, 0.632)], Bishop score before induction started 4 [AOR=5.155, CI: 3.062– 7.387]. Indications for IOL: PROM more likely than IUGR [AOR=4.158, 95% CI: (2.415, 9.554)], time from start of induction to deliver less than twelve hours [AOR=6.511, 95% CI: (2.477, 10.116)], were statistically significant determinants of failed induction of labor.
Conclusion: Magnitude of failed induction of labor was law in Arsi zone public hospitals when compared to the study done in St. Luke C. Hospital. The factors identified as significantly associated with FIOL in this study were maternal age, maternal residence, prime para, Bishop score four, indications for induction of labor: PROM and post-term pregnancy, and time from the start of induction to deliver, twelve hours.
Keywords: associated factors: failed induction, labor, Arsi zone, Ethiopia
Introduction
Induction of labor (IOL) is the process of artificially stimulating the uterus to start labor.1 Induction of labor is a common obstetric procedure, and performed when the benefits to either the mother or fetus outweigh those of continuing the pregnancy. The indication of Hypertensive Disorders of Pregnancy is eclampsia, Post-term pregnancy, Intra-uterine Fetal Death (IUFD), congenitally abnormal fetus incompatible with life, Premature Rupture of Membranes (PROM), Rh-Isoimmunization, Gestational Diabetes mellitus at term, Intra-uterine Growth Retardation (IUGR), Placental Abruption and minor degree the goal of labor induction must always be to ensure the best possible outcome for the mother and newborn.2
Most studies define failed IOL as the impossibility of achieving a vaginal delivery, although many other factors appear during labor that may hinder or prevent a vaginal delivery.3
Induction of labor is safe and beneficial in well-selected and properly monitored high-risk pregnancies.4 Health care institution carried out Induction of labor when the risk of continuing pregnancy outweighs the benefits. Failed induction of labor is when induced labor fails to cervical dilatation or unable to progress even though there was a good contraction and either of those ends in a caesarean section.5,6 vaginal delivery is the goal of the induction process. However, this occurs less often than when a woman’s labor spontaneously.7,8
It is important to perform Induction of labor (IOL) with caution since the procedure carries the risk of uterine hyper-stimulation, uterine rupture, and non-reassuring fetal heart rate tracing. Failed induction of labor does not show a caesarean section. Health care institution perform induction of labor (IOL) with caution since the procedure carries the risk of uterine hyper-stimulation, uterine rupture, and non-reassuring fetal heart rate tracing. Failed induction of labor does not show a caesarean section. Where possible, they perform IOL at facilities where a caesarean section is relevant.9 longer latent labor time only allows a woman to have a full opportunity to have a safe, successful vaginal delivery. The minimum allowed time is 24 hrs after cervical ripening and oxytocin administration before diagnosing a failed induction.10
Globally, maternal mortality has declined by 44% since 1990, with about 303,000 maternal deaths in 2015. The maternal mortality ratio is the highest in the African Region at 542 per 100 000.11 Globally, the number of neonatal deaths decreased by half from 5 million in 1990 to 2.5 million in 2017. In the African Region, the share of neonatal deaths is 37%.11
According to the Ethiopian demographic health survey (EDHS) 2016, maternal mortality in Ethiopia is 412 deaths per 100,000 live births, which is a high and unacceptable death related to world health organization (WHO) standards.12
According to the 2019 Ethiopian mini demographic health survey (EMDHS), the neonatal mortality rate in Ethiopia is 30 deaths per 1,000 live births.13
In recent decades, more and more pregnant women around the world have undergone IOL to deliver their babies and In developed countries, up to 25% of all deliveries at term now involve IOL and also in developing countries, the rates are lower, but in some settings, they can be as high as those observed in developed countries.
In the United States, the incidence of labor induction rose 2.5-fold from 9.5% in 1991 to 23.8% in 2015. At Parkland Hospital, approximately 35% of labor is induced or augmented.14 According to a study done in Nigeria in 2016, the IOL rate was 12.7%.16 The prevalence of failed induction of labor varies from place to place. In the tertiary care hospital in Bhubaneswar, Odisha, India in 2016, the failed IOL was 50.5%. At Paropakar Maternity and Women’s Hospital, Thapathali, Kathmandu, Nepal, the failure rate of induction was 23.5%. In Southwest Nigeria in 2016, the failed IOL was 36.5%. In Ethiopia, failed induction of labor: in Wolaita Sodo, South Ethiopia, 26.5%, in Hawassa Public Health Facilities, Ethiopia, 2015, 17.3%, in Dessie Referral Hospital in 2017, 19.7%, in Jimma University Specialized Hospital, failed induction was diagnosed at 21.4%, and in Wolliso St. Luke, Catholic Hospital, South West Shewa, in 2017, failed IOL was 42%.3,8,15–20.
Failed induction of labor is the challenge in all obstetrics care given all over the world, which increases the incidence and percentage of C-sections, especially related to failed induction of labor. Most failed inductions ended with caesarean delivery. Caesarean delivery has a risk of adverse maternal outcomes following delivery by caesarean delivery: Overall severe morbidity and mortality, maternal mortality, amniotic fluid embolism, placental abnormalities, urinary incontinence, postpartum depression, and adverse neonatal outcome: Respiratory morbidity increases more than vaginal delivery.21 Failed induction of labor is Challenging in all obstetric care being given all over the world, including developed countries.
Methods and Materials
Study Area and Period
We conducted this study in selected public hospitals in the Arsi Zone, Oromia regional state, in the South East of Ethiopia. The Arsi Zone is one of the twenty zones found in the Oromia Regional State. Arsi Zone has 25 woreda and four urban administrations (Huruta, Abomsa, Dhera, and Bokoji). The total population of the Arsi zone is 3,589,624, of these, males 1,758,915 and females 1,830,708. (40) Arsi Zone has one referral and teaching hospital (Arsi University referral and teaching hospital) and seven public (governmental) primary hospitals (Bokoji Primary hospital, Abomsa Primary hospital, Gobessa Primary hospital, Kersa Primary hospital, Robe Dida Primary hospital, Kula Primary hospital, Chancho Primary hospital). The town in the Arsi zone is Asella, which is 175 km from Addis Ababa. We carried out the study from March 16 to May 16, 2020.
Study Design
We conducted an institution-based cross-sectional study design.
Population
Source Population
The source population of the study was those who gave birth at public hospitals in the Arsi zone, southeast Ethiopia, during the study period.
Study Population
The study population was those mothers who underwent induction of labor at selected public hospitals in the Arsi zone, southeast Ethiopia, during the study period.
Eligibility Criteria
Inclusion Criteria
All women attended the induction of labor after 28 weeks of gestational age at the selected public hospitals in the Arsi zone during the study period.
Exclusion Criteria
We excluded Women who referred to higher hospitals for further diagnosis and management in case of emergency after induction of labor started.
Sample Size Determination
We calculated the sample size by using a single population formula for objective one and calculating the sample size for objective two by using Epi Info version 7.2.2.10 software.
The sample size for the magnitude of failed induction of labor
n = (Z/2) 2 P (1-P)
Where:
n = sample size
Z = standard normal distribution corresponding to significance level at = 0.05 p = proportion of failed induction of labor
we assumed the “P” proportion of failed induction of labor is to be 19.7%, which is taken from a study conducted at Dessie Referral Hospital in 2019. 3
d = margin of error of 5%
= 3.84 (0.197) (0.803) = 0.0025
By adding 10% of the non-response rate to the sample size, 243+10% of the calculated sample size will be 243+24 = 267
The sample size for associated factors of failed induction of labor. We calculated the sample size for objective two by using Epi Info version 7.2.2.10 software. We took the proportion of associated factors from previous studies conducted at Hawassa Public Health Facilities, Ethiopia, in 2015. Advanced maternal age, poor Bishop score, PROM, and greater gestation were significantly associated with failed induction of labor.18
We selected the final sample size as objective two (268), which was the largest sample size of the study (Table 1).
 |
Table 1 Sample Size Determination for Associated Factors of Failed Induction of Labor Among Women Delivered at Public Hospitals of Arsi Zone, South East, Ethiopia, 2020 |
Sampling Technique and Procedure
In the Arsi zone, there is one teaching and referral hospital and seven primary public hospitals (Bokoji hospital, Abomsa hospital, Chancho hospital, Kersa hospital, Kula hospital, Robe Dida hospital, and Gobessa hospital). This study was done at the selected three hospitals from the eight hospitals. The lottery method selected to select the three hospitals, AURTH, Bokoji primary hospital, and Kersa primary hospital. The proportional allocation of samples to each hospital was done based on the average estimated monthly IOL cases of the three hospitals based on the last two months of estimated induction of labor.
Within consecutive two months, there were about 300 inductions of labor. From these, 166 IOL cases from AURTH, 78 IOL cases from Kersa hospital, and 56 induction of labor cases from Bokoji Hospital. Then, we calculated the final sample size and proportionally allocated to those hospitals by considering their last 2 months of induction of labor cases. We collected data consecutively from all women who attended the induction of labor in the study area until we achieved the desired sample size (268) during the study period from March 16 to May 16, 2020.
n = required sample size (268)
Ni = Estimated number of inductions of labor in the past 2 months in a specific hospital
N = Total estimated number of inductions of labor in the past 2 months in all study areas (300) (Figure 1).
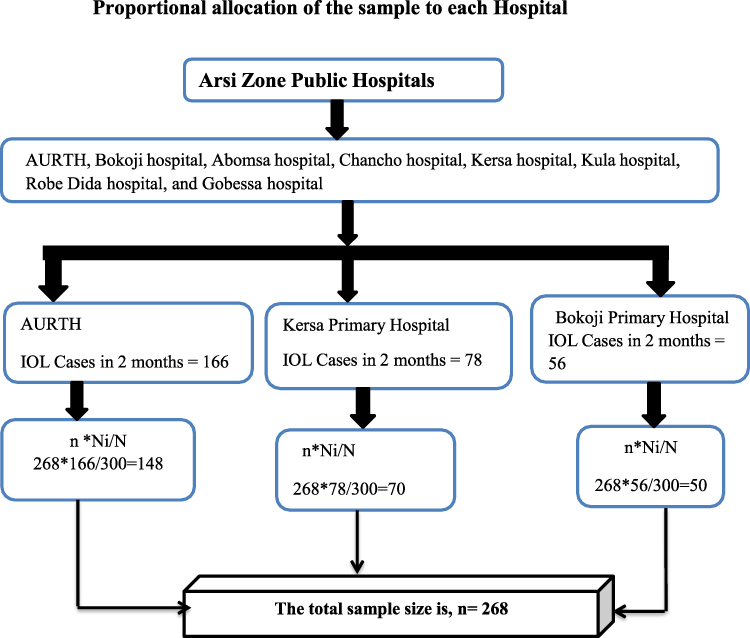 |
Figure 1 Schematic representation of the sampling techniques on the Magnitude of Failed Induction of Labor and Associated Factors among Women Attending Induction of Labor in Public Hospitals of Arsi Zone, South Ethiopia, 2020. |
Study Variables
Dependent Variable
Failed induction of labor.
Independent Variables
Socio-demographic factors of women: Age, residence.
Anthropometry: BMI
Obstetric factors: ANC follow-up, number of parity, gestational age, Bishop Score, blood pressure, weight and sex of the newborn, membrane status at the start of induction.
Oxytocin only, oxytocin with a prior cervical rip, misoprostol only, ARM, Foley catheter.
Indications for induction of labor: Post-term pregnancy, PIH, PROM, Oligohydramnios, Congenital anomaly, IUFD, chorioamnionitis, IUGR
Operational Definitions
Failed induction of labor: Diagnosed when there has been no cervical change or descent of the presenting part after 6–8 hours of Oxytocin administration and use of the maximum dose for at least one hour, or contraction of 3 in 10 min. (adequate uterine contraction) has not been achieved.6
The Bishop score is a method of assessing the cervical condition. Score 4 is unfavorable or unripened.
Score 5–8 is intermediate and score 9 is favorable.
Gestational age: Is the duration of pregnancy calculated from the first day of the last menstrual.
Period.
Parity: A state of previous pregnancy beyond the period of viability.
Post-term pregnancy: Is a pregnancy that has extended to or beyond the gestational age of 42.
Oligohydramnios: We used the diagnosis of Oligohydramnios based on the records on the patient cards or 294 days from the first day of the last normal menstrual period, or 40 weeks of gestation from the time of conception.
Data Collection Tools and Techniques
The tools contained a structured interviewer-administered questionnaire, an anthropometry measurement, and a checklist. Structured questionnaire has two parts: Part I socio-demographic factors and Part II obstetric factors. We used the structured questionnaires to collect data containing variables used to assess socio-demographic factors; obstetric factors from the study participants by direct interview. We initially adopted the questionnaire in the English language and then translated into Afaan Oromoo and re-translated back into the English language by a language expert. Since there was no similar questionnaire tool to assess the magnitude and associated factors of failed induction of labor in WHO, UNICEF, or other standardized organizations, the questionnaire was adapted from previous research.3,20 We used Cronbach’s alpha coefficient check reliability and validity data gathering instrument.
We recorded Anthropometry measurement (BMI) of mothers after delivery of the baby by using a weight and height scale. Finally, we used a checklist that contains obstetric factors, an indication of induction of labor, and methods of indication of labor.
Four Bsc nurses who are working in the study hospital in another ward collected the data and one Bsc midwife supervised during the data collection period. We assigned one data collector for each hospital from the same hospital staff (for Kersa primary hospital and Bokoji primary hospital), and two data collectors for AUTRH from the same hospital staff.
Data Quality Control
To ensure the quality of data gathered, we made pre-test on 5% (14 participants) of the sample size at the Abomsa Primary Hospital before the actual data collection started. We made the necessary modifications to the questioners based on the identified gaps. We gave a one-day training for data collectors and supervisors on the objective and relevance of the study, how to gather the appropriate information, procedures for data collection techniques, and the whole contents of the questionnaire before the actual data collection.
The supervisors and principal investigators reviewed and checked for completeness and relevance every day after data collection and they made a thorough check before receiving a questionnaire from each data collector during the whole data collection period. Principal investigators calibrated anthropometry measurements every week by triangulating with standard weight.
Data Analysis and Procedures
After we checked data for its completeness and consistency, the data cleaned, coded, entered into Epi data version 3.10, and exported to the SPSS version 25-software package for data analysis. The data were analyzed using logistic regression to determine the effect of various factors on the outcome variable. We carried out A Bi variable analysis to determine the association of different potential factors. Variables with a p-value of 0.25 were candidates for multivariate logistic regression to control the confounding effect. Those variables with a p-value of less than 0.05 we took as statistically significant determinants of failed IOL In multivariate logistic regression. In addition, we used Hosmer-Lemeshow goodness-of-fit test for checking model fitness with a p-value > 0.05. We presented the data using text, tables, and charts, frequencies, percentages, and medians.
Ethical Consideration
We took an ethical clearance letter from the Wollega University Ethical Review Board, and received approval letter from selected public hospitals in the Arsi zone. The ethical review board approved to provide Participants under 18 years of age were by the informed consent on their behalf. We explained the procedure and purpose of the study to the study participants and took written informed consent from them. We maintained confidentiality by the patient’s name not being included in the questioners and we conducted the study s per the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of the Respondents
In this study, 268 mothers were interviewed with a response rate of 100%, and their documents were reviewed during the study period. The median age of the respondents was 26 years, with a range of 16–45 years. Among respondents’ mothers, a greater proportion of 126 (47.0%) was Muslims, followed by Orthodox Christians 116 (43.3%), and 26 (9.7%) were protestant by religion. The majority of respondents’ marital status was 261 (97.4%) were married, 5 (1.9%) were single and 2 (0.7%) were divorced. Concerning educational level, 95 (35.4%) completed secondary education, while 79 (29.5%) were primary and 72 (26.7%) were college or above. Only 22 (8.2%) of respondents were unable to read and write. Regarding monthly income, the majority of respondents (128 (47.3%) had a monthly income of > 5358–10,015 ETB, 54 (20.1%) of the monthly income had 1100 ETB. 37 (13.8%) earned > 2344–5358 ETB (Table 2).
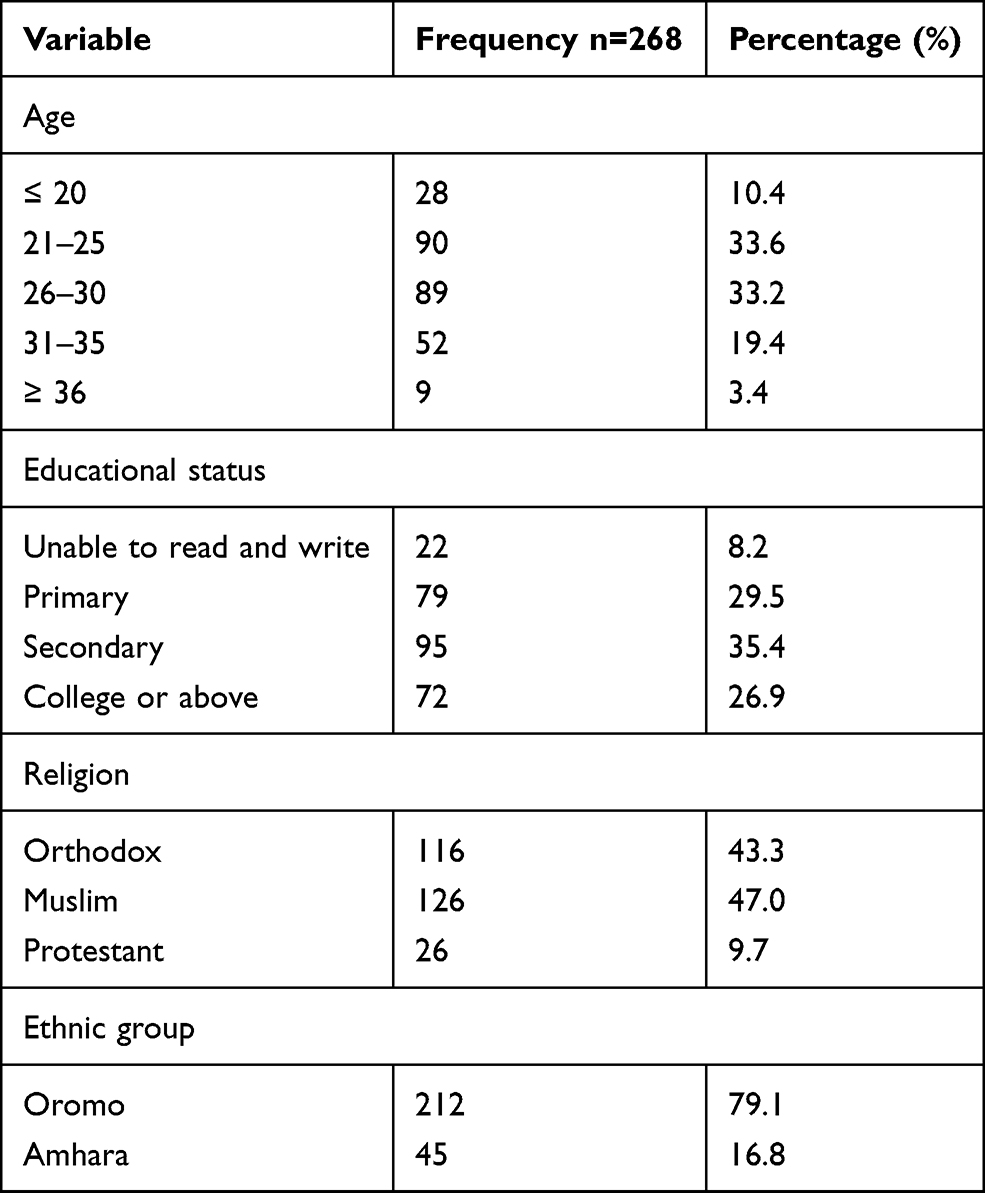 |
Table 2 Sociodemographic Characteristics of Women Who Underwent Induction of Labor from March 16 to May 16, 2020, in Public Hospitals of Arsi Zone in AUTRH, Kersa Primary Hospital & Bokoji Primary Hospital |
Obstetric Characteristics of the Study Participants
This study shows that of the total participants, more than half (59.7%) of them were prime para. About 253 (94.4%) of the participants had ANC follow-up during pregnancy. Out of the total study participants (268), 200 (74.6%) of them had a blood pressure of 90/60 to 140/90 mmHg at admission. The majority of participants’ gestational age was 163, (60.8) was a term pregnancy. Among women who underwent induction of labor, 113 (42.2%) had premature rupture of membranes (PROM) (Table 3).
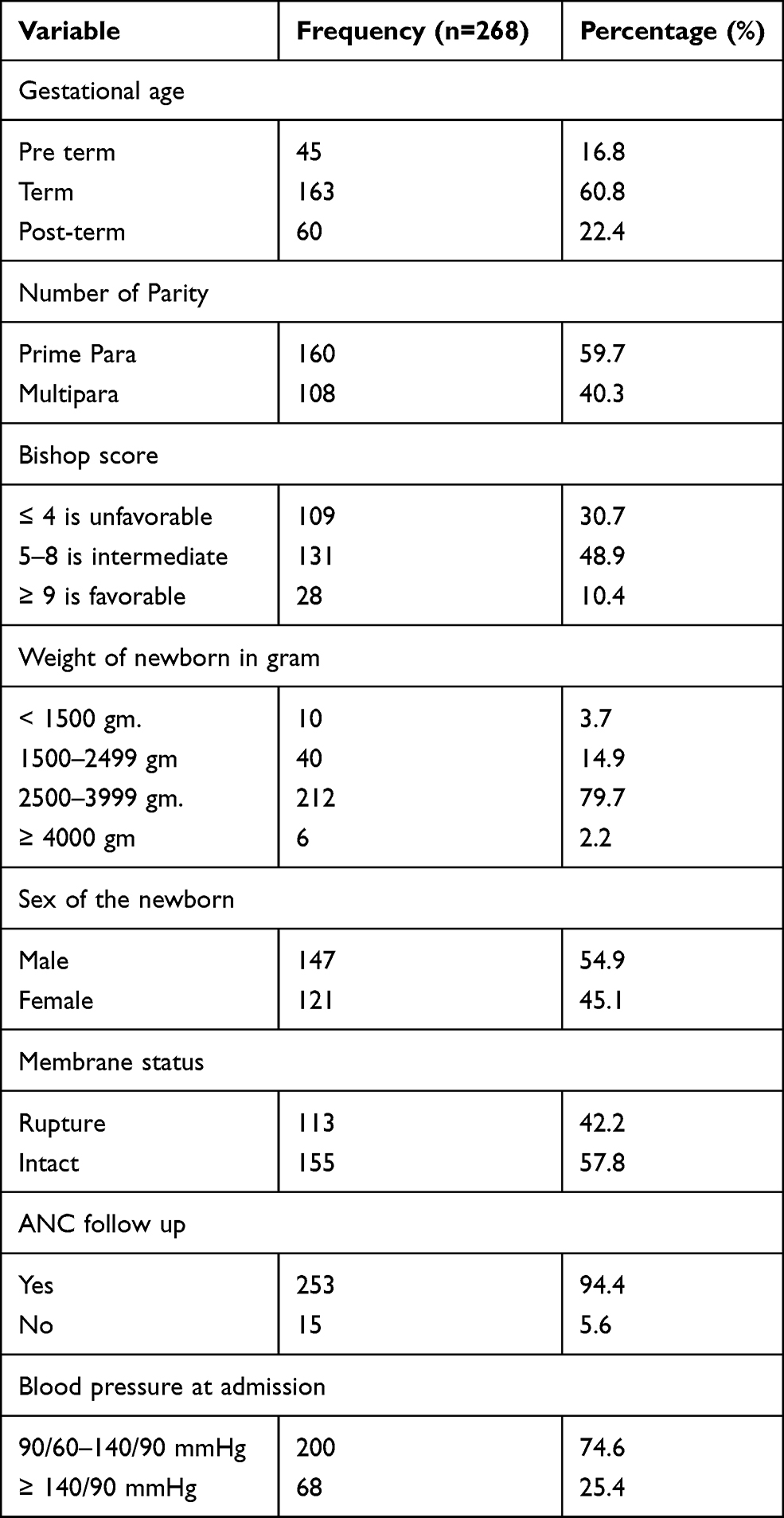 |
Table 3 Obstetric Characteristics of Women Who Underwent Induction of Labor in Public Hospitals of Arsi Zone from March 16 to May 16, 2020 (n=268) |
Indication for Induction of Labor
In this study, there were different indications of induction of labor. From this, PROM takes the largest account of 100 (37.3%). The second-largest indication of induction of labor was pregnancy-induced hypertension 54 (20.1%), followed by post-term pregnancy 46 (17.2%), Oligohydramnios 35 (13.1%), Antepartum hemorrhage (APH) 11 (4.1%), Chorioamnionitis 10 (3.7%), Intrauterine fetal death (IUFD) 7 (2.6%), and Congenital anomaly 5 (1.9%).
Methods of Induction of Labor
In this study, the most commonly used method of induction was the Foley catheter for ripening, followed by Oxytocin IV infusion 159 (59.3%). The second commonest method of induction was Oxytocin only 81 (30.2%), followed by Misoprostol for ripening, then Oxytocin 27 (10.1%), and ARM and Oxytocin 1. (0.4%).
The Magnitude of Failed Induction of Labor
In this study, the magnitude of failed induction of labor in the Arsi zone was 57 (21.3%). (Figure 2).
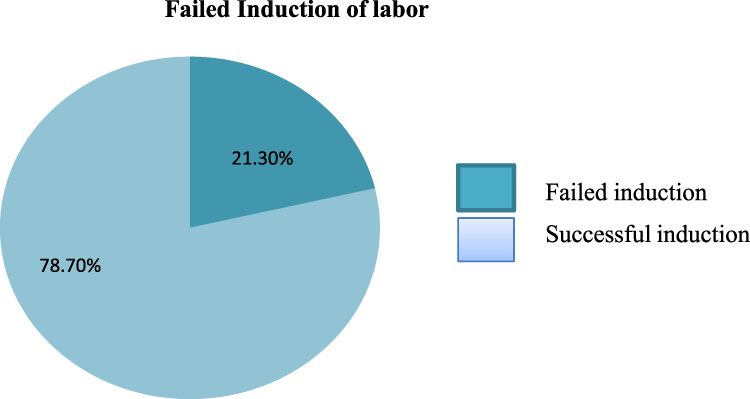 |
Figure 2 Magnitude of failed induction of labor among women who underwent induction of labor from March 16 to May 16, 2020, in Arsi zone public hospital, 2020. |
BMI
From the 268 study participants, BMI 18.5 - 24.9 were 185 (69 %), 25 - 29.9 were 68 (25.4 %) and <18.5 were 15. (5.6 %).
Factors Associated with Failed Induction of Labor in Bivariable Logistic Regression Analysis
In bivariable analysis, the association of independent variables for failed induction of labor was investigated and seven variables were found significantly associated with failed induction of labor. Those variables were maternal age, maternal residence, Bishop Score before induction started, premature rupture of membrane (PROM), indications for induction of labor, and time from the start of induction to delivery were significantly associated with failed induction of labor (Table 4).
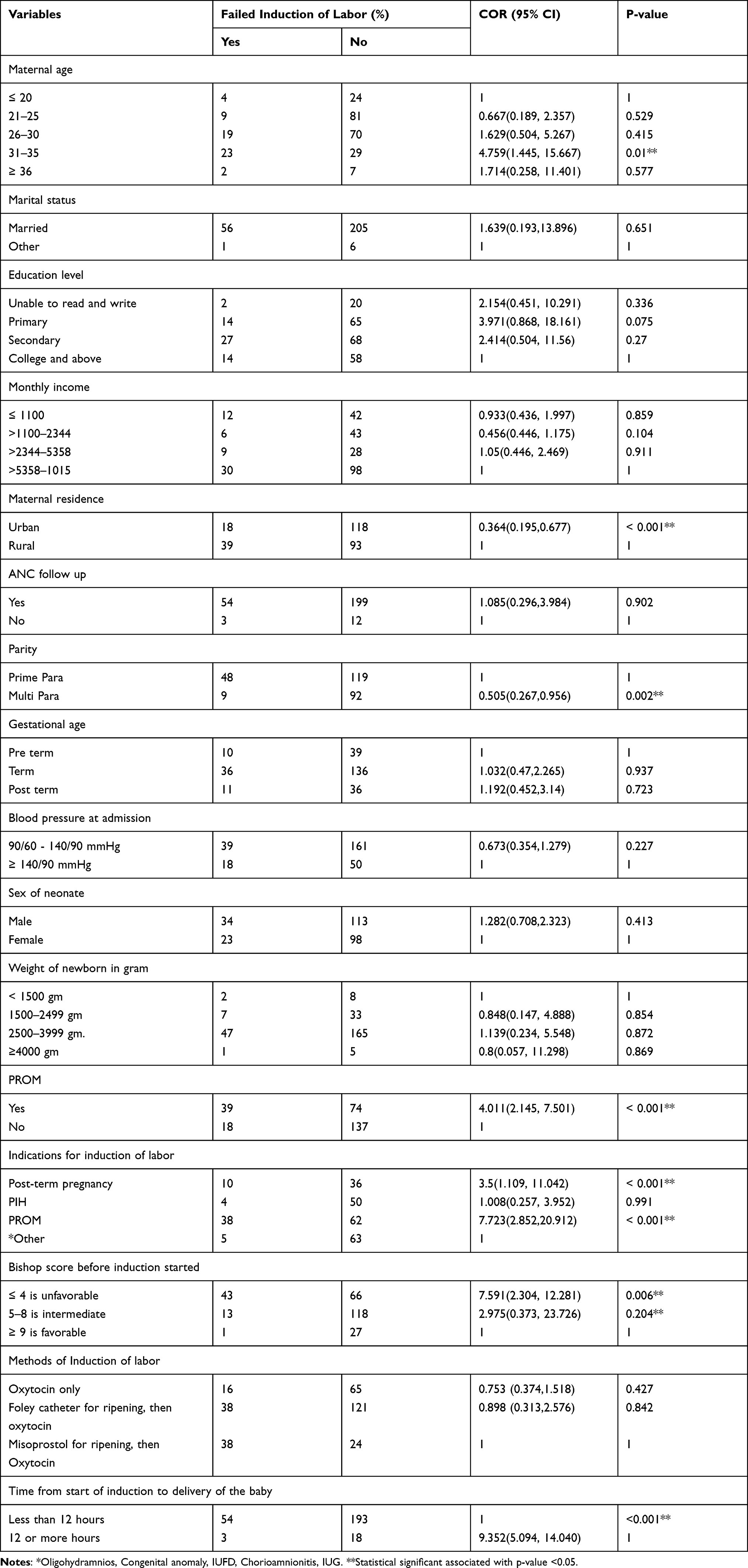 |
Table 4 Bi-Variable Analysis of Independent Variables Associated Factors for the Failed Induction of Labor Among Women Delivered in the Public Hospitals of the Arsi Zone from March 16 to May 16, 2020 (n=268) |
Associated with Failed Induction of Labor in Multivariable Logistic Regression Analysis
The results of multiple logistic regression models revealed that maternal age, maternal residence, Multi Para, Bishop Score 4, indications for induction of labor: PROM and post-term, and time from the start of induction to delivery were significantly associated with failed induction of labor.
Maternal age at 31–35 years was 8.788 times more likely to have failed induction of labor than at age 20 years [AOR =8.788, 95% CI = (2.884–12.397)]. Maternal residence in urban areas is 0.356 times less likely to fail induction of labor than maternal residence in rural areas, with an odds ratio of [AOR=0.356, 95% CI: (0.143–0.886], and Multi Para is 0.390 times less likely than Prime Para with an odds ratio of [AOR=0.390, 95% CI: (0.147, 0.632). Those with a Bishop Score before induction started at 4 (unfavorable Bishop Score) were 5.155 times more likely to fail IOL than those with a Bishop Score of 9 (favorable Bishop Score) [AOR=5.155, 95% CI: 3.062–7.387].
Indications for induction of labor (PROM) are 4.15 times more likely to fail induction of labor than those indications are Oligohydramnios, Congenital anomalies, IUFD, Chorioamnionitis, and IUGR [AOR=4.158, 95% CI: (2.415, 9.554). 6.511 times more likely than greater than twelve hours [AOR =6.511, 95% CI: (2.477,10.116)] (Table 5).
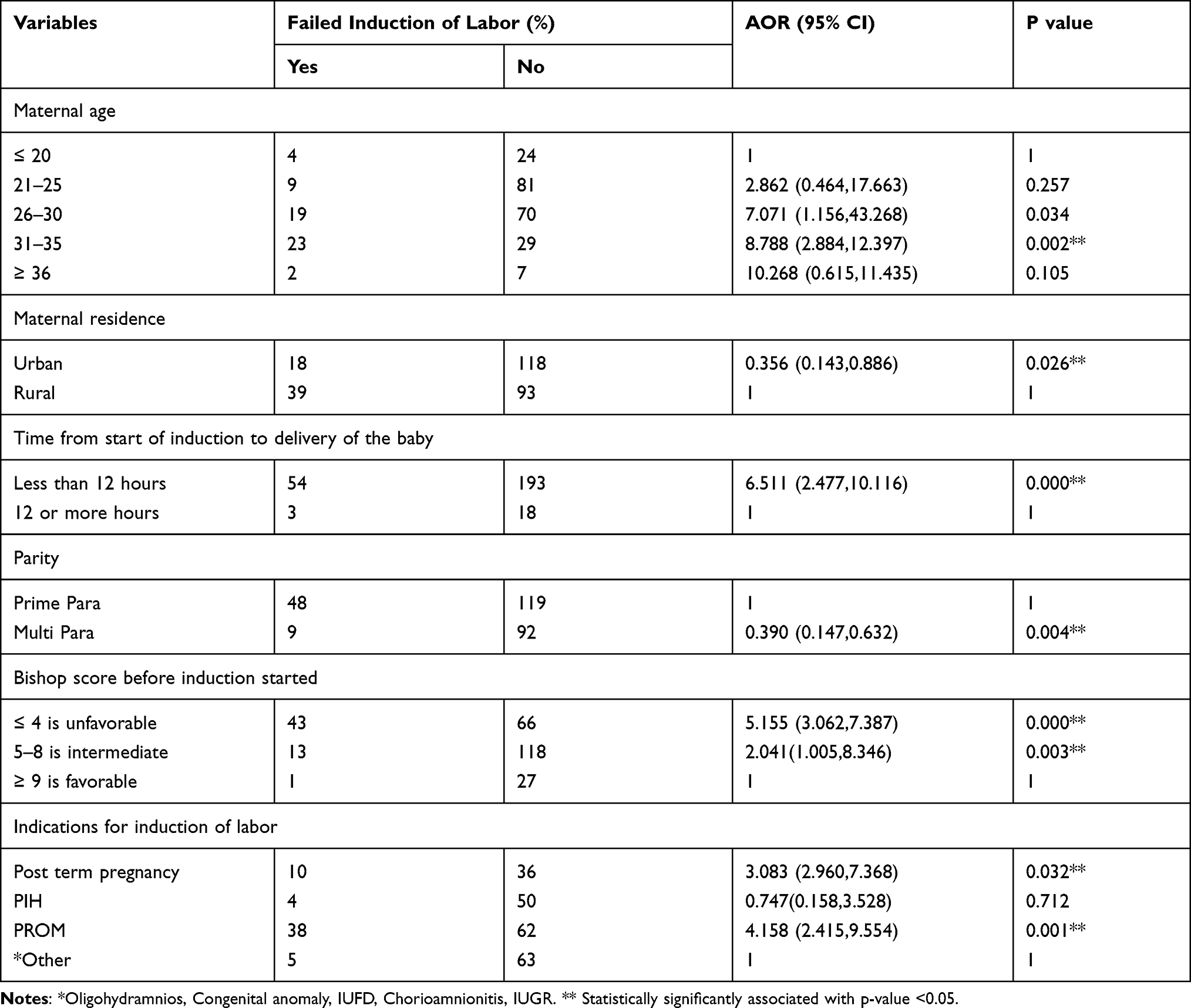 |
Table 5 Multivariate Analysis of Independent Variables Associated Factors for the Failed Induction of Labor Among Delivered in the Public Hospitals of Arsi Zone from March 16 to May 16, 2020 (n=268) |
Discussion
This study gives important information regarding the magnitude of failed inductions of labor and the factors associated with them, such as socio-demographic factors of women, anthropometry, obstetric factors, and methods of induction of labor, and indications for induction of labor.
In this study, the magnitude of the failed induction of labor was 57 (21.3%). This shows that out of five women who underwent induction into labor, one woman had experienced a failed induction into labor development. This result was in line with the study conducted at Jimma University Specialized Hospital, in which 21.4% experienced failed induction of labor.
These findings are in line with the study done in Hawassa Public Health Facilities, where 17.3% of women had a failed outcome of IOL.3,18
On the other hand, in this study, the rate of failed induction of labor was lower than in the studies done in Bhubaneswar city, Odisha (50.5%), Southwest Nigeria (36.5%), and Wolliso St. Luke Catholic Hospital (42%). This difference may be due to variation in commonly used methods for induction of labor, which was Foley catheter for ripening, then Oxytocin 157 (58.6%) was the most commonly used method of induction in the study area. While in other cases, misoprostol with other alternatives, like balloon catheters, was used as a common practice.6,15,20,
The finding of this study shows that mothers aged 31–35 years are 8.788 times more likely to fail induction of labor than mothers aged 20 years. This result is in agreement with the results reported by Hawassa Public Health Facilities, which shows that 9.21 times more likely in advanced maternal age.18
This study showed that being multipara was 61% less likely to fail induction of labor than being prime para with an odds ratio. Similarly, according to the study done in Hawassa Public Health, Facilities and Jimma University Specialized Hospital, failed induction was associated with primiparous women rather than multiparous.18,19
According to this study, women living in urban areas are 64.4% less likely to fail induction than women living in rural areas. Similarly, according to a study done at Dessie Referral Hospital, the odds of failed induction were more likely to fail IOL in women who lived in rural areas than in women who lived in urban areas.
This study shows that the time from the start of induction to delivery of the baby is less than twelve hours, more likely to fail IOL than the start of induction to delivery of a baby twelve hours or more than twelve hours. Similarly, Gabbe’s seventh edition recommends allowing adequate time for cervical ripening and development of active labor before diagnosing a failed induction helps to minimize the magnitude of the failed IOL.7
The finding of this study shows that an unfavorable Bishop 20 is more likely than a favorable Bishop score. Similarly, the study done in Hawassa Public Health Facilities shows an unfavorable Bishop is more likely than a favorable Bishop Score.18
The finding of this study show that the odds of failed induction were more likely in women with post-term pregnancies than in others. Similarly, a study done in a health resource-poor setting shows that the risk of failed induction of labor increases (p=0.0001) with post-term pregnancy than with preterm and post-term pregnancy.22
These studies reveal that premature rupture of the membrane increases the chance of failed induction of labor more than an intact membrane. This study is in line with a study done at Assam Medical College and Hospital, Dibrugarh, Assam, India, which shows that being PROM increases the chance of failed induction of labor.22
Strength and Limitation
Strength of the Study
- Add BMI variable on the study which was not previously done in our country
- Use of primary data
- A high response rate of respondents
Limitation of the Study
- Recall Bias of the mothers during giving the data.
- Since this study was a cross-sectional study design, the nature of the study may be difficult to ascertain the causal relationship between the study variables.
Conclusion
Based on this finding, it was concluded that the overall Arsi zone public hospital magnitude of failed induction of labor was 23%. Failed induction of labor in this study is relatively the same as failed induction of labor reported by other studies from different countries. The factors identified to be significantly associated with failed induction of labor in this study were: maternal age, maternal residence, multi-para, Bishop Score before induction started, indications for induction of labor: PROM and post-term pregnancy, and time from the start of induction to delivery were significantly associated with failed induction of labor.
Abbreviations
AOR, Adjusted Odds Ratio; APGAR, Appearance, Pulse, Grimace, Activity, Respiration; ARM, Artificial Rupture of Membranes; AUTRH, Arsi University Referral and Teaching Hospital; BMI, Body Mass Index; BP, Blood Pressure; CS, Cesarean Section; EMDHS, Ethiopian Mini Demography Health Survey; ETB, Ethiopian Birr; FOIL, Failed induction of labor; IOL, Induction of Labor; IUFD, Intra Uterine Fetal Death; IUGR, Intrauterine Growth Restriction; NICU, Neonatal Intensive Care Unit; OR, Odds Ratio; PIH, Pregnancy Induced Hypertension; PPROM, Preterm Premature Rupture of the Membranes; PROM, Premature Rupture of the Membranes; SDG, Sustainable Development Goal; SPSS, Statistical Package for Social Science; VD, Vaginal Delivery; W/H2, Weight over height square; WHO, World Health Organization.
Data Sharing Statement
We can affirm that the data we have used for this research is available on our hands and we can provide it when it is needed by this journal.
Ethics Approval and Informed Consent
An ethical clearance letter was taken from Wollega University Ethical Review Board. The approval letter was obtained from selected public hospitals of the Arsi zone. The procedure and purpose of the study were explained to the study participant and written informed consent was taken from participants.
Consent for Publication
We, the undersigned, gave our consent for the publication to be published in the above Journal and Article. We confirm that we have seen and been allowed to read both the Material and the Article. We understand that journals may be available in both print and on the internet, and will be available to a broader audience through marketing channels and other third parties. Therefore, anyone can read material published in the Journal.
Acknowledgments
We would like to thanks Wollega University, the institute of health sciences, the School of nursing, and the midwifery Department of nursing for giving us the chance to conduct this study and financial support. We would also like to express our heartfelt gratitude to the participant of this study. We also would like to thanks our advisors Mr. Reta Tsegaye (BSc, MSc, Assistance Professor) and Dr. Aaga Wakgari (MD, Assistance professor in Obstetrics and Gynecology) for their constructive advice, support, valuable comments, and suggestions during the process of conducting this study.
Author Contributions
Both authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, and acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
Wollega university institute of health science has funded us with twenty-five thousand (25000) Ethiopian birr.
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. WHO Recommendations: Induction of Labor at or Beyond Term.Geneva: World Health Organization; 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535795/.
2. Rajput DA, Bhalerao MV. Induction of labor: a review. J Midwifery Women’s Health. 2014;24(11):1057–1064.
3. Dilnessa T, Temesgen K, Workie A. The proportion of failed induction of labour and associated factors among women undergoing induction of labour in Dessie referral hospital: northeast Ethiopia a cross-sectional study. Asian J Preg Childbirth. 2019;2(3):1–13.
4. Lawani OL, Onyebuchi AK, Iyoke CA, Okafo CN, Ajah LO. Obstetric outcome and significance of labour induction in a health resource poor setting. Obstet Gynecol Int. 2014;2014:419621. doi:10.1155/2014/419621
5. West HM, Jozwiak M, Dodd JM. Methods of term labor induction for women with a previous cesarean section. Cochrane Database Syst Rev. 2017;2017(6):CD009792. doi:10.1002/14651858.CD009792.pub3
6. Segni H, Negussie D. Obstetric management guideline for Jimma University Specialized Hospital (JUSH); In use since Sept.2010. 2010;1–302. Available from: https://www.researchgate.net/publication/275029069_Obstetric_management_guideline_for_Jimma_University_Specialized_Hospital_JUSH_In_use_since_Sept2010. Accessed September 20, 2021.
7. Niebly JR. Consult E. In: Gabbe S, Niebyl J, Simpson J, editors. Obstetrics Normal and Problem Pregnancies.
8. Tripathy P, Pati T, Baby P, Mohapatra SK. Prevalence and predictors of failed induction. Int J Pharm Sci Rev Res. 2016;39(2):189–194.
9. Sharada K, Warrier H, Reddy AK, Thulasi P. Misoprostol and Oxytocin in the induction of labor. Int Arch Integr Med. 2018;5(3):97–105.
10. Ahmed I. Factors associated with failed induction of labor in a secondary care hospital. J Pak Med Assoc. 2012;62(January):6–10.
11. World Health Organization. The Global Strategy for Women’s, Children’s and Adolescents’ Health (2016–2030); 2015:1–108. Available from: https://www.who.int/life-course/partners/global-strategy/globalstrategyreport2016-2030-lowres.pdf. Accessed September 20, 2021.
12. Federal Democratic Republic of Ethiopia. Demographic and Health Survey; 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf. Accessed September 14, 2021.
13. Ethiopian Public Health Institute and ICF. Ethiopia; Mini Demographic and Health Survey; 2019. Available from: https://dhsprogram.com/pubs/pdf/FR363/FR363.pdf. Accessed September 14, 2021.
14. Cunningham FG, Leveno KJ, Bloom SL. Williams Obstetrics.
15. Bello FA, Akinyotu OO. Predictors of successful induction of labour at a tertiary obstetric service in Southwest Nigeria.Trop J Obstet Gynaecol. 2016;33(2):143–148. doi:10.4103/0189-5117.192213
16. Acharya T, Devkota R. Outcome of misoprostol and oxytocin in the induction of labor. SAGE Open Med. 2017;5:1–7. doi:10.1177/2050312117700809
17. Bekru ET, Yirdaw BE. Success of labor induction institution-based cross-sectional study Wolaita Sodo, South Ethiopia. Int J Nurs Midwifery. 2018;10(12):161–167. doi:10.5897/IJNM2018.0303
18. Hurissa BF, Geta M, Belachew T. Prevalence of failed induction of labor and associated factors among women delivered in Hawassa Public Health Facilities, Ethiopia, 2015. J Women’s Health Care. 2015;4(5):1000253. doi:10.4172/2167-0420.1000253
19. Girma W, Tseadu F, Wolde M. Outcome of Induction and Associated Factors among Term and Post- Term Mothers Managed at Jimma University Specialized Hospital: a Two Years ’ Retrospective Analysis. Ethiop J Health Sci. 2016; 26(2):121–130.
20. Abdulkadir Y, Dejene A, Geremew MA, Dechasa B. Induction of Labor Prevalence and Associated Factors for Its Outcome at Wolliso St. Luke, Catholic Hospital, South West Shewa, Oromia. Intern Med.2017;7(5): 1000255. doi:10.4172/2165-8048.1000255
21. Bassetty KC, Ahmed RD. Failed induction of labor (IOL): an overview regarding obstetric outcome and its significance in a health resource poor setting over a period of 11 months. Int J Reprod Contracept Obstet Gynecol. 2017;6(8):3646-3650. doi:10.18203/2320-1770.ijrcog20173502
22. Bassetty KC, Ahmed RD. Failed induction of labor (IOL): an overview regarding the obstetric outcome and its significance in a health resource-poor setting for 11 months. Int J Reprod Contraception Obstet Gynecol. 2017;6(8):3646. doi:10.18203/2320-1770.ijrcog20173502
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.